Back to Journals » International Medical Case Reports Journal » Volume 18
Septo-Optic Dysplasia Plus with Bilateral Homonymous Hemianopia – Case Report
Authors Lestak J ![]() , Fus M
, Fus M ![]() , Kyncl M
, Kyncl M
Received 19 December 2024
Accepted for publication 27 August 2025
Published 8 September 2025 Volume 2025:18 Pages 1159—1165
DOI https://doi.org/10.2147/IMCRJ.S513192
Checked for plagiarism Yes
Review by Single anonymous peer review
Peer reviewer comments 2
Editor who approved publication: Dr Scott Fraser
Jan Lestak, Martin Fus, Martin Kyncl
Faculty of Biomedical Engineering, Czech Technical University in Prague, Kladno, Czech Republic
Correspondence: Jan Lestak, Faculty of Biomedical Engineering, Czech Technical University in Prague, Kladno, Czech Republic, Email [email protected]
Abstract: The paper presents a case report of a man (born1968) who was examined for unusual changes in the visual fields. During the examination in 2020, the right eye had esotropia, the pupillary reaction was correct. The ocular findings on the anterior segment and the ocular media were normal. The papilla of the right eye was temporally paler with c/d=0.5, the left papilla was pale with c/d=0.6, otherwise the background was normal. IOP: 16/18 mmHg. During the examination, diffuse loss of the nerve fiber layer (50 um, resp. 49 um) was detected using OCT, and similarly low values were also found for vessel density. The visual fields showed left-sided homonymous hemianopia with central sparing, partially extending into the upper right quadrants. Electrophysiological examinations of the retina (pattern electroretinogram) and the entire visual analyzer (pattern visual evoked potential – PVEP) showed bilaterally lower amplitudes. The latencies of the P00 VEP peak were not prolonged. For these changes, a magnetic resonance imaging (MRI) examination of the brain was performed with the finding of agenesis of the corpus callosum, associated trigone of the lateral ventricles on both sides. Malformation of the development of the cerebral cortex temporooccipitally medially on the right, of the nature of plymicrogyria. Heterotopia of gray matter periventricularly occipitally on the right. Bilateral atrophy of the optic nerves and chiasm. In the case report of SOD plus, unusual changes in the visual fields are described – homonymous left-sided hemianopia with central sparing. MRI examination of the brain helped to classify this lesion in the temporo-occipital medial region on the right with polymicrogyria.
Keywords: septo-optic dysplasia, visual field – homonymous left-sided hemianopia with central sparing, imaging methods, electrophysiological examinations
Introduction
In a previous paper, a case report of a young man with optic nerve hypoplasia was described, where apart from deep central excavation on the fundus papillae, low values of the retinal nerve fiber layer and narrower chiasm, there were no morphological changes. Functional changes were characterized by concentric narrowing of the visual field and abnormal visual evoked responses.1
Another case of optic nerve hypoplasia may occur with otherwise normal ocular findings but with intracranial abnormalities. Such a finding may be septo-optic dysplasia (SOD), characterized by agenesis of the septum pellucidum and/or dysgenesis of the corpus callosum, hypoplasia of the chiasm or optic nerves, and hormonal dysfunction with pituitary or hypothalamic changes. Most cases also show abnormalities of cortical development known as septo-optic dysplasia plus.2
Because we had the opportunity to observe this extreme case with intracranial abnormalities, we would like to present this case report. In addition, an unusual visual field defect was found in this patient.
Case Report
A man (born 1968), who had complained of poor motor skills since childhood, was examined by ophthalmologists for unusual changes in the visual fields (homonymous left-sided hemianopia). He was examined by the first author in 3/2020 for these changes in visual fields with the following findings: Visual acuity 1.0 with +1 D sphere −0.5 D cylinder in axis 180 degrees in both eyes; near visual acuity to near was 1.0 with addition +2,5 D; intraocular pressure: 16/18 mmHg (Ocular Response Analyser).
Esotropia of the right eye (5 degrees), free motility, no diplopia. Pupillary functions were correct. Ocular findings on the anterior segment and ocular media normal. Papilla of the right eye temporally paler with c/d=0.5, left papilla pale with c/d=0.6, otherwise background normal (Figure 1). Color perception was impaired (numbers are pronounced but sometimes interpreted incorrectly).
