Back to Journals » Patient Preference and Adherence » Volume 16
Self-Reported Low Lithium Adherence Among Chinese Patients with Bipolar Disorder in Shenzhen: A Cross-Sectional Study
Authors Chen Y, Zhang J, Hou F, Bai Y ![]()
Received 17 August 2022
Accepted for publication 21 October 2022
Published 2 November 2022 Volume 2022:16 Pages 2989—2999
DOI https://doi.org/10.2147/PPA.S384683
Checked for plagiarism Yes
Review by Single anonymous peer review
Peer reviewer comments 3
Editor who approved publication: Dr Johnny Chen
Yifeng Chen,* Jian Zhang,* Fengsu Hou, Yuanhan Bai
Shenzhen Mental Health Center, Shenzhen Kangning Hospital, Shenzhen, People’s Republic of China
*These authors contributed equally to this work
Correspondence: Yuanhan Bai, Shenzhen Kangning Hospital, Shenzhen Mental Health Center, No. 77 Zhenbi Road, Pingshan District, Shenzhen City, 518118, People’s Republic of China, Email [email protected]
Background: Lithium has been widely used to treat bipolar disorder (BD), although its adherence is rarely reported in China. This study aimed to explore the rate of lithium adherence and its associated factors in patients with BD, which has rarely been reported in China.
Methods: We conducted a cross-sectional study among patients in Shenzhen Mental Health Center (Shenzhen Kangning Hospital), who were aged 12 years or above, were diagnosed with BD based on the International Classification of Diseases, tenth edition (ICD-10), and had been on lithium for at least 1 month. We collected information on sociodemographic and clinical characteristics and on knowledge about and attitudes toward lithium. We also investigated patients’ concerns while taking lithium and where they can and wish to obtain information on lithium.
Results: Of the 244 enrolled patients and 221 patients aged 18 years or older, 52% and 50% disclosed low adherence to lithium, respectively. Factors associated with poor lithium adherence were a younger age (odds ratio (OR): 0.962, 95% confidence interval (CI): 0.933– 0.992), female sex (OR: 2.171, 95% CI: 1.146– 4.112), and no hospitalization history (OR: 0.389, 95% CI: 0.217– 0.689) for the full sample, and more years of education (OR: 4.086, 95% CI: 1.397– 11.946) and fewer hospitalizations (OR: 0.615, 95% CI: 0.467– 0.809) for patients aged 18 years or older. Less knowledge of periodic tests conducted during lithium treatment played a critical role in low lithium adherence (regression analysis of the full sample: OR: 0.642, 95% CI: 0.532– 0.775, regression analysis of subgroups: OR: 0.609, 95% CI: 0.500– 0.742). The treatment duration was a major concern among patients on lithium, and patients preferred obtaining lithium-associated information through health services and WeChat.
Conclusion: The rate of lithium adherence was low in this study. Psychoeducation to increase lithium compliance should mainly focus on patients who are young and provide thorough background information on lithium. Health services should actively provide lithium-associated information. A greater need for medication information based on WeChat was observed, implying its potential role in adherence-related psychoeducation.
Keywords: bipolar disorder, lithium, adherence, China
Introduction
Bipolar disorder (BD) is a common mood disorder characterized by alternating manic/hypomanic and depressive episodes that affects at least 1% of the global population1 and 0.6% of the Chinese population.2 Successful treatment of BD mainly depends on effective and adequate medication treatment.3 However, the rate of nonadherence to medication ranges from 20% to 60% in patients with BD.4 Nonadherence may increase the risks of morbidity, hospitalization, and suicide in patients with BD.5
Lithium was first introduced as a treatment for mania by Australian psychiatrist John Cade in 1949 and then approved by the Food and Drug Administration of the United States for treating mania in 1970 and as a bipolar maintenance treatment in 1974 based on its efficacy and safety in randomized control trials (RCTs).6 As a typical mood stabilizer (MS), lithium is one of the first-line treatments for acute management and prophylaxis of mood episodes7–9 and may reduce the suicide risk.10 Despite the efficacy of lithium in clinical trials, its effectiveness is unsatisfactory in clinical practice. Poor adherence may be one of the causes.11,12 Nonadherence to lithium was associated with mood recurrences,13 increased number and duration of hospital admissions,14 and a higher risk of suicide.15
In addition to unexpected adverse events (AEs),10 nonpharmacological factors lead to poor lithium adherence. A study suggested that attitudes and behaviors would predict adherence to MSs.11 Changing attitudes toward and increasing knowledge of lithium might increase lithium adherence.12,16 Although knowledge and attitudes have been associated with lithium adherence, extrapolating findings from Western countries to Asian areas should be done cautiously due to cultural differences.
Lithium is the first-line treatment for BD listed in the Chinese guideline.8 Studies conducted in Asia suggested a positive association between attitudes and lithium adherence.17,18 However, the underlying elements affecting lithium-taking behaviors remain unclear in China since no consistent findings from two earlier studies with small numbers of patients were found. Lee et al emphasized that therapeutic alliance was more important than better knowledge in promoting lithium adherence,19 while Wong et al suggested that insight played a critical role.20 Conclusions regarding the factors associated with lithium compliance are far from satisfying. Thus, this study aimed to explore the rate of low lithium adherence and associated factors in China and to provide insights into the development of strategies to increase lithium adherence among patients with BD and improve their prognosis. This study may help Chinese psychiatrists modify psychoeducation programs to enhance patients’ lithium adherence, and may enable clinicians from around the world to understand lithium compliance under different cultural contexts.
Methods
This was a cross-sectional study conducted in Shenzhen Mental Health Center (Shenzhen Kangning Hospital, Shenzhen, Guangdong Province, China) from November 2020 to November 2021. The Ethics Committee of Shenzhen Mental Health Center reviewed and approved the current study (No. 2020-K026-01). Written informed consent was obtained from patients and/or their guardians before the investigation. Their participation in the study would not affect or change the medical care provided by their treating clinicians. Our study strictly complied with the Declaration of Helsinki.
Inclusion and Exclusion Criteria
Outpatients of either sex were recruited in the study if they met all of the following criteria: 1) aged 12 years old and above; 2) diagnosed with BD based on the International Classification of Diseases, tenth edition (ICD-10); and 3) treated with lithium for at least 1 month. Patients who 1) were diagnosed with mental disorders other than BD, 2) had a comorbid diagnosis of any major mental disorder (personality disorders, drug abuse, intellectual disability, etc.), 3) could not understand half or more of the items in the questionnaire, or 4) refused to provide written consent were excluded.
