Back to Journals » Patient Preference and Adherence » Volume 16
Self-Reported Medication Adherence Among Patients with Ulcerative Colitis in Japan and the United Kingdom: A Secondary Analysis for Cross-Cultural Comparison
Authors Kawakami A, Tanaka M ![]() , Choong LM, Kunisaki R, Maeda S, Bjarnason I, Hayee B
, Choong LM, Kunisaki R, Maeda S, Bjarnason I, Hayee B
Received 14 December 2021
Accepted for publication 19 February 2022
Published 8 March 2022 Volume 2022:16 Pages 671—678
DOI https://doi.org/10.2147/PPA.S346309
Checked for plagiarism Yes
Review by Single anonymous peer review
Peer reviewer comments 2
Editor who approved publication: Dr Johnny Chen
Aki Kawakami,1,2 Makoto Tanaka,2 Lee Meng Choong,1 Reiko Kunisaki,3 Shin Maeda,4 Ingvar Bjarnason,1 Bu’Hussain Hayee1
1Department of Gastroenterology, King’s College Hospital, London, UK; 2Department of Critical and Invasive-Palliative Care Nursing, Graduate School of Health Care Sciences, Tokyo Medical and Dental University (TMDU), Bunkyo-ku, Japan; 3Inflammatory Bowel Disease Center, Yokohama City University Medical Center, Yokohama, Japan; 4Department of Gastroenterology, Yokohama City University Graduate School of Medicine, Yokohama, Japan
Correspondence: Makoto Tanaka, Department of Critical and Invasive-Palliative Care Nursing, Graduate School of Health Care Sciences, Tokyo Medical and Dental University (TMDU), 1-5-45, Yushima, Bunkyo-ku, Tokyo, 113-8519, Japan, Tel +81-3-5803-4507, Fax +81-3-5803-4507, Email [email protected]
Purpose: Non-adherence to medication was reported by 28% of Japanese patients with ulcerative colitis, but in the United Kingdom, patients with inflammatory bowel disease have lower medication adherence, which increases clinical relapse risk. The objective of this study was to compare medication adherence among patients with ulcerative colitis in Japan with previously reported results and patients in the United Kingdom.
Patients and Methods: This cross-cultural comparison study investigated medication adherence among 100 ulcerative colitis patients in the United Kingdom and 432 ulcerative colitis patients in Japan. Adherence was assessed using The Morisky Medication Adherence Scale-8 questionnaire. Patient clinical features were collected from medical records and the questionnaire. Distribution of responses for each item, questionnaire total score, difference in ratio for each item between Japanese and UK patients, and difference in percentage of low/medium/high adherence between Japanese and UK patients were compared.
Results: The proportion of low/medium or high adherence was significantly different between countries (42.6% and 7.4% [Japan] vs 24.0% and 76.0% [United Kingdom]; p< 0.01). Significantly more Japanese patients reported taking medication correctly the day before the questionnaire compared with UK patients.
Conclusion: UK patients were more likely to not take medication when they felt their symptoms were under control compared with Japanese patients. UK patients perceived it was more difficult to remember to take the medication than Japanese patients. This study highlights culturally sensitive medication-taking behaviors in Japanese and UK patients with ulcerative colitis.
Keywords: cross-cultural comparison, self-management, race, inflammatory bowel disease
Introduction
Ulcerative colitis (UC) is a chronic, idiopathic, inflammatory bowel disease (IBD) of the large intestine, and its disease course is characterized by periods of relapse and remission.1 Its main symptoms are bloody stool, diarrhea, abdominal pain, and frequent bowel movements.2 UC is a lifelong condition that often first presents in the teens and twenties (25% of cases present in adolescence).3 The number of patients with UC is gradually increasing globally.3,4 These diseases have increased in Europe and North America and estimated UC prevalence rates of 154–233 per 100,000 were reported in the United Kingdom.5 The incidence of UC in 20th century Asia is lower than in Europe. However, IBD incidence in Asia is increasing rapidly with a UC incidence of 172.9 per 100,000 in Japan.6
Regarding medical management of UC, patients are administered 5 aminosalicylic acid (5ASA) during relapse and remission, with additional rectal formulation, corticosteroids, immunomodulators, and anti-TNF agents, depending on disease activity.5 The patients are encouraged to increase their adherence to 5ASA to prevent relapse. Nurses-European Crohn’s & Colitis organization statements reported that nurses should assess IBD patient needs and self-care behavior.7 Increasing medication adherence is an important self-care behavior that prevents relapse.
