Back to Journals » Clinical Ophthalmology » Volume 13
Self-perceived preparedness and competence among ophthalmology residents for open globe repair
Authors Zafar S, Chen X, Woreta F ![]() , Sikder S
, Sikder S ![]()
Received 4 April 2019
Accepted for publication 20 May 2019
Published 16 July 2019 Volume 2019:13 Pages 1273—1278
DOI https://doi.org/10.2147/OPTH.S211144
Checked for plagiarism Yes
Review by Single anonymous peer review
Peer reviewer comments 2
Editor who approved publication: Dr Scott Fraser
Sidra Zafar, Xinyi Chen, Fasika Woreta, Shameema Sikder
Wilmer Eye Institute, Johns Hopkins Hospital, Baltimore, MD, USA
Purpose: To assess which surgical training resources residents find most useful for open globe repair.
Methods: A nationwide, survey-based, cross-sectional analysis of ophthalmology residents enrolled in accredited training programs in the United States was performed to determine the association of surgical training methods with self-perceived resident preparedness and competence for open globe repair. The survey was developed at the Wilmer Eye Institute, Johns Hopkins Hospital.
Results: The individual response rate in our study was 38.6% (118/306 participant responses from 24 programs). Pre-operative surgical planning, in the form of review of patient charts and case discussion with senior faculty, was associated with higher self-perceived levels of both preparedness and competence for several different steps of globe repair. Both supervised and independent lab practice on animal or synthetic eyes were also found to be significantly associated with increased levels of self-perceived competence, especially for steps that involved scleral and limbal reapproximation.
Conclusion: Open globe repair is an important skill that all ophthalmologists must learn to master. To improve surgical training, residency programs must focus on developing a structured surgical curriculum that incorporates training for managing ocular trauma and open globes. Possible components can include implementation of pre-operative briefings and case discussion with faculty as well as, encouraging regular utilization of practice labs in a distributed pattern to consolidate learning among residents.
Keywords: resident education, open globe repair, self-perceived, competence, preparedness
Introduction
Ocular trauma and open globe injury (OGI) particularly is one of the leading global causes of visual impairment.1 Children and young adults are among the most commonly affected age groups1 and depending on the population studied, the reported incidence is known to vary from 32% to 95%.2–4 Given the scope of public health problem presented by eye trauma, training of residents in the successful surgical repair of open globe to obtain optimal outcomes is of utmost importance.
In the United States, The Accreditation Council for Graduate Medical Education (ACGME) describes specific milestones that graduating residents are often required to achieve.5 These changes were introduced as part of an improved effort to formalize and make training more uniform across programs and to ensure early physicians gained adequate knowledge and skills before they practiced independently. In ophthalmology, one of the criteria set forth by the ACGME requires resident physicians to perform a minimum of 4 globe repairs.6 However, based on the teaching institute’s trauma level designation, patient volume can vary widely.7 Surgical experience is known to directly correlate with procedural efficiency and inversely correlate with the rate of complications.8 The variability in case volume between programs can subsequently lead to different levels of training and skill acquisition among residents for handling globe repair.
Recent years have seen a rapid growth in surgical teaching resources available to ophthalmology residency programs. Utilization of these training resources has been shown to correlate with increased levels of resident preparedness and competence for cataract surgery.9 We believe that the proper use of these resources can similarly help residents prepare for open globe repair. However, given the myriad of resources available, ranging from traditional lectures to wet labs and more advanced surgical simulators, it is important to understand which resources residents find most useful. To better address this gap in knowledge, we developed a survey to determine what teaching methods are currently used and the perceived usefulness of these teaching methods among residents. The survey included questions asking residents how confident and prepared they felt performing each step of globe repair.
Materials and methods
Study design and population
We performed a nationwide, survey-based, cross-sectional analysis of ophthalmology residents enrolled in accredited training programs in the United States. The survey was developed at the Wilmer Eye Institute and sent to residency program directors across the country through the Association of University Professors of Ophthalmology (AUPO) electronic mailing list server. Since no identifying data were requested through the survey, the study was reviewed and deemed exempt by the Johns Hopkins’ Institutional Review Board. A consent script was included to the surveys to inform respondents of their participation being voluntary.
