Back to Journals » Neuropsychiatric Disease and Treatment » Volume 14
Sensory function in cluster headache: an observational study comparing the symptomatic and asymptomatic sides
Authors Malo-Urriés M, Hidalgo-García C ![]() , Estébanez-de-Miguel E, Tricás-Moreno JM, Santos-Lasaosa S
, Estébanez-de-Miguel E, Tricás-Moreno JM, Santos-Lasaosa S ![]() , Jahanshahi M
, Jahanshahi M ![]()
Received 31 August 2018
Accepted for publication 3 October 2018
Published 10 December 2018 Volume 2018:14 Pages 3363—3371
DOI https://doi.org/10.2147/NDT.S186051
Checked for plagiarism Yes
Review by Single anonymous peer review
Peer reviewer comments 3
Editor who approved publication: Dr Roger Pinder
Miguel Malo-Urriés,1 César Hidalgo-García,1 Elena Estébanez-de-Miguel,1 José Miguel Tricás-Moreno,1 Sonia Santos-Lasaosa,2 Marjan Jahanshahi3
1Physiotherapy Research Unit, Department of Physiatry and Nursing, University of Zaragoza, Zaragoza, Spain; 2Neurology Service, University Clinical Hospital Lozano Blesa, Zaragoza, Spain; 3Cognitive Motor Neuroscience Group, Department of Clinical and Movement Neurosciences, University College London Queen Square Institute of Neurology, The National Hospital for Neurology and Neurosurgery, London, UK
Background: Based on inconsistent sensory alterations demonstrated in cluster headache (CH), the aim of this study was to determine whether patients with CH develop sensory changes in the symptomatic side compared to the asymptomatic side.
Methods: Quantitative sensory testing (QST), including pressure pain threshold (PPT), tactile detection threshold (TDT), prick detection threshold (PDT), and two-point detection threshold (2PDT), was evaluated in 16 patients (seven women; age 41.9±6.8 years) with CH. Test sites included the first, second, and third divisions of the trigeminal nerve, cervical spine, and thenar eminence in the symptomatic and asymptomatic sides.
Results: The symptomatic side, compared to the asymptomatic side, presented significantly decreased PPT in the first (P=0.011; 423.81±174.05 kPa vs 480.13±214.99 kPa) and second (P=0.023; 288.88±140.80 kPa vs 326.38±137.33 kPa) divisions of the trigeminal nerve, significantly increased TDT in the first (P=0.002; 2.44±0.40 vs 1.74±0.24) and second (P=0.016; 1.92±0.34 vs 1.67±0.09) divisions, and increased 2PDT in the first division (P=0.004; 18.13±4.70 mm vs 15.0±4.92 mm) and neck (P=0.007; 45.31±20.65 mm vs 38.44±16.10 mm).
Conclusion: These results support the prior evidence suggesting a specific pattern of alteration of sensory function with alterations in the symptomatic side compared to the asymptomatic side.
Keywords: cluster headache, trigeminal autonomic cephalalgia, quantitative sensory testing
Introduction
Cluster headache (CH) is a primary headache disorder, which is classified as trigeminal autonomic cephalalgias (TACs).1 The characteristic symptoms are strictly unilateral headache, lasting from 15 to 180 minutes, usually involving the regions related to the first division of the trigeminal nerve, accompanied by ipsilateral autonomic features such as lacrimation, conjunctival injection, rhinorrhea, ptosis, miosis, or periorbital edema. Although CH is the most common primary TAC, its prevalence in the general population is about 0.1%.2
The pathophysiology of CH is not completely known.3 Clinical characteristics of CH suggest the involvement of the hypothalamus.4,5 Several studies have evidenced the activation of the suprachiasmatic nucleus of the hypothalamus in CH.6 Moreover, during the attack, a secondary activation of the trigemino-autonomic reflex has been demonstrated, probably through a hypothalamic trigeminal pathway, leading to the cranial autonomic features of CH.7,8 This includes the peripheral nerve fibers that innervate the pain-producing cranial vessels and dura mater and the centrally projecting fibers that synapse in the trigeminocervical complex.9
Repetitive activity in afferent fibers produced by CH may induce plastic alterations in somatosensory synaptic processing. Sensory disturbances including hypersensitive responses to mechanical, thermal, and electrical stimulation have been consistently shown to be a feature of headache patients, being associated with augmented central nervous system pain-processing mechanisms.10 Sensory changes have also been shown to be associated with poor prognosis in different pain conditions including CH.11 Thus, several authors have emphasized the importance of an accurate neurological evaluation in patients with CH.12,13
Quantitative sensory testing (QST) is a valid and reliable tool to evaluate somatosensory function and may be useful in characterizing patients with trigeminal pain disorders.14,15 QST provides information to illuminate the underlying mechanisms of CH.16
It has been proposed that CH may only affect certain aspects of sensory function following a specific pattern.8 However, previous evidence studying specific sensory changes in sensory function has offered inconsistent results. Ellrich et al11 evidenced a significant reduction in pressure pain in the periorbital region of the symptomatic side compared to the contralateral asymptomatic side of CH patients. Similarly, Coppola et al17 demonstrated lower pain thresholds on the symptomatic side compared to the asymptomatic side in episodic CH patients during the bout. On the other hand, Ashkenazi and Young18 found no evidence of specific sensory disturbances in CH. Ladda et al19 measured mechanical thresholds of the cheeks and the back of the hands in CH patients and found that the side of the body had no influence on the sensory perception and pain thresholds.