However, a previous study reported that non-adherence to 5ASA, defined as taking less than 80% of the prescribed dose, was reported by 28% of UC patients in Japan, which increased the risk of clinical relapse 2.3-fold.8 Several studies reported many IBD patients have low adherence in the United Kingdom.9–14 Therefore, to improve this, medication adherence should be evaluated. The Morisky Medication Adherence Scale-8 (MMAS-8) is a self-reported adherence scale developed by Morisky to determine medication adherence.15 It is a popular self-reporting method in the literature and a relevant approach for evaluating medication adherence in a clinical setting.16–18 It has been used in over 100 countries and is validated in over 75 different languages.19 The MMAS-8 is useful for providing reasons for non-adherence as well as the degree of adherence. The English version was developed for patients with UC in the United States20 and has been used to assess the adherence of IBD patients in the United Kingdom.21 We recently validated the Japanese version for UC patients in Japan.22
In any assessment of cross-cultural medication adherence, the impact of culturally unique response patterns in item selection must be taken into consideration. Jackson et al reported that medication adherence was better for “white” Crohn’s disease patients than for African-American patients.12 Another study showed that adherence was higher among “white” IBD patients compared with “black” patients.23 However, no comparison of adherence between Asian and European patients with UC assessed using a common scale has been reported. The results of this type of study might highlight tendencies of specific nations when interpreting reported adherence. Therefore, the objective of this study was to compare medication adherence among Japanese and UK patients with UC assessed using the MMAS-8.
Materials and Methods
This was a retrospective analysis of our previously reported studies22,24 and part of an international comparative research project. To collect data, a cross-sectional survey was conducted at King’s College Hospital in London from April 2016 to April 2017. Sociodemographic and clinical characteristics of the UK participants were reported in a previous study.22 For comparison, we used our previously reported Japanese data.22 The period of data collection in Japan was from May 2012 to December 2012.
Subjects
Patients diagnosed with UC and attending a clinic at King’s College Hospital in London, UK were enrolled consecutively in this study. We enrolled patients who: 1) met the criteria for diagnosis of UC; 2) were over 20 years old; and 3) were prescribed 5ASA. Patients were excluded if they 1) were intolerant to 5ASA; 2) had a history of surgery for UC; 3) were unable to complete the questionnaires or understand Japanese or English; 4) had any serious complication; or 5) participated in other clinical studies at the time of study entry. The Japanese participants were recruited based on the same criteria from May 2012 to December 2012.22
Data Collection Procedure
Before the patients had consulted with a medical doctor or nurse, doctors or nurses selected patients who met the inclusion/exclusion criteria and introduced them to the investigator. These patients were asked to answer questionnaires in a space where their privacy was ensured. Data on the participants’ clinical features were collected from their medical records and through the questionnaire.
Measurements
Medication Adherence
Medication adherence was assessed using a Japanese or English version of the MMAS-8. The MMAS-8 is composed of eight questions, and response categories are yes/no for each item with a dichotomous response and a five-point Likert Scale response for the last item. The original English version was developed for patients with hypertension15 and its reliability and validity among patients with a variety of conditions has been confirmed.16–18 Factor validity, internal consistency, concurrent validity, and scale discriminant validity among patients with UC were confirmed for the Japanese version of the MMAS-8.22
Disease, Medication, Sociodemographic Characteristics, and Abdominal Symptoms
The following clinical information was collected from medical records: disease characteristics such as duration of UC, family history, duration of current remission, disease region as determined via recent colonoscopy, and medication characteristics (frequency of medication per day, daily number of tablets, daily prescribed dose, current concomitant therapy). Subjects were asked about their abdominal symptoms (stool consistency, bowel movements, urgency, pain, visible bleeding) and sociodemographic characteristics (sex, age, employment, marital status, educational level, living situation) in the questionnaire.