Survey
A 13-item questionnaire was developed by surgical educators at Wilmer (Qualtrics. Provo, Utah) and distributed electronically among program directors, who were members of the AUPO. Program directors were asked to forward the survey to their residents. Responses were collected from November 2017 to April 2018. Data collected included information on residency program characteristics (geographic region, size, affiliation with a Veterans Administration (VA) hospital or a medical school) and surgical training resources. Participants were also asked to report the number of open globe repairs they had performed as well as their self-perceived levels of preparedness and competence for each of the different steps of open globe repair. These steps included sitting at an operating room microscope, making the paracentesis, injecting substances through the paracentesis incision, suturing the cornea, limbus, and sclera, and disinserting muscle when necessary. Competency, defined as the ability to perform the steps of surgery successfully and efficiently, was assessed on a four-point Likert scale: not competent, able to do with moderate coaching from supervising surgeon, able to do with minimal input from supervising surgeon, and able to do without input from supervising surgeon. Preparedness was defined as readiness to perform the steps of surgery and was assessed on a five-point Likert scale (have not performed yet, not prepared, a little prepared, moderately prepared, very prepared).
Data analysis
Comparisons were made for how often a resident partook in particular activities to prepare for initial open globe repair versus their level of preparedness when performing the different steps of globe repair for the first time. A similar comparison was also made for how competent a resident felt when performing particular steps of surgery. The association of current components of residency surgical curriculum with both resident preparedness and competence was also evaluated. The Fisher exact test was used to test the difference in the distribution of the data between categories. A P-value of less than 0.05 was considered significant.
Results
Participant demographics and program characteristics
The individual response rate in our study was 38.6% (118/306 participant responses from 24 programs). Of the 118 participants who completed the survey, 30 (25.4%) were PGY-2, 35 (29.7%) were PGY-3, and 53 (44.9%) were PGY-4. Most residents (61.0%) had performed between 0 and 5 open globe repair surgeries (in part or in total). Approximately, 22.0% had performed between 6 and 10 open globe repairs and 13.6% had performed around 11–20. Only a minority (3.3%) had done more 20 procedures, and no resident had performed more than 50 surgeries (Table 1).