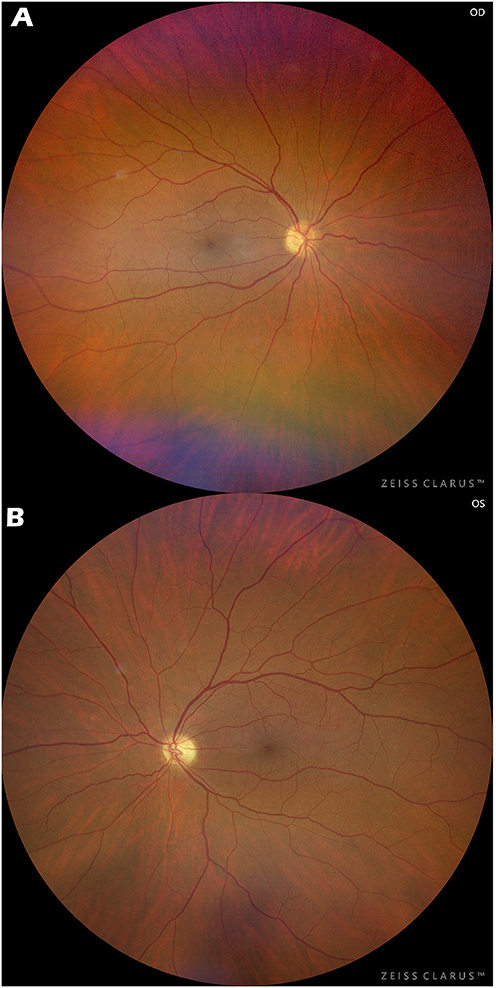 |
Figure 1 Photograph of the fundus. On the right, temporal papilla pallor (A), On the left, pale papilla (B). |
Visual Field: left-sided hemianopia partially extending into the upper right quadrants with central sparing (Figure 2).
 |
Figure 2 Visual field of the right eye (A) and left eye (B) Left-sided hemianopia extending into the right upper quadrants with central sparing. The examination was performed using the Medmont M700 neurological program. |
During the examination, a diffuse loss of the retinal nerve fiber layer (RNFL – 50 µm, respectively 49 µm) was detected using OCT. A similar decrease in vessel density was also detected. The examination was performed on the Optovue AngioVue/Avanti device (Figure 3).
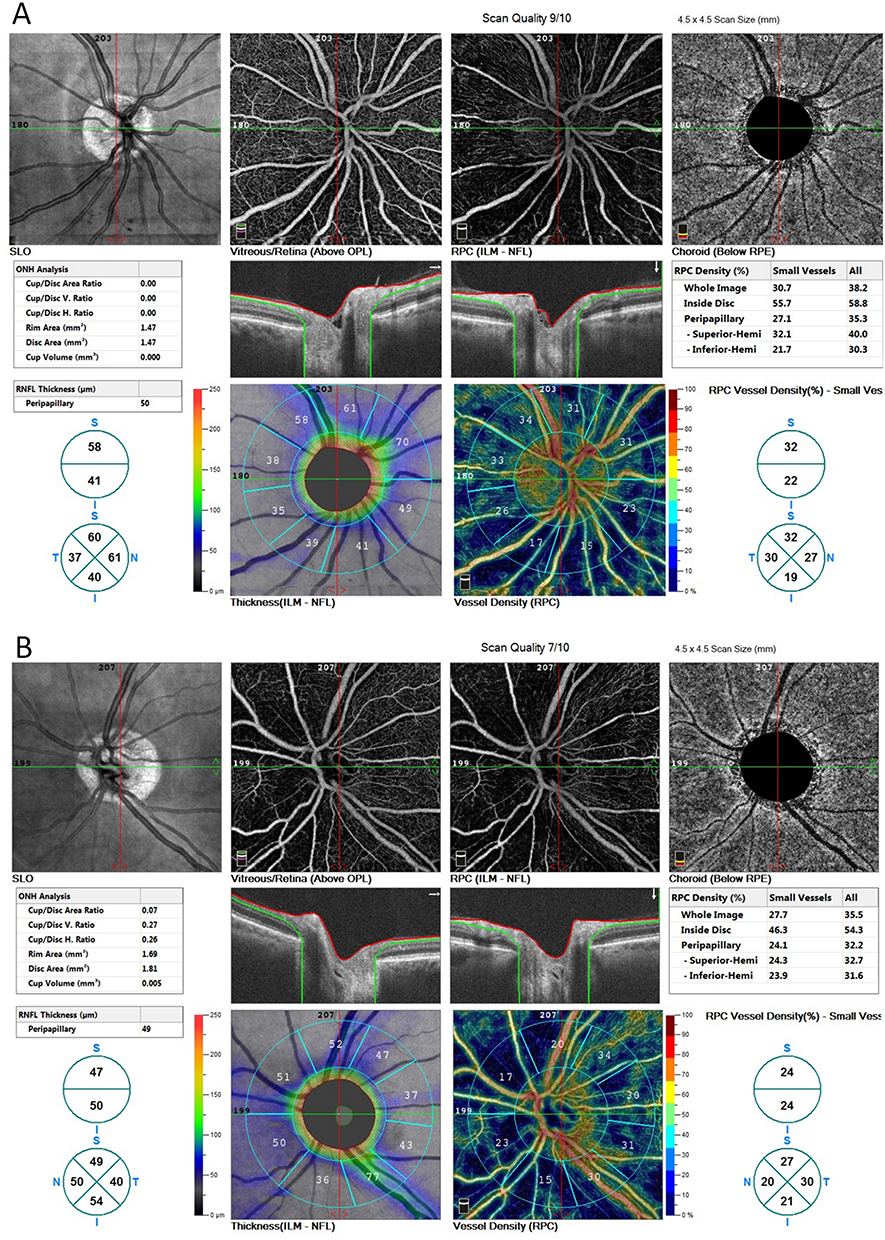 |
Figure 3 Average peripapillary RNFL values are bilaterally pathological. Right 50 um (A), left 49 um (B). Similarly, vessel density values. VDs right 27.1, left 24.1%. In the upper images (SLO), atrophic choroid rims are also visible around the optic nerve targets. The examination was performed with an OCT device Optovue AngioVue/Avanti. |
Electrophysiological examination of the retina (pattern electroretinogram – PERG) showed bilaterally lower amplitudes, right 9 uV, left 7.1 uV. Visual evoked potentials (PVEP): with 1 degree square stimulation, bilaterally lower amplitudes (7.5 uV, respectively 6.5 uV), without prolongation of P100 latency. With 15 minutes square stimulation, the responses were lower (6.5 uV, respectively 8.4 uV). Even with this stimulation, the latency of the P100 peak was not prolonged. The examination was performed with the Roland Consult electrophysiological diagnostic system according to the ISCEV methodology. The size of the stimulation field was 41×31 angular degrees.
Neurological findings were normal. Magnetic resonance imaging (MRI) of the brain was recommended to elucidate alterations in the visual fields. MRI of the brain conducted in December 2022 revealed a spectrum of telencephalic commissural malformations: agenesis of the corpus callosum and associated enlargement of the trigones of the lateral ventricles bilaterally (progressing to a form of colpocephaly). A malformation of cortical development characterized by abnormal postmigratory development and cortical arrangement, consistent with polymicrogyria, was observed in the temporal-occipital region medially on the right. Heterotopia of the cerebral gray matter, a disorder classified within the group of abnormal cell migration, was identified periventricularly in the occipital region on the right. Furthermore, bilateral atrophy of the optic nerves and optic chiasm was evident (Figures 4–6).
