Back to Journals » Patient Preference and Adherence » Volume 14
Self-Report for Measuring and Predicting Medication Adherence: Experts’ Experience in Predicting Adherence in Stable Psychiatric Outpatients and in Pharmacokinetics
Authors De las Cuevas C ![]() , de Leon J
, de Leon J ![]()
Received 30 May 2020
Accepted for publication 25 September 2020
Published 9 October 2020 Volume 2020:14 Pages 1823—1842
DOI https://doi.org/10.2147/PPA.S242693
Checked for plagiarism Yes
Review by Single anonymous peer review
Peer reviewer comments 2
Editor who approved publication: Dr Johnny Chen
Carlos De las Cuevas,1,2 Jose de Leon3– 5
1Department of Internal Medicine, Dermatology and Psychiatry, University of La Laguna, San Cristóbal de La Laguna, Canary Islands, Spain; 2Instituto Universitario de Neurociencia (IUNE), Universidad de La Laguna, San Cristóbal de La Laguna, Spain; 3Mental Health Research Center at Eastern State Hospital, Lexington, KY, USA; 4Psychiatry and Neurosciences Research Group (CTS-549), Institute of Neurosciences, University of Granada, Granada, Spain; 5Biomedical Research Centre in Mental Health Net (CIBERSAM), Santiago Apóstol Hospital, University of the Basque Country, Vitoria, Spain
Correspondence: Carlos De las Cuevas
Department of Internal Medicine, Dermatology and Psychiatry, Universidad de La Laguna,, Campus de Ofra s/n, San Cristóbal de La Laguna, Canary Islands, Spain
Tel +34-922-316502
Fax +34-922-319353
Email [email protected]
The Problem: Poor adherence to appropriately prescribed medication is a global challenge for psychiatrists.
Prior Studies: Measuring adherence is complicated. In our recent three-country naturalistic study including more than 1000 patients and their adherence to multiple medication prescriptions at the same time, patients’ self-report of adherence to each specific drug was the only practical option for measuring adherence. Systematic literature reviews provide inconsistent results for sociodemographic, clinical and medication variables as predictors of adherence to psychiatric drugs. Our studies over the last 10 years in relatively stable psychiatric outpatients have shown that some self-reported health beliefs had consistent, strong effects and a better predictive role. Three dimensions of these health beliefs are characteristics of the individual: 1) attitudes toward psychiatric medication such as pharmacophobia (fear of taking drugs or medicines), 2) health locus of control (the belief patients have about who or what agent determines the state of their health), 3) psychological reactance (an emotional reaction in direct contradiction to rules or regulations that threaten or suppress certain freedoms in behavior). They can be measured by the Patient Health Beliefs Questionnaire on Psychiatric Treatment. The attitude toward each specific medication can be measured by the necessity-concern framework and summarized as the presence or absence of skepticism about that drug. After 25 years conducting pharmacokinetic studies in psychiatric drugs, particularly antipsychotics, we have limited understanding of how to use blood levels to predict the effects of non-adherence or to establish it.
Expert Opinion on Future Studies: Future studies to predict adherence should include the inpatient setting and explore insight. Studying the pharmacokinetics associated with non-adherence in each psychiatric drug is a major challenge. Medication adherence is a complex and dynamic process changing over time in the same patient. Personalizing adherence using psychological or pharmacological variables are in their initial stages.
Keywords: attitude to health, drug monitoring, health behavior, medication adherence, psychiatry, psychopharmacology
Plain Language Summary
Why was the review done? Self-report can be used to measure medication adherence. Self-report can also be used to study some psychological attitudes that may predict adherence to psychiatric medications. The literature on predictors of adherence in psychiatric drugs provides inconsistent results for sociodemographic, clinical and medication variables.
What did the authors do? In their recent three-country naturalistic study including more than 1000 patients and their adherence to multiple medication prescriptions at the same time, the authors found that patients’ self-report of adherence to each specific drug was the only practical option for measuring adherence. The authors reviewed the literature, including systematic reviews on how sociodemographic, clinical and medication characteristics are being associated with adherence to prescribed psychiatric medications. They also compared these sociodemographic, clinical and medication characteristics against the self-reported psychological measures included in their studies over the last 10 years in relatively stable psychiatric outpatients.
What do these results mean? To summarize the self-reported dimensions that may predict medication adherence, the authors developed a new questionnaire. Future studies need to explore insight (recognition that one has a psychiatric disorder and awareness that treatment could be helpful) and include the inpatient setting. Medication adherence is a complex and dynamic variable that changes over time even in the same patient.
Introduction to Medication Adherence in Psychiatry
This Expert Opinion article reviews the literature in 3 sections: introduction to medication adherence in psychiatry, methods for measuring adherence as applied to psychiatry, and predictors of adherence in psychiatric patients. Then, it describes our psychiatric studies on medication adherence in stable outpatients and on pharmacokinetics as it relates to adherence. Finally, we provide sections on future studies and an expert opinion on the complexity of studying medication adherence in psychiatry.
This introduction to adherence in psychiatry has 4 subsections: defining medication adherence, relevance of adherence to psychiatric medications, adherence in severe mental illness in general and adherence in specific severe mental illnesses.
Defining Medication Adherence
Medication-taking is a complex human health behavior discussed extensively in the literature amid notable controversy.1 In the past, the literature used the term compliance, but lately, adherence has been used more often. Compliance, adherence and concordance are overlapping terms reflecting the complexity of medicine-taking behaviors.2,3
In 2003, the World Health Organization defined adherence as
The extent to which a person’s behavior – taking medication, following a diet, and/or executing lifestyle changes, corresponds with agreed recommendations from a health care provider.4
This wide definition extends adherence to successful self-management, since it emphasizes agreement and communication between the patient and the healthcare professional and includes more than strict compliance in taking prescribed medication. Treatment adherence can be considered in terms of points on a continuum ranging from treatment refusal to proper follow-up of prescriber instructions. It is essential to establish a sufficient level of treatment adherence to ensure effectiveness for each patient at each given moment.
Relevance of Adherence to Psychiatric Medications
Although the efficacy of psychiatric medications is frequently questioned,5 taking psychiatric drugs at prescribed doses, at correct intervals, and for the period recommended is still essential for psychiatric patients to obtain the maximum possible benefits of these medications.6 However, it is estimated that up to 45% of psychiatric medications are not taken as prescribed,7 resulting in considerable cost for individual patients and healthcare systems.4 At the patient level, inadequate adherence to prescribed psychiatric medications has been found to be associated with poorer outcomes for patients, including the early return of symptoms within the expected duration of a current episode (relapse) or new episodes (recurrence) following initial short-term improvement or remission, as well as hospital admissions.8,9 Furthermore, inadequate adherence can be a risk factor for violence in psychotic disorders,10 for suicide in major depressive disorders,11,12 and for premature mortality in schizophrenia.13 Finally, at the healthcare system level, psychiatric medication non-adherence represents a significant cost burden although related research is limited and of varying quality.14,15
Adherence in Severe Mental Illnesses in General
In principle, every psychiatric patient has the right to be treated and the right to refuse treatment, exceptions being emergency situations in which there is an imminent danger to self or others. Unfortunately, it is common that those patients with greater need of treatment (those with severe mental illnesses) are the more inclined to refuse it and this fact is posed in direct contradiction to the ethical principles of beneficence and respect for patient autonomy.16
It is assumed that psychiatric patients are able to choose; act rationally, intentionally, and responsibly; and make decisions in terms of costs and benefits.17 However, patients with severe mental illnesses such as schizophrenia, bipolar disorder, and major depression can go through phases in which their awareness of illness is impaired; this lack of insight, or anosognosia, represents the most significant reason for treatment refusal when they are acutely ill.18 Therefore, adherence is a process that requires time for its proper development, where people suffering a psychiatric disorder need to identify as patients, develop awareness of their mental illness, participate in their mental health care, and establish a relationship of trust and collaboration with mental health professionals. Adherence to prescribed psychiatric medication in severe mental illness is a dynamic variable and there are major differences between in- and outpatient treatments.
In acute inpatient treatment, clinicians hope that after refusal of essential medication, the patient will move to reacceptance of, and long-term compliance with, medication. The pathway to reacceptance of essential medication by patients who have refused medication can take various forms. Sometimes psychiatrists have no choice but to turn to involuntary medication. Patients may then voluntarily accept medication or it may be necessary to get a court order.19 Although there are no systematic studies, during psychiatric hospitalization most, if not all, patients become adherent as a consequence of the close supervision of medicine-taking behaviors. Adherence is usually good after the initial hospital discharge but decreases substantially over time.20
Adherence in Specific Severe Mental Illnesses
There are controversies in the psychiatric literature about the benefits of psychiatric medications during acute exacerbations and maintenance in the three major severe mental illnesses. However, most expert reviews in schizophrenia,21,22 bipolar disorder,23,24 or major depression25,26 agree on the need for medication in acute severe cases and for avoiding relapses.
Unfortunately, the literature on adherence for these three severe mental illnesses does not appear to be very helpful in providing specific recommendations to clinicians regarding predicting adherence in individual patients, although experts agree on the importance of medication adherence.27
Recent expert reviews on adherence in schizophrenia tend to describe general aspects and rarely provide specific recommendations which can be used by practicing clinicians. Tham et al28 state that greater insight and less severe psychotic symptoms are associated with increased adherence in general but they do not integrate their review in the context of the phases of the illness and the differences between in- and outpatients. Kikkert and Dekker29 say that, although it is an intensively studied phenomenon, we have little understanding of underlying mechanisms leading to nonadherence. Kane and Correll30 emphasized the role of long-acting injection (LAI) antipsychotics in increasing adherence during maintenance treatment in outpatients. Bright31 focused on difficulties in measuring adherence but in our experience with stable outpatients this problem is common to all patients with severe mental illnesses. Weiden32 stresses that patients with schizophrenia frequently do not disclose to their treating physicians that they are not adherent. This explains why, in a relatively small study using blood levels to identify schizophrenia patients considered by their psychiatrists to be treatment-resistant, one-third of them had subtherapeutic serum concentrations which in many cases may be associated with lack of consistent adherence.33
Recent reviews focused on adherence during maintenance treatment of bipolar disorder also tend to provide limited specific information for orienting practicing clinicians. Levin et al34 provided a narrative review with no specific data on the significance of the variables in the various studies concerning what they call barriers to adherence, including those related to 1) bipolar pathology, 2) an individual’s circumstances and 3) external factors such as treatment setting or healthcare system. Systematic reviews of interventions for improving adherence stressed the limitations of methodology for establishing long-term adherence in patients with bipolar disorder.35,36 In the last five years, as new formulations of second-generation LAIs are being developed by pharmaceutical companies, the companies have realized that the LAI market may not only include patients with chronic schizophrenia but also patients needing maintenance in bipolar disorder.37 Therefore, some recent reviews focus on the potential role of LAI antipsychotics38 but there are no long-term studies with these compounds in bipolar disorder. After a systematic review of drug discontinuation in both schizophrenia and bipolar disorder, Gentile39 had the opinion that new second-generation LAIs may not be any better than the less expensive compounds (oral or first-generation LAIs) for individualizing treatment.
There are fewer expert reviews of adherence in major depression than in schizophrenia and bipolar disorder. In a narrative review of adherence to antidepressants in general, Hung40 stressed the multiple factors that may contribute to non-adherence. The most significant contributors to poor adherence that they list include minority status, immigrant status, low income, lack of health insurance, adverse effects, pregnancy, dissatisfaction with treatment, poor relationship of patients with healthcare professionals and lack of information. The factors they listed as contributing to better adherence were old age, positive attitudes to depression and antidepressants, previous experiences and vicarious experiences of depression and antidepressant treatment. Rush and Thase41 maintain that, for improving adherence in major depression, clinicians need to practice patient-centered medical management.
Measuring Medication Adherence in Psychiatry
A prior Expert Opinion article in this journal was completely dedicated to medication adherence. In that article, Whalley Buono et al42 stressed three important facts: 1) the most robust medication adherence measures are often ill-suited for large-scale use, 2) less robust measures including self-report are commonly misinterpreted in population-level analyses, and 3) in the absence of a gold standard, the choice of the method for measuring adherence must consider the purposes of the study.