Based on the documented activation of the trigeminocervical system in CH and the controversy of previous literature about the specificity of mechanical sensory changes produced by CH, our study had a double objective: first, to determine whether patients with CH develop sensory changes to mechanical stimuli in the symptomatic side compared to the asymptomatic side; second, to investigate whether a specific pattern of sensory alteration is produced depending on the locations where the CH is experienced. We hypothesized that patients with CH would demonstrate altered sensory thresholds to mechanical stimuli in the symptomatic side compared to the asymptomatic side and the pattern of sensory alterations would depend on the locations where the CH is experienced.
Methods
The study was approved by the local ethics committee (Comité Ético de Investigación Clínica de Aragón) and was conducted in accordance with the Declaration of Helsinki. All participants were unpaid volunteers and gave their written informed consent before participation. The protocol was carried out in the facilities of the Faculty of Health Sciences, University of Zaragoza. The data for this study were collected during 2013–2016.
Participants
Eligible patients were older than 18 years with a clinical diagnosis of CH by a neurologist following the International Classification of Headache Disorders, third edition (ICHD-3). Participants were excluded if they presented any contraindication to QST or were unable to understand instructions or communicate with researchers.
The sample consisted of nine (56.3%) men and seven (43.8%) women with a mean age of 41.9 (SD=6.8) years. The average intensity of CH was 9.50 (SD=0.78) points on a visual analog scale (0–10 points) with an average duration of 77.5 (SD=55.0) minutes. Ten (62.5%) patients had episodic CH (in remission of more than 3 months), and six (37.5%) had chronic CH. Regarding the lateralization of pain, nine (56.3%) patients had right CH and seven (43.8%) left CH. The average age at the onset of the first CH attack was 27.4 (SD=8.2) years with a mean duration of illness of 13.4 (SD=10.7) years. The area related to the first division of the trigeminal nerve was the most frequently symptomatic (100.0%) followed by the area related to the second division of the trigeminal nerve (31.3% for main symptoms; 43.8% for shadows) and the area related to the third division of the trigeminal nerve (25.0% and 31.3% like shadows; shadow is a low-level ipsilateral persistent headache that can be a precursor of a CH attack).
Measurements
First, participants were asked to complete a questionnaire with demographic and clinical data, including age, gender, height, weight, and characteristics of CH (location, intensity, frequency, duration, and past history). The location of the pain was recorded by the patient on a scheme of the human body. The painful area was categorized into three divisions of the trigeminal nerve.
QST was performed to quantitatively measure the mechanical sensory function. Different modalities of mechanical stimuli were incorporated to provide an indirect measure of primary afferents that mediated both innocuous and painful sensation. This included pressure pain threshold (PPT), tactile detection threshold (TDT), prick detection threshold (PDT), and two-point detection threshold (2PDT).
PPT was measured using a pressure algometer (Somedic AB, Farsta, Sweden) with a probe size of 1 cm2 and application rate of 30 kPa/s in a perpendicular direction to the skin.20,21 The patients were instructed to press the button when the sensation under the probe changed from pressure to pressure and pain.22 Three measurements were performed at each site, and the geometric mean was used for further analysis. Test sites included bilaterally the first division of the trigeminal nerve (V1) on the forehead, second division of the trigeminal nerve (V2) on the cheek, third division of the trigeminal nerve (V3) on the jaw, cranium on the parietal bone, upper trapezius muscle, articular pillar of C2–C3, suboccipital muscles, and thenar eminence.
TDT and PDT were measured with a set of 20 calibrated Semmes–Weinstein monofilaments (Saehan, marking number 1.65–6.65; force 0.005–447 g) delivering a precise amount of pressure.20,21 To determine TDT and PDT, the method of limits was used, following a standardized protocol of five ascending and descending series.14 In the ascending series, monofilaments were applied in increasing order of strength until the patient reported the presence of the stimulus. In the descending series, monofilaments were applied in decreasing order of strength until the patient no longer detected the stimulus. Using the method of limits with suprathreshold and infrathreshold values, the geometrical mean was calculated. The number indicated in the monofilament was registered, corresponding to a logarithmic function of the applied force in grams.20,21 For TDT, the patient, with closed eyes, was instructed to indicate the detection of the touch of a monofilament. For PDT, the patient was instructed to indicate when the tactile sensation of the monofilament changed to sensation of prick. TDT and PDT were measured bilaterally on V1 (forehead), V2 (cheek), V3 (jaw), cervical spine (on the sternocleidomastoid muscle), ear (between lobule and tragus), and thenar eminence.
For 2PDT, a digital caliper (Mitutoyo) was used.23,24 To determine 2PDT, the method of limits was used, following a standardized protocol.25 The application was repeated five times, in ascending and descending order, obtaining a series of suprathreshold and infrathreshold values that were used to calculate a geometric mean. The separation of the two jaws of the caliper was modified by 5 mm. The patient, with closed eyes, was instructed to indicate “one” or “two” depending on the tactile points detected.23 This measure was performed bilaterally on V1 (forehead), V2 (cheek), V3 (jaw), cervical spine (on the sternocleidomastoid muscle), and thenar eminence.