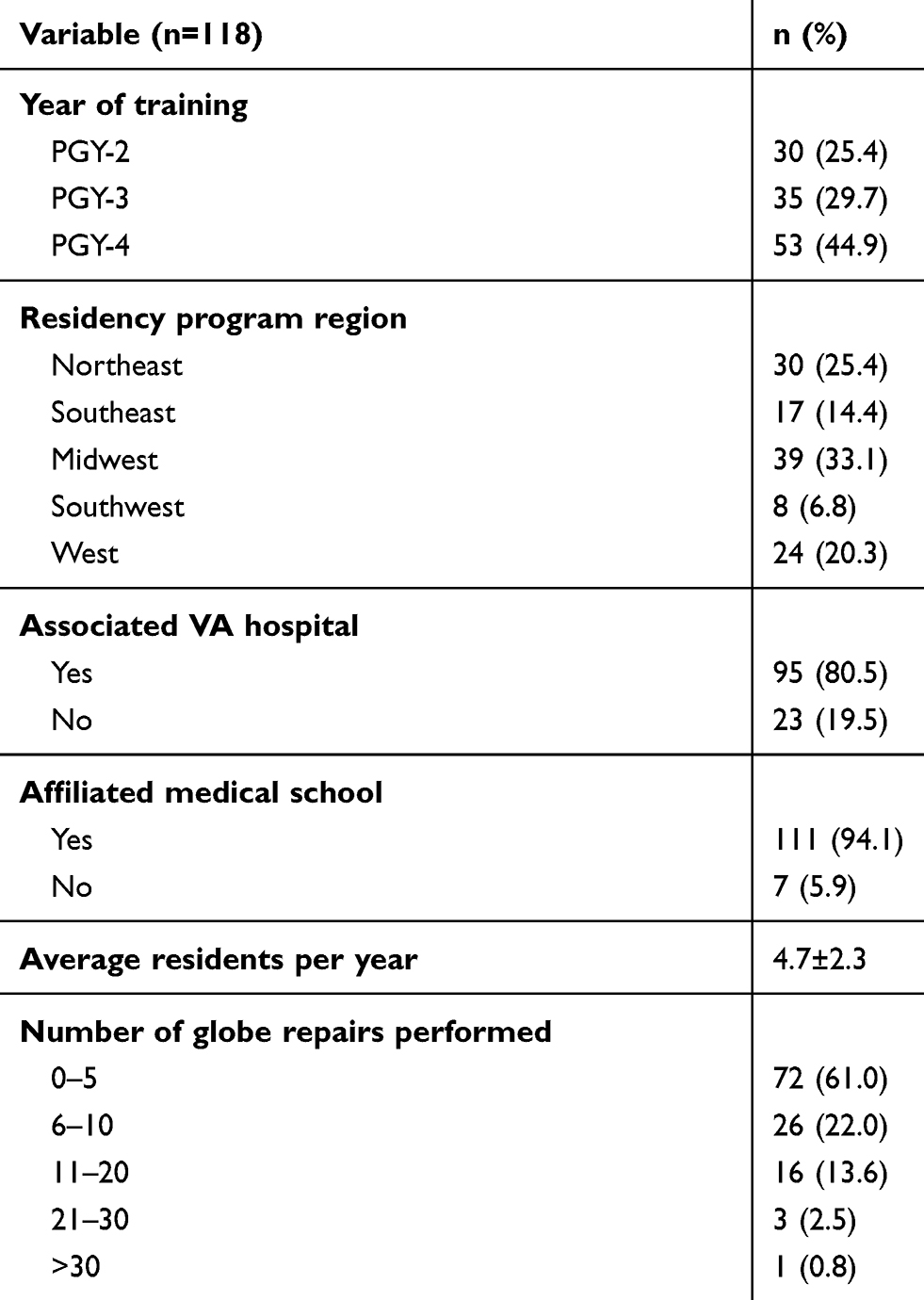 |
Table 1 Baseline participant characteristics |
Educational resources and self-perceived levels of resident preparedness and competence
Pre-operative surgical planning, in the form of review of patient charts and case discussion with senior faculty, was associated with higher self-perceived levels of both preparedness and competence for several different steps of globe repair. We found both supervised and independent lab practice on animal or synthetic eyes to be significantly associated with increased levels of competence, especially for steps that involved reapproximation (scleral, limbal, and/or corneal reapproximation). Independent lab practice was also associated with increased levels of resident preparedness for the same steps. Residents who watched surgical videos or read up about the procedure felt more prepared making the paracentesis and injecting through it. No educational resource was associated with influencing resident preparedness for muscle disinsertion during globe repair (Tables 2 and 3).
 |
Table 2 Educational resources and residents’ perceived level of preparedness in steps of globe repair |
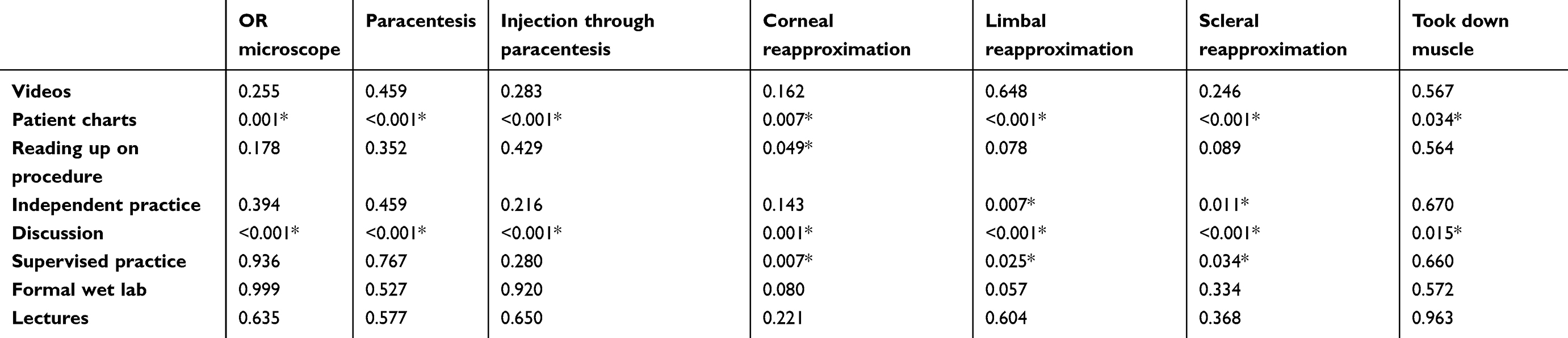 |
Table 3 Educational resources and residents’ perceived level of competence in steps of globe repair |
Discussion
As the transitional period bridging medical school and independent practice, residency training is critical for the development of physician confidence and for fostering a feeling of professional competence. Confidence is important during residency training because it encompasses several personal attributes that, if channeled appropriately, may lead to professional satisfaction and success. Limited data presently exist on resident opinions regarding the best methods for surgical training and optimizing performance. As residency programs across the United States continue to implement new surgical training methods, it is important to determine the value of these measures in improving the quality and efficiency of intraoperative resident education. Our study therefore attempted to ascertain resident-perceived benefit of such educational methods and add to the current literature on ophthalmology resident training.