We completely agree with these 3 facts, which have become obvious as we have moved toward greater complexity in our medication adherence studies in relatively stable outpatients. In 2013, the first author43 recruited only at one site and only patients with one diagnosis in a cross-sectional sample. Moreover, he assumed that a global measure of self-reported adherence was a good reflection of adherence, ignoring the fact that most psychiatric patients take several medications and thus may have differing levels of adherence for these different medications. Our most recent study44,45 with a similar cross-sectional design included 1372 patients from 3 recruitment sites in 3 different countries (Argentina, Spain and Venezuela), having different levels of access to health care. After consecutive recruitment of patients willing to sign a consent form at each site, we were able to collect adherence levels for 2454 oral psychiatric medications which reflected 80 different pharmacological compounds.
After almost 10 years of research, we have a very practical approach to the issue of measuring medication adherence in psychiatric patients. We propose to review the subject in 4 subsections: measuring adherence to a single oral medication, measuring adherence to multiple oral psychiatric medications in large samples, adherence to LAI psychiatric medications and the limitation of clinical samples.
Adherence to a Single Oral Medication
Based on our experience and, more importantly, on recent review articles,42,46,47 Table 1 provides a brief summary of the direct and indirect methods which can be used to study medication adherence to a single psychiatric drug, along with their strengths and weaknesses.
Adherence to Multiple Oral Psychiatric Medications in Large Samples
Objective methods such as blood levels or pill counts are not possible in countries with limited resources and are not practical when dealing with patients who may be taking as many as 6 psychiatric medications at the same time; each patient could adhere differently to the various medications prescribed. This type of study was not possible until the introduction of the Sidorkiewicz adherence tool, which uses self-report of adherence to each medication.48 This tool has five questions and each question has two or three possible answers. The tool uses non-threatening language to reduce social desirability bias and features practical examples and pictographs to help patients recognize their medicine-taking behaviors. The instrument defines six medication adherence levels for a given medication which are dichotomously classified as adherence (levels 1–3) or non-adherence (levels 4–6, ranging from poor medication adherence to discontinuation).48
On 09/10/20 a PubMed search using “Sidorkiewicz adherence” provided 8 articles, of which 4 were on psychiatry.44,49–51 All of them were from our group, so no other psychiatric researcher has yet published results using this adherence tool.
Adherence to LAI Antipsychotic Medications
As indicated in the introduction: 1) schizophrenia experts recommend using LAI antipsychotics to decrease the risk of non-adherence and 2) some experts are also promoting the use of LAI antipsychotics for the maintenance of bipolar disorder, although the benefits are less well established.
Measuring LAI adherence is conceptually different that measuring adherence to oral medications since the only issue is whether or not the patient comes to receive the injection. Thus, patients on LAI may need to be considered separately when considering representativeness in schizophrenia samples. On the other hand, the use of LAI antipsychotics across different countries is extremely variable52,53 and is probably influenced by medical, pharmaceutical and legal issues. Clinical experience and training on the use of LAI appears to be quite variable among psychiatrists across different countries. Moreover, different countries have different levels of access to different LAI compounds. First-generation compounds tend to be cheap while second-generation compounds tend to be expensive. Many states in the USA and some other countries54 offer involuntary outpatient or community treatment laws that may facilitate the use of LAIs, but these forced outpatient treatment orders are not present in many European countries which, on the other hand, offer easy access to free psychiatric treatment including free medications.
Limitations When Using Clinical Sampling
Our three-country study has opened our eyes to the limitations when clinical sampling is used for the study of adherence. Any study using self-report of adherence in clinical samples is “doomed” from the start since patients who not sign the consent form will not be included. Although in our studies, the research staff who helped patients access our study are not directly involved in patient care, it cannot be ruled out that patients who are less adherent may be less cooperative in signing a consent form for a medication adherence study.
Argentina and Venezuela have very fragmented health systems with limited access for those individuals with limited resources. In Spain we have focused on a catchment area within the national health system, which offers free universal treatment, such that any individual who wants to receive voluntary treatment with psychiatric medications has access to it; there are no community outpatient laws and very limited LAI use since patients prefer oral medications. The most non-adherent patients from this catchment area probably are the ones who have not come for treatment for years. No data exists in our Spanish catchment area concerning how many schizophrenia patients do not come for treatment. Finland has a free universal health system similar to that of Spain and has a national database. A national cohort in Finland indicated that, on average, up to 30% of schizophrenia treatment years may not include antipsychotic treatment.55 We are not aware of similar estimations in European countries for bipolar disorder or major depression.
Predicting Adherence: Variables Possibly Associated with Adherence
There is general agreement that adherence to psychiatric treatments is a really complex multidimensional phenomenon influenced by various factors that interact and lead to individual health behaviors.56 In high-quality healthcare systems that guarantee universal full coverage for all citizens, treatment adherence is determined by the interplay of patient-related, disorder-related, and medication-related factors. Although research on treatment adherence is inherently biased due to numerous methodological limitations, significant findings that are consistently identified across studies likely reflect valid associations with relevant clinical implications.57 Moreover, tolerability and efficacy of psychiatric drugs and, therefore, outcomes of mental disorders are not only determined by the medication’s pharmacological profile but also through the interaction of additional factors, including the doctor–patient relationship and the patients’ attitudes toward their illnesses and toward their prescribed medications.58
Although the literature does not provide consistent findings of which variables may predict adherence in psychiatric patients,59 we have tried to summarize the findings in Table 2,60–64 by including 5 systematic reviews and/or meta-analyses that have attempted to identify predictors of treatment adherence in psychiatric disorders. In order to review these predicting variables, we have classified them into four subsections: sociodemographic variables, clinical variables in mental disorders, medication variables, and self-reported health beliefs.
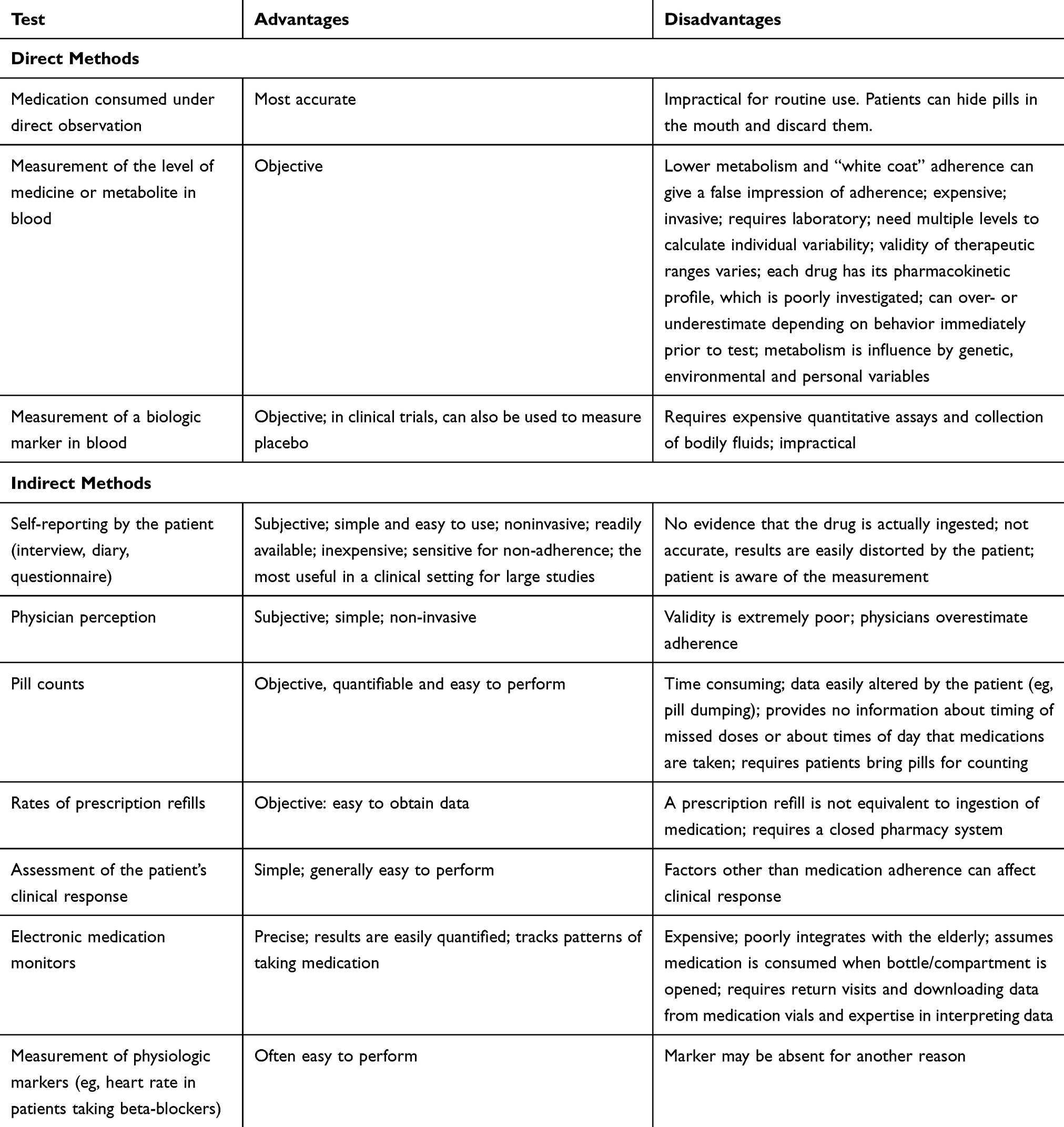 |
Table 1 Methods to Assess Adherence to Oral Medications |
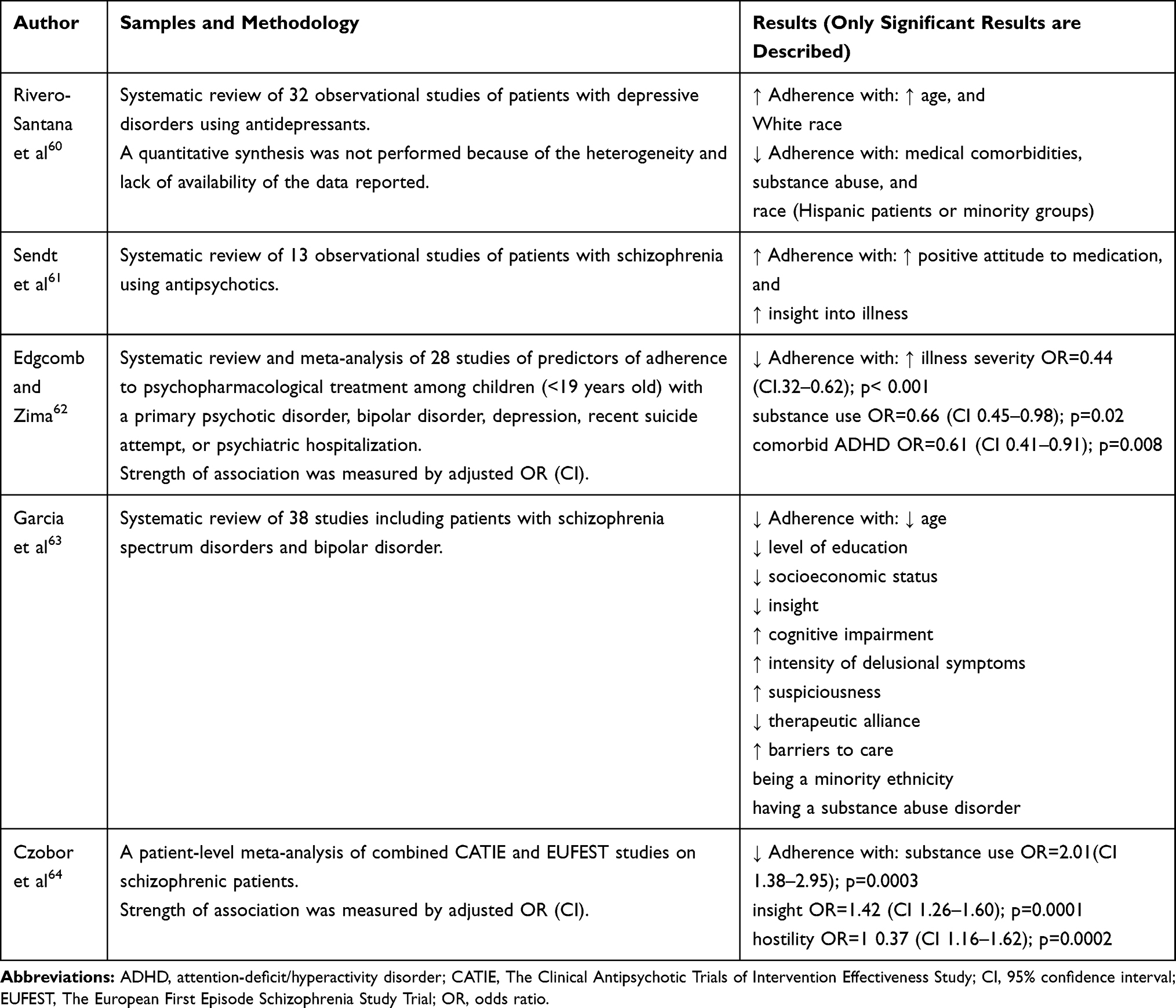 |
Table 2 Systematic Reviews of Sociodemographic and Clinical Predictors of Adherence with Prescribed Psychiatric Treatment |
Sociodemographic Variables as Predictors of Adherence
The idea that sociodemographic variables are the sole determinants of adherence is discredited by evidence that a patient’s level of adherence may vary widely over time but most sociodemographic variables are relatively stable.65 Not surprisingly, Table 2 shows no consistent effects of sociodemographic variables on adherence. The only variable that changes remarkably over time is age, although one systematic review of adherence to antidepressants associated increased age with increased adherence, while another in schizophrenia and bipolar disorder reports the opposite.
