Back to Journals » Clinical, Cosmetic and Investigational Dentistry » Volume 12
Self-Reported Oral Health Attitudes and Behaviors, and Gingival Status of Dental Students
Authors Karem Hassan B ![]() , Jabbar Ali B
, Jabbar Ali B ![]() , Mahmood Alwan A, Badeia RA
, Mahmood Alwan A, Badeia RA ![]()
Received 13 February 2020
Accepted for publication 21 May 2020
Published 25 June 2020 Volume 2020:12 Pages 225—232
DOI https://doi.org/10.2147/CCIDE.S249708
Checked for plagiarism Yes
Review by Single anonymous peer review
Peer reviewer comments 2
Editor who approved publication: Professor Christopher E. Okunseri
Ban Karem Hassan, Banaz Jabbar Ali, Alyamama Mahmood Alwan, Raed A Badeia
Department of Periodontal Dentistry, College of Dentistry, University of Mustansiriyah, Baghdad, Iraq
Correspondence: Banaz Jabbar Ali Email [email protected]
Aim: The aim of this study was to assess self-reported oral health attitudes and behaviors of the Iraqi dental students and compare the variations in these attitudes and behaviors that linked to dental education level and gender.
Materials and Methods: A self-administered questionnaire depended on the English version of the Hiroshima University Dental Behavioral Inventory (HU-DBI) was prepared, the questionnaire given to 198 dental students.
Results: About 91.4% of the dental students were worried about the teeth colour, and merely minor percentage of them (18.8%) thought it is not crucial to seek dental advice until they acquire a tooth pain; however, 26.3% of the students were disturbed because of their gum colour, and 75.3% of them examined their teeth after brushing. Besides, 72.2% of the students replied that gum disease could not be prevented by tooth brushing only, 60.1% of the students do not give visiting the dentist such concern, and 14.1% of dental students were smokers. The plaque and gingival indices were significantly higher in preclinical students than clinical students.
Conclusion: Iraqi dental students had somewhat good oral health behavior and attitudes; however, extra concentrating is required on the anticipatory and behavioral aspects of oral self-care practices. Female dental students displayed better oral health behavior and attitudes than male colleagues on some issues.
Keywords: periodontal health, dental students, self-reported, gingival index, Hiroshima University Dental Behavioral Inventory
Introduction
A healthy mouth is a unique and incomparable wealth; it is considered an essential human right to sustain a good oral condition.1 From the highly prevalent chronic oral disease in adults, is the chronic periodontal disease in which greater than 50% of people over all the world are affected by its prevalence.2
Periodontal disease is significantly associated with the cause of numerous systemic diseases like cardiovascular disease and diabetes mellitus. Therefore it is of ultimate general health concern.3 There is a new appreciation that for the best health facility to be supplied to the population, it’s crucial to provide motivated and trained staff.4 As the dental students are the prospective health professionals, retaining precise oral health awareness and behavior during school years anticipated from them. Simultaneously, their oral health condition impacted their specific health and lifestyle along with its reflection on their oral health attitude and behavior, is notably crucial.5
Kawamura established that, the Hiroshima University-Dental Behavioral Inventory (HU-DBI) which is a questionnaire to recognize patients’ oral health awareness.6 Initially, the Japanese printed the HU-DBI and after that interpreted into English and established to achieve adequate test-retest reliability and paraphrase validity.7 Oral health attitudes and behaviors altered at the preclinical period when compared with the clinical years of training, as shown by research on dental students,8,9 also different between cultures and countries.10,12 Furthermore, these are different among the students following diverse practicing curriculums in dentistry, dental health, dental technician and pharmacy.13,14
With the development in dental school, some parts of dental students’ oral health consciousness and attitudes get developed, as established by recent study used the modified Hiroshima University-Dental Behavioral Inventory.15–17
There is a universal tendency concerning the regulation of dental education and the involvement of health establishment in dentistry. Comparative studies will be imperative in determining dental students’ oral health behaviors and attitudes in different cultures and various educational and health care systems.18,19 Slight is recognized concerning the oral health behaviors and attitudes of Iraqi dental students, along with the effect of educational training on the advance of their oral behaviors and attitudes. Therefore, the current study intended to estimate self-reported oral health attitudes and behavior in Iraqi dental students, to determine the effect of dental education on dental students’ health attitudes, oral sanitation, and gingival status. Moreover, to compare the alterations in oral health attitude among male and female dental students and to evaluate if the self-reported periodontal health is interrelated with clinically evaluated periodontal status. Depending on the outcomes of this study, alterations may be proposed to develop the dental education program.
Materials and Methods
The study was carried out at the college of dentistry/Mustansiriyah University using the modified English-language version of the HU-DBI Questionnaire15 comprising 18 questions (Appendix 1) in dichotomous response format (agree/disagree), which was organized and given to dental students of the academic year 2017–2018. Additional data regarding members’ age, gender, as well as education grade, gathered from dental students. Ethical committee agreement and the dean permission of college of dentistry/Mustansiriyah University were acquired with no subjective data from a participant was taken. A summary of the purpose of the research, procedures and the nature of the questions was explained, and the students who approve to participate in the study were asked to fill in the questionnaire which considered as an agreement to take part in the research.