QST was administered by the same specially trained researcher who was blinded to the symptomatic side.
Statistical analyses
The statistical analysis was performed with SPSS 20.0 (IBM Corporation, Armonk, NY, USA) for Windows. Categorical variables were summarized with frequencies. Normally distributed continuous variables are presented with mean, SD, and range, and in the case of nonnormality, median, and range were used. Categorical variables were compared using the chi-squared test, and continuous variables were compared using Wilcoxon signed-rank test for related samples and Mann–Whitney U test and Kruskal–Wallis tests for independent samples or Student’s t-test depending on the normality of the data. To evaluate the associations between QST and clinical and demographic characteristics of CH patients, Spearman correlation coefficient was calculated. The level of significance was set at P=0.05.
Results
Sixteen patients with CH diagnosed by neurologists on the basis of International Headache Society (IHS) criteria were recruited via advertisement. All patients met the selection criteria and were included in the study. Table 1 summarizes the baseline demographic and clinical data.
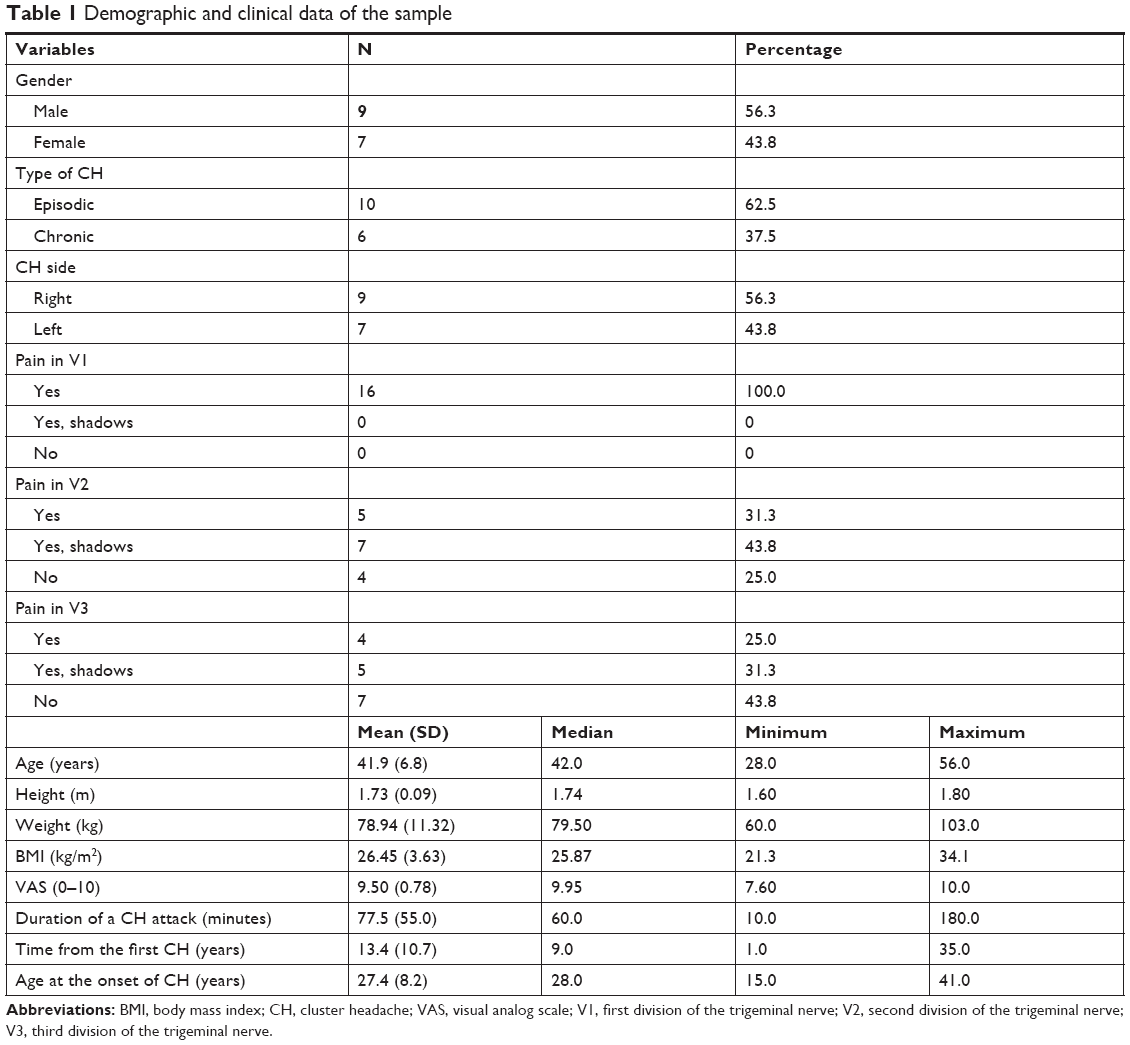 | Table 1 Demographic and clinical data of the sample |
The results of mechanical sensory thresholds are presented in Table 2. The symptomatic side presented significantly lower PPT in V1 (423.81 kPa, SD=174.05) and V2 (288.80 kPa, SD=174.05) areas compared to the asymptomatic side (480.13 kPa, SD=214.99; 326.38 kPa, SD=137.33; P=0.011 and P=0.023). With regard to the TDT, the symptomatic side showed significantly higher values in the V1 (2.42, SD=0.40) and V2 (1.92, SD=0.34) areas compared to the asymptomatic side (1.74, SD=0.24; 1.67, SD=0.09; P=0.002 and P=0.016). No statistically significant difference between the symptomatic and asymptomatic side was found for PDT. The 2PDT was significantly higher in the symptomatic side compared to the asymptomatic side in the V1 area (18.13 mm, SD=4.70; 15.0 mm, SD=4.92; P=0.004) and in the neck (45.31 mm, SD=20.65; 38.44 mm, SD=16.10; P=0.007).