Clinical Variables in Mental Disorders as Predictors of Adherence
Table 2 indicates that clinical variables produced conflicting and inconsistent findings with relatively weak associations. The most consistent findings are that 3/5 of the reviews indicate that substance use disorders and poor insight are associated with poor adherence. The problem with using substance use disorders as a predictor is that they vary enormously from country to country and from culture to culture but it appears reasonable that in those countries with substantial prevalence, active substance abuse is an important factor independent of lack of adherence in psychiatric patients. Once substance abuse has ceased, the treatment of the severe mental illness and medication adherence can become the focus.
The third more consistent clinical variable is that measures of increased severity within a disorder may decrease adherence; this appears to happen in patients with depression,60 children62 and patients with schizophrenia and bipolar disorder.63 Interestingly, we could not find any systematic review that compared adherence across the three severe mental illnesses: schizophrenia, bipolar disorder and depression. The expert review in schizophrenia with a heavy emphasis on LAI antipsychotics to avoid non-adherence appears to imply that non-adherence may be a greater problem in schizophrenia, but we cannot find any study supporting this widely held belief. As indicated, the problem is that it is not easy to study adherence from a public health point of view unless one has access to a comprehensive national registry.
Medication Variables as Predictors of Adherence
The studies focused on a class of medication are contaminated by diagnoses, meaning that adherence to antidepressants tend to be studied in patients with depression while adherence to antipsychotics tend to be studied in patients with schizophrenia. As psychiatric patients tend to have comorbidities and are prescribed many psychiatric medications beyond the specific medication for that diagnosis, it would be interesting to know whether patients with a main diagnosis tend to have varying adherence levels across medication classes or not. Patients with bipolar disorder frequently receive mood stabilizers and antipsychotics during maintenance treatment. It would be interesting to know whether the level of adherence and the predictors of adherence are the same or not, but we cannot find studies in the literature considering that approach.
Self-Reported Health Beliefs as Predictors of Adherence
Medication adherence in psychiatric patients may be influenced by health beliefs that are provided by the patients when they are asked. The self-reported health beliefs can refer to the patient or to a specific medication.
Self-Reported Health Beliefs Regarding the Patient
Health psychologists developed the health belief model (HBM)66–68 to explain and predict health-related behaviors (Box 1). There are 3 self-reported health beliefs that may be relevant for medication adherence: first, the attitude towards medication in general, second, the health locus of control (HLOC), which refers to who is responsible for the management of a patient’s disorders, and third, psychological reactance.
Positive and negative attitudes toward medication in general are usually measured by the Drug Attitude Inventory-10 (DAI-10).69 After a complex transformation70 this led to the concepts of pharmacophobia, or fear of the use of pharmacological treatments, and pharmacophilia, or a positive attitude toward using or testing medications (Box 1). The association between more positive attitudes toward medication and higher adherence to prescribed treatments has been revealed in numerous studies in psychiatric patients.71–76 Table 2 shows that one of the systematic reviews61 of adherence in schizophrenia lists this association.
The HLOC dimension is measured by a scale called the Multidimensional HLOC.77 In psychiatric patients, two HLOC dimensions are important: internal HLOC and doctor HLOC, in which either the patient or the doctor is responsible for the management of the disorders (Box 1).78–80 Our research on this topic has shown that psychiatric outpatients have the conviction that their psychiatrists have greater influence on their mental health status even though they were, at the same time, aware of the efficacy of their own activities in coping with their mental disorder. Those psychiatric patients with low internal and external HLOC beliefs described greater adherence to treatment, while patients with high internal and external HLOC beliefs described lower adherence.81
Psychological reactance is defined precisely in Box 1,82–86 but a simplified version is an emotional reaction toward rules perceived as a threat; it is typically measured using the Hong Psychological Reactance Scale.86 In psychiatric outpatients, those who are more prone to reactance tend to show decreased adherence to prescribed treatment.87,88
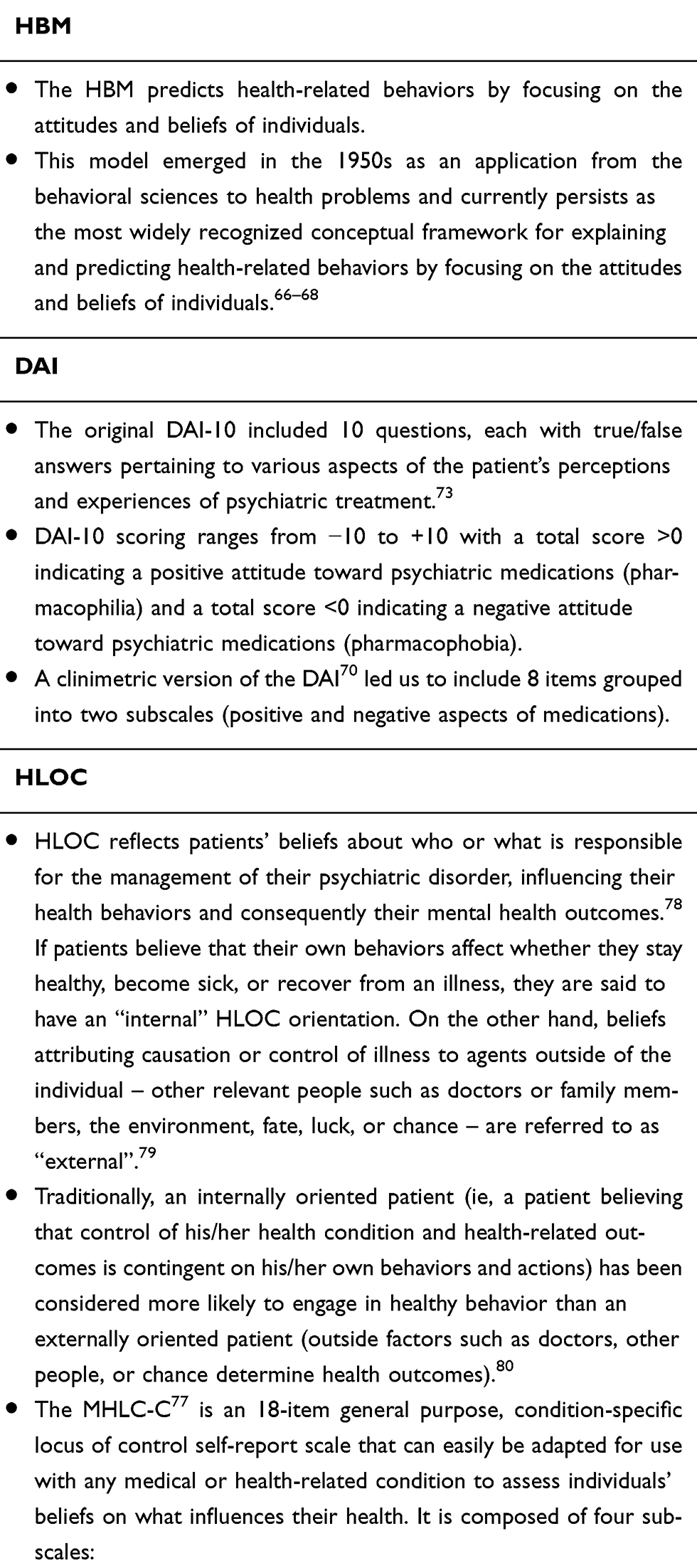 |
Box 1 HBM and Medication Adherence |
To complete these three scales (DAI-10, Multidimensional HLOC and Hong Psychological Reactance Scale), which refer to the health beliefs of the patient, requires from 1 to 1.5 hours of the patient’s time. Thus, we have developed the Patient Health Beliefs Questionnaire on Psychiatric Treatment50 which summarizes the most important aspects and only requires 15 minutes. Patients are asked to rate, on a 6-point Likert scale (from 1, totally disagree, to 6, totally agree), the degree to which they agree or disagree with each statement. Higher scores on each subscale indicate a stronger belief. It includes major items from the 3 scales and has 5 subscales: 1) positive aspects of medication, 2) negative aspects of medication 3) psychological reactance, 4) internal HLOC, and 5) doctor HLOC.50
Health Beliefs Toward Specific Medications
Two key beliefs of patients have been found to have utility in explaining non-adherence to specific medications in psychiatric disorders: perceptions of personal need for treatment (necessity beliefs) and concerns about a range of potential adverse consequences (concern beliefs).89 This Necessity-Concern Framework (NCF) asserts that patients implicitly weigh the costs against the benefits of taking a medication when deciding whether or not to adhere to it and that medication adherence will be greater the more a patient’s beliefs in the necessity of the medication exceed his/her concerns.90
A meta-analytic review of the NCF to assess its utility in explaining nonadherence to prescribed medicines showed that higher adherence was associated with stronger perceptions of the necessity of treatment (OR = 1.74, 95% CI [1.57, 1.9], p=0.0001) and fewer concerns about treatment (OR = 0.504, 95% CI: [0.450, 0.564], p=0.0001); these relationships remained significant when data were stratified by study size, type of adherence measure used and country.89
The NCF can best be explored by using The Beliefs about Medicines Questionnaire (BMQ).91 The BMQ-Specific scale includes 10 items on two subscales, each with five items assessing patients’ beliefs about the medication they were prescribed for a specific illness in terms of necessity and concern about taking it. The degree of agreement with each statement is indicated on a 5-point Likert scale, ranging from 1 (strongly disagree) to 5 (strongly agree). Patients can be categorized into attitudinal groups based on their beliefs about their psychiatric medications.92 The Necessity and Concerns scores can be split at the median to generate four attitudinal groups: Accepting (high necessity, low concern), Ambivalent (high necessity, high concern), Indifferent (low necessity, low concern), and Skeptical (low necessity, high concern).93 In our studies, we have found that the NCF is better summarized by a dichotomous measure, the presence or absence of skepticism about that specific drug.