Sample Size
This study incorporated (198) volunteers dental students aged between (18–24) years old. Inclusion criteria involved all systemically healthy dental students willing to partake in the research and answer the questionnaire and undergo the clinical examination. The exclusion criteria included students who did not want to join the study or did not have the time or completed the questionnaire but did not complete the clinical examination as well as those with orthodontic treatment. The students distributed into the preclinical group (which was the first three years of dental education) and the clinical group (the last two years). The preclinical group involved 98 students, while the clinical group involved 100 students. The instruction was given to the participant to inquire if they had any questions concerning filling up the questionnaires. (Appendix 1)
Periodontal Examination
The examiner assessed periodontal health parameters of students after they finished filling the self-reported periodontal questionnaire on dental chair in a semi-supine position using dental light and in a dry field by using a sterilized examination kit (mouth mirrors and standardized periodontal probes with Williams’s markings). The examiner who accomplished the periodontal examination blinded to the reactions of participants on the self-reported questionnaire. The evaluation of oral hygiene and the periodontal status of all teeth, excluding third molars, used plaque index (PLI) of Löe,20 and gingival indexes (GI) of Löe and Silness.21 The measurement of the parameters was at four sites (mesial, facial, distal, and lingual) per tooth. The data documented by a specific examination formula. (Appendix II)
Data Analysis
The data analyzed with SPSS version 23, statistical descriptive done by the mean, standard deviation (SD), and percent. The questionnaire showed good test reliability (Cronbach’s alpha score, 0.72).