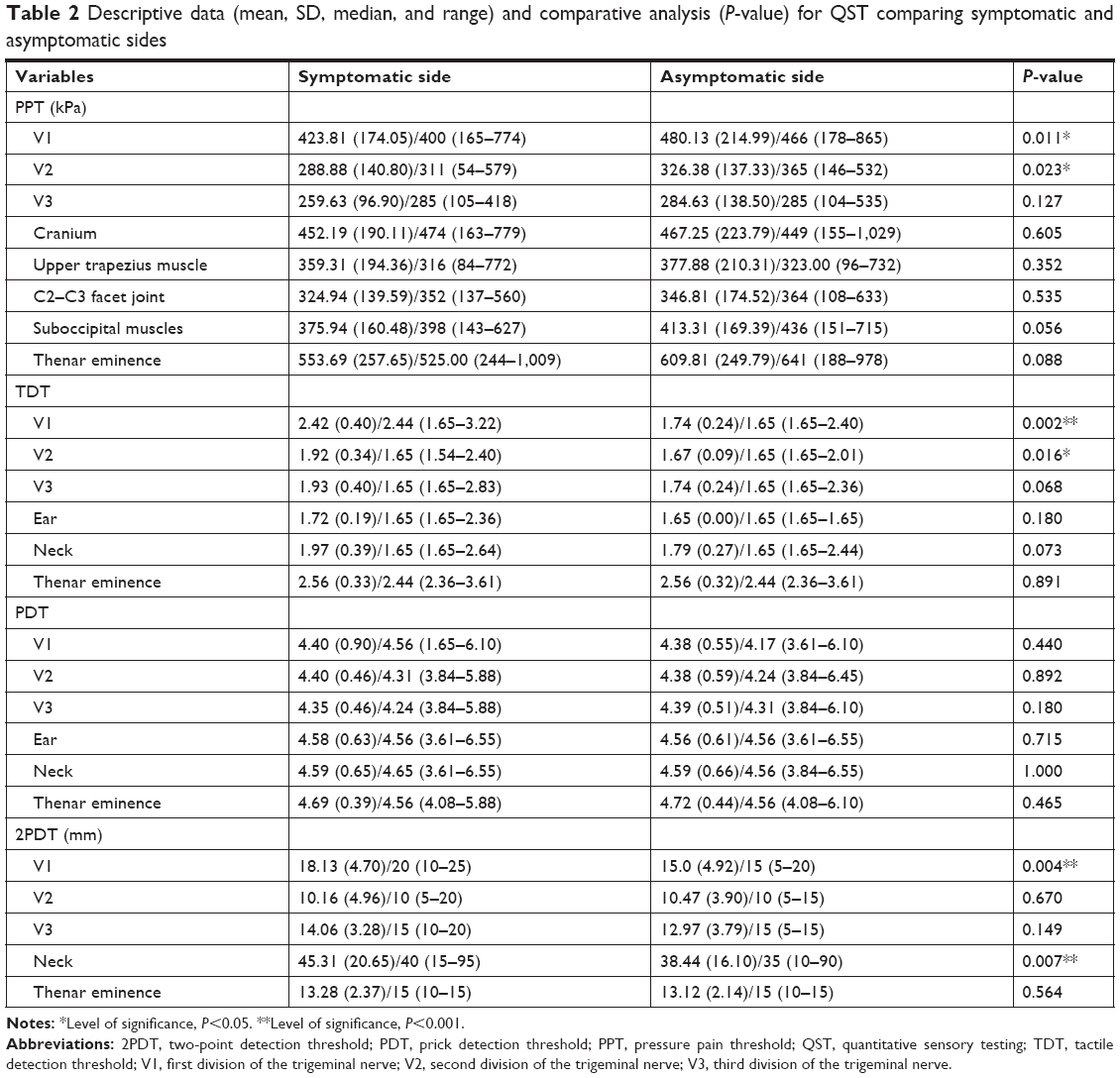 | Table 2 Descriptive data (mean, SD, median, and range) and comparative analysis (P-value) for QST comparing symptomatic and asymptomatic sides |
Tables 3 and 4 summarize the mechanical sensory thresholds in the symptomatic side of patients depending on the presence of symptoms in V2 and V3 areas, respectively. The only statistically significant difference found was a higher PPT in the cranium of patients who did not present any symptoms (656.00 kPa [SD=92.86]) in the V2 region compared to those who had symptoms (420.40 kPa [SD=185.93]) or shadows (358.43 kPa [SD=155.59]) in V2 (P=0.034).