Procedure
The diagnosis of BD was verified by experienced psychiatrists in the hospital who performed recruitment. All included patients were symptomatic and the psychiatrists evaluated their ability to complete questionnaires before the investigation. Once participants provided written consent, they completed the questionnaire. It took participants approximately 30 minutes to independently complete the survey. Doctors and participants’ guardians could help them understand items in the questionnaire, but they could not complete the survey for them. All participants were informed to answer questions based on reality. Their personal information and survey data were strictly confidential.
Measurements
The questionnaire was divided into four parts: 1) sociodemographic and clinical features (self-designed), 2) lithium-associated knowledge and attitudes (self-designed), 3) the eight-item Morisky Medication Adherence Scale (MMAS-8) (The MMAS-8 Scale, content, name, and trademarks are protected by US copyright and trademark laws. Permission for use of the scale and its coding is required. A license agreement is available from MMAR, LLC., Donald E. Morisky, ScD, ScM, MSPH, www.moriskyscale.com), and 4) patients’ concerns during lithium treatment (self-designed). Thirteen items concerning sociodemographic characteristics and clinical features were included in the first part of the questionnaire (age, sex, partner and living status, education, overseas education background, income status, medical insurance, awareness of diagnosis, duration of BD, hospitalization history and frequency, and the number of medications other than lithium). Of note, nine years was set as a cutoff point for the item of education years given the Chinese nine-year compulsory education policy.
Chinese versions of the Lithium Knowledge Test (LKT)21 and the Lithium Attitudes Questionnaire (LAQ)22 are unavailable. We referenced some items from previous studies and the LKT and LAQ to explore lithium-associated knowledge and attitudes. At the stage of questionnaire design, we collected information on doctors’ habits in terms of informing patients of lithium knowledge in our hospital and interviewed some patients about their ways of expressing attitudes towards lithium. We developed the questionnaire based on information collected before and revised statements suitable for the Chinese context. Patients’ lithium-related knowledge was assessed by asking about the reason for being prescribed lithium, lithium formulations, monitoring indices during lithium treatment, salt intake, and lithium-associated AEs. For the items in the lithium-associated knowledge section, the scoring method of two questions needs to be explained. The question “Do you know the lithium-associated indices that should be monitored regularly during lithium treatment?” was followed by 4 options for responding: lithium blood levels, thyroid function (TF), renal function (RF), and electrocardiogram (ECG). The number of options was recorded as the item’s score, from 0 (no idea) to 4 (knowing all of the tests). The question “How many lithium-associated AEs do you know about?” was provided with the following multiple response options: general, gastrointestinal, neurologic, cardiac, renal, endocrinologic, psychotic, toxic, hematologic, and dermatologic AEs. The number of options was regarded as the item’s score, from 0 (no idea) to 10 (knowing all of the AEs). Patients’ attitudes toward lithium were assessed by the usefulness and duration of lithium treatment, approaches to handling AEs induced by lithium, and changes in lithium-taking behaviors after being notified of the AEs.
The MMAS-8,23–25 a widely used assessment tool measuring medication-taking behaviors, was used to evaluate lithium adherence. Before the investigation, the subjects were informed to complete the MMAS-8 only based on their lithium-taking behaviors. The total score on the MMAS-8 ranges from 0 to 8, with higher scores representing higher levels of adherence. Total scores < 6, 6 to 7, and 8 are considered low, medium, and high adherence, respectively.23–25 In this study, we set the cutoff point at 6 to categorize participants into a low adherence group (LA) and a medium/high adherence group (MHA).
We also applied two self-designed questions to explore participants’ needs while taking lithium: 1) “What types of information on lithium do you want to know?” and 2) “Where can you or where do you wish to acquire lithium-associated information?’.
Statistical Analyses
Invalid questionnaires were excluded before the statistical analyses (questionnaires that were finished in less than 5 minutes or more than 50% of the answers on the questionnaire were blank). Missing data were imputed using the mean or median based on the original data distribution. Independent two-sample t-tests were used to assess the normally distributed continuous variables. Numerical and nonnormally distributed variables were compared by Mann–Whitney U-tests. Categorical variables were analyzed by chi-square tests. Data are reported as the mean ± standard deviation, frequency, or median. An α of 0.1 in the univariate comparison was used as the cutoff for the inclusion of a variable in the regression model to avoid the loss of potential variables. A stepwise forward logistic regression was used to explore the factors associated with lithium adherence. The regression procedure started with variables that had p < 0.10 in univariate analyses. At each step, the model rejected any variable that had p > 0.05 and was then recalculated. The regression procedure stopped when the remaining variables could not be excluded. Odds ratios (ORs) with 95% confidence intervals (CIs) were reported. In addition, the variance inflation factor (VIF) for the multicollinearity test was reported to clarify the interaction among variables in the logistic regression. We also performed the subgroup analyses after stratifying patients based on an age of 18 years or older. Statistical analyses and graph descriptions were performed with SPSS Statistics version 24.0 (IBM Corporation, the US) and GraphPad Prism version 9.0 (Dennis, Radushev).
Results
From November 2020 to November 2021, we initially screened 346 outpatients. Ninety-seven patients were excluded because the primary diagnosis was not BD. Of the 249 questionnaires, 5 were invalid. A total of 244 questionnaires were included in the analyses.
Univariate Analyses
Sociodemographic and clinical data are shown in Table 1. A total of 244 Chinese patients with BD on lithium were included in the study. The mean age of all included patients was 28.84 ± 9.84 years, with a range from 14 to 67 years. The median age was 24 in the LA group and 30 in the MHA group. The sample consisted of 171 females and 73 males, and there were 98 females in the LA group and 73 in the MHA group. The mean MMAS-8 score across all participants was 5.58 ± 1.95. Approximately half (52.0%) of all subjects reported low lithium adherence. Compared with participants in the MHA group, participants in the LA group were younger (p < 0.001), more likely to be female (p = 0.012), and more likely to lack medical insurance (p = 0.011). The patients in the LA group had less hospitalization experience (p < 0.001) and were hospitalized fewer times (p < 0.001). In subgroup analyses, patients aged 18 years or older accounted for 90.6% of all enrolled patients. As shown in Table 1, the median age was 25 (18 to 67) years in the LA group and 30.5 (18 to 57) years in the MHA group. Eighty-five females were included in the LA group and 71 in the MHA group. Fifty percent of patients disclosed poor lithium adherence. Compared with subjects in the MHA group, patients in the LA group were younger (p < 0.001), more likely to have more years of education (p = 0.005), and more likely to lack medical insurance (p = 0.030). Patients’ hospital admission experience was less (p < 0.001) and fewer hospitalizations were documented (p < 0.001) in the LA group than in the MHA group.