Each of the questions analyzed with the chi-square test of the clinical and preclinical stage, and in gender, the parametric Student’s T-test used to compared the two independent groups for plaque, gingival index, and age.
Result
A total of 198 dental students participated in the study and divided into preclinical 98 and clinical 100 students with a mean age of (21.06 ±1.57). The percentages of “yes and no” responses for all dental student participated in the study and for the preclinical and clinical stages are shown in Table 1. Out of 18 questions, 14 questions showed no significant differences in distribution between clinical and preclinical groups. The significant differences observed in 4 items; (Q7), (Q8), (Q13), and (Q17). Among all the participants (198), there were 80 (40.4%) males and 118 (59.6%) females. Percentages of “yes and no” responses according to the gender shown in (Table 2). Statistically significant differences in distribution were found only for items (15) and (16).
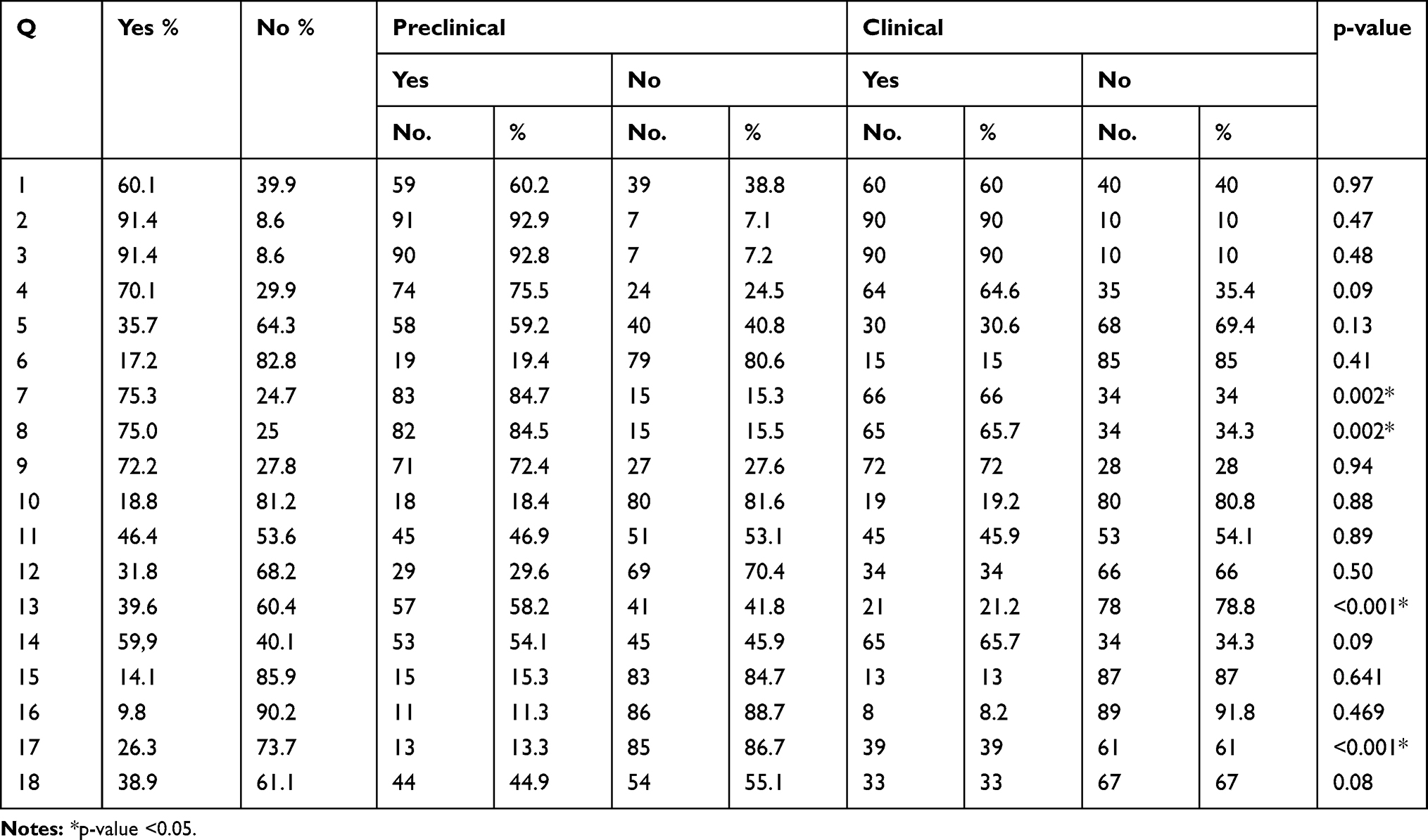 |
Table 1 The Percentages and Analysis of “Yes” and “No” Responses According to the Preclinical and Clinical Stage |
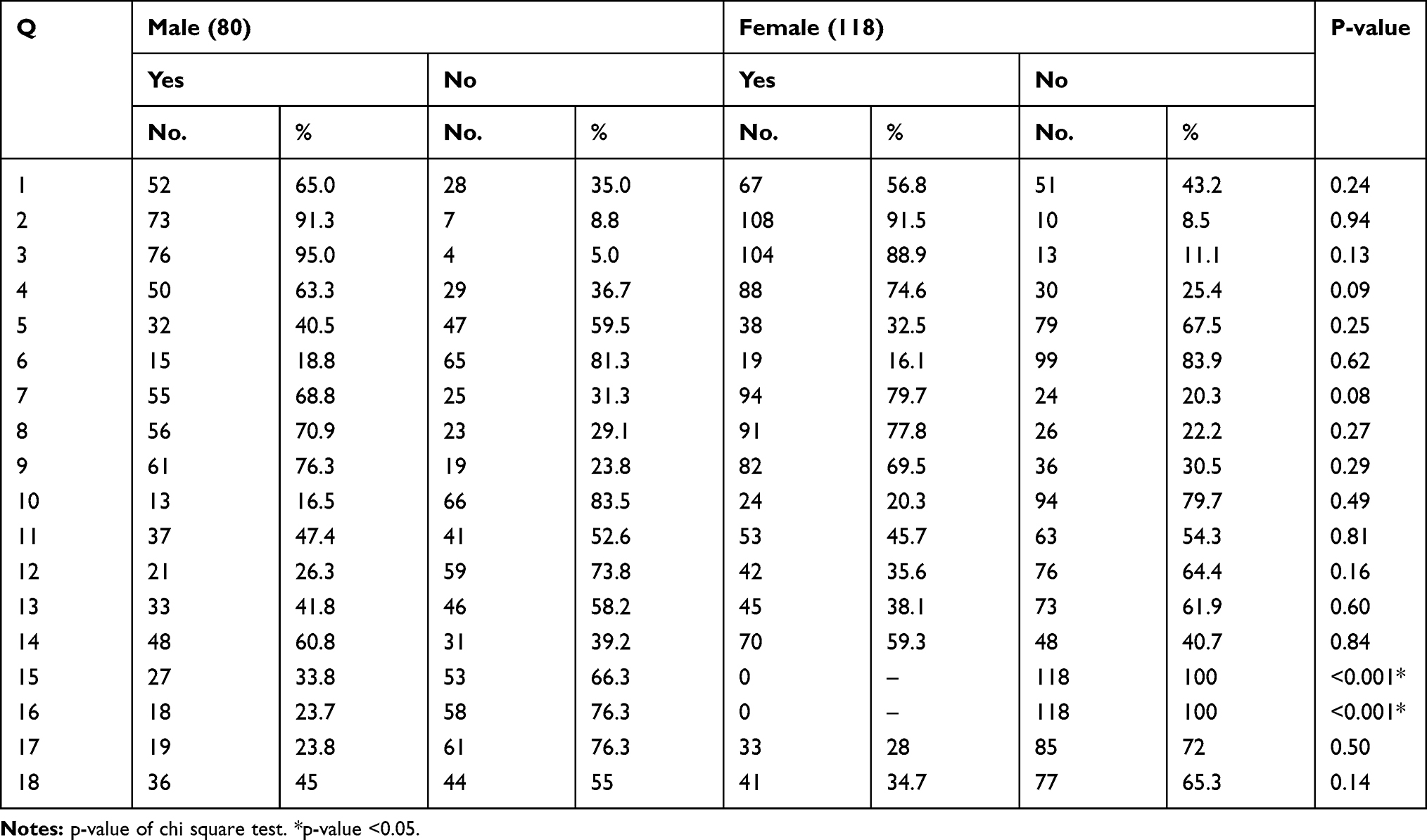 |
Table 2 Percentages of “Yes and No” Responses According to Gender |
Higher plaque (PLI) and gingival (GI) indices were found in male students and according to the parametric Student’s t-test. Statistically, the non-significant difference was found between the PLI of males and females (p=0.078), while for the gingival index, the difference was statistically significant, as shown in Table 3. According to the T-test, the comparison of mean values of plaque and gingival index between preclinical and clinical students shows a statistically significant difference between them (p<0.05), as shown in Table 4.