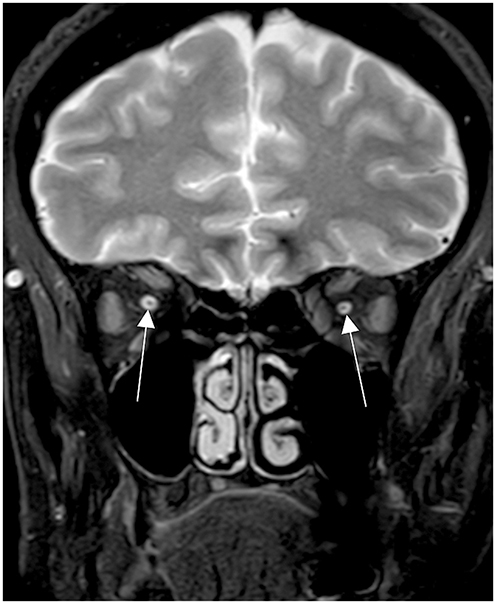 |
Figure 4 MRI of the optic nerve; T2 mDIXON sequence. Arrows indicate the hypoplastic intraorbital diameters of both the optic nerves. |
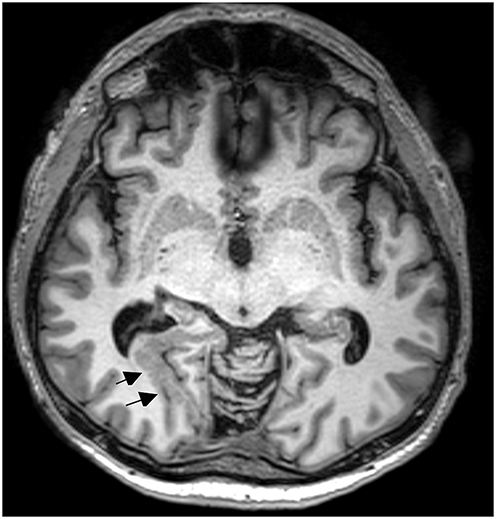 |
Figure 5 Brain MRI, MPRAGE, axial reconstruction of the image. Short arrows indicate polymicrogyria in the right occipital region. Colpocephaly was observed. |
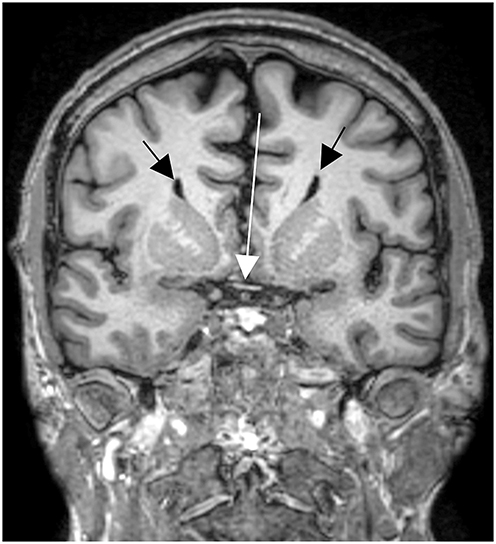 |
Figure 6 Brain MRI scan. The primary white arrow highlights chiasmal atrophy. Secondary black arrows indicate the distinctive bull’s horn configuration of the lateral ventricles associated with agenesis of the corpus callosum. |
Discussion
Septo-optic dysplasia syndrome (SOD), a congenital disorder of the midbrain structures, was first described by the French-Swiss neurologist Georges de Morsier.3
Although phenotypic penetrance can be highly variable, the result is broad heterogeneity, characterized by the following triad:
- optic nerve hypoplasia,
- agenesis of middle structures (septum pellucidum and corpus callosum),
- hypoplasia of the hypothalamic-pituitary axis.
For a correct diagnosis to be made, at least two abnormalities from this triad must be present.4
On the other hand, patients with SOD, in addition to the pathologies described above, may also show other specific brain abnormalities.
Due to this complexity, the scientific community still discusses the most appropriate nomenclature to standardize the diagnosis of this disorder and recommends the use of the term SOD plus syndrome.5
SOD plus typically presents with less severe optic nerve damage and cortical anomalies such as polymicrogyria or cortical dysplasia.6
Visual field defects in SOD may be characterized by concentric narrowing, bitemporal hemianopia, central, binasal, or altitudinal hemianopia.7,8
Another unusual finding in the presented case report was left-sided homonymous hemianopia with preservation of the central visual field. A similar finding would be localized in the visual cortex. Using MRI of the brain, we localized it in the medial temporo-occipital region on the right, where polymicrogyria was demonstrated. We have not recorded a similar case of changes in the visual fields in the available literature.