In our study, we found pre-operative case preparation (review of patient charts and case discussion with faculty) to be associated with significantly higher levels of self-perceived preparedness and competence among residents for open globe repair. The environmental and situational stress typically associated with the operating room (OR) setting can complicate resident learning.10 Stress levels are especially increased during complicated and time-sensitive surgeries like globe repair. Trainees inconsistently recognize educational experiences in such unstructured environments, which can potentially lead to errors. Intraoperative judgment errors have, in fact, been recognized as one the most common reasons for resident surgical incompetence.11 Optimizing the learning environment for every case involves a proactive approach by both the faculty and the trainee. Such briefings can help assess the needs and deficits as well as establish learning objectives for the trainee. Furthermore, while we did not assess this in our study, deliberate teaching followed by immediate and specific feedback by experienced faculty has indeed shown to be associated with better and more memorable learning.12 Grober et al argued that early and more meaningful participation in the operating room is critical to learn operative competence.13 We believe that the educational environment might also influence resident confidence which can, in turn, influence self-perceived levels of competence and preparedness. Given the limited exposure of residents to open globes, it is imperative all cases of globe repairs are staffed by competent faculty in order to improve the learning experience for their surgical trainees while ensuring patient safety.14 The real-time recognition of and feedback on the management steps can further assimilate the trainee’s skill set learned from lab practice.
The overall average surgical rate for dealing with ocular trauma among residents remains low. From 2009 to 2014, residents in the United States reported performing an average of only 7 cases of globe repair during their training.15A separate study from the United Kingdom found that 60% of the ophthalmology trainees had never repaired an open globe.16 Practical learning experiences are essential to developing surgical confidence. Residents’ surgical confidence, in turn, has been shown to be associated with their perceived operating skills.17 Thus, in light of the limited surgical volume associated with ocular trauma, it is not surprising that only 64% of the ophthalmology residents feel comfortable managing globe repair.18 Since variability in surgical volume between programs will continue to exist, we believe that the goal of training should be to prepare residents with the ability to provide excellent ophthalmic care in similar real-life encounters. Practice labs are one such example, of an educational resource that can be used to provide residents with hands-on training in a low-stress environment and help develop their surgical skill set, while promoting surgical confidence. Multiple studies have, in fact, reported on the utility of such training in preparing residents for the OR.9 A similar trend was also observed in our study. We found residents who spent more time practicing on animal or synthetic eyes, either independently or under supervised guidance, to demonstrate higher self-perceived levels of competence, for performing corneal, limbal, and scleral reapproximation during globe repair. Independent lab practice was also found to be associated with greater self-perceived resident preparedness for the same steps. Our findings seem to suggest that in addition to supervised training, there is also value in resident utilization of labs for independent practice, to continue to develop their surgical confidence and enhance their fine motor skills.
Our study, however, failed to find any association between resident-perceived benefits and participation in formal wet lab courses. Similar findings were also reported by Puri et al,9 who evaluated the usefulness of several different teaching resources in preparing residents for cataract surgery. We believe that this lack of association may have been attributable to the way in which learning is delivered during these courses. Formal wet lab courses are short, intensive (1 day or weekend) sessions, commonly associated with a delay between the time the skill is learned in the laboratory and the time the skill is applied in the OR. While we did not specifically assess how this may have had influenced resident learning in our sample, a clinical trial involving 38 surgical residents found that participants randomized to 1 day (massed) training sessions performed significantly worse on acquiring new skill compared to those in weekly (distributed) practice regimens.19 The authors proposed that the superiority of distributed learning may have been due to consolidation of learning; with each practice session, key aspects of the skill being learned became more deeply encoded into memory. Thus, compared to independent or supervised lab practice, formal wet lab courses are more likely to mirror massed training sessions.
This is the first study to describe educational resources that can be useful in preparing residents for open globe repair and by doing so, adds to the limited literature on ophthalmology resident surgical training. One limitation of our study is the low response rate. We depended on program directors to distribute the survey to their residents, thus limiting the study to 24 programs. Although we had representation from each geographic region, increasing the number of programs participating in future studies will help make the data more generalizable. Another limitation is that the survey provided to residents was subjective in nature and did not include objectively measured competency and preparedness (eg, resident preparedness and competency versus patient outcomes and complication rates). Future studies that incorporate objective assessment in the wet lab may be useful. Finally, further research is needed in order to determine whether utilization of surgical training resources and increased self-perceived resident preparedness and competence translate into actual competence and to improve clinical outcomes of globe repair.