Although it has never been systematically studied, skepticism about a specific drug is probably partly explained by past experiences. According to Chang et al94 decisions patients make about new prescriptions are dependent on pre-existing beliefs and expectations rather than based on objective interpretations of health information. Dolovich et al95 proposed that past experiences with medications and relationships with health-care providers influenced patients’ expectations of their medications. Horne et al91 showed that patients’ pre-existing beliefs about treatment influence their evaluation of the new prescriptions and their adherence. There is need for studies exploring the relationship between past and present experiences with specific medications and skepticism about them.
Our Studies on Medication Adherence and on Antipsychotic Pharmacokinetics
The first author started almost 10 years ago conducting studies of medication adherence, particularly in relatively stable psychiatric patients, which led to a collaboration with the second author in the last 4 years. The second author has spent 25 years conducting pharmacokinetics studies of psychiatric drugs, particularly antipsychotics, which recently led him to explore the pharmacological complexity of non-adherence.
Predictors of Medication Adherence in Our Studies of Relatively Stable Psychiatric Outpatients
Table 3 describes our 3 largest non-overlapping studies44,80,96 of these predictors.
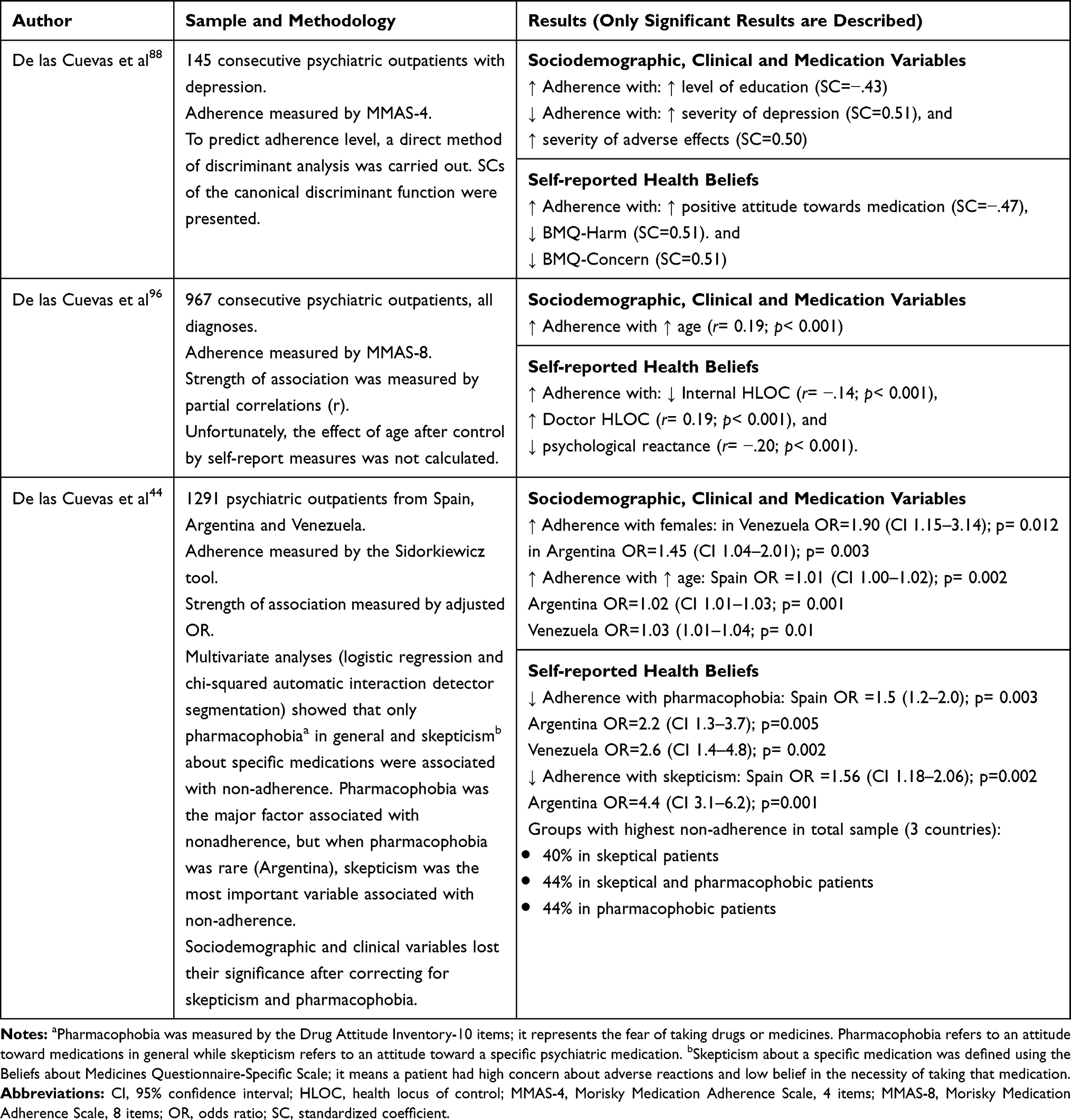 |
Table 3 Our Studies in Medication Adherence of Psychiatric Medication in Outpatients That Analyzed Sociodemographic (Gender, Age and Educational Level) Variables, Clinical Variables (Psychiatric Diagnosis), Medication Variables (Class, Treatment Duration, Polypharmacy), and Self-Reported Health Beliefs |
Sociodemographic Variables as Predictors of Adherence
Table 3 demonstrates that our research on the role of sociodemographic variables in medication adherence has led to inconsistent results. Among them, only age and level of education appeared to be frequently related to treatment adherence. While older age increases adherence, lower educational level decreases adherence. Our experience gained from the studies shown in Table 3 suggests that some of the effects of different levels of education or gender probably just reflect different levels of self-reported health beliefs based on gender, education or age.
Clinical Variables as Predictors of Adherence
Table 3 shows that our research on the role of clinical variables in medication adherence has found that these variables are rarely significant. Only one study in depressive patients showed adherence decreasing as clinical severity increased. On the other hand, it is very likely that our stable patients do not include active substance users who are treated using other resources specific for substance users; therefore, medication adherence in our studies was not contaminated by obvious active substance use. We plan to study whether the effects of self-reported health beliefs on adherence vary based on the main diagnosis: schizophrenia, bipolar disorder and major depression.
Medication Variables as Predictors of Adherence
Table 3 demonstrates that our research on the role of medication variables in medication adherence has found that these variables are rarely significant. Only one study in depressive patients showed adherence decreasing as adverse effects increased. Neither the class of psychiatric drug nor duration of use had been a significant predictor of adherence behavior, but our studies had been limited by never exploring in a large sample whether or not drug variables may become significant within diagnostic groups.
Self-Reported Health Beliefs as Predictors of Adherence
The studies shown in the last row of Table 3 suggest that pharmacophobia in general and skepticism about a specific drug may be the best predictors of poor adherence, but one has to take into account that some countries may have very low levels of pharmacophobia, probably causing skepticism to become more important in that country. Future studies will need to consider whether the combination of psychological reactance and HLOC may be more relevant in specific psychiatric disorders.
Pharmacokinetic Studies and Adherence in Psychiatric Patients
The second author has spent 25 years97 conducting pharmacokinetic studies by using what psychiatrists call blood levels and pharmacologists call therapeutic drug monitoring (TDM) in order to establish which genetic,98 environmental99 and personal variables100 govern the relationship between dosages and serum concentrations of each psychiatric drug. Most of his studies have observed inpatients taking medications under close supervision, so he has been able to assume that most patients were consistently adherent.101
Clozapine has a very peculiar place in psychiatry because it is a very effective drug in treatment-resistant schizophrenia. In spite of its complex toxicological profile, when properly used it decreases the mortality of patients with treatment-resistant schizophrenia.102 The next 3 subsections include a summary of the second author’s studies on clozapine non-adherence in reference to clinical relevance, half-life and TDM.
Clozapine Non-Adherence and Clinical Relevance
The pharmacological effects of antipsychotic non-adherence vary from acute treatment to relapse prevention during maintenance treatment. Sudden antipsychotic discontinuation during the acute treatment phase probably causes rapid relapse as most antipsychotics are completely eliminated from the body in one week. It is quite more complicated to predict the effects of sudden antipsychotic discontinuation once the patient is stable under treatment maintenance, since some patients may relapse but others may not or take many months to relapse.
Patients with treatment-resistant schizophrenia are ideal candidates for studying the effect of non-adherence since most of them need continuous antipsychotic treatment to avoid harm to self or others. Moreover, clozapine is frequently used for both acute and maintenance treatments in these patients, making it perhaps the ideal drug for a study of antipsychotic non-adherence. In fact, clozapine has a peculiar pharmacodynamic103 and pharmacokinetic profile,104 and when patients who are consistently taking it decide to stop suddenly, this non-adherence can manifest with serious clozapine withdrawal syndromes including cholinergic rebound,105 worsening of psychosis and motor symptoms,106 or appearance of never-manifested symptoms such as catatonia.107
Clozapine Non-Adherence and Half-Life
The relationship between non-adherence and decreased clozapine TDM levels is governed by the concept of half-life. Pharmacokinetic textbooks108 usually state that five half-lives are required to 1) reach steady state after starting a dose and, 2) to eliminate 95% of the serum drug concentrations once steady state has been reached and the drug is stopped. The literature on how to establish clozapine half-life in the average clozapine patient and in a specific clozapine patient is not straightforward.
Pharmacokinetic clozapine studies usually have been conducted using single dosing,109 but this design is not a good representation of clozapine half-life in the clinical environment after repeated dosing. The clozapine package insert in the US110 proposes that after repeated dosing average clozapine half-life is 12 hours. This relatively short half-life is not compatible with the possibility of single-day administration.102 As the matter of fact, by using drug discontinuation in the clinical environment, the second author obtained a half-life of 17 hours in one patient and 34 hours in another.104 Clozapine is lipophilic and deposits in the fat tissue111 which explains the dramatic increase in clozapine half-life after repeated dosing.109
In the clinical environment, the problem is the half-life that governs clozapine elimination after discontinuation is not average clozapine half-life, but rather the individual’s clozapine half-life, which varies according to the metabolic characteristics of each patient. Pharmacogenetic science was developed by first establishing that some patients had very high concentrations when given an average dosage; they were called poor metabolizers (PMs). Conversely, other patients had non-detectable concentrations with average doses; they were called ultrarapid metabolizers (UMs).112
Thus, according to pharmacokinetic science PMs are characterized by having extremely long half-lives and very high concentration-to-dose (C/D) ratios. On the other hand, UMs are characterized by having extremely short half-lives and very low C/D ratios. The application of this principle to clozapine is facilitated because in therapeutic doses clozapine follows linear kinetics, which means the relationship between concentrations and doses is stable; the clozapine C/D ratio is a constant in a specific individual unless it is modified by an environmental variable.112 Complexity ensues, however, because: 1) estrogens are inhibitors of clozapine metabolism, meaning that females have higher clozapine C/D ratios; 2) smoking is an inducer of clozapine metabolism, meaning that non-smokers have higher C/D ratios; and 3) Asians have lower clozapine metabolism, meaning that Asians have higher clozapine C/D ratios. In summary, to classify a clozapine patient as PM or UM one has to define ranges after stratifying for gender, smoking and ethnicity.112
Clozapine Non-Adherence and TDM
The second author has reviewed thousands of clozapine TDMs in hundreds of inpatients under standard conditions and, regarding establishing non-adherence, he can provide a basic scientific principle and some recommendations. The basic principle is that any clozapine TDM, to be easily interpreted, has to be steady state: the clozapine dosage must not have been changed for at least 1 week (>5 half-lives) and must have been drawn early in the morning before taking any clozapine dosage (at least 12 hours after the last dosage).
Recommendations on interpreting non-adherence vary among the following: 1) inpatient with many repeated clozapine TDMs, 2) outpatient with repeated clozapine TDMs and 3) outpatient with no prior clozapine TDM.