Conclusion
Optic hypoplasia in septo-optic dysplasia may not always have clear morphological and functional ophthalmological manifestations. Left-sided hemianopia with central sparing is evidence of this in this case report. Brain MRI examination helped us to verify and localize it, which, in addition to intracranial abnormalities typical of SOD, also demonstrated temporooccipital polymicrogyria on the right.
Data Sharing Statement
The datasets used and/or analysed during the present study are available from the corresponding author on reasonable request.
Ethics Statement
All details, medical records, figures, medical history or test results were used with the written consent for publication from the patient. All data used were anonymized. The presented case report was performed according to the Declaration of Helsinki. No official institutional approval was required by the internal ethics committee of the JL Eye Clinic (Prague, Czech Republic) to publish the details of the case report. The JL Eye Clinic is a clinical department of the university department of the Faculty of Biomedical Engineering CTU and works under its auspices.
Author Contributions
All authors made a significant contribution to the work reported, whether that is in the conception, study design, execution, acquisition of data, analysis and interpretation, or in all these areas; took part in drafting, revising or critically reviewing the article; gave final approval of the version to be published; have agreed on the journal to which the article has been submitted; and agree to be accountable for all aspects of the work.
Funding
No funding was received.
Disclosure
All authors have nothing to disclose related to this case report. All authors report no conflict of interests.
References
1. Lestak J, Prazakova L, Fus M, Kyncl M. Optic nerve hypoplasia - case report. Int Med Case Rep J. 2024;17:835–841. doi:10.2147/IMCRJ.S479333
2. Reyes A, Galvis J, Estupiñán Y. Septo-optic dysplasia plus: a case report for reviewing and recognizing this condition. Biomédica. 2024;44(4):451–459. doi:10.7705/biomedica.7370
3. De Morsier G. Etudes sur les dysraphies cranioencephaliques: agenesis du septum lucidum acec malformatnio du tractus optique. La Dysplasie Septooptique. Schweiz Arch Neurol Psychiatr. 1956;77(1–2):267–292.
4. Izenberg N, Rosenbtum M, Parks JS. The endocrine spectrum of septo-optic dysplasia. . Clin Pediatr. 1984;23(11):632–636. doi:10.1177/000992288402301105
5. Miller SP, Shevell MI, Patenaude Y, Poulin C, O’Gorman AM. Septo-optic dysplasia plus: a spectrum of malformations of cortical development. . Neurology. 2000;54(8):1701–1703. doi:10.1212/WNL.54.8.1701
6. Zoric L, Nikolic S, Stojcic M, Zoric D, Jakovljevic S. Septo-optic dysplasia plus: a case report. BMC Res Notes. 2014;7(1):191. doi:10.1186/1756-0500-7-191
7. Katagiri S, Nishina S, Yokoi T, et al. Retinal structure and function in eyes with optic nerve hypoplasia. . Sci Rep. 2017;7(1). doi:10.1038/srep42480
8. Brooks DB, Subramanian PS. Monocular temporal hemianopia with septo-optic dysplasia. J Neuroophthalmol. 2006;3(3):195–196. doi:10.1097/01.wno.0000235582.10546.43
 © 2025 The Author(s). This work is published and licensed by Dove Medical Press Limited. The
full terms of this license are available at https://www.dovepress.com/terms
and incorporate the Creative Commons Attribution
- Non Commercial (unported, 4.0) License.
By accessing the work you hereby accept the Terms. Non-commercial uses of the work are permitted
without any further permission from Dove Medical Press Limited, provided the work is properly
attributed. For permission for commercial use of this work, please see paragraphs 4.2 and 5 of our Terms.
© 2025 The Author(s). This work is published and licensed by Dove Medical Press Limited. The
full terms of this license are available at https://www.dovepress.com/terms
and incorporate the Creative Commons Attribution
- Non Commercial (unported, 4.0) License.
By accessing the work you hereby accept the Terms. Non-commercial uses of the work are permitted
without any further permission from Dove Medical Press Limited, provided the work is properly
attributed. For permission for commercial use of this work, please see paragraphs 4.2 and 5 of our Terms.