Data Analyses
The distribution of response for each item and the total score of MMAS-8 was determined. Next, the difference in ratio between Japan and the United Kingdom was compared for each of the eight items in the MMAS-8. Finally, the difference in percentage between Japan and the United Kingdom was compared for three levels (low/medium/high) of the total score of MMAS-8. All statistical tests were two-tailed, and statistical significance was defined as p < 0.05. All analyses were performed with SAS version 9.4 for Windows (SAS Institute Inc., Cary, NC, USA).
Ethics Approval and Informed Consent
The investigation conformed to the principles outlined in the Declaration of Helsinki. The Ethics Committee of King’s College Hospital National Health Service Foundation Trust approved the protocol of this survey (IRAS project ID: 198963). The investigator explained the outline of this study and the protection of personal information to the subjects using a “patient information sheet” and obtained their written consent. Patients were informed that there would be no disadvantage to their treatment even if they did not consent to the study.
Results
Subject Characteristics
Of 118 UK patients who consented to answer the questionnaire, six failed to return the questionnaire, and 12 did not respond to any of the items concerning adherence and therefore could not be analyzed. The final number of analyzable participants was 100 (84.7%), and the valid response rate was 94.1%. The Japanese data included 432 subjects with a 94.1% valid response rate.22 Japanese and UK participant characteristics are shown in Table 1. Mean age and proportions of each sex were similar in both countries. Japanese patients were prescribed 5ASA significantly more often than UK patients, and Japanese patients took 5ASA significantly more frequently than UK patients. Abdominal symptoms were generally milder in Japanese patients compared with UK patients. We found that 51.6% of patients in Japan and 53.0% of patients in the United Kingdom were taking drugs other than 5ASA. Visible bleeding, an important sign of relapse, was reported by 26.9% of respondents in Japan and 33.0% in the United Kingdom.