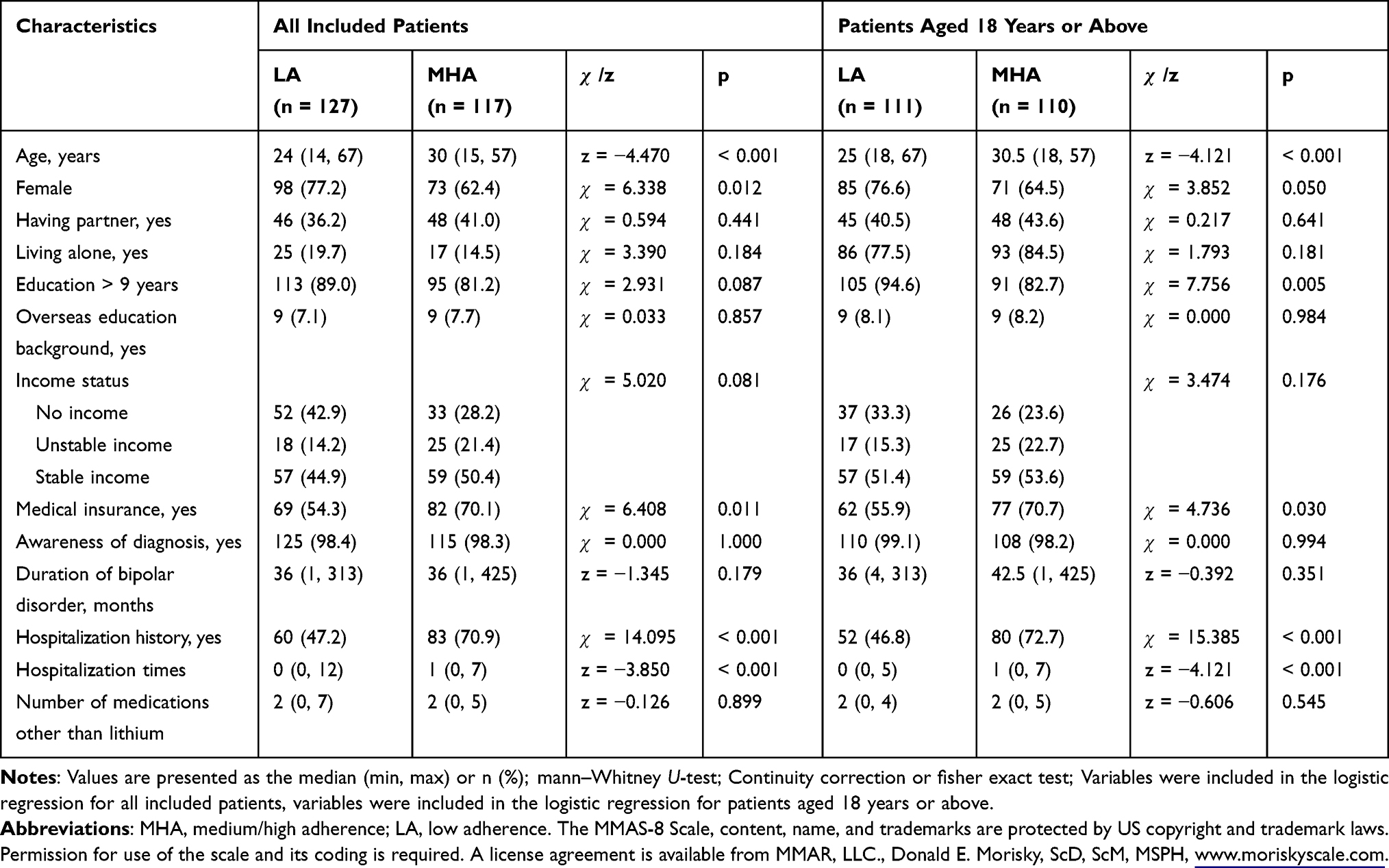 |
Table 1 Sociodemographic and Clinical Characteristics of the Study Subjects |
The comparisons of lithium-associated knowledge and attitudes between the two groups are shown in Table 2. The patients with low adherence had less understanding of periodic tests conducted during lithium treatment (p < 0.001) and salt intake (p < 0.001) while taking lithium. There was a significant difference in how to handle lithium-associated AEs between the two groups (p = 0.045). In subgroup analyses, less understanding of periodic tests conducted during lithium treatment was observed in the LA group than in the MHA group (p < 0.001).