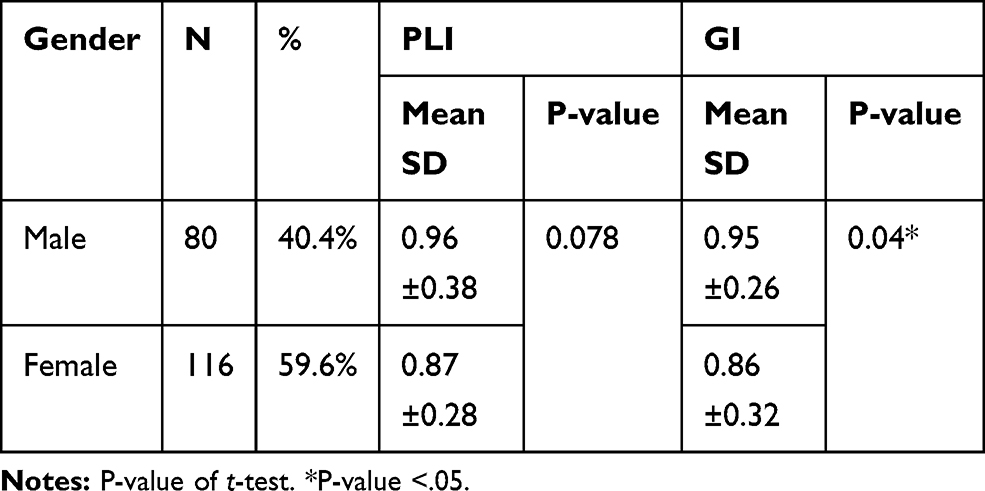 |
Table 3 Plaque and Gingival Index for Male and Female |
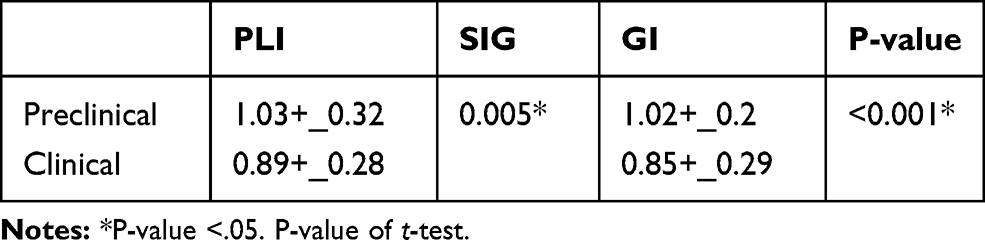 |
Table 4 Plaque and Gingival Index of Preclinical and Clinical Student |
Table 5 shows the analysis of PLI and GI index between clinical and preclinical, which respond “yes” for the four items (Q3) (Q7) (Q17) and (Q18). A higher percentage of dental students of two groups, without significant difference between them, confirmed that they had noticed some sticky deposits on their teeth. Still, when we compared the plaque index and GI, we found a high score in preclinical than the clinical student with a significant difference.