 | Table 3 Descriptive data (mean, SD, median, and range) and comparative analysis (P-value) for QST in the symptomatic side comparing patients without symptoms in V2, with shadows in V2, and with symptoms in V2 |
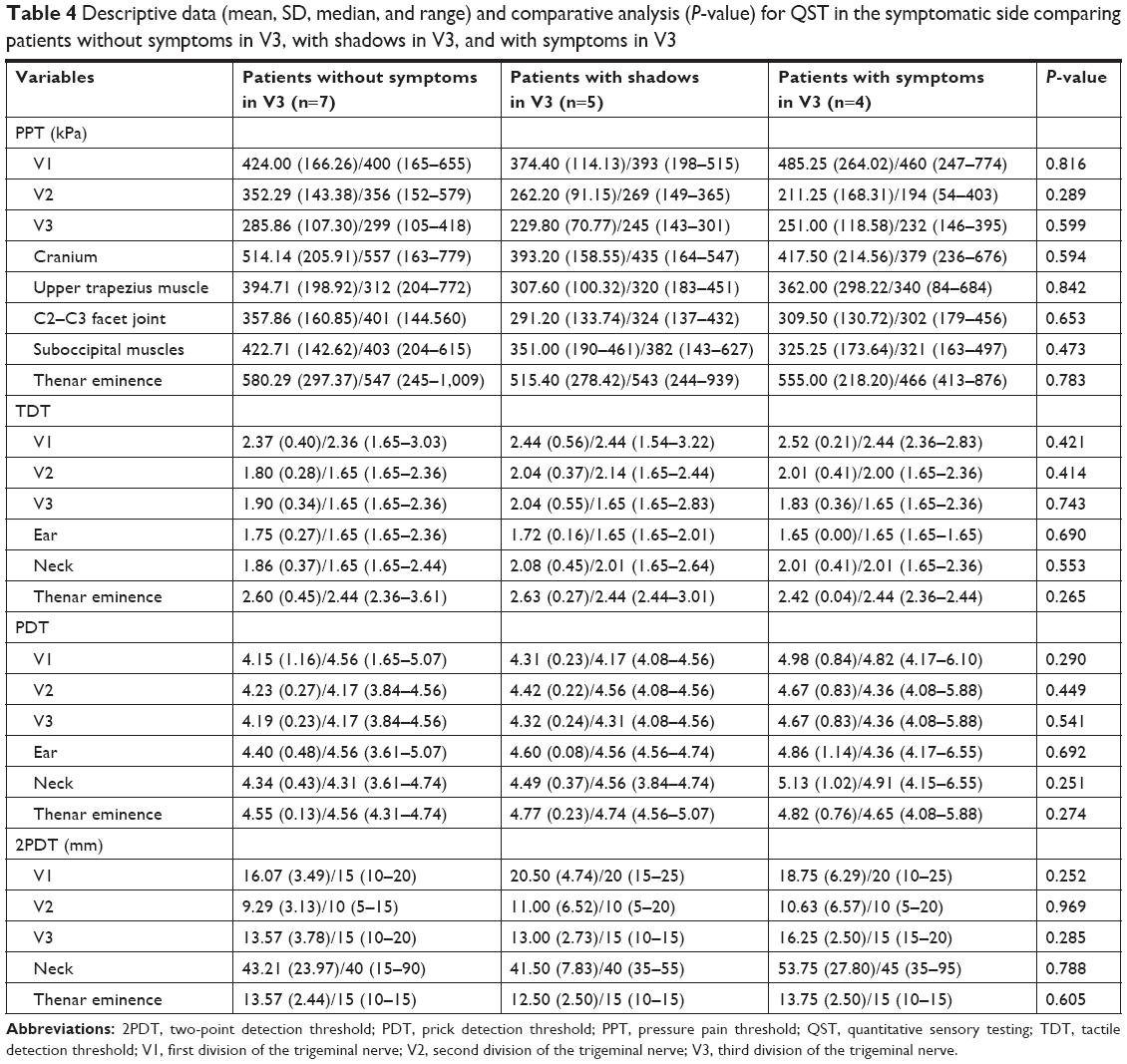 | Table 4 Descriptive data (mean, SD, median, and range) and comparative analysis (P-value) for QST in the symptomatic side comparing patients without symptoms in V3, with shadows in V3, and with symptoms in V3 |
No statistically significant correlation of clinical relevance was found between the variables of interest: mechanical sensory thresholds (PPT, TDT, PDT, and 2PDT), demographic and clinical data (age, gender, height, weight, and characteristics of CH).
Discussion
Altered mechanical sensory thresholds were found in the symptomatic side compared to the asymptomatic side of CH patients, with decreased PPT in V1 and V2, increased TDT in V1 and V2, and 2PDT in V1 and neck. Our results reflect lateralized pathological variation in the trigeminocervical system in CH patients.