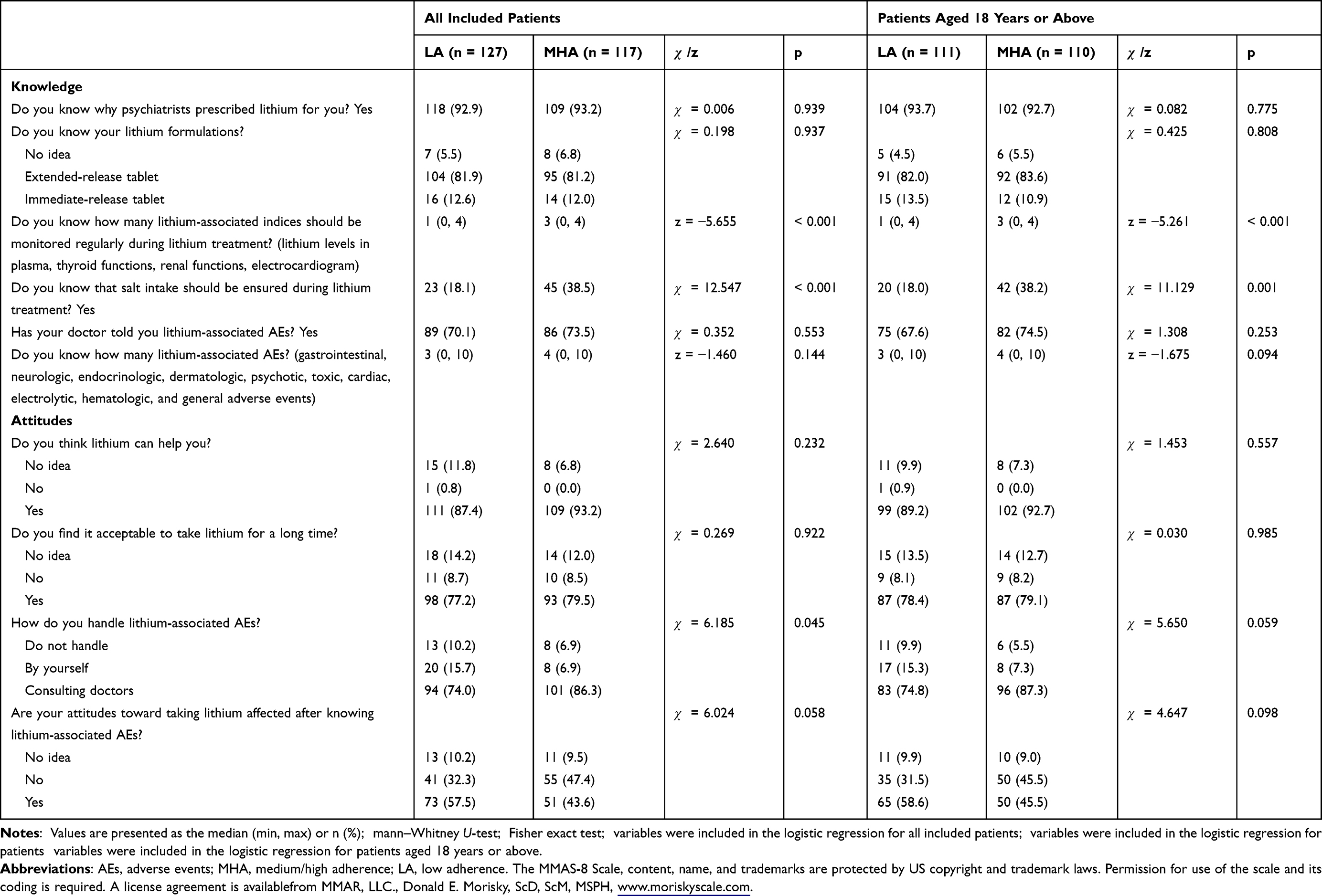 |
Table 2 Lithium-Associated Knowledge and Attitudes in the Study Subjects |
Logistic Regression
After 4 iterations, Table 3 displays the best fitting model (Hosmer–Lemeshow Test, p = 0.878). Four variables were significant predictors of low lithium adherence: younger age (OR: 0.962, 95% CI: 0.933–0.992), female sex (OR: 2.171, 95% CI: 1.146–4.112), no hospitalization history (OR: 0.389, 95% CI: 0.217–0.689), and less knowledge of the periodic tests associated with lithium treatment (OR: 0.642, 95% CI: 0.532–0.775). The best fitting model for the subgroups after 3 iterations was the logistic regression model (Hosmer–Lemeshow Test, p = 0.974). Three factors predicted poor lithium adherence: education > 9 years (OR: 4.086, 95% CI: 1.397–11.946), fewer hospitalizations (OR: 0.615, 95% CI: 0.467–0.809), and less knowledge of the periodic tests associated with lithium treatment (OR: 0.609, 95% CI: 0.500–0.742).
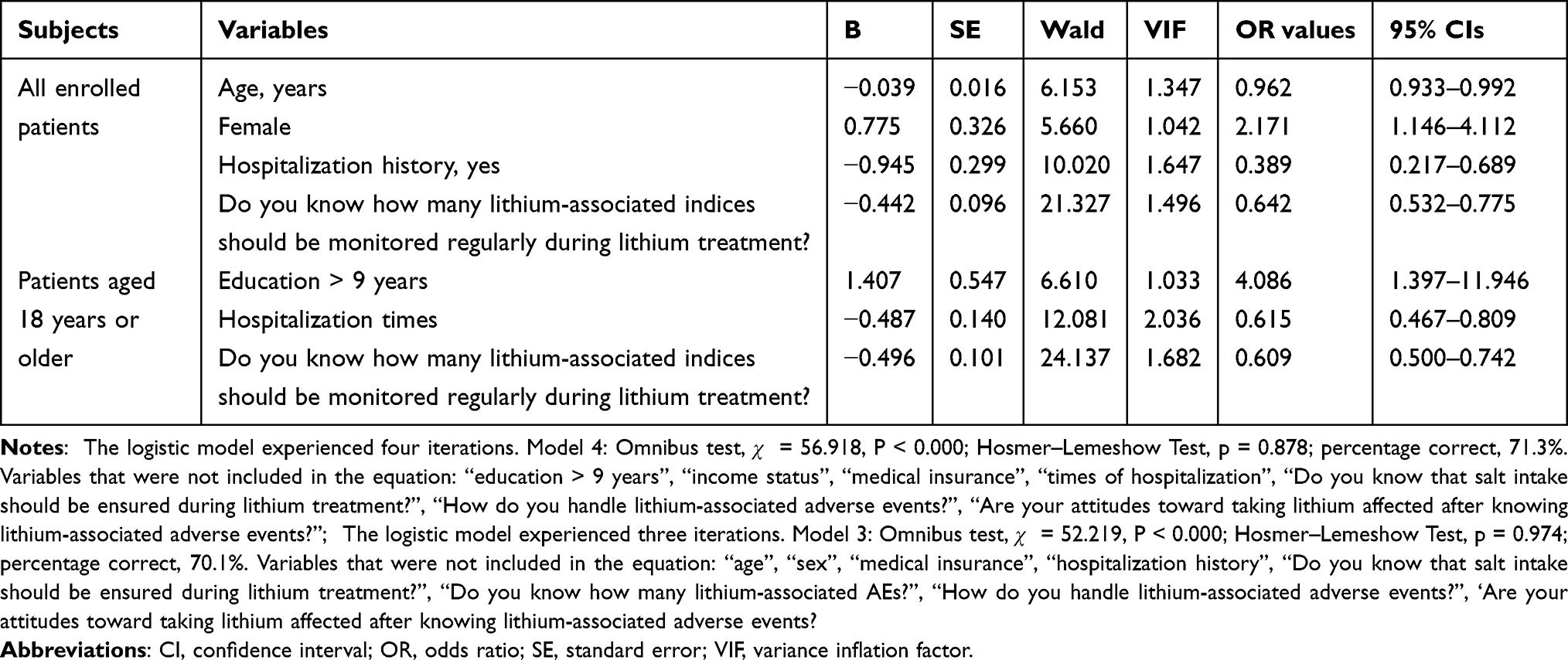 |
Table 3 Logistic Regression Step Forward (Conditional) of Demographic, Clinical, Attitude, and Knowledge Variables on Low Lithium Adherence |
Investigation of Patient Needs During Lithium Treatment
As shown in Figure 1, more than 70% of the patients with BD wanted to know the “duration of taking lithium”, while the “reasons for taking lithium” (45.9%) was the last “want to know” among patients. As shown in Figure 2, the patients with BD acquired lithium-associated information mainly from health services (68.9%), instructions (57.8%), and other social media (19.3%). The patients preferred to obtain lithium-associated information from health services (84%) and WeChat (27.9%).