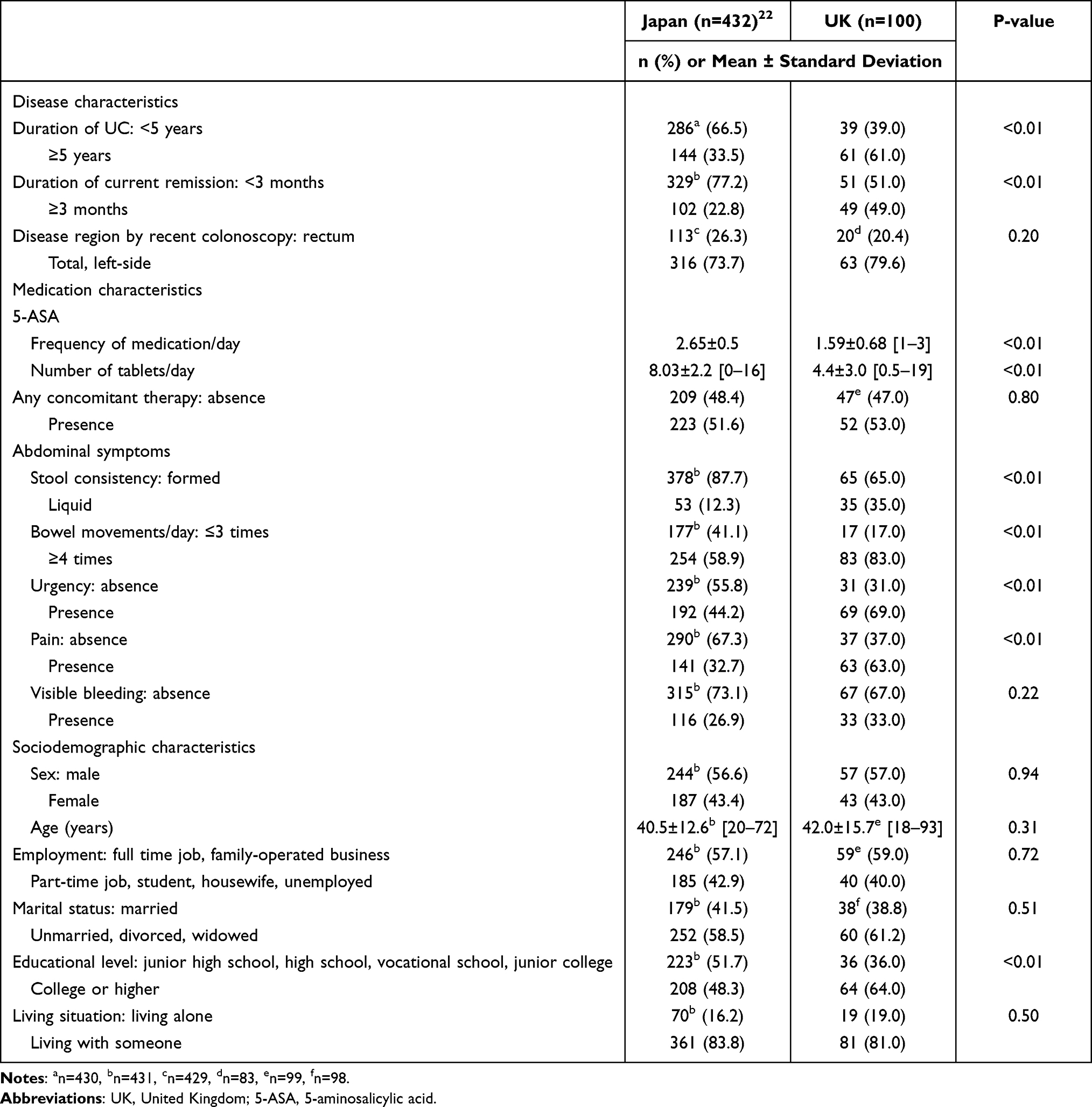 |
Table 1 Subject Characteristics of Japanese and UK Patients |
Total MMAS-8 Score in UK and Japanese Patients
The mean ± standard deviation (SD) score for MMAS-8 was 5.4 ± 1.95 among patients in Japan, and 5.4 ± 2.1 in the United Kingdom, which was not significantly different (p = 0.99). The proportion of low and medium or high adherence was significantly different: 42.6% and 57.4% in Japan compared with 24.0% and 76.0% in the United Kingdom (p < 0.01).
Individual MMAS-8 Scores Between UK and Japanese Patients
Table 2 shows the ratio of each country that answered “yes” for each item of the MMAS-8 and the difference in the ratio of the score in Japan minus the score in the United Kingdom. More than 60% of UK and Japanese patients reported that they sometimes forgot to take their IBD medication (item 1). The proportion of subjects who had reduced or stopped taking their medication without telling their doctor because they felt worse when they took it (item 3) was minimal at 15% in both countries. Significantly more Japanese patients reported taking medication correctly the day before the questionnaire compared with UK patients (difference in ratio (DIR) and 95% confidence interval (CI): 0.08, 0.02 to 0.17). UK patients were more likely to not take medication when they felt their symptoms were under control compared with Japanese patients (DIR: −0.13 and 95% CI: −0.22 to −0.03). UK patients felt it was more difficult to remember to take the medication than Japanese patients (DIR: −0.13 and 95% CI: −0.21 to −0.05).
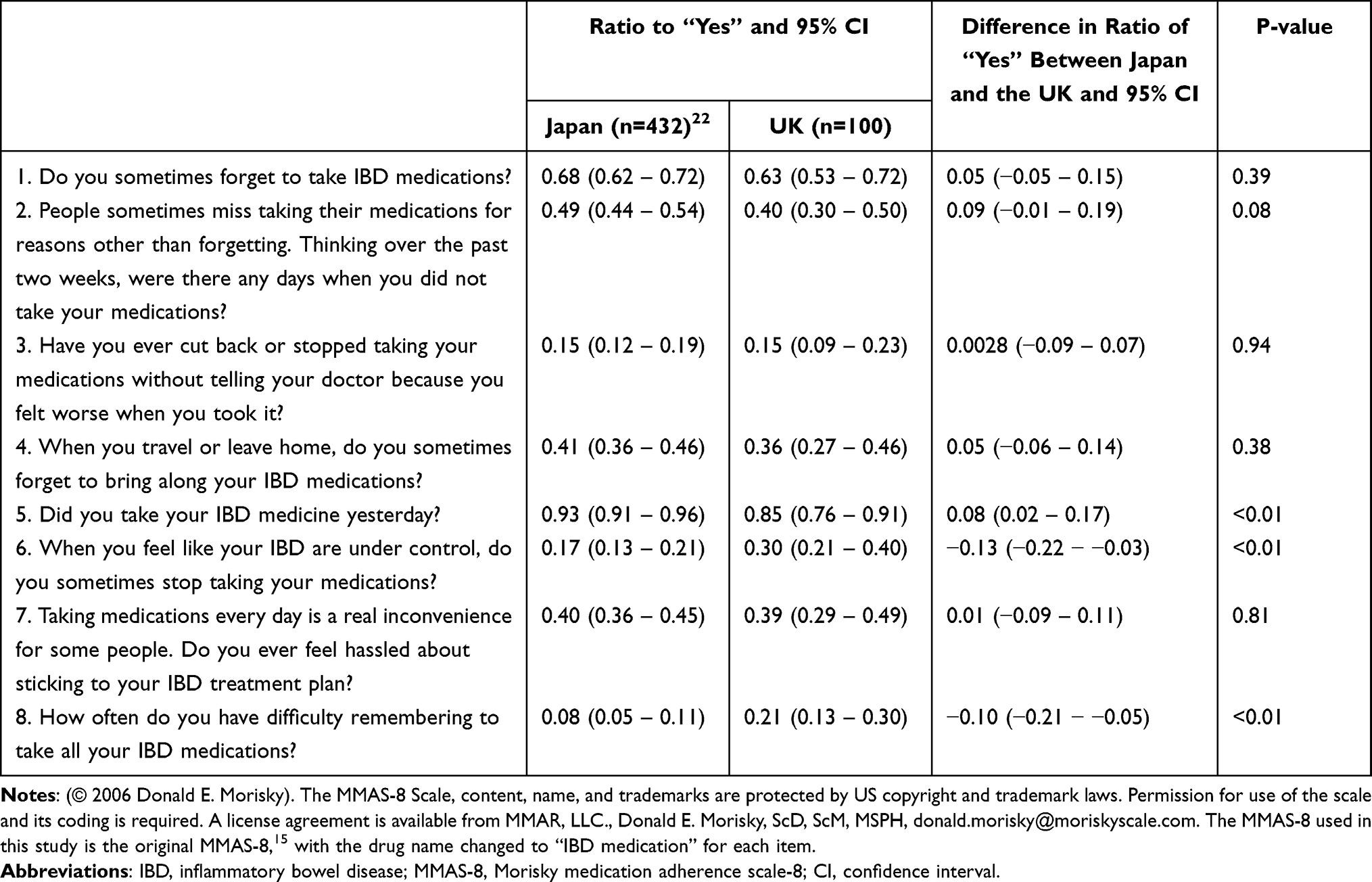 |
Table 2 The Frequency Distribution of the Japanese Version of the MMAS-8 |