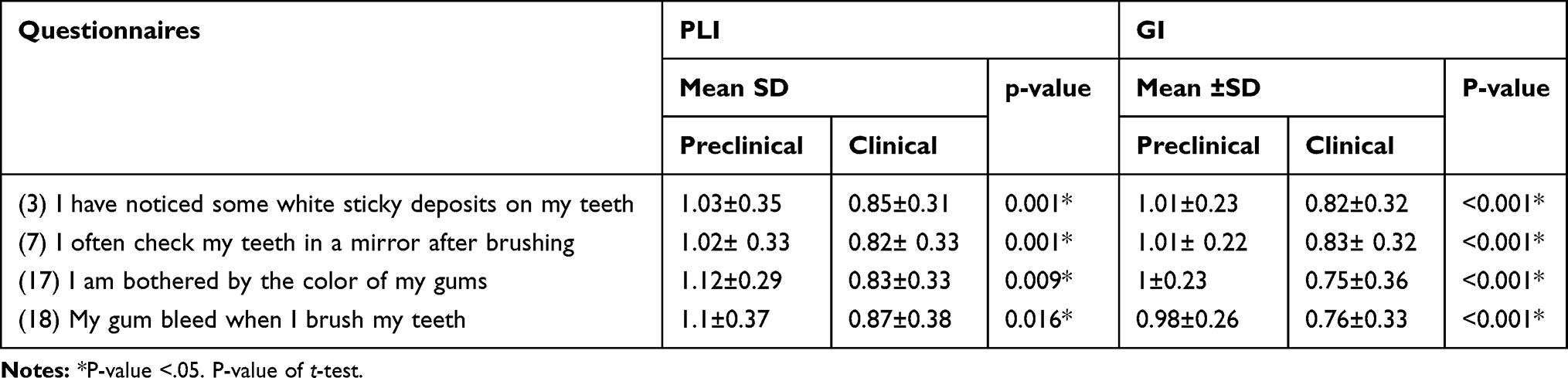 |
Table 5 Analysis of PLI and GI Index with “Yes” Response for the Items (3, 7, 17 and 18) in Clinical and Preclinical Students |
Also, 84.7% of preclinical students said that they often checked their teeth in a mirror after brushing, and 66% of clinical students agreed with this statement (p=0.002). In contrast, when we checked the plaque and the gingival index of them we found, the higher PLI and GI was found in preclinical student with a highly significant difference between them. About 39% of clinical students worried about the colour of their gum compared to (13.3%) for the preclinical student, with a highly significant difference (p=0.000), and the higher PL and GI index found in the preclinical group.
About (44.9%) of preclinical student reported that their gum bleed when brush while the percentage less than for clinical student (33%), the PLI and GI index was higher in preclinical students than clinical with a statistically significant difference between them (P<0.05), as shown in Table 5.
Discussion
From the imperative responsibilities of oral health providers, instructing the patients about the precise oral habits, and raising their consciousness on how to avoid oral diseases. As dental students are the prospective health professionals, so it is crucial that students posse a correct approach concerning their oral hygiene. This study focused on the oral and periodontal health of Iraqi dental students throughout their educational period along with the degree to which the understanding earned redirected toward their own oral and periodontal health. The result revealed that 60.1% of the students do not worry much regarding visiting the dentist, and this was lower than Indian (70.6%)22 and Turkish (81.3%)23 dental students and higher than Croatian students (23.5%).24 Furthermore, 72.2% of the students replied that it is impossible to avoid gingival disease by toothbrushing alone which was the higher proportion in comparison to Indian (58.9%) and Turkish (67.4%) students.22,23 This high proportion perhaps attributable to that they did not have the understanding of the significance of the mechanical elimination of dental plaque and the secondary role of the toothpaste.25
The result estimated that about 91.4% of the dental students were worried about the teeth colour as compared to 84% of dental students in India and 67% of Jordanian dental students.26 Similarly, it established that merely a minor percentage of the dental students (18.8%) reported that they postponed visiting the dentist till their teeth hurt them. However, in a study on Indian dental students, the percentage was 68%.16 Komabayashi et al11 in previous cross-cultural studies noted that 18% of the British and 77% of the Chinese students were disturbed from their gum colour, and 72% of the British and 32% of the Chinese dental students were checking their teeth after brushing. In the current study, for the same items (Items 17 and 7), the percent for the Iraqi dental students was 26.3% and 75.3%, respectively. This result showed that the students in this study gave good attention to their oral hygiene maintenance and were as well much worried regarding their esthetics.
Around 38.9% of dental students in the current study revealed bleeding gingiva after brushing, and this was greater than dental students in India (14%)16 and Japanese (25%) dental students and lesser than Finnish dental students (45%).10 59.9% of the students were pleased with the look of their teeth, and this was in agreement with the percentage (58%) observed in both Indian and Turkish students.16,17 About 31.8% of the students consumed dental floss frequently, and this was greater than the percentage stated by a study on Indian dental student (16%) and 75% of dental students concerned about having oral halitosis which was in agreement with the Indian (76%) dental student16 and greater than Jordanian (60%)26 and Turkish (45.1%) students.23 Dentists have vital role models for their patients, and those consuming tobacco probably are less likely to advise their patients to give up. In the current study, only 14.1% of dental students were smokers. Comparable smoking rates found among Jordanians (17.2 %) and Saudi Arabia (17%), dental students.27,28 Nevertheless, the result was lesser than Turkish (26%), Bangladesh (22%), Holland (24%), and Norway (24%) dental students.17,29,30
About 9.8% of the Iraqi dental student revealed that they smoke more than ten cigarettes per day in comparison to 15.6% of Turkish dental students.15 The result of our study shown that 91.4% of the students approve to item 3 (I have noticed some white sticky deposits on my teeth), and this percentage was greater than Indian (9.6%)16 and Turkish (58.0%).15 About 39.6% of the students consumed mouth rinse regularly in comparison to 54.8% of the Indian16 and Turkish (13.7%) students,15 and this specifies good consciousness of the adjunctive role of mouthwash to mechanical plaque elimination and the probable unwanted consequence of long term mouthwash use. In India, around 30.2% of the dental students informed that they do not have learned the professional way of brushing, and 38.3% of them informed that their dentist told them they brush very well.22 Nevertheless, in the current study, the percentage was 35.7% and 46.4% correspondingly. 