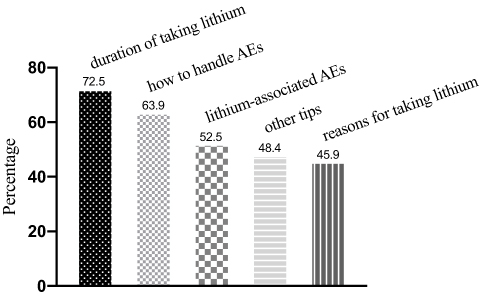 |
Figure 1 Ranks of lithium-associated information the patients want to acquire during lithium treatment. |
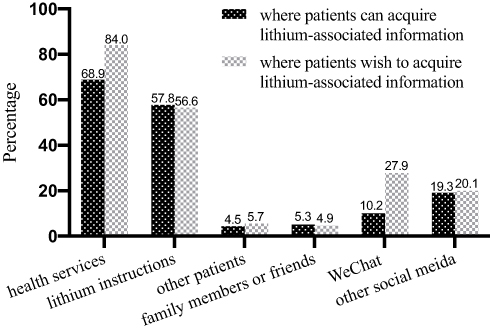 |
Figure 2 Where patients can and wish to acquire lithium-associated information. |
Discussion
This is one of the few studies in China exploring lithium adherence in BD patients, which may help clinicians worldwide understand the factors associated with lithium adherence across cultures. As a typical MS, stable lithium concentrations between 0.4 and 1.0 mmol/L are critical for BD treatment.26 The increased efficacy of lithium over time is another feature when treating BD.10 Thus, the role of lithium in stabilizing mood relies on good adherence. Unfortunately, compliance to lithium in all participants was suboptimal, with an average MMAS-8 score of 5.58 ± 1.95 (scores less than 6 were defined as low adherence). More than half (52%) of the study participants were not adherent to lithium, consistent with the results from two Asian studies.17,27 Non-adherence to lithium has been reported as up to 54% of patients in a Swedish study.28 Although higher lithium adherence was reported in two Chinese studies,19,20 these results were limited by subjective assessments. Since stable lithium therapy is known to be effective in BD, its compliance merits more attention. This study found that younger age, female sex, no hospitalization history, and less knowledge of periodic tests conducted during lithium treatment were predictors of low lithium adherence. Among patients aged ≥ 18 years, more years of education, fewer hospital admissions, and less knowledge of periodic tests conducted during lithium treatment contributed to poor lithium adherence.
In analyses of the full sample, a younger age was a significant risk factor for low lithium adherence. However, the effect of age on lithium adherence disappeared after the adjustment for the age subgroup. Children and adolescents may contribute to poor lithium adherence. A previous study showed that lower lithium adherence was more likely to be observed in younger patients with BD.29 Younger patients with BD are at risk for nonadherent behaviors,4,30–32 partially due to limited insight into their mental condition.33 Children and adolescents may not adequately understand lithium knowledge and the value of lithium in treating BD. The poor effect of lithium on mixed states34 contributes to low adherence because patients with an early age of BD onset often present with mixed episodes.35 This study recruited patients aged 12 to 17 years, and their caregivers/guardians may have interfered with patients’ lithium-taking behaviors due to concerns about lithium-associated AEs. Tremor and cognitive slowing induced by lithium36 impacts school-age youth, which increases the risk for low adherence in this group. Thus, the insights of younger patients with mixed states, their guardians’ attitudes, and the effects of neurologic AEs on their school study should receive special attention when prescribing lithium for youth.
To our knowledge, this is the first study reporting the relationship between female sex and low lithium adherence in China. However, the findings on the effects of sex on adherence have been inconsistent across studies.17,27,32,33,37 We believe several factors may explain this finding. Women with BD are more likely to experience mixed and depressive episodes than men,38,39 which implies a poor response to lithium. Women are more sensitive than men to lithium-associated hypothyroidism10 and weight gain.40 Pregnancy and lactation may influence lithium-taking behaviors, and these clinical characteristics may lead to low lithium adherence in women with BD. Interestingly, in this study, no relationship was observed between the female sex and low lithium adherence in adults. This result did not contradict the outcome of the analysis of the complete sample. In China, lithium is approved for patients with BD aged 12 years or older. Given the risks of the valproate-associated polycystic ovarian syndrome and antipsychotic-related metabolic syndrome, lithium is one of the few optimal medications prescribed for female teenagers with BD. However, lithium-associated tremor and cognitive slowing36 disturb their performance in school and social activities. These patients would likely discontinue lithium with a high probability. This finding may explain the insignificant effect of the female sex on lithium adherence when we removed the sample of patients aged less than 18 years. Further studies are needed to determine whether the female sex is an independent risk factor for low lithium adherence.
In the present study, less hospital admission experience and fewer hospitalizations were associated with poor lithium compliance. In the hospital, patients may have more opportunities to learn about their mental conditions and medication from medical staff and psychoeducation. Some patients perceive the necessity of taking medication to avoid mood relapse and readmission.41 Previous studies reported the relationship between more frequent hospitalizations (≥ 10 times) and low lithium adherence.42 However, the median number of hospitalizations was 1 in the present study. In the early treatment period, patients may adhere to lithium treatment when they are told its therapeutic effects on BD. However, negative consequences over time, such as readmission, can reduce patient confidence in and adherence to lithium. A U-shape relationship between the number of hospitalizations and low lithium compliance may exist. Further investigations are needed to determine whether the decrease in lithium compliance is positively correlated with the frequency of hospitalization. In addition, the hospital admission status has been associated with adherence in patients with BD.43
Another interesting finding was that the effect of more years of education on low lithium adherence became significant when conducting regression analyses of subgroups. Although studies have reported that a high education level was a determinant for good adherence,44–46 our result may imply another possible effect of the education level on adherence. Undoubtedly, patients with more education are more likely to adhere to treatment because of their higher awareness of and more positive attitude towards the disease. However, with the knowledge of BD accumulating over time, patients with high-level education would be disposed to challenging the authority of doctors. We are currently unable to clarify the correlation between the education level and adherence. This patient-related effect on adherence may be easily affected by external factors, such as psychoeducation or the patient-doctor relationship.