When the second author studies inpatients who are supervised by nurses during clozapine intake and live under controlled conditions including a stable smoking routine, he always calculates a mean C/D ratio in that specific patient based on at least 3–4 TDMs. Non-adherence should be suspected when a clozapine C/D ratio decreases more than half than the mean C/D ratio of prior TDMs from that specific patient and there is no alternative explanation (discontinuation of an inhibitor or addition of an inducer).113
If the patient is outpatient and even when multiple clozapine TDMs are available, the unresolved issue is how many of the collected measures are contaminated by non-adherence. Thus, one needs to review all changes in medications, caffeine intake, smoking or infections, and use common sense to eliminate values that appear suspicious. Then, use remaining values to calculate the mean C/D ratio which may represent clozapine metabolism in that patient and which can be used for future comparisons.
If there are no prior measures, it is extremely difficult to establish non-adherence. In that case, the second author compares the clozapine C/D ratio with those he has found among clozapine UMs, according to their definitions after stratification by gender, smoking status and ancestry.112 As a general principle, any very low clozapine C/D ratio compatible with being a UM in the absence of inducers (eg, carbamazepine or valproate) is likely to be explained by non-adherence.114
In summary, despite 25 years of research on clozapine TDM, the second author cannot provide any simple advice on how to use clozapine TDM to identify non-adherent patients. Furthermore, as will be discussed in the section on future studies, the use of TDM to predict the effects of or to identify non-adherence for other psychiatric drugs appears much more complicated. In a published editorial, the first and second authors acknowledged that the distinction between non-adherent patients and UMs is more an art than a science.115 Furthermore, they agree that if they were provided all the money and technology currently available they do not have enough knowledge to use TDM of 80 different psychiatric drugs to reliably determine non-adherence in their three-country study that included 1372 patients taking 2454 psychiatric medications.
Future Studies
We are planning future studies in psychiatric patients on predictors of medication adherence and the use of TDM to explore non-adherence.
Future Studies on Predictors of Medication Adherence
We are planning future psychiatric studies in outpatients focused on insight and studies in inpatients.
Future Studies of Insight in Outpatients
Our outpatient studies of adherence to medication in psychiatric patients have not explored the role of the complex topic called “insight” which may include patients’ recognition of having a psychiatric disorder and awareness that treatment could be helpful. There is general agreement that insight into mental illness is a multi-dimensional complex construct that can be impaired in many, if not all, mental disorders.116 The scientific literature indicates a strong link between impaired insight and nonadherence to psychiatric medication.117,118 For this reason, in order to increase the validity of the adherence tool when we first published it, we proposed the incorporation of a new Insight subscale into the questionnaire.50 The insight literature frequently focus in schizophrenia and includes 3 relevant components: 1) awareness of having an illness, 2) attribution of one’s symptoms to the illness and 3) acknowledgment of a need for treatment. The second component (attribution of one’s symptoms to the illness) was not included in our insight subscale because varies from schizophrenia to other psychiatric disorder. On the other hand, we included the need to see a psychiatrist (rather than the family doctor) as an attempt to assess one step further toward insight into mental illness. In our ongoing studies, patients are being asked to rate, on a 6-point Likert scale, the degree to which they agree or disagree with each statement, from strongly disagree to strongly agree. In summary, the principles governing the design of this subscale are that insight: 1) is relevant for all psychiatric disorders, 2) is measured as a continuum, and 3) involve 3 components (awareness of having an illness, acknowledgment of a need for treatment and the need to see a psychiatrist).
Future Studies in Acute Inpatients
As we have seen, self-report measures of health beliefs play a valuable role in predicting adherence, but their validity depends upon the individuals’ willingness and ability to accurately report their experiences. Patients in an acute phase of a mental illness, particularly although not exclusively psychotic disorders, usually present a deteriorated perception of reality and are often characterized by a lack of awareness and poor insight. Nevertheless, according to Bell et al119 self-report psychological testing instruments may be valid even when patients lack awareness of their illness, awareness of the need for treatment, or awareness of the consequences of their illness. During hospitalization in a psychiatric ward, medication-taking behavior is closely supervised by medical personnel and medication adherence approaches 100%, but after hospital discharge treatment adherence tends to decrease over time.20
With this set of limitations, future studies of acute psychiatric inpatients may have no options other than exploring adherence once the patients are stable and ready to be discharged. As a matter of fact, predischarge planning programs are considered important in assisting patients to take charge of their illness, become partners in the treatment process, reduce the likelihood of readmission120 and at the same time become educated concerning medications and encouraged toward medication adherence.121 It is possible that this predischarge moment would be an opportune time to study the self-reported dimensions in order to predict future adherence in outpatient settings. As far as we know, there are no studies of these self-report measures at the time of discharge.
Future Studies of TDM and Non-Adherence
We are planning further studies on clozapine TDM and non-adherence. Then, we comment on the greater complexity involved in studying the relationship between non-adherence and TDM of other antipsychotic or other psychiatric drugs.
Future Studies of Clozapine TDM and Non-Adherence
We have started to explore non-adherence in clozapine outpatients through the use of large databases of repeated samples by collaborating with some of the leaders in outpatient TDM.122 Regarding the use of single clozapine TDM to establish non-adherence, the first step is to further extend the criteria of low clozapine C/D ratios after stratification by gender and smoking from Asians114 to Caucasians. In a second step, we think that there is potential for using the metabolite norclozapine,123 which appears to have a longer half-life than clozapine.
Future Studies of TDM Based on Other Antipsychotics and Non-Adherence
These are interesting times to use TDM to establish non-adherence in antipsychotics other than clozapine since the literature is starting to 1) acknowledge its relevance, 2) pay attention to a TDM guideline, and 3) include interest on the part of commercial companies. On the other hand, we comment on the complexity of moving forward in this area.
Many authors33,124 are starting to acknowledge that many of the schizophrenia patients considered treatment-resistant by their psychiatrists are merely non-adherent. It is very clear that when a patient is taking doses that are therapeutic in an average patient and has no detectable serum concentrations using a well-validated method, the patient is obviously non-compliant. It is much more complicated when the serum concentrations are low. A major step occurred in 2004,125 when a group of experts published the first TDM guideline providing lower and upper therapeutic ranges for many psychiatric drugs. In 2018,126 the third version of this guideline was published and this version has received much more attention to the point that a modified section of the antipsychotic TDM guideline was published in a journal targeting clinicians.127 In summary, most psychiatrists would agree that when a patient has a serum concentration below the therapeutic range for this antipsychotic, the dosage should be increased and another TDM obtained before considering the patient treatment-resistant to that antipsychotic. On the other hand, it is much more complicated to establish how to diagnose non-adherence based on subtherapeutic concentrations of a specific antipsychotic, since it may be explained by pharmacokinetic confounders.
To diagnose a low C/D ratio as compatible with non-adherence there is need for a thorough understanding of the pharmacokinetic variables influencing drug clearance and the C/D ratio of each specific antipsychotic. After clozapine, oral risperidone and oral paliperidone are the antipsychotics of which we are most knowledgeable,101 but the literature on C/D ratios show some discrepancies between some European labs and the US and other European labs for oral risperidone128 and between Korean and non-Korean studies of oral paliperidone.129 The literature on C/D ratios of LAI risperidone128 and paliperidone130 is limited by little data and lack of knowledge of the half-life of the different formulations.131 The use of olanzapine and quetiapine C/D ratios in clinical practice is just starting.132 Most other second-generation antipsychotic TDM science is too underdeveloped to firmly establish therapeutic ranges.126
Until recently, antipsychotic TDM held no interest for pharmaceutical companies and was only studied by independent investigators with limited funding, who frequently used naturalistic designs from TDM outpatient databases that offered limited access to clinical information. More recently, some commercial companies133 began introducing new commercial TDM methods that can provide same-day data even to outpatient facilities. Such a system has been marketed first for clozapine.134 Both the interest of commercial companies in this area and the development of new TDM technologies are excellent pieces of news, but increase the risk of promoting non-validated practices such as using antipsychotic concentrations in urine to detect non-adherence.135 Renal drug elimination of any antipsychotic and its metabolites is an extremely complex and poorly understood topic.
Future Studies of TDM Based on Other Psychiatric Drugs and Non-Adherence
Antidepressant TDM is reviewed by the expert guideline,126 but there is little information on second-generation antidepressants and some of them, such as paroxetine and fluoxetine, definitively inhibit their own metabolism, making the interpretation of their C/D ratios very complicated. Their C/D ratios do not follow linear kinetics,136 and the C/D ratio is not constant in an individual patient since it varies with the dosage.
TDM of mood stabilizers is reviewed by the expert guideline.126 Most psychiatrists agree that lithium TDM is well established, but it is more complicated for those mood stabilizers which are also antiepileptic drugs and have complicated pharmacokinetics.136 Carbamazepine does not follow linear kinetics due to auto-induction.132 Valproate TDM is severely neglected and very complicated since the total serum valproate concentrations do not follow linear kinetics due to protein displacement137 and its auto-induction has received almost no attention.138
Most TDM experts will probably agree that we are very far from being able to use serum TDM to diagnose non-adherence in patients taking antidepressants or mood stabilizers. Most patients with non-detectable serum concentrations taking therapeutic dosages are likely to be non-adherent. On the other hand, it is a very humbling experience to remember that the concept of UM was introduced in medicine when a group of Swedish psychiatrists observed 2 families with several members taking tricyclic antidepressants (TCAs). They found repeated non-detectable serum concentrations in spite of reassurance by the patients and families that the patients were taking the TCAs. A gene study of the metabolic enzyme explained that these 2 families have multiple active copies of the gene, leading to the first description of the genetic UMs.139
Our conclusion after 25 years of conducting pharmacokinetic studies in psychiatric drugs is that we have limited understanding of how to use blood levels to predict the effects of non-adherence or to establish it. The next 25 years should bring much better understanding if systematic studies are conducted in the real clinical environment.
Expert Opinion on the Complexity of Studying Medication Adherence in Psychiatry
The last two subsections provide our expert opinion on the complexity of adherence due to its dynamic profile and on personalized approaches.
Complexity of Adherence Studies: Adherence Changes Over Time
According to the Common-Sense Theoretical Model of Illness, adherence is a dynamic process that changes over time based on the feedback mechanism between health threats (symptom identification) and appraisal of the coping behavior (taking medications).140 Since the social and environmental contexts of psychiatric patients may change over time, their experiences with and perceptions of their psychiatric disorders and prescribed treatments may also change. These experiences and perceptions can challenge and modify previous beliefs about illness and medications, and therefore their adherence to medicines may change.141 The changes in adherence add complexity to the study of large samples with a cross-sectional design. Any longitudinal study of a non-adherent patient may be made impossible by the lack of collaboration of the most non-adherent patients.
The Need for a Personalized Approach When Studying Adherence
The term personalized medicine or the narrower term personalized prescription may mean different things to different professionals.140 A psychologist may propose that it means using individualized treatment based on the individual psychological characteristics of the patient. A pharmacologist may propose that it means using individualized treatment based on the individual pharmacological characteristics of the patient. Both versions are discussed as our final message on medication adherence in psychiatric patients.
Personalization Based on Psychology with Potential for Improving Non-Adherence
We hope that once we integrate the insight subscale into our Patient’s Health Belief Questionnaire on Psychiatric Treatment50 and also consider skepticism about some specific drugs, this assessment will provide a comprehensive way of measuring self-reported health beliefs as a predictor of non-adherence and, more importantly, develop personalized interventions based on the patient’s reasons for non-adherence. On the other hand, we acknowledge that personalized prescription by using psychological measures from self-report is in its early stages.
Personalization Based on Pharmacology for Preventing Non-Adherence
In our studies, patients frequently explain their non-adherence as skepticism about some specific drugs. We have no definitive proof, but our experience suggests that many cases may be due to lack of consideration of a personalized approach to prescriptions by their psychiatrists. Many patients do not tolerate or respond to average doses and need lower or higher doses, so they may not tolerate an average dose of a specific psychiatric drug very well. We hope as the science of personalized prescription advances and pharmacogenetics and TDM are used to personalize dosing and drug selection,100 the number of patients with this negative experience may be reduced. On the other hand, we acknowledge that personalized prescription by using pharmacological principles is also in its early stages of implementation. We do not recommend current commercial pharmacogenetic tests since they are not validated.98
To conclude our review of the literature and of our studies, as we have previously recognized, our studies have limitations that may bias our opinions. On the issue of the prediction of adherence in psychiatric patients, our reflections are limited by not having taken into consideration the patient’s insight, not having expanded our studies to acute patients admitted to psychiatric wards, and the fact that those related to active substance abuse were not obviously active in our outpatient samples. Finally, we acknowledge we are only starting to understand the pharmacological principles behind the clinical relevance of non-adherence which may be different for different drugs and how TDM can be used in psychiatry to establish their non-adherence or predict its consequences.