Discussion
This is the first study to examine country-related differences in MMAS-8 scores among patients with UC in Japan and the United Kingdom. The mean MMAS-8 score between the two countries was similar. However, from a categorical perspective, the percentage of Japanese with low adherence was higher than that in the United Kingdom.
Surprisingly, the proportion of low adherence was higher in Japanese patients compared with UK patients, in contrast to previously reported adherence in Japanese patients,8 which was better than that of European and American patients.25 There are two possible reasons for this. First, the method of measuring adherence differs between the previous studies and this study. Previous studies quantified adherence by the degree to which patients were taking the medication as prescribed during a certain period. However, the MMAS-8 used in this study scores behavioral patterns related to “easy to forget to take IBD medication” or “difficulty in maintaining IBD medication”. Therefore, the tendency of a nation for self-evaluation and interpretation of certain words such as “sometimes” might have influenced the adherence score in this comparison study between Japanese patients and UK patients. In addition, a previous study reported that Japanese acquiesce more often than Americans who agree on an item without thoroughly examining a question.26 Therefore, Japanese people have a higher “yes-saying tendency”. Five of the eight items tended to lower the adherence score when patients answered “yes” and this bias may have affected the low adherence rates. Another reason is that abdominal symptoms affected adherence scores in this study. A systematic review reported that being in clinical remission is a factor related to non-adherence.12 Calming abdominal symptoms is an important finding of remission and the proportion of low adherence was higher in Japanese with calm abdominal symptoms.