Findings regarding the effects of knowledge or attitudes on lithium adherence have been inconsistent.12,16,17,19 Although assessment tools represented by the LKT and LAQ have been employed in lithium adherence studies, the associations between scores and adherence do not necessarily reflect patients’ real concerns about lithium-taking behaviors. Thus, psychiatrists can optimize strategies for prescribing lithium by understanding the concrete factors associated with low adherence. In logistic regression analyses of the total sample and subgroups, lack of knowledge about blood and cardiac tests during lithium treatment was a predictor of poor adherence, consistent with a study conducted in Asia suggesting that insufficient knowledge about the necessity of periodic blood tests was associated with negative attitudes toward lithium. This limited knowledge would lead to missing follow-ups.47 We propose that patients prefer taking lithium when their physical condition is regularly monitored.
Psychoeducation has been broadly recognized to improve medication adherence. In routine practice, clinicians usually fail to focus on patients’ concerns.45 Thus, we investigated patients’ needs while taking lithium to improve future psychoeducation strategies. More than 70% of patients wanted information related to the “duration of taking lithium”; however, less than half of them wanted information related to the “reasons for taking lithium”. This result was quite different from a Western study in which the reason for taking lithium was a major concern in patients.48 The inconsistent results may reflect the distinct cognitions related to medication-taking behaviors across cultures. The social stigma of mental disorders is broadly endorsed in China.49,50 Patients worry that taking lithium over the long term may reveal their diagnosis to friends and colleagues.
In this study, the majority of patients (68.9%) received information from health services, and more than 80% of patients wanted to acquire knowledge from health services. The gap reflected insufficient psychoeducation from mental health providers. We found that only 10.2% of the patients could obtain information from WeChat, whereas nearly 30% wished to acquire knowledge from WeChat. With the popularity of this network, people are accustomed to getting information from portable devices. WeChat is a Chinese multipurpose instant messaging app with a wide range of functions that has a vast user group (https://en.wikipedia.org/wiki/WeChat). Studies have used WeChat to improve medication adherence in China,51,52 but its application for adherence to lithium is rare. This finding suggests that Chinese psychiatrists should partly change their approach to providing lithium-associated psychoeducation.
Limitations
The conclusion from the present study should be extrapolated to real practice with caution because of the limited sample size and single-center design. This study was limited by its cross-sectional design, which allowed us to observe the factors associated with low lithium adherence but not their causal relationships. This study was conducted in the outpatient setting, making many patients unwilling to participate in the survey because of the time required. Multicenter design can be considered for further research. We did not use structured rating scales to assess lithium-associated knowledge and attitudes, which may lead to an insufficiently comprehensive assessment. Mood episodes and comorbid diagnoses were not considered, which may interact with lithium adherence. Self-reported adherence combined with lithium concentrations may be more optimal in terms of the evaluation of lithium adherence.
Conclusion
Although lithium is a first-line treatment for BD, poor adherence to lithium treatment was observed for up to half of the participants in the study. Particular attention should be given to BD patients who are young, female, and have no hospital admission history when prescribing lithium. Knowledge about periodic physical examinations must be provided to patients during lithium treatment. Health services have to provide more information associated with lithium. WeChat should be widely used for psychoeducation to improve lithium adherence in China. To conclude, we hope unexpected outcomes are not from poor adherence.
Acknowledgments
The MMAS-8 Scale, content, name, and trademarks are protected by US copyright and trademark laws. Permission for use of the scale and its coding is required. A license agreement is available from MMAR, LLC., Donald E. Morisky, ScD, ScM, MSPH, www.moriskyscale.com. We would like to thank the participants and their caregivers for their collaboration. The authors express their gratitude to Dr. Haichen Yang, PhD, the director of the Department of Bipolar Disorder at Shenzhen Kangning Hospital, for his suggestions on and proof-reading of the manuscript. The authors thank Dr. Guohua Li, Dr. Zhiqiang Zeng, Dr. Xianbiao Liu, Dr. Hongtao Hu, and Dr. Lin Gong at Shenzhen Kangning Hospital, for their help in assessing patients in the outpatient setting.
Funding
This study was partly supported by the Shenzhen Fund for Guangdong Provincial High-level Clinical Key Specialties (No. SZGSP013), Shenzhen Key Medical Discipline Construction Fund (No. SZXK043), Sanming Project in Medicine of Shenzhen City (No. SZSM201612006). None of the funding agencies had a role in the preparation, data analyses and interpretation, or approval of the manuscript.
Disclosure
The authors report no conflicts of interest in this work.