Acknowledgments
The authors acknowledge Lorraine Maw, M.A., at the Mental Health Research Center at Eastern State Hospital, Lexington, KY, USA, who helped in editing this article.
Disclosure
No commercial organizations had any role in the completion or publication of this study. The authors declare that they have had no conflicts of interest in relation to the subject of this study.
References
1. De Las Cuevas C. Towards a clarification of terminology in medicine taking behavior: compliance, adherence and concordance are related although different terms with different uses. Curr Clin Pharmacol. 2011;6(2):74–77. doi:10.2174/157488411796151110
2. Aronson JK. Compliance, concordance, adherence. Br J Clin Pharmacol. 2007;63(4):383–384. doi:10.1111/j.1365-2125.2007.02893.x
3. Kelley M. Limits on patient responsibility. J Med Philos. 2005;30(2):189–206. doi:10.1080/03605310590926858
4. Sabaté E. Adherence to Long-Term Therapies: Evidence for Action. Geneva (Switzerland): World Health Organization; 2003.
5. Leucht S, Hierl S, Kissling W, Dold M, Davis JM. Putting the efficacy of psychiatric and general medicine medication into perspective: review of meta-analyses. Br J Psychiatry. 2012;200(2):97–106. doi:10.1192/bjp.bp.111.096594
6. Chapman SC, Horne R. Medication nonadherence and psychiatry. Curr Opin Psychiatry. 2013;26(5):446–452. doi:10.1097/YCO.0b013e3283642da4
7. Bulloch AG, Patten SB. Non-adherence with psychotropic medications in the general population. Soc Psychiatry Psychiatr Epidemiol. 2010;45(1):47–56. doi:10.1007/s00127-009-0041-5
8. Morken G, Widen JH, Grawe RW. Non-adherence to antipsychotic medication, relapse and rehospitalisation in recent-onset schizophrenia. BMC Psychiatry. 2008;8(1):32. doi:10.1186/1471-244X-8-32
9. San L, Bernardo M, Gómez A, Martínez P, González B, Peña M. Socio-demographic, clinical and treatment characteristics of relapsing schizophrenic patients. Nord J Psychiatry. 2013;67(1):22–29. doi:10.3109/08039488.2012.667150
10. Witt K, van Dorn R, Fazel S, Zhang XY. Risk factors for violence in psychosis: systematic review and meta-regression analysis of 110 studies. PLoS One. 2013;8(2):e55942. doi:10.1371/journal.pone.0055942
11. Lindström E, Eriksson L, Levander S. Suicides during 7 years among a catchment area cohort of patients with psychoses. Nord J Psychiatry. 2012;66(1):8–13. doi:10.3109/08039488.2011.577186
12. Ruengorn C, Sanichwankul K, Niwatananun W, Mahatnirunkul S, Pumpaisalchai W, Patumanond J. A risk-scoring scheme for suicide attempts among patients with bipolar disorder in a Thai patient cohort. Psychol Res Behav Manag. 2012;5:37–45. doi:10.2147/PRBM.S30878
13. Cullen BA, McGinty EE, Zhang Y, et al. Guideline-concordant antipsychotic use and mortality in schizophrenia. Schizophr Bull. 2013;39(5):1159–1168. doi:10.1093/schbul/sbs097
14. Joe S, Lee JS. Association between non-compliance with psychiatric treatment and non-psychiatric service utilization and costs in patients with schizophrenia and related disorders. BMC Psychiatry. 2016;16(1):444. doi:10.1186/s12888-016-1156-3
15. Cutler RL, Fernandez-Llimos F, Frommer M, Benrimoj C, Garcia-Cardenas V. Economic impact of medication non-adherence by disease groups: a systematic review. BMJ Open. 2018;8(1):e016982. doi:10.1136/bmjopen-2017-016982
16. Schwab AP. The epistemic responsibilities in medicine of beneficence and respect for patient autonomy. Ethics Med Public Health. 2017;3(2):233–240. doi:10.1016/j.jemep.2017.04.015
17. Almanza M, Romero-Mendoza M, San Luis AG. The process of adherence to treatment in people living with HIV, in “advances in HIV and AIDS control”. IntechOpen. 2018. doi:10.5772/intechopen.77032
18. Kessler RC, Berglund PA, Bruce ML, et al. The prevalence and correlates of untreated serious mental illness. Health Serv Res. 2001;36(6 Pt 1):987–1007.
19. Owiti J, Bowers L. A Literature Review: Refusal of Psychotropic Medication in Acute Inpatient Psychiatric Care. Report from the Conflict and Containment Reduction Research Program. London (United Kingdom): Institute of Psychiatry; 2010.
20. Yalamova IV. Post-discharge medication adherence in schizophrenia. Arch Psychiatry Psychother. 2015;17(4):39–47. doi:10.12740/APP/60513
21. Leucht S, Leucht C, Huhn M, et al. Sixty years of placebo-controlled antipsychotic drug trials in acute schizophrenia: systematic review, Bayesian meta-analysis, and meta-regression of efficacy predictors. Am J Psychiatry. 2017;174(10):927–942. doi:10.1176/appi.ajp.2017.16121358
22. Leucht S, Tardy M, Komossa K, et al. Antipsychotic drugs versus placebo for relapse prevention in schizophrenia: a systematic review and meta-analysis. Lancet. 2012;379(9831):2063–2071. doi:10.1016/S0140-6736(12)60239-6
23. Grande I, Vieta E. Pharmacotherapy of acute mania: monotherapy or combination therapy with mood stabilizers and antipsychotics? CNS Drugs. 2015;29(3):221–227. doi:10.1007/s40263-015-0235-1
24. Miura T, Noma H, Furukawa TA, et al. Comparative efficacy and tolerability of pharmacological treatments in the maintenance treatment of bipolar disorder: a systematic review and network meta-analysis. Lancet Psychiatry. 2014;1(5):351–359. doi:10.1016/S2215-0366(14)70314-1
25. Cipriani A, Furukawa TA, Salanti G, et al. Comparative efficacy and acceptability of 21 antidepressant drugs for the acute treatment of adults with major depressive disorder: a systematic review and network meta-analysis. Lancet. 2018;391(10128):1357–1366. doi:10.1016/S0140-6736(17)32802-7
26. Singh JB, Fedgchin M, Daly EJ, Drevets WC. Relapse prevention in treatment-resistant major depressive disorder with rapid-acting antidepressants. Adv Pharmacol. 2020;89:237–259. doi:10.1016/bs.apha.2020.05.002
27. Velligan DI, Weiden PJ, Sajatovic M, et al. The expert consensus guideline series: adherence problems in patients with serious and persistent mental illness. J Clin Psychiatry. 2009;70(Suppl 4):1–46. doi:10.4088/JCP.7090su1cj
28. Tham XC, Xie H, Chng CM, Seah XY, Lopez V, Klainin-Yobas P. Factors affecting medication adherence among adults with schizophrenia: a literature review. Arch Psychiatr Nurs. 2016;30(6):797–809. doi:10.1016/j.apnu.2016.07.007
29. Kikkert MJ, Dekker J. Medication adherence decisions in patients with schizophrenia. Prim Care Companion CNS Disord. 2017;19(6). doi:10.4088/PCC.17n02182
30. Kane JM, Correll CU. Optimizing treatment choices to improve adherence and outcomes in schizophrenia. J Clin Psychiatry. 2019;80(5). doi:10.4088/JCP.IN18031AH1C
31. Bright CE. Measuring medication adherence in patients with schizophrenia: an integrative review. Arch Psychiatr Nurs. 2017;31(1):99–110. doi:10.1016/j.apnu.2016.09.003
32. Weiden PJ. Redefining medication adherence in the treatment of schizophrenia: how current approaches to adherence lead to misinformation and threaten therapeutic relationships. Psychiatr Clin North Am. 2016;39(2):199–216. doi:10.1016/j.psc.2016.01.004
33. McCutcheon R, Beck K, D’Ambrosio E, et al. Antipsychotic plasma levels in the assessment of poor treatment response in schizophrenia. Acta Psychiatr Scand. 2018;137(1):39–46. doi:10.1111/acps.12825
34. Levin JB, Krivenko A, Howland M, Schlachet R, Sajatovic M. Medication adherence in patients with bipolar disorder: a comprehensive review. CNS Drugs. 2016;30(9):819–835. doi:10.1007/s40263-016-0368-x
35. MacDonald L, Chapman S, Syrett M, Bowskill R, Horne R. Improving medication adherence in bipolar disorder: A systematic review and meta-analysis of 30 years of intervention trials. J Affect Disord. 2016;194:202–221. doi:10.1016/j.jad.2016.01.002
36. Hartung D, Low A, Jindai K, et al. Interventions to improve pharmacological adherence among adults with psychotic spectrum disorders and bipolar disorder: a systematic review. Psychosomatics. 2017;58(2):101–112. doi:10.1016/j.psym.2016.09.009
37. Greene M, Yan T, Chang E, Hartry A, Touya M, Broder MS. Medication adherence and discontinuation of long-acting injectable versus oral antipsychotics in patients with schizophrenia or bipolar disorder. J Med Econ. 2018;21(2):127–134. doi:10.1080/13696998.2017.1379412
38. Boyce P, Irwin L, Morris G, et al. Long-acting injectable antipsychotics as maintenance treatments for bipolar disorder-A critical review of the evidence. Bipolar Disord. 2018;20(Suppl 2):25–36. doi:10.1111/bdi.12698
39. Gentile S. Discontinuation rates during long-term, second-generation antipsychotic long-acting injection treatment: A systematic review. Psychiatry Clin Neurosci. 2019;73(5):216–230. doi:10.1111/pcn.12824
40. Hung CI. Factors predicting adherence to antidepressant treatment. Curr Opin Psychiatry. 2014;27(5):344–349. doi:10.1097/YCO.0000000000000086
41. Rush AJ, Thase ME. Improving depression outcome by patient-centered medical management. Am J Psychiatry. 2018;175(12):1187–1198. doi:10.1176/appi.ajp.2018.18040398
42. Whalley Buono E, Vrijens B, Bosworth HB, Liu LZ, Zullig LL, Granger BB. Coming full circle in the measurement of medication adherence: opportunities and implications for health care. Patient Prefer Adherence. 2017;11:1009–1017. doi:10.2147/PPA.S127131
43. De Las Cuevas C, Peñate W, Sanz EJ. Psychiatric outpatients’ self-reported adherence versus psychiatrists’ impressions on adherence in affective disorders. Hum Psychopharmacol. 2013;28(2):142–150. doi:10.1002/hup.2293
44. De Las Cuevas C, Motuca M, Baptista T, de Leon J. Skepticism and pharmacophobia toward medication may negatively impact adherence to psychiatric medications: A comparison among outpatient samples recruited in Spain, Argentina, and Venezuela. Patient Prefer Adherence. 2018;12:301–310. doi:10.2147/PPA.S133513
45. De Las Cuevas C, Motuca M, Baptista T, Villasante-Tezanos AG, de Leon J. Ethnopsychopharmacology study of patients’ beliefs regarding concerns about and necessity of taking psychiatric medications. Hum Psychopharmacol. 2019;34(2):e2688. doi:10.1002/hup.2688
46. Velligan DI, Maples NJ, Pokorny JJ, Wright C. Assessment of adherence to oral antipsychotic medications: what has changed over the past decade? Schizophr Res. 2020;215:17–24. doi:10.1016/j.schres.2019.11.022
47. Stirratt MJ, Dunbar-Jacob J, Crane HM, et al. Self-report measures of medication adherence behavior: recommendations on optimal use. Transl Behav Med. 2015;5(4):470–482. doi:10.1007/s13142-015-0315-2