Scores of three out of the eight items in the MMAS-8 showed differences between the two groups. Acommon feature of all three items was that UK patients were more likely to respond to low adherence than Japanese patients. First, compared with UK patients, more Japanese patients reported that they took the IBD medication correctly theday before they answered the MMAS-8 (item5). This item does not ask the reason or perception of not being able to take medication, but simply asks whether patients took the medication theday before they answered the MMAS-8. Therefore, the results of this study support the results of previous studies, indicating that adherence is higher in Japanese patients than in European patients. Second, compared with Japanese patients, UK patients were more likely to respond that they sometimes stopped taking IBD medication when their symptoms were under control (item6). Asystematic review reported that being in UC remission was amajor factor for non-adherence.12 Apotential reason for the greater adherence in this item among Japanese patients compared with previous studies among UK patients might be the obedient nature of Japanese people. Asai etal reported that 47% of Japanese patients would accept recommendations made by physicians even if the recommendations went against their wishes.27 Therefore, compared with UK patients, asmaller proportion of Japanese patients might answer “discontinuing IBD medication” even if their abdominal symptoms had disappeared. Finally, compared with Japanese patients, UK patients responded that they were more likely to have difficulty remembering to take the medication (item8). Although Japanese patients took the medication more frequently perday compared with UK patients, it seemed it was more difficult for UK patients to remember to take the drug compared with Japanese patients. The reason for this is unclear, but aprevious study reported that people in East Asian countries, including Japan, China, and Korea, perceive enduring hardships as avirtue, and they understate the situation if they perceive any difficulties.28
This study had some limitations. First, there was a possibility of sampling bias because the study was conducted at inflammatory bowel disease specialist clinics in urban areas. Of note, the results of the present study were derived from a sample population containing many patients who had been well educated regarding their disease and treatment, and this may have affected their medication adherence. Second, we were unable to match the backgrounds of the Japanese and United Kingdom subjects and this study included patients with various disease activities, and more patients in the United Kingdom had worse abdominal symptoms than Japanese patients, which might have influenced the results. In the future, it will be necessary to compare adherence scores by matching subject backgrounds, including abdominal symptoms. Third, the United Kingdom and Japan surveys were conducted as sub-surveys and therefore sample sizes were not calculated for this study. The difference in the number of participants may have affected statistical significance. Finally, the points in data collection in Japan and the United Kingdom differed by 4–5 years and new formulations of 5ASA have been developed, which might have influenced adherence. In the future, it will be necessary to adjust factors that might affect the score in multivariate analysis and evaluate whether specific country characteristics affect the scores.
Conclusion
The low adherence rate calculated by MMAS-8 was higher in Japanese UC patients than in UK patients. This comparative study between patients with UC in Japan and the United Kingdom demonstrated certain tendencies for some items in the MMAS-8. Three out of the eight MMAS-8 items showed differences between the two groups and a common feature of the three items was that UK patients were more likely to respond to low adherence than Japanese patients. The findings of this study might lead to a better understanding of culturally-sensitive medication-taking behavior. This study suggests that UC patients from Japan need to be assessed carefully for perceptions or difficulties regarding taking medication and it is important for healthcare providers to interpret results by considering the characteristics of the adherence scale used and response bias.
Acknowledgments
The MMAS-8 Scale, content, name, and trademarks are protected by US copyright and trademark laws. Permission for use of the scale and its coding is required. A license agreement is available from MMAR, LLC., Donald E. Morisky, ScD, ScM, MSPH, e-mail: [email protected]. We thank J. Ludovic Croxford, PhD, from Edanz for editing a draft of this manuscript.
Author Contributions
All authors made a significant contribution to the work reported, whether that is in the conception, study design, execution, acquisition of data, analysis and interpretation, or in all these areas; took part in drafting, revising or critically reviewing the article; gave final approval of the version to be published; have agreed on the journal to which the article has been submitted; and agree to be accountable for all aspects of the work.
Funding
This work was supported by JSPS KAKENHI Grant Numbers JP 20K19049 and JP19K10764.
Disclosure
DrAki Kawakami and Makoto Tanaka report grants from JSPS KAKENHI, during the conduct of the study; involved in collaborative research for Takeda Pharmaceutical company, outside the submitted work. The authors report no other conflicts of interest in this work.