The characteristics of our sample are similar to those in the previous literature. Previous demographic studies have reported that CH is more prevalent in men than women with ratios ranging from 1.3:1 to 7:1.26,27 As in our sample, episodic CH is more common than chronic CH.28 Regarding pain location, right-sided pain has been shown to be predominant in CH in previous studies with the distribution of the first division of the trigeminal nerve being the most frequent, followed by the second and third divisions as in our sample.26,27
Although it has been proposed that CH may only affect certain aspects of sensory function following a specific pattern, previous evidence studying specific changes in mechanical sensory function has offered conflicting results.8 The results of the present study indicate that patients with CH evidence mechanical sensory alterations in the symptomatic side compared to the asymptomatic side. A significant reduction in PPT was evidenced in V1 (P=0.011) and V2 areas (P=0.023) in the symptomatic side compared to the asymptomatic side in CH patients. These results support previous evidence of Ellrich et al11 and Coppola et al17 indicating a reduction in PPT in the symptomatic side compared to the asymptomatic side of 25 and 18 CH patients, respectively. However, Ladda et al19 found bilaterally increased thresholds in 16 CH patients, with no side influence, and not restricted to the trigeminal innervation, but were also on the back of the hands. Regarding TDT, the present study found higher values in V1 (P=0.002) and V2 (P=0.016) of the symptomatic side, indicating features of hypoesthesia in the symptomatic regions of V1 and V2. In the same line, Ashkenaz and Young18 evidenced mechanical sensory alterations in six out of 10 patients with CH, but found no evidence of specific mechanical sensory disturbances in the symptomatic side compared to the asymptomatic side. Ladda et al19 found no differences between the symptomatic and asymptomatic sides. Nevertheless, test sites evaluated by Ladda et al19 are limited to the cheek (V2) and the back of the hands, but V1 area was not evaluated. According to the pain distribution in patients with CH, the evaluation of sensory function of the territory innervated by V1 may be of greater clinical value. The absence of significant differences between the symptomatic and asymptomatic side in PDT in our study supports the results of Ashkenaz and Young.18 This lack of differences may reflect the specificity of pathophysiological changes in CH, which would not affect the nerve fibers examined with PDT. Finally, regarding 2PDT, according to our knowledge, this is the first study to evaluate 2PDT in CH population. The results indicate higher 2PDT in V1 (P=0.004) and neck (P=0.007), which may reflect a decrease in the density of tactile receptors in these symptomatic regions, or even an alteration in some level of sensory processing. In any case, these results have to be contrasted with future research.
The examination of sensory function in patients with CH may be a very useful clinical tool. Baseline deficits of mechanical sensory function support a subclinical neuropathy that have previously been demonstrated to be predictive of poor prognosis in different clinical subgroups including CH.11 This could allow to detect those patients who are going to become chronic before it happens with the purpose of taking preventive measures.
The most commonly reported location of CH is under the distribution of V1, mostly occurring behind the eye, in the periorbital region or in the temple. Areas related to V2 or V3 are less frequent.26,27 Mechanical sensitivity patterns of patients with symptoms, shadows or without symptoms in V2 and V3, respectively, were compared. Despite the staggered tendency in patients with symptoms and shadows in V2 and V3 to present lower PPT and higher DTT, especially in that region, when compared to patients with asymptomatic V2 and V3 regions, statistical significance was not reached except for PPT in the cranium (P=0.034). It is possible that the important tendency to evidence lower PPT and higher DTT in the specific symptomatic (or shadows) area did not reach statistical significance due to the small sample size of each subgroup. To the best of our knowledge, this is the first study that addresses this issue. Larger studies can perhaps be powered to detect subtle changes in mechanical sensory function depending on the specific symptomatic area. Previous studies have also evidenced that sensory alterations also seem to be determined by the temporal profile of the headache.29,30 Future studies should take into account not only the location of pain but also the intensity and temporal profile of the headache in CH patients.
Previous studies that had found bilateral mechanical sensory alterations not restricted to the territory of the trigeminal innervation suggested that a central process is responsible for these changes.19 The results of the present study, where specific mechanical sensory changes have been found in the symptomatic side compared to the asymptomatic side, are interpreted as a sign of secondary sensitization of pain-processing second-order neurons within the trigeminocervical nucleus.29 The role of the trigeminal nerve in CH is indicated both by the increased concentrations of calcitonin gene-related peptide in the ipsilateral jugular vein during attacks and by the pain improvement after surgical lesioning of this nerve.7,31 Nevertheless, although trigeminal system activation is necessary for a CH attack, it is not sufficient on its own to produce CH.32 The evidence regarding the debate about peripheral vs central origin of pain in CH indicates that the central component plays a major part in generating the pain.4 Neuroimaging studies have confirmed the hypothalamic involvement in CH and have prompted the suggestion that the posterior hypothalamus was the CH generator.5 Evidence shows that the hypothalamus affects craniofacial region through an activation of the trigeminal system by a direct two-way connection between the posterior hypothalamus and the trigeminocervical nucleus through trigeminohypothalamic tract.33,34
Nevertheless, the current evidence shows that, although the hypothalamus is a key area for the pathophysiology of primary CH, we should probably move beyond thinking in terms of a single trigger zone and consider a hypothalamic activation of the pain matrix, involving cognitive, affective, and autonomic functions.4
This study had several limitations. First, the study lacked diagnostic validation. Even though all study participants had a clinical diagnosis of CH by a neurologist, specialists can still mistake one TAC for another. Second, clinical features were collected retrospectively compared to prospective data collection using headache diaries. For the survey questions, an inherent recall bias may have potentially occurred. Nevertheless, CH is a severe and excruciating headache disorder making difficult not to correctly remember episodes. In addition, some participants usually kept a record of their CH attacks in a headache diary. Moreover, QST was performed to quantitatively measure mechanical sensory function, but we must be aware that QST is a quasi-objective measurement, combining objective measures with patient reports of sensory detection. This subjective component involves a risk of respondent bias. In any case, QST is a noninvasive psychophysiological test that can be used in a clinical setting to quantify neurological function of both small- and large-fiber nerves.14 Unlike excitability studies, QST assesses small-fiber function as well to better capture symptoms such as pain.35 Furthermore, QST allows the measurement of subclinical neurological changes early on to identify patients most likely to become chronic sufferers.11 Finally, the relatively small sample size limits the generalizability of the results. Larger studies are needed to validate these findings.