48. Sidorkiewicz S, Tran VT, Cousyn C, Perrodeau E, Ravaud P. Development and validation of an instrument to assess treatment adherence for each individual drug taken by a patient. BMJ Open. 2016;6(5):e010510. doi:10.1136/bmjopen-2015-010510
49. De Las Cuevas C, Peñate W, Manuel García de Cecilia J, de Leon J. Predictive validity of the Sidorkiewicz instrument in Spanish: assessing individual drug adherence in psychiatric patients. Int J Clin Health Psychol. 2018;18(2):133–142. doi:10.1016/j.ijchp.2017.11.003
50. De Las Cuevas C, de Leon J. Development and validation of the patient’s health belief questionnaire on psychiatric treatment. Patient Prefer Adherence. 2019;10(13):527–536. doi:10.2147/PPA.S201144
51. De Las Cuevas C, Betancort M, de Leon J. The necessity-concern framework in the assessment of treatment adherence of psychiatric patients and the role of polypharmacy in a Spanish sample. Hum Psychopharmacol. 2020;35(1):e2721. doi:10.1002/hup.2721
52. Tang CT, Chua EC, Chew QH, et al. Patterns of long acting injectable antipsychotic use and associated clinical factors in schizophrenia among 15 Asian countries and region. Asia Pac Psychiatry. 2020;29:e12393. doi:10.1111/appy.12393
53. Bobrovitz N, Heneghan C, Onakpoya I, et al. Medications that reduce emergency hospital admissions: an overview of systematic reviews and prioritisation of treatments. BMC Med. 2018;16(1):115. doi:10.1186/s12916-018-1104-9
54. Corring D, O’Reilly RL, Sommerdyk C, Russell E. What clinicians say about the experience of working with individuals on community treatment orders. Psychiatr Serv. 2018;69(7):791–796. doi:10.1176/appi.ps.201700492
55. Taipale H, Mittendorfer-Rutz E, Alexanderson K, et al. Antipsychotics and mortality in a nationwide cohort of 29,823 patients with schizophrenia. Schizophr Res. 2018;197:274–280. doi:10.1016/j.schres.2017.12.010
56. Irwin M. Theoretical foundations of adherence behaviors: synthesis and application in adherence to oral oncology agents. Clin J Oncol Nurs. 2015;19(3 Suppl):31–35. doi:10.1188/15.S1.CJON.31-35
57. Velligan DI, Sajatovic M, Hatch A, Kramata P, Docherty JP. Why do psychiatric patients stop antipsychotic medication? A systematic review of reasons for nonadherence to medication in patients with serious mental illness. Patient Prefer Adherence. 2017;11:449–468. doi:10.2147/PPA.S124658
58. De Las Cuevas C, Sanz EJ. Attitudes toward psychiatric drug treatment: the experience of being treated. Eur J Clin Pharmacol. 2007;63(11):1063–1067. doi:10.1007/s00228-007-0358-5
59. Semahegn A, Torpey K, Manu A, Assefa N, Tesfaye G, Ankomah A. Psychotropic medication non-adherence and associated factors among adult patients with major psychiatric disorders: a protocol for a systematic review. Syst Rev. 2018;7(1):10. doi:10.1186/s13643-018-0676-y
60. Rivero-Santana A, Perestelo-Perez L, Pérez-Ramos J, Serrano-Aguilar P, De Las Cuevas C. Sociodemographic and clinical predictors of compliance with antidepressants for depressive disorders: systematic review of observational studies. Patient Prefer Adherence. 2013;7:151–169. doi:10.2147/PPA.S39382
61. Sendt KV, Tracy DK, Bhattacharyya S. A systematic review of factors influencing adherence to antipsychotic medication in schizophrenia-spectrum disorders. Psychiatry Res. 2015;225(1–2):14–30. doi:10.1016/j.psychres.2014.11.002
62. Edgcomb JB, Zima B. Medication adherence among children and adolescents with severe mental illness: a systematic review and meta-analysis. J Child Adolesc Psychopharmacol. 2018;28(8):508–520. doi:10.1089/cap.2018.0040
63. García S, Martínez-Cengotitabengoa M, López-Zurbano S, et al. Adherence to antipsychotic medication in bipolar disorder and schizophrenic patients: a systematic review. J Clin Psychopharmacol. 2016;36(4):355–371. doi:10.1097/JCP.0000000000000523
64. Czobor P, Van Dorn RA, Citrome L, Kahn RS, Fleischhacker WW, Volavka J. Treatment adherence in schizophrenia: a patient-level meta-analysis of combined CATIE and EUFEST studies. Eur Neuropsychopharmacol. 2015;25(8):1158–1166. doi:10.1016/j.euroneuro.2015.04.003
65. Horne R. The Nature, Determinants and Effects of Medication Beliefs in Chronic Illness [PhD thesis]. University of London; 1997.
66. Rosenstock IM. Historical origins of the health belief model. Health Educ Monogr. 1974;2(4):328–335. doi:10.1177/109019817400200403
67. Jones CJ, Smith H, Llewellyn C. Evaluating the effectiveness of health belief model interventions in improving adherence: a systematic review. Health Psychol Rev. 2014;8(3):253–269. doi:10.1080/17437199.2013.802623
68. Sulat J, Prabandari Y, Sanusi R, Hapsari E, Santoso B. The validity of health belief model variables in predicting behavioral change: a scoping review. Health Educ. 2018;118(6):499–512. doi:10.1108/HE-05-2018-0027
69. Hogan TP, Awad AG, Eastwood R. A self-report scale predictive of drug compliance in schizophrenics: reliability and discriminative validity. Psychol Med. 1983;13(1):177–183. doi:10.1017/s0033291700050182
70. De Las Cuevas C, de Leon J. A clinimetric approach for improving the measurement of pharmacophobia with replication in two other samples. Psychother Psychosom. 2019;88(2):116–118. doi:10.1159/000495940
71. Brain C, Allerby K, Sameby B, et al. Drug attitude and other predictors of medication adherence in schizophrenia: 12 months of electronic monitoring (MEMS(®)) in the Swedish COAST-study. Eur Neuropsychopharmacol. 2013;3(12):1754–1762. doi:10.1016/j.euroneuro.2013.09.001
72. Lacro JP, Dunn LB, Dolder CR, Leckband SG, Jeste DV. Prevalence of and risk factors for medication nonadherence in patients with schizophrenia: a comprehensive review of recent literature. J Clin Psychiatry. 2002;63(10):892–909. doi:10.4088/jcp.v63n1007
73. Day JC, Bentall RP, Roberts C, et al. Attitudes toward antipsychotic medication: the impact of clinical variables and relationships with health professionals. Arch Gen Psychiatry. 2005;62(7):717–724. doi:10.1001/archpsyc.62.7.717
74. Moritz S, Peters MJ, Karow A, Deljkovic A, Tonn P, Naber D. Cure or curse? Ambivalent attitudes towards neuroleptic medication in schizophrenia and non-schizophrenia patients. Ment Ill. 2009;1(1):4–9. doi:10.4081/mi.2009.e2
75. De Las Cuevas C, Peñate W. Explaining pharmacophobia and pharmacophilia in psychiatric patients: relationship with treatment adherence. Hum Psychopharmacol. 2015;30(5):377–383. doi:10.1002/hup.2487
76. De Las Cuevas C, Peñate W, Sanz EJ. Risk factors for non-adherence to antidepressant treatment in patients with mood disorders. Eur J Clin Pharmacol. 2014;70(1):89–98. doi:10.1007/s00228-013-1582-9
77. Wallston KA, Stein MJ, Smith CA. Form C of the MHLC scales: a condition-specific measure of locus of control. J Pers Assess. 1994;63(3):534–553. doi:10.1207/s15327752jpa6303_10
78. Wallston KA, Wallston BS. Who is responsible for your health? The construct of health locus of control. In: Sanders G, Suls J, editors. Social Psychology of Health and Illness. Hillsdale (NJ): Lawrence Erlbaum and Associates; 1982.
79. Wallston KA. Assessment of control in health-care settings. In: Steptoe A, Apples A, editors. Stress, Personal Control and Health. New York: John Wiley & Son; 1989.
80. Nazareth M, Richards J, Javalkar K, et al. Relating health locus of control to health care use, adherence, and transition readiness among youths with chronic conditions, North Carolina, 2015. Prev Chronic Dis. 2016;21:
81. De Las Cuevas C, Peñate W, Cabrera C. Perceived health control: a promising step forward in our understanding of treatment adherence in psychiatric care. J Clin Psychiatry. 2016;77:e1233–e1239. doi:10.4088/JCP.15m09769
82. Rosenberg BD, Siegel JT. A 50-year review of psychological reactance theory: do not read this article. Motiv Sci. 2017;4(4):281–300. doi:10.1037/mot0000091
83. Reynolds-Tylus T. Psychological reactance and persuasive health communication: a review of the literature. Front Commun. 2019;4(56):1–12. doi:10.3389/fcomm.2019.00056
84. Brehm JW. A Theory of Psychological Reactance. New York, NY: Academic Press; 1966.
85. Steindl C, Jonas E, Sittenthaler S, Traut-Mattausch E, Greenberg J. Understanding psychological reactance: new developments and findings. Z Psychol. 2015;223(4):205–214. doi:10.1027/2151-2604/a000222
86. Hong S-M, Faedda S. Refinement of the Hong psychological reactance scale. Educ Psychol Meas. 1996;56(1):173–182. doi:10.1177/0013164496056001014
87. De Las Cuevas C, Peñate W, Betancort M, de Rivera L. Psychological reactance in psychiatric patients: examining the dimensionality and correlates of the Hong psychological reactance scale in a large clinical sample. Pers Individ Dif. 2014;70:85–91. doi:10.1016/j.paid.2014.06.027
88. De Las Cuevas C, Peñate W, Sanz EJ. The relationship of psychological reactance, health locus of control and sense of self-efficacy with adherence to treatment in psychiatric outpatients with depression. BMC Psychiatry. 2014;14(1):324. doi:10.1186/s12888-014-0324-6
89. Horne R, Chapman SC, Parham R, Freemantle N, Forbes A, Cooper V. Understanding patients’ adherence-related beliefs about medicines prescribed for long-term conditions: a meta-analytic review of the necessity-concerns framework. PLoS One. 2013;8(12):e80633. doi:10.1371/journal.pone.0080633
90. Phillips LA, Diefenbach MA, Kronish IM, Negron RM, Horowitz CR. The necessity-concerns framework: a multidimensional theory benefits from multidimensional analysis. Ann Behav Med. 2014;48(1):7–16. doi:10.1007/s12160-013-9579-2
91. Horne R, Weinman J, Hankins M. The beliefs about medicines questionnaire: the development and evaluation of a new method for assessing the cognitive representation of medication. Psychol Health. 1999;14(1):1–24. doi:10.1080/08870449908407311
92. Aikens JE, Nease DE
93. Menckeberg TT, Bouvy ML, Bracke M, et al. Beliefs about medicines predict refill adherence to inhaled corticosteroids. J Psychosom Res. 2008;64(1):47–54. doi:10.1016/j.jpsychores.2007.07.016
94. Chang DS, Kang OS, Kim HH, et al. Pre-existing beliefs and expectations influence judgments of novel health information. J Health Psychol. 2012;17(5):753–763. doi:10.1177/1359105311421044
95. Dolovich L, Nair K, Sellors C, Lohfeld L, Lee A, Levine M. Do patients’ expectations influence their use of medications? Qualitative study. Can Fam Physician. 2008;54(3):384–393.