References
1. Baumgart DC, Carding SR. Inflammatory bowel disease: cause and immunobiology. Lancet. 2007;369(9573):1627–1640. doi:10.1016/S0140-6736(07)60750-8
2. Baumgart DC, Sandborn WJ. Inflammatory bowel disease: clinical aspects and established and evolving therapies. Lancet. 2007;369(9573):1641–1657. doi:10.1016/S0140-6736(07)60751-X
3. Molodecky NA, Soon IS, Rabi DM, et al. Increasing incidence and prevalence of the inflammatory bowel diseases with time, based on systematic review. Gastroenterology. 2012;142(1):46–54. doi:10.1053/j.gastro.2011.10.001
4. Ng SC, Shi HY, Hamidi N, et al. Worldwide incidence and prevalence of inflammatory bowel disease in the 21st century: a systematic review of population-based studies. Lancet. 2018;390(10114):2769–2778. doi:10.1016/s0140-6736(17)32448-0
5. Bardhan KD, Simmonds N, Royston C, Dhar A, Edwards CM. A United Kingdom inflammatory bowel disease database: making the effort Worthwhile. J Crohns Colitis. 2010;4(4):405–412. doi:10.1016/j.crohns.2010.01.003
6. Murakami Y, Nishiwaki Y, Oba MS, et al. Estimated prevalence of ulcerative colitis and Crohn’s disease in Japan in 2014: an analysis of a nationwide survey. J Gastroenterol. 2019;54(12):1070–1077. doi:10.1007/s00535-019-01603-8
7. O’Connor M, Bager P, Duncan J, et al. N-ECCO Consensus statements on the European Nursing roles in caring for patients with Crohn’s disease or ulcerative colitis. J Crohns Colitis. 2013;7(9):744–764. doi:10.1016/j.crohns.2013.06.004
8. Kawakami A, Tanaka M, Nishigaki M, et al. Relationship between non-adherence to aminosalicylate medication and the risk of clinical relapse among Japanese patients with ulcerative colitis in clinical remission: a prospective cohort study. J Gastroenterol. 2013;48(9):1006–1015. doi:10.1007/s00535-012-0721-x
9. Robinson A, Hankins M, Wiseman G, Jones M. Maintaining stable symptom control in inflammatory bowel disease: a retrospective analysis of adherence, medication switches and the risk of relapse. Aliment Pharmacol Ther. 2013;38(5):531–538. doi:10.1111/apt.12396
10. Gillespie D, Hood K, Farewell D, Stenson R, Probert C, Hawthorne A. Electronic monitoring of medication adherence in a 1-year clinical study of 2 dosing regimens of mesalazine for adults in remission with ulcerative colitis. Inflamm Bowel Dis. 2014;20(1):82–91. doi:10.1097/01.MIB.0000437500.60546.2a
11. Selinger CP, Eaden J, Jones DB, et al. Modifiable factors associated with nonadherence to maintenance medication for inflammatory bowel disease. Inflamm Bowel Dis. 2013;19(10):2199–2206. doi:10.1097/MIB.0b013e31829ed8a6
12. Jackson CA, Clatworthy J, Robinson A, Horne R. Factors associated with non-adherence to oral medication for inflammatory bowel disease: a systematic review. Am J Gastroenterol. 2010;105(3):525–539. doi:10.1038/ajg.2009.685
13. Horne R, Parham R, Driscoll R, et al. Patients’ attitudes to medicines and adherence to maintenance treatment in inflammatory bowel disease. Inflamm Bowel Dis. 2009;15(6):837–844. doi:10.1002/ibd.20846
14. Hawthorne AB, Rubin G, Ghosh S. Review article: medication non-adherence in ulcerative colitis–strategies to improve adherence with mesalazine and other maintenance therapies. Aliment Pharmacol Ther. 2008;27(12):1157–1166. doi:10.1111/j.1365-2036.2008.03698.x
15. Morisky DE, Ang A, Krousel-Wood M, et al. Predictive validity of a medication adherence measure in an outpatient setting. J Clin Hypertens. 2008;10(5):348–354. doi:10.1111/j.1751-7176.2008.07572.x
16. Krousel-Wood MA, Islam T, Webber LS, Re RS, Morisky DE, Muntner P. New Medication Adherence Scale Versus Pharmacy Fill Rates in Seniors With Hypertension. Am J Manag Care 2009;15(1):59-66.