59.2%of preclinical students approved that they had never learned the professional way of brushing, this due to to the fact that they do not receive any information regarding teeth cleaning methods and oral hygiene preservation measures until the fourth stage (first clinical year). Whereas for clinical students, the proportion was 30.6%, and this may be as they deduced this inquiry that they had never been taught by their dentists in their subjective dental visit, as all of them had had lectures and practice on oral hygiene. The consequence of our study indicated that 70.1% of the students concerned that my teeth are getting poorer despite day-to-day brushing in comparison to 26.6% of Indian students.22 A significant difference established between preclinical and clinical students for the plaque and gingival indices. Higher indices estimated in the preclinical group that points to better oral hygiene in clinical group dental students. This result attributed to the fact that the periodontology course begins earlier in the fourth stage (first clinical year) for the clinical group dental students. The course gives strong importance on plaque control methods, tooth brushing procedures, and ways to control the effectiveness of tooth brushing. These results established that oral health attitudes and behavior enhanced with an accumulative education degree.2,13 A comparable consequence observed by Shah et al in which the comparison of plaque index presented a significant difference between the first and the final year BDS (Bachelor of Dental Surgery) students.31 Whereas, Lalani et al, established a non-significant difference in the plaque and gingival indices between third and final year dental students.32
The extensive recommendation to prevent periodontal diseases is to floss teeth regularly.33 Our results discovered that 34% of clinical and 29.6% of preclinical students regularly used dental floss. Even though in Turkish dental students, the percentages were 31% in clinical and 19% in preclinical students.17 Although, the clinical students were marginally better than preclinical students; however, both of them should have further learning regarding the impotence of flossing frequently. As the dental students proceeded through the syllabus, a variable positive attitude and behaviors were perceived, and the clinical group students being more improved than the preclinical group students in some points of the questionnaire even though the difference was statistically non-significant. Numerous studies have stated that: as the level of education rises, dental health attitudes get more helpful and are enhanced.10,13,16
The positive behavior of the clinical students reflected by a better response in items (4, 5, 12, 14, and 18). Similarly, the clinical students exhibited significantly superior responses regarding item 13, and the comparable result established among Sudanese Dental Students.34 Conversely, the clinical students displayed comparable outcomes to the preclinical students regarding items 1, 2, 3, 9, 10 and 11. The result for item15 and item 16 was fairly near in preclinical and clinical students with a somewhat improved response in the clinical group. Entertainingly, the preclinical students had extra concern than the clinical students with item 7 and item 8 which was similar to the result instituted in studies on dental students in Istanbul (Turkey)23 and Sudan34 and this attributable to the fact that the clinical students had much information to conquer the previous concern than the preclinical students.34
Even though some thoughts might have proposed that students’ qualifications might influence their oral health attitude irrespective of the acquaintance they had earned, Khami et al,35 stated that “Education and training in preventive measures should be effective enough to overcome background characteristics.” Generally, the females in our study provided improved periodontal Health Attitudes and Behaviors in several aspects than male dental students. It should point out that 59.6% of dental students in this study were females reflecting the greater number of females linked to males entering the dental field in Iraq. This high percentage of females in the dental field furthermore established in further studies in Greece and Croatia.9,24 Greater plaque and gingival indices observed in male dental students could indicate this behavior. This result is similar to the result found in previous studies,15,35,36 in which female students found to have superior oral health awareness, attitudes, and behaviors than males classmates. They would be more concerned about going to the dentist and would have a tendency to be better educated regarding their oral health despite attending a previous course associated with dentistry.10 Conversely, Badovinac et al24 had established that gender did not have an impact on the HU-DBI score. The female students presented superior reactions concerning item 5, item 7, item 8, item 9, item 12, item 15, item 16, and item 18.
When we investigated PLI and GI index with “yes” for the items 3, 7, 17, and 18 in clinical and preclinical students we recognized that the clinical students had superior awareness regarding their oral and periodontal health than preclinical students and the difference between them was statistically significant, this outcome perhaps because of the introduction of clinical students to the clinical environment and to the fact that they yield periodontology courses comprising: plaque control, tooth brushing techniques, flossing, gingival and periodontal disease and other periodontal health data. As our study was cross-sectional, the results cannot be adequate for curricular modifications; however, it can be a good pointer of needed alterations in the undergraduate curriculum, chiefly in preventive dentistry and oral hygiene courses.
Conclusion
Depended on the results of the current study, it can illustrate that Iraqi dental students had reasonably good oral health behaviors and attitudes; however, additional implementation required on the significance of anticipatory facet of optimum oral hygiene practice. Female dental students presented with better responses only in some items of the questionnaire than male colleagues. Some differences in oral health behaviors were established between preclinical and clinical levels of dental education, although the difference was not significant.