96. De Las Cuevas C, Peñate W, Betancort M, Cabrera C. What do psychiatric patients believe regarding where control over their illness lies? Validation of the multidimensional health locus of control scale in psychiatric outpatient care. J Nerv Ment Dis. 2015;203(2):81–86. doi:10.1097/NMD.0000000000000244
97. de Leon J. A critical commentary on the 2017 AGNP consensus guidelines for therapeutic drug monitoring in neuropsychopharmacology. Pharmacopsychiatry. 2018;51(1–2):63–68. doi:10.1055/s-0043-117891
98. de Leon J. Pharmacogenetic tests in psychiatry: from fear to failure to hype. J Clin Psychopharmacol. 2016;36(4):299–304. doi:10.1097/JCP.0000000000000522
99. de Leon J. Why do you keep telling me that drug-drug interactions are important in psychopharmacology when I do not see them in my clinical practice?: my failure to convince clinicians. J Clin Psychopharmacol. 2019;39(1):1–4. doi:10.1097/JCP.0000000000000924
100. de Leon J. The future (or lack of future) of personalized prescription in psychiatry. Pharmacol Res. 2009;59(2):81–89. doi:10.1016/j.phrs.2008.10.002
101. de Leon J. Personalizing dosing of risperidone, paliperidone and clozapine using therapeutic drug monitoring and pharmacogenetics. Neuropharmacology. 2020;168:107656. doi:10.1016/j.neuropharm.2019.05.033
102. de Leon J, Ruan CJ, Schoretsanitis G, De Las Cuevas C. A rational use of clozapine based on adverse drug reactions, pharmacokinetics, and clinical pharmacopsychology. Psychother Psychosom. 2020;89(4):200–214. doi:10.1159/000507638
103. Verghese C, De Leon J, Nair C, Simpson GM. Clozapine withdrawal effects and receptor profiles of typical and atypical neuroleptics. Biol Psychiatry. 1996;39(2):135–138. doi:10.1016/0006-3223(95)00215-4
104. de Leon J, Henighan V, Stanilla JK, Simpson GM. Clozapine levels after clozapine discontinuation. J Clin Psychopharmacol. 1996;16(2):193–194. doi:10.1097/00004714-199604000-00016
105. de Leon J, Stanilla JK, White AO, Simpson GM. Anticholinergics to treat clozapine withdrawal. J Clin Psychiatry. 1994;55(3):119–120.
106. Stanilla JK, de Leon J, Simpson GM. Clozapine withdrawal resulting in delirium with psychosis: a report of three cases. J Clin Psychiatry. 1997;58(6):252–255. doi:10.4088/jcp.v58n0603
107. Bilbily J, McCollum B, de Leon J. Catatonia secondary to sudden clozapine withdrawal: a case with three repeated episodes and a literature review. Case Rep Psychiatry. 2017;2017:2402731. doi:10.1155/2017/2402731
108. Bauer LA. Clinical Pharmacokinetics Handbook. New York, NY: McGraw-Hill; 2006.
109. Fang J, Mosier KE. Literature values of terminal half-lives of clozapine are dependent on the time of the last data point. J Pharm Pharm Sci. 2014;17(2):187. doi:10.18433/j3kc7p
110. Inc S. Clozapine-clozapine tablet. Highlights of prescribing information. Princeton, NJ:Sandoz Inc; 2020. Available from: https://dailymed.nlm.nih.gov/dailymed/drugInfo.cfm?setid=e503b3cd-574e-ed6a-c7ed-3368115f7f72.
111. Diaz FJ, Josiassen RC, de Leon J. The effect of body weight changes on total plasma clozapine concentrations determined by applying a statistical model to the data from a double-blind trial. J Clin Psychopharmacol. 2018;38(5):442–446. doi:10.1097/JCP.0000000000000926
112. Ruan CJ, de Leon J. Is there a future for CYP1A2 pharmacogenetics in the optimal dosing of clozapine? Pharmacogenomics. 2020;21(6):369–373. doi:10.2217/pgs-2020-0015
113. de Leon J, Schoretsanitis G, Kane JM, Ruan CJ. Using therapeutic drug monitoring to personalize clozapine dosing in Asians. Asia Pac Psychiatry. 2020;12(2):e12384. doi:10.1111/appy.12384
114. Ruan CJ, Wang CY, Tang YL, et al. Exploring the prevalence of clozapine phenotypic poor metabolizers in 4 Asian samples: they ranged between 2% and 13. J Clin Psychopharmacol. 2019;39(6):644–648. doi:10.1097/JCP.0000000000001125
115. de Leon J, De Las Cuevas C. The art of pharmacotherapy: reflections on pharmacophobia. J Clin Psychopharmacol. 2017;37(2):131–137. doi:10.1097/JCP.0000000000000675
116. Konstantakopoulos G. Insight across mental disorders: a multifaceted metacognitive phenomenon. Psychiatriki. 2019;30(1):13–16. doi:10.22365/jpsych.2019.301.13
117. Kim J, Ozzoude M, Nakajima S, et al. Insight and medication adherence in schizophrenia: an analysis of the CATIE trial. Neuropharmacology. 2020;168:107634. doi:10.1016/j.neuropharm.2019.05.011
118. Gutiérrez-Rojas L, Martínez-Ortega JM, Pérez-Costillas L, Jiménez-Fernández S, Carretero MD, Gurpegui M. Illness insight and medication adherence among patients with bipolar disorder. J Nerv Ment Dis. 2020;208(6):481–487. doi:10.1097/NMD.0000000000001151
119. Bell M, Fiszdon J, Richardson R, Lysaker P, Bryson G. Are self-reports valid for schizophrenia patients with poor insight? Relationship of unawareness of illness to psychological self-report instruments. Psychiatry Res. 2007;151(1–2):37–46. doi:10.1016/j.psychres.2006.04.012
120. Buckwalter KC, Kerfoot KM. Teaching patients self care: a critical aspect of psychiatric discharge planning. J Psychosoc Nurs Ment Health Serv. 1982;20(5):15–20.
121. Alghzawi HM. Psychiatric discharge process. ISRN Psychiatry. 2012;638943. doi:10.5402/2012/638943
122. Smith RL, O’Connell K, Athanasiu L, et al. Identification of a novel polymorphism associated with reduced clozapine concentration in schizophrenia patients-a genome-wide association study adjusting for smoking habits. Transl Psychiatry. 2020;10(1):198. doi:10.1038/s41398-020-00888-1
123. Schoretsanitis G, Kane JM, Ruan CJ, Spina E, Hiemke C, de Leon J. A comprehensive review of the clinical utility of and a combined analysis of the clozapine/norclozapine ratio in therapeutic drug monitoring for adult patients. Expert Rev Clin Pharmacol. 2019;12(7):603–621. doi:10.1080/17512433.2019.1617695
124. Kyllesø L, Smith RL, Ø K, Andreassen OA, Molden E. Undetectable or subtherapeutic serum levels of antipsychotic drugs preceding switch to clozapine. NPJ Schizophr. 2020;6(1):17. doi:10.1038/s41537-020-0107-7
125. Baumann P, Hiemke C, Ulrich S, et al. The AGNP-TDM expert group consensus guidelines: therapeutic drug monitoring in psychiatry. Pharmacopsychiatry. 2004;37(6):243–265. doi:10.1055/s-2004-832687
126. Hiemke C, Bergemann N, Clement HW, et al. Consensus guidelines for therapeutic drug monitoring in neuropsychopharmacology: update 2017. Pharmacopsychiatry. 2018;51(1–2):e1. doi:10.1055/s-0037-1600991
127. Schoretsanitis G, Kane JM, Correll CU, et al. Blood levels to optimize antipsychotic treatment in clinical practice: a joint consensus statement of the American society of clinical psychopharmacology and the therapeutic drug monitoring task force of the arbeitsgemeinschaft für neuropsychopharmakologie und pharmakopsychiatrie. J Clin Psychiatry. 2020;81(3):19cs13169. doi:10.4088/JCP.19cs13169
128. Schoretsanitis G, Spina E, Hiemke C, de Leon J. A systematic review and combined analysis of therapeutic drug monitoring studies for long-acting risperidone. Expert Rev Clin Pharmacol. 2017;10(9):965–981. doi:10.1080/17512433.2017.1345623
129. Schoretsanitis G, Spina E, Hiemke C, de Leon J. A systematic review and combined analysis of therapeutic drug monitoring studies for oral paliperidone. Expert Rev Clin Pharmacol. 2018;11(6):625–639. doi:10.1080/17512433.2018.1478727
130. Schoretsanitis G, Spina E, Hiemke C, de Leon J. A systematic review and combined analysis of therapeutic drug monitoring studies for long-acting paliperidone. Expert Rev Clin Pharmacol. 2018;11(12):1237–1253. doi:10.1080/17512433.2018.1549489
131. Schoretsanitis G, Villasante-Tezanos AG, de Leon J. Studies of half lives of long-acting antipsychotics are needed. Pharmacopsychiatry. 2019;52(1):45–46. doi:10.1055/a-0755-7692
132. Chopra N, Ruan CJ, McCollum B, Ognibene J, Shelton C, de Leon J. High doses of drugs extensively metabolized by CYP3A4 were needed to reach therapeutic concentrations in two patients taking inducers. Rev Colomb Psiquiatr. 2020;49(2):84–95. doi:10.1016/j.rcp.2018.07.002
133. Horvitz-Lennon M, Mattke S, Predmore Z, Howes OD. The role of antipsychotic plasma levels in the treatment of schizophrenia. Am J Psychiatry. 2017;174(5):421–426. doi:10.1176/appi.ajp.2016.16040402
134. Kalaria SN, Kelly DL. Development of point-of-care testing devices to improve clozapine prescribing habits and patient outcomes. Neuropsychiatr Dis Treat. 2019;15:2365–2370. doi:10.2147/NDT.S216803
135. Cohen AN, Collins G, Nucifora FC
136. Italiano D, Spina E, de Leon J. Pharmacokinetic and pharmacodynamic interactions between antiepileptics and antidepressants. Expert Opin Drug Metab Toxicol. 2014;10(11):1457–1489. doi:10.1517/17425255.2014.956081
137. Lana F, Martí-Bonany J, Fuster J, de Leon J. Reduction in serum concentration of valproic acid secondary to the intake of ibuprofen as an example of valproic acid auto-induction metabolism. Actas Esp Psiquiatr. 2016;44(4):136–144.
138. Jackson J, McCollum B, Ognibene J, Diaz FJ, de Leon J. Three patients needing high doses of valproic acid to get therapeutic concentrations. Case Rep Psychiatry. 2015;2015:542862. doi:10.1155/2015/542862
139. Johansson I, Lundqvist E, Bertilsson L, Dahl ML, Sjöqvist F, Ingelman-Sundberg M. Inherited amplification of an active gene in the cytochrome P450 CYP2D locus as a cause of ultrarapid metabolism of debrisoquine. Proc Natl Acad Sci USA. 1993;90(24):11825–11829. doi:10.1073/pnas.90.24.11825
140. Levanthal H, Brissette I, Levanthal EA. The common sense model of self-regulation of health and illness. In: Routledge, editor. The Self-Regulation of Health and Illness Behavior. London: Routledge; 2003:42–65.
141. Unni EJ, Shiyanbola OO, Farris KB. Change in medication adherence and beliefs in medicines over time in older adults. Glob J Health Sci. 2016;8(5):39–47. doi:10.5539/gjhs.v8n5p39
 © 2020 The Author(s). This work is published and licensed by Dove Medical Press Limited. The
full terms of this license are available at https://www.dovepress.com/terms
and incorporate the Creative Commons Attribution
- Non Commercial (unported, 3.0) License.
By accessing the work you hereby accept the Terms. Non-commercial uses of the work are permitted
without any further permission from Dove Medical Press Limited, provided the work is properly
attributed. For permission for commercial use of this work, please see paragraphs 4.2 and 5 of our Terms.
© 2020 The Author(s). This work is published and licensed by Dove Medical Press Limited. The
full terms of this license are available at https://www.dovepress.com/terms
and incorporate the Creative Commons Attribution
- Non Commercial (unported, 3.0) License.
By accessing the work you hereby accept the Terms. Non-commercial uses of the work are permitted
without any further permission from Dove Medical Press Limited, provided the work is properly
attributed. For permission for commercial use of this work, please see paragraphs 4.2 and 5 of our Terms.