17. Bress AP, Bellows BK, King JB, et al. Cost-effectiveness of intensive versus standard blood-pressure control. N Engl J Med. 2017;377(8):745–755. doi:10.1056/NEJMsa1616035
18. Berlowitz DR, Foy CG, Kazis LE, et al. Effect of intensive blood-pressure treatment on patient-reported outcomes. N Engl J Med. 2017;377(8):733–744. doi:10.1056/NEJMoa1611179
19. Moon SJ, Lee WY, Hwang JS, Hong YP, Morisky DE. Correction: Accuracy of a screening tool for medication adherence: A systematic review and meta-analysis of the Morisky Medication Adherence Scale-8. PLoS One. 2018; 17;13(4):e0196138. doi:10.1371/journal.pone.0196138.
20. Trindade AJ, Ehrlich A, Kornbluth A, Ullman TA. Are your patients taking their medicine? Validation of a new adherence scale in patients with inflammatory bowel disease and comparison with physician perception of adherence. Inflamm Bowel Dis. 2011;17(2):599–604. doi:10.1002/ibd.21310
21. Goodhand JR, Kamperidis N, Sirwan B, et al. Factors associated with thiopurine non-adherence in patients with inflammatory bowel disease. Aliment Pharmacol Ther. 2013;38(9):1097–1108. doi:10.1111/apt.12476
22. Tanaka M, Kawakami A, Maeda S, Kunisaki R, Morisky DE. Validity and reliability of the Japanese version of the morisky medication adherence scale-8 in patients with ulcerative colitis. Gastroenterol Nurs. 2021;44(1):31–38. doi:10.1097/sga.0000000000000533
23. Nguyen GC, LaVeist TA, Harris ML, Datta LW, Bayless TM, Brant SR. Patient trust-in-physician and race are predictors of adherence to medical management in inflammatory bowel disease. Inflamm Bowel Dis. 2009;15(8):1233–1239. doi:10.1002/ibd.20883
24. Kawakami A, Tanaka M, Nishigaki M, et al. A screening instrument to identify ulcerative colitis patients with the high possibility of current non-adherence to aminosalicylate medication based on the health belief model: a cross-sectional study. BMC Gastroenterol. 2014;14:220. doi:10.1186/s12876-014-0220-z
25. Kawakami A, Choong LM, Tanaka M, et al. Validation of the English version of the difficulty of life scale for patients with ulcerative colitis. Eur J Gastroenterol Hepatol. 2020;32(3):312–317. doi:10.1097/meg.0000000000001595
26. Tasaki K, Shin J. Japanese response bias: cross-level and cross-national comparisons on response style. Jpn J Psychol. 2018;88(1):32–42. [in Japanese]. doi:10.4992/jjpsy.88.15065
27. Asai A, Kishino M, Tsugaya F, et al. A report from Japan: choices of Japanese patients in the face of disagreement. Bioethics. 1998;12(2):162-72. doi:10.1111/1467-8519.00102.
28. Ono N. Cultural competence in medical settings. Juntendo Global Liberal Arts. 2016;1:70–79. [in Japanese].
 © 2022 The Author(s). This work is published and licensed by Dove Medical Press Limited. The
full terms of this license are available at https://www.dovepress.com/terms
and incorporate the Creative Commons Attribution
- Non Commercial (unported, 3.0) License.
By accessing the work you hereby accept the Terms. Non-commercial uses of the work are permitted
without any further permission from Dove Medical Press Limited, provided the work is properly
attributed. For permission for commercial use of this work, please see paragraphs 4.2 and 5 of our Terms.
© 2022 The Author(s). This work is published and licensed by Dove Medical Press Limited. The
full terms of this license are available at https://www.dovepress.com/terms
and incorporate the Creative Commons Attribution
- Non Commercial (unported, 3.0) License.
By accessing the work you hereby accept the Terms. Non-commercial uses of the work are permitted
without any further permission from Dove Medical Press Limited, provided the work is properly
attributed. For permission for commercial use of this work, please see paragraphs 4.2 and 5 of our Terms.