References
1. Merikangas KR, Jin R, He JP, et al. Prevalence and correlates of bipolar spectrum disorder in the world mental health survey initiative. Arch Gen Psychiatry. 2011;68(3):241–251. doi:10.1001/archgenpsychiatry.2011.12
2. Huang Y, Wang Y, Wang H, et al. Prevalence of mental disorders in China: a cross-sectional epidemiological study. Lancet Psychiatry. 2019;6(3):211–224. doi:10.1016/S2215-0366(18)30511-X
3. Geddes JR, Miklowitz DJ. Treatment of bipolar disorder. Lancet. 2013;381(9878):1672–1682. doi:10.1016/S0140-6736(13)60857-0
4. Levin JB, Krivenko A, Howland M, Schlachet R, Sajatovic M. Medication adherence in patients with bipolar disorder: a comprehensive review. CNS Drugs. 2016;30(9):819–835. doi:10.1007/s40263-016-0368-x
5. MacDonald L, Chapman S, Syrett M, Bowskill R, Horne R. Improving medication adherence in bipolar disorder: a systematic review and meta-analysis of 30 years of intervention trials. J Affect Disord. 2016;194:202–221. doi:10.1016/j.jad.2016.01.002
6. Snitow ME, Bhansali RS, Klein PS. Lithium and therapeutic targeting of GSK-3. Cells. 2021;10(2):255. doi:10.3390/cells10020255
7. Yatham LN, Kennedy SH, Parikh SV, et al. Canadian network for mood and anxiety treatments (CANMAT) and international society for bipolar disorders (ISBD) 2018 guidelines for the management of patients with bipolar disorder. Bipolar Disord. 2018;20(2):97–170. doi:10.1111/bdi.12609
8. Wang Z, Chen J, Yang H, et al. Assessment and management of bipolar disorder: principal summary of updated Chinese guidelines. Bipolar Disord. 2018;20(3):289–292. doi:10.1111/bdi.12646
9. Malhi GS, Gessler D, Outhred T. The use of lithium for the treatment of bipolar disorder: recommendations from clinical practice guidelines. J Affect Disord. 2017;217:266–280. doi:10.1016/j.jad.2017.03.052
10. Barroilhet SA, Ghaemi SN. When and how to use lithium. Acta Psychiatr Scand. 2020;142(3):161–172. doi:10.1111/acps.13202
11. Scott J, Pope M. Nonadherence with mood stabilizers: prevalence and predictors. J Clin Psychiatry. 2002;63(5):384–390. doi:10.4088/JCP.v63n0502
12. Dharmendra MS, Eagles JM. Factors associated with patients’ knowledge of and attitudes towards treatment with lithium. J Affect Disord. 2003;75(1):29–33. doi:10.1016/S0165-0327(02)00027-7
13. Baldessarini RJ, Tondo L, Viguera AC. Discontinuing lithium maintenance treatment in bipolar disorders: risks and implications. Bipolar Disord. 1999;1(1):17–24. doi:10.1034/j.1399-5618.1999.10106.x
14. Schumann C, Lenz G, Berghofer A, Muller-Oerlinghausen B. Non-adherence with long-term prophylaxis: a 6-year naturalistic follow-up study of affectively ill patients. Psychiatry Res. 1999;89(3):247–257. doi:10.1016/S0165-1781(99)00108-0
15. Gonzalez-Pinto A, Mosquera F, Alonso M, et al. Suicidal risk in bipolar I disorder patients and adherence to long-term lithium treatment. Bipolar Disord. 2006;8(5 Pt 2):618–624. doi:10.1111/j.1399-5618.2006.00368.x
16. Rosa AR, Marco M, Fachel JM, Kapczinski F, Stein AT, Barros HM. Correlation between drug treatment adherence and lithium treatment attitudes and knowledge by bipolar patients. Prog Neuropsychopharmacol Biol Psychiatry. 2007;31(1):217–224. doi:10.1016/j.pnpbp.2006.08.007
17. Singh S, Kumar S, Mahal P, Vishwakarma A, Deep R. Self-reported medication adherence and its correlates in a lithium-maintained cohort with bipolar disorder at a tertiary care centre in India. Asian J Psychiatr. 2019;46:34–40. doi:10.1016/j.ajp.2019.09.015
18. Lee Y, Lee MS, Jeong HG, Youn HC, Kim SH. Medication adherence using electronic monitoring in severe psychiatric illness: 4 and 24 weeks after discharge. Clin Psychopharmacol Neurosci. 2019;17(2):288–296. doi:10.9758/cpn.2019.17.2.288
19. Lee S, Wing YK, Wong KC. Knowledge and compliance towards lithium therapy among Chinese psychiatric patients in Hong Kong. Aust N Z J Psychiatry. 1992;26(3):444–449. doi:10.3109/00048679209072068
20. Wong SS, Lee S, Wat KH. A preliminary communication of an insight scale in the assessment of lithium non-adherence among Chinese patients in Hong Kong. J Affect Disord. 1999;55(2–3):241–244. doi:10.1016/S0165-0327(99)00003-8
21. Peet M, Harvey NS. Lithium maintenance: 1. A standard education programme for patients. Br J Psychiatry. 1991;158:197–200. doi:10.1192/bjp.158.2.197
22. Harvey NS. The development and descriptive use of the Lithium Attitudes Questionnaire. J Affect Disord. 1991;22(4):211–219. doi:10.1016/0165-0327(91)90067-3
23. Morisky DE, Ang A, Krousel-Wood M, Ward HJ. Predictive validity of a medication adherence measure in an outpatient setting. J Clin Hypertens. 2008;10(5):348–354. doi:10.1111/j.1751-7176.2008.07572.x
24. Bress AP, Bellows BK, King JB, et al. Cost-effectiveness of intensive versus standard blood-pressure control. N Engl J Med. 2017;377(8):745–755. doi:10.1056/NEJMsa1616035
25. Berlowitz DR, Foy CG, Kazis LE, et al. Effect of intensive blood-pressure treatment on patient-reported outcomes. N Engl J Med. 2017;377(8):733–744. doi:10.1056/NEJMoa1611179
26. Malhi GS, Gershon S, Outhred T. Lithiumeter: version 2.0. Bipolar Disord. 2016;18(8):631–641. doi:10.1111/bdi.12455
27. Selvakumar N, Menon V, Kattimani S, Cross-sectional A. Analysis of patterns and predictors of medication adherence in bipolar disorder: single center experience from South India. Clin Psychopharmacol Neurosci. 2018;16(2):168–175. doi:10.9758/cpn.2018.16.2.168
28. Öhlund L, Ott M, Oja S, et al. Reasons for lithium discontinuation in men and women with bipolar disorder: a retrospective cohort study. BMC Psychiatry. 2018;18(1):37. doi:10.1186/s12888-018-1622-1
29. Kessing LV, Sondergard L, Kvist K, Andersen PK. Adherence to lithium in naturalistic settings: results from a nationwide pharmacoepidemiological study. Bipolar Disord. 2007;9(7):730–736. doi:10.1111/j.1399-5618.2007.00405.x
30. Johnson FR, Ozdemir S, Manjunath R, Hauber AB, Burch SP, Thompson TR. Factors that affect adherence to bipolar disorder treatments: a stated-preference approach. Med Care. 2007;45(6):545–552. doi:10.1097/MLR.0b013e318040ad90
31. Barraco A, Rossi A, Nicolo G, Group ES. Description of study population and analysis of factors influencing adherence in the observational Italian study “Evaluation of Pharmacotherapy Adherence in Bipolar Disorder” (EPHAR). CNS Neurosci Ther. 2012;18(2):110–118. doi:10.1111/j.1755-5949.2010.00225.x