Recommendation
To serve as a good model for their patients, friends, and family members, the development of dental students’ results should be much higher. So the preventive dentistry and periodontology courses should begin since the first year of dental education. Prospective cross-sectional and longitudinal studies relating to dental students from other universities to get a clearer insight into the oral health behavior of dental students in Iraq.
Disclosure
The authors report no conflicts of interest in this work.
References
1. Jin LJ, Lamster IB, Greenspan JS, Pitts NB, Scully C, Warnakulasuriya S. Global burden of oral diseases: emerging concepts, management, and interplay with systemic health. Oral Dis. 2016;22(7):609–619. doi:10.1111/odi.12428
2. Loesche WJ, Grossman NS. Periodontal disease as a specific, albeit chronic, infection: diagnosis and treatment. Clin Microbiol Rev. 2001;14:727–752.
3. Seymour GJ, Ford PJ, Cullinan MP, Leishman S, Yamazaki K. Relationship between periodontal infections and systemic disease. Clin Microbiol Infect. 2007;13 Suppl 4:3–10. doi:10.1111/j.1469-0691.2007.01798.x
4. World Health Organization. Working Together for Health - the World Health Report. Geneva: WHO; 2006.
5. Yao K, Yao Y, Shen X, Changqing L, Guo Q. Assessment of oral health behavior, knowledge, and status among dental and medical undergraduate students: a cross-sectional study. BMC Oral Health. 2019;19:26. doi:10.1186/s12903-019-0716-6
6. Kawamura M. Dental behavioral science: the relationship between perceptions of oral health and oral status in adults. J Hiroshima Univ Dent Soc. 1988;20(2):273–286.
7. Kawamura M, Kawabata K, Sasahara H, Fukuda S, Iwamoto Y. Dental, behavioral science: part IX. Bilinguals’ responses to the dental, behavioral inventory (HU-DBI) written in English and in Japanese. J Hiroshima Univ Dent Soc. 1992;22:198–204.
8. Dumitrescu AL, Wagle M, Dogaru BC, Manolescu B. Modeling the theory of planned behavior for intention to improve oral health behaviors: the impact of attitudes, knowledge, and current behavior. J Oral Sci. 2011;53(3):369–377. doi:10.2334/josnusd.53.369
9. Polychronopoulou A, Kawamura M, Athanasouli T. Oral self-care behavior among dental school students in Greece. J Oral Sci. 2002;44(2):73–78. doi:10.2334/josnusd.44.73
10. Kawamura M, Honkala E, Widström E, Komabayashi T. Cross-cultural differences of self-reported oral health behaviour in Japanese and Finnish dental students. Int Dent J. 2000;50:46–50. doi:10.1111/j.1875-595X.2000.tb00546.x
11. Komabayashi T, Kwan SY, Hu DY, Kajiwara K, Sasahara H, Kawamura M. A comparative study of oral health attitudes and behaviour using the Hiroshima University - Dental Behavioural Inventory (HU-DBI) between dental students in Britain and China. J Oral Sci. 2005;47(1):1–7. doi:10.2334/josnusd.47.1
12. Polychronopoulou A, Kawamura M. Oral self-care behaviours: comparing Greek and Japanese dental students. Eur J Dent Educ. 2005;9(4):164–170. doi:10.1111/j.1600-0579.2005.00387.x
13. Al-Wahadni AM, Al-Omiri MK, Kawamura M. Differences in self-reported oral health behavior between dental students and dental technology/dental hygiene students in Jordan. J Oral Sci. 2004;46(3):191–197. doi:10.2334/josnusd.46.191
14. Kumar S, Busaly IA, Tadakmadla J, Tobaigy F. Attitudes of dental and pharmacy students to oral health behaviour at Jazan University, Kingdom of Saudi Arabia. Arch Orofac Sci. 2012;7(1):9–13.
15. Peker I, Alkurt MT. Oral health attitudes and behavior among a group of Turkish dental students. Eur J Dent. 2009;3(1):24–31. doi:10.1055/s-0039-1697402
16. Neerajaa R, Kayalvizhia G, Sangeethaa P. Oral health attitudes and behavior among a group of dental students in Bangalore, India. Eur J Dent. 2011;5:163–167. doi:10.1055/s-0039-1698874
17. Yildiza S, Dogana B. Self reported dental health attitudes and behaviour of dental students in Turkey. Eur J Dent. 2011;5:253–259. doi:10.1055/s-0039-1698889
18. Kawamura M, Wright FA, Declerck D, et al. An exploratory study on cultural variations in oral health attitudes, behaviour, and values of freshman (first-year) dental students. Int Dent J. 2005;55(4):205–211. doi:10.1111/j.1875-595X.2005.tb00317.x
19. Komabayashi T, Kawamura M, Kim KJ, et al. The hierarchical cluster analysis of oral health attitudes and behaviour using the Hiroshima University-Dental Behavioural Inventory (HUDBI) among final year dental students in 17 countries. Int Dent J. 2006;56(5):310–316. doi:10.1111/j.1875-595X.2006.tb00106.x
20. Loe H. The gingival index, the plaque index, and the retention index systems. J Periodontol. 1967;38(6 Part II):610–616. doi:10.1902/jop.1967.38.6_part2.610
21. Silness J, Loe H. Periodontal disease in pregnancy II. Correlation between oral hygiene and periodontal condition. Acta Odontol Scand. 1964;22:121–135. doi:10.3109/00016356408993968
22. Dagli RJ, Tadakamadla S, Dhanni C, Duraiswamy P, Kulkarni S. Self reported dental health attitude and behavior of dental students in India. J Oral Sci. 2008;50(3):267–272. doi:10.2334/josnusd.50.267
23. Peker K, Uysal O, Bermek G. Dental training and changes in oral health attitudes and behaviors in Istanbul dental students. J Dent Educ. 2010;74(9):1017–1023.