Conclusion
This study is the first to investigate mechanical sensory function in CH patients throughout the entire craniofacial region: in the three divisions of the trigeminal nerve (V1, V2, and V3), neck (superficial cervical plexus), and ear (trigeminal and facial nerves), including a control region (hand). The results of the present study showed decreased PPT and increased TDT in V1 and V2 of the symptomatic side associated with increased 2PDT in V1 and neck of the symptomatic side, supporting prior evidence that suggested a specific pattern of alteration of mechanical sensory function.
This study is the first attempt to evaluate specific mechanical sensory changes in the symptomatic side depending on the symptomatic area in a sample of CH patients. Despite the tendency in patients with symptoms and shadows in V2 and V3 to present lower PPT and higher DTT compared to patients with asymptomatic V2 and V3 regions, statistical significance was not reached. Future studies with larger samples are needed to further elucidate this issue.
Clinical implications
- Sensory changes have been shown to be associated with poor prognosis in different pain conditions including CH.
- QST is a valid and reliable tool to evaluate somatosensory function and is useful in characterizing patients with CH.
- CH patients evidence altered mechanical sensory thresholds in the symptomatic side compared to the asymptomatic side.
- Somatosensory alterations indicate a lateralized pathological variation in the trigeminocervical system in CH patients.
Acknowledgment
Marjan Jahanshahi is now affiliated with The Clinical Hospital of Chengdu Brain Science Institute, MOE Key Lab for Neuroinformation, University of Electronic Science and Technology of China, Chengdu, China, as a visiting professor.
Disclosure
The authors report no conflicts of interest in this work.
References
Headache Classification Committee of the International Headache Society (IHS). The International classification of headache disorders, 3rd edition (beta version). Cephalalgia. 2013;33(9):629–808. | ||
Fischera M, Marziniak M, Gralow I, Evers S. The incidence and prevalence of cluster headache: a meta-analysis of population-based studies. Cephalalgia. 2008;28(6):614–618. | ||
Goadsby PJ. Pathophysiology of cluster headache: a trigeminal autonomic cephalgia. Lancet Neurol. 2002;1(4):251–257. | ||
Leone M, Bussone G. A review of hormonal findings in cluster headache. Evidence for hypothalamic involvement. Cephalalgia. 1993;13(5):309–317. | ||
May A, Bahra A, Büchel C, Frackowiak RS, Goadsby PJ. Hypothalamic activation in cluster headache attacks. Lancet. 1998;352(9124):275–278. | ||
Holle D, Obermann M. Cluster headache and the hypothalamus: causal relationship or epiphenomenon? Expert Rev Neurother. 2011;11(9):1255–1263. | ||
Goadsby PJ, Edvinsson L. Human in vivo evidence for trigeminovascular activation in cluster headache. Neuropeptide changes and effects of acute attacks therapies. Brain. 1994;117:427–434. | ||
Jürgens TP, Leone M, Proietti-Cecchini A, et al. Hypothalamic deep-brain stimulation modulates thermal sensitivity and pain thresholds in cluster headache. Pain. 2009;146(1–2):84–90. | ||
Hoskin KL, Zagami AS, Goadsby PJ. Stimulation of the middle meningeal artery leads to Fos expression in the trigeminocervical nucleus: a comparative study of monkey and cat. J Anat. 1999;194:579–588. | ||
Curatolo M, Petersen-Felix S, Arendt-Nielsen L, Giani C, Zbinden AM, Radanov BP. Central hypersensitivity in chronic pain after whiplash injury. Clin J Pain. 2001;17(4):306–315. | ||
Ellrich J, Ristic D, Yekta SS. Impaired thermal perception in cluster headache. J Neurol. 2006;253(10):1292–1299. | ||
Mainardi F, Trucco M, Maggioni F. A comprehensive reappraisal. Cephalalgia. 2010;30(4):399–412. | ||
Mijajlović MD, Aleksić VM, Covičković Šternić NM. Cluster headache as a first manifestation of multiple sclerosis: case report and literature review. Neuropsychiatr Dis Treat. 2014;10:2269–2274. | ||
Rolke R, Magerl W, Campbell KA, et al. Quantitative sensory testing: a comprehensive protocol for clinical trials. Eur J Pain. 2006;10(1):77–88. | ||
Schytz HW, Olesen J. Laboratory tests of headache disorders – dawn of a new era? Cephalalgia. 2016;36(13):1268–1290. | ||
Kim HK, Kim KS, Kim ME. Thermal perception as a key factor for assessing effects of trigeminal nerve injury. J Oral Facial Pain Headache. 2017;31(2):129–138. | ||