32. Leclerc E, Mansur RB, Brietzke E. Determinants of adherence to treatment in bipolar disorder: a comprehensive review. J Affect Disord. 2013;149(1–3):247–252. doi:10.1016/j.jad.2013.01.036
33. Inoue T, Sano H, Kojima Y, Yamada S, Shirakawa O. Real-world treatment patterns and adherence to oral medication among patients with bipolar disorders: a retrospective, observational study using a healthcare claims database. Neuropsychiatr Dis Treat. 2021;17:821–833. doi:10.2147/NDT.S299005
34. Grunze H, Vieta E, Goodwin GM, et al. The World Federation of Societies of Biological Psychiatry (WFSBP) guidelines for the biological treatment of bipolar disorders: acute and long-term treatment of mixed states in bipolar disorder. World J Biol Psychiatry. 2018;19(1):2–58. doi:10.1080/15622975.2017.1384850
35. Saxena K, Kurian S, Saxena J, Goldberg A, Chen E, Simonetti A. Mixed states in early-onset bipolar disorder. Psychiatr Clin North Am. 2020;43(1):95–111. doi:10.1016/j.psc.2019.10.009
36. Grant B, Salpekar JA. Using lithium in children and adolescents with bipolar disorder: efficacy, tolerability, and practical considerations. Paediatr Drugs. 2018;20(4):303–314. doi:10.1007/s40272-018-0289-x
37. Bauer M, Glenn T, Alda M, et al. Trajectories of adherence to mood stabilizers in patients with bipolar disorder. Int J Bipolar Disord. 2019;7(1):19. doi:10.1186/s40345-019-0154-z
38. Burt VK, Rasgon N. Special considerations in treating bipolar disorder in women. Bipolar Disord. 2004;6(1):2–13. doi:10.1046/j.1399-5618.2003.00089.x
39. Subramanian K, Sarkar S, Kattimani S. Bipolar disorder in Asia: illness course and contributing factors. Asian J Psychiatr. 2017;29:16–29. doi:10.1016/j.ajp.2017.04.009
40. Yaramala SR, McElroy SL, Geske J, et al. The impact of binge eating behavior on lithium- and quetiapine-associated changes in body weight, body mass index, and waist circumference during 6 months of treatment: findings from the bipolar CHOICE study. J Affect Disord. 2020;266:772–781. doi:10.1016/j.jad.2018.09.025
41. Chakrabarti S. Treatment-adherence in bipolar disorder: a patient-centred approach. World J Psychiatry. 2016;6(4):399–409. doi:10.5498/wjp.v6.i4.399
42. Aagaard J, Vestergaard P, Maarbjerg K. Adherence to lithium prophylaxis: II. Multivariate analysis of clinical, social, and psychosocial predictors of nonadherence. Pharmacopsychiatry. 1988;21(4):166–170. doi:10.1055/s-2007-1014670
43. Schuepbach D, Novick D, Haro JM, et al. Determinants of voluntary vs. involuntary admission in bipolar disorder and the impact of adherence. Pharmacopsychiatry. 2008;41(1):29–36. doi:10.1055/s-2007-993213
44. Kirchner SK, Lauseker M, Adorjan K, et al. Medication adherence in a cross-diagnostic sample of patients from the affective-to-psychotic spectrum: results from the psycourse study. Front Psychiatry. 2021;12:713060. doi:10.3389/fpsyt.2021.713060
45. Garcia S, Martinez-Cengotitabengoa M, Lopez-Zurbano S, et al. Adherence to antipsychotic medication in bipolar disorder and schizophrenic patients: a systematic review. J Clin Psychopharmacol. 2016;36(4):355–371. doi:10.1097/JCP.0000000000000523
46. Dou L, Hu L, Zhang N, Cutler H, Wang Y, Li S. Factors associated with medication adherence among patients with severe mental disorders in China: a propensity score matching study. Patient Prefer Adherence. 2020;14:1329–1339. doi:10.2147/PPA.S255934
47. Kumar S, Singh S, Mahal P, Vishwakarma A, Deep R. Assessment of lithium-related knowledge and attitudes among patients with bipolar disorder on long-term lithium maintenance treatment. Indian J Psychiatry. 2020;62(5):577–581. doi:10.4103/psychiatry.IndianJPsychiatry_339_19
48. Pope M, Scott J. Do clinicians understand why individuals stop taking lithium? J Affect Disord. 2003;74(3):287–291. doi:10.1016/s0165-0327(02)00341-5
49. Lam TP, Sun KS. Stigmatizing opinions of Chinese toward different types of mental illnesses: a qualitative study in Hong Kong. Int J Psychiatry Med. 2014;48(3):217–228. doi:10.2190/PM.48.3.f
50. Liu J, Ma H, He YL, et al. Mental health system in China: history, recent service reform and future challenges. World Psychiatry. 2011;10(3):210–216. doi:10.1002/j.2051-5545.2011.tb00059.x
51. Zhang Y, Fan D, Ji H, Qiao S, Li X. Treatment adherence and secondary prevention of ischemic stroke among discharged patients using mobile phone- and wechat-based improvement services: cohort study. JMIR Mhealth Uhealth. 2020;8(4):e16496. doi:10.2196/16496
52. Wang J, Zeng Z, Dong R, et al. Efficacy of a WeChat based intervention to adherence to secondary prevention in patients undergoing coronary artery bypass graft in China: a randomized controlled trial. J Telemed Telecare. 2020;2020:1357633X20960639. doi:10.1177/1357633X20960639
 © 2022 The Author(s). This work is published and licensed by Dove Medical Press Limited. The
full terms of this license are available at https://www.dovepress.com/terms
and incorporate the Creative Commons Attribution
- Non Commercial (unported, 3.0) License.
By accessing the work you hereby accept the Terms. Non-commercial uses of the work are permitted
without any further permission from Dove Medical Press Limited, provided the work is properly
attributed. For permission for commercial use of this work, please see paragraphs 4.2 and 5 of our Terms.
© 2022 The Author(s). This work is published and licensed by Dove Medical Press Limited. The
full terms of this license are available at https://www.dovepress.com/terms
and incorporate the Creative Commons Attribution
- Non Commercial (unported, 3.0) License.
By accessing the work you hereby accept the Terms. Non-commercial uses of the work are permitted
without any further permission from Dove Medical Press Limited, provided the work is properly
attributed. For permission for commercial use of this work, please see paragraphs 4.2 and 5 of our Terms.
Recommended articles
Long-Term Trends in the Burden of Bipolar Disorder in China, 1990–2052: An Analysis of the Global Burden of Disease Study 2023
Lin D, Guo P, Kou M, Xie X, Li Y, Luo S, Xue A, Liang J
Psychology Research and Behavior Management 2026, 19:617390
Published Date: 30 June 2026