24. Badovinac A, Božić D, Vučinac I, Vešligaj J, Vražić D, Plancak D. Oral health attitudes and behavior of dental students at the University of Zagreb, Croatia. J Dent Educ. 2013;77(9):1171–1178.
25. Pacauskiene IM, Smailiene D, Siudikienė J, Savanevskyte J, Nedzelskiene I. Self-reported oral health behavior and attitudes of dental and technology students in Lithuania. Stomatologija. 2014;16(2):65–71.
26. Al- Omari QD, Hamasha AA. Gender- specific oral health attitudes and behavior among dental students in Jordan. J Contemp Dent Pract. 2005;6:107–114. doi:10.5005/jcdp-6-1-107
27. Alomari Q, Barrieshi-Nusair K, Said K. Smoking prevalence and its effect on dental health attitudes and behavior among dental students. Med Princ Pract. 2006;15(3):195–199. doi:10.1159/000092181
28. AlSwuailem AS, AlShehri MK, Al-Sadhan S. Smoking among dental students at King Saud University: consumption patterns and risk factors. Saudi Dent J. 2014;26(3):88–95. doi:10.1016/j.sdentj.2014.03.003
29. Centers for Disease Control and Prevention (CDC). Tobacco use and cessation counseling–global health professionals survey pilot study, 10 countries, 2005. MMWR Morb Mortal Wkly Rep. 2005;54(20):505–509.
30. Smith DR, Leggat PA. An international review of tobacco smoking among dental students in 19 countries. Int Dent J. 2007;57:452–458. doi:10.1111/j.1875-595X.2007.tb00149.x
31. Shah R, Ghosh S, Chaudhary S, Shah S. Comparison of oral health status between first and final year BDS students: a cross-sectional study. Acta Sci Dent Sci. 2018;2(9):83–86.
32. Lalani A, Dasar PL, Sandesh N, Mishra P, Kumar S, Balsaraf S. Assessment of relationship between oral health behavior, oral hygiene, and gingival status of dental students. Indian J Dent Res. 2015;26:592–597. doi:10.4103/0970-9290.176922
33. Schüz B, Wiedemann AU, Mallach N, Scholz U. Effects of a short behavioural intervention for dental fl ossing: randomized-controlled trial on planning when, where, and how. J Clin Periodontol. 2009;36:498–505. doi:10.1111/j.1600-051X.2009.01406.x
34. Khalid K, Naidoo S, Elamin FI. Oral health behaviours and attitudes using the modified Arabic Version of Hiroshima University - Dental Behavioural Inventory (HU-DBI) among sudanese dental students. Int J Dent Oral Sci. 2016;3(9):326–330.
35. Khami MR, Virtanen JI, Jafarian M, Murtomaa H. Oral health behaviour and its determinants amongst Iranian dental students. Eur J Dent Educ. 2007;11:42–47. doi:10.1111/j.1600-0579.2007.00424.x
36. Al-Omiri MK, Barghout NH, Shaweesh AI, Malkawi Z. Level of education and gender-specific self-reported oral health behavior among dental students. Oral Health Prev Dent. 2012;10:29–35.
 © 2020 The Author(s). This work is published and licensed by Dove Medical Press Limited. The
full terms of this license are available at https://www.dovepress.com/terms
and incorporate the Creative Commons Attribution
- Non Commercial (unported, 3.0) License.
By accessing the work you hereby accept the Terms. Non-commercial uses of the work are permitted
without any further permission from Dove Medical Press Limited, provided the work is properly
attributed. For permission for commercial use of this work, please see paragraphs 4.2 and 5 of our Terms.
© 2020 The Author(s). This work is published and licensed by Dove Medical Press Limited. The
full terms of this license are available at https://www.dovepress.com/terms
and incorporate the Creative Commons Attribution
- Non Commercial (unported, 3.0) License.
By accessing the work you hereby accept the Terms. Non-commercial uses of the work are permitted
without any further permission from Dove Medical Press Limited, provided the work is properly
attributed. For permission for commercial use of this work, please see paragraphs 4.2 and 5 of our Terms.