Coppola G, di Lorenzo C, Bracaglia M, et al. Lateralized nociceptive blink reflex habituation deficit in episodic cluster headache: Correlations with clinical features. Cephalalgia. 2015;35(7):600–607. | ||
Ashkenazi A, Young WB. Dynamic mechanical (brush) allodynia in cluster headache. Headache. 2004;44(10):1010–1012. | ||
Ladda J, Straube A, Förderreuther S, Krause P, Eggert T. Quantitative sensory testing in cluster headache: increased sensory thresholds. Cephalalgia. 2006;26(9):1043–1050. | ||
Komiyama O, de Laat A. Tactile and pain thresholds in the intra- and extra-oral regions of symptom-free subjects. Pain. 2005;115(3):308–315. | ||
Komiyama O, Obara R, Iida T, et al. Influence of age and gender on trigeminal sensory function and magnetically evoked masseteric exteroceptive suppression reflex. Arch Oral Biol. 2012;57(7):995–1002. | ||
Sterling M, Treleaven J, Jull G. Responses to a clinical test of mechanical provocation of nerve tissue in whiplash associated disorder. Man Ther. 2002;7(2):89–94. | ||
Moseley GL. I can’t find it! Distorted body image and tactile dysfunction in patients with chronic back pain. Pain. 2008;140(1):239–243. | ||
Vriens JP, van der Glas HW. Extension of normal values on sensory function for facial areas using clinical tests on touch and two-point discrimination. Int J Oral Maxillofac Surg. 2009;38(11):1154–1158. | ||
Vriens JP, van der Glas HW. The relationship of facial two-point discrimination to applied force under clinical test conditions. Plast Reconstr Surg. 2002;109(3):943–952. | ||
Rozen TD, Fishman RS. Cluster headache in the United States of America: demographics, clinical characteristics, triggers, suicidality, and personal burden. Headache. 2012;52(1):99–113. | ||
Dong Z, di H, Dai W, et al. Clinical profile of cluster headaches in China – a clinic-based study. J Headache Pain. 2013;14(1):27. | ||
Mitsikostas DD, Edvinsson L, Jensen RH, et al. Refractory chronic cluster headache: a consensus statement on clinical definition from the European Headache Federation. J Headache Pain. 2014;15:79. | ||
Burstein R, Yarnitsky D, Goor-Aryeh I, Ransil BJ, Bajwa ZH. An association between migraine and cutaneous allodynia. Ann Neurol. 2000;47(5):614–624. | ||
Rozen TD, Haynes GV, Saper JR, Sheftell FD. Abrupt onset and termination of cutaneous allodynia (central sensitization) during attacks of SUNCT. Headache. 2005;45(2):153–155. | ||
Sprenger T, Valet M, Platzer S, Pfaffenrath V, Steude U, Tolle TR. SUNCT: bilateral hypothalamic activation during headache attacks and resolving of symptoms after trigeminal decompression. Pain. 2005;113(3):422–426. | ||
May A, Leone M, Boecker H, et al. Hypothalamic deep brain stimulation in positron emission tomography. J Neurosci. 2006;26(13):3589–3593. | ||
Bartsch T, Levy MJ, Knight YE, Goadsby PJ. Differential modulation of nociceptive dural input to [hypocretin] orexin A and B receptor activation in the posterior hypothalamic area. Pain. 2004;109(3):367–378. | ||
Malick A, Strassman RM, Burstein R. Trigeminohypothalamic and reticulohypothalamic tract neurons in the upper cervical spinal cord and caudal medulla of the rat. J Neurophysiol. 2000;84(4):2078–2112. | ||
Krøigård T, Schrøder HD, Qvortrup C, et al. Characterization and diagnostic evaluation of chronic polyneuropathies induced by oxaliplatin and docetaxel comparing skin biopsy to quantitative sensory testing and nerve conduction studies. Eur J Neurol. 2014;21(4):623–629. |
 © 2018 The Author(s). This work is published and licensed by Dove Medical Press Limited. The
full terms of this license are available at https://www.dovepress.com/terms
and incorporate the Creative Commons Attribution
- Non Commercial (unported, 3.0) License.
By accessing the work you hereby accept the Terms. Non-commercial uses of the work are permitted
without any further permission from Dove Medical Press Limited, provided the work is properly
attributed. For permission for commercial use of this work, please see paragraphs 4.2 and 5 of our Terms.
© 2018 The Author(s). This work is published and licensed by Dove Medical Press Limited. The
full terms of this license are available at https://www.dovepress.com/terms
and incorporate the Creative Commons Attribution
- Non Commercial (unported, 3.0) License.
By accessing the work you hereby accept the Terms. Non-commercial uses of the work are permitted
without any further permission from Dove Medical Press Limited, provided the work is properly
attributed. For permission for commercial use of this work, please see paragraphs 4.2 and 5 of our Terms.