Conclusions
Open globe repair is an important skill that all graduating ophthalmology residents should learn and be confident with. Since resident training for managing ocular trauma can be limited by the variable surgical volume which can negatively affect residents’ perception of their competency, residency program should consider developing a structured surgical curriculum that incorporates training for managing ocular trauma and open globes. Possible components can include encouraging regular utilization of practice labs in a distributed pattern to consolidate learning among residents. Surgical cases should be staffed by competent faculty to encourage pre-, intra-, and postoperative discussions and facilitate resident learning. Future studies could possibly evaluate correlations between a resident-perceived level of competency, the number of procedures required to achieve competency, and surgical outcomes.
Acknowledgment
We would like to thank the residency program directors across the United States who distributed our survey to their residents.
Disclosure
The authors report no conflict of interest in this work.
References
1. Parver LM. Eye trauma: the neglected disorder. Arch Ophthalmol. 1986;104(10):1452–1453.
2. Batur M, Seven E, Esmer O, Akaltun MN, Yasar T, Cinal A. Epidemiology of adult open globe injury. J Craniofac Surg. 2016;27(7):1636–1641. doi:10.1097/SCS.0000000000003001
3. Cakmak SS, Unlu MK, Olmez G, Caca I, Sakalar YB, Acemoglu H. Penetrating eye injuries from southeastern Anatolia region of Turkey. Public Health. 2004;118(8):570–575. doi:10.1016/j.puhe.2003.12.018
4. Knyazer B, Bilenko N, Levy J, et al. Open globe eye injury characteristics and prognostic factors in southern Israel: a retrospective epidemiologic review of 10 years experience. IMAJ. 2013;15(3):158–162.
5. Arnold A. Developing the educational milestones for ophthalmology. J Grad Med Educ. 2014;6(1s1):144–145. doi:10.4300/JGME-06-01s1-37
6. Education ACfGM. Required minimum number of procedures for graduating residents in ophthalmology. Rev Committee Ophthalmol. 2013.
7. MacKenzie EJ, Hoyt DB, Sacra JC, et al. National inventory of hospital trauma centers. JAMA. 2003;289(12):1515–1522. doi:10.1001/jama.289.12.1515
8. Randleman J, Wolfe JD, Woodward M, Lynn MJ, Cherwek DH, Srivastava SK. The resident surgeon phacoemulsification learning curve. Arch Ophthalmol. 2007;125(9):1215–1219. doi:10.1001/archopht.125.9.1215
9. Puri S, Srikumaran D, Prescott C, Tian J, Sikder S. Assessment of resident training and preparedness for cataract surgery. J Cataract Refract Surg. 2017;43(3):364–368. doi:10.1016/j.jcrs.2016.12.032
10. Butvidas LD, Anderson CI, Balogh D, Basson MD. Disparities between resident and attending surgeon perceptions of intraoperative teaching. Am J Surg. 2011;201(3):385–389. doi:10.1016/j.amjsurg.2010.08.027
11. Binenbaum G, Volpe NJ. Ophthalmology resident surgical competency: a national survey. Ophthalmology. 2006;113(7):1237–1244. doi:10.1016/j.ophtha.2006.03.026
12. Roberts NK, Williams RG, Kim MJ, Dunnington GL. The briefing, intraoperative teaching, debriefing model for teaching in the operating room. J Am Coll Surg. 2009;208(2):299–303. doi:10.1016/j.jamcollsurg.2008.10.024
13. Grober ED, Jewett MAS. The concept and trajectory of “operative competence” in surgical training. Can J Surg. 2006;49(4):238–240.
14. Anderson CI, Gupta RN, Larson JR, et al. Impact of objectively assessing surgeons’ teaching on effective perioperative instructional behaviors. JAMA Surg. 2013;148(10):915–922. doi:10.1001/jamasurg.2013.2144
15. Chadha N, Liu J, Maslin JS, Teng C. Trends in ophthalmology resident surgical experience from 2009 to 2015. Clin Ophthalmol (Auckland, NZ). 2016;10:1205–1208. doi:10.2147/OPTH
16. Rodrigues IA, Symes RJ, Turner S, Sinha A, Bowler G, Chan WH. Ophthalmic surgical training following modernising medical careers: regional variation in experience across the UK. BMJ Open. 2013;3(5):e002578. doi:10.1136/bmjopen-2013-002578
17. Bucholz EM, Sue GR, Yeo H, Roman SA, Bell RH, Sosa JA. Our trainees’ confidence: results from a national survey of 4136 us general surgery residents. Arch Surg. 2011;146(8):907–914. doi:10.1001/archsurg.2011.178
18. Abdelfattah NS, Radwan AE, Sadda SR. Perspective of ophthalmology residents in the United States about residency programs and competency in relation to the International Council of Ophthalmology guidelines. J Curr Ophthalmol. 2016;28(3):146–151. doi:10.1016/j.joco.2016.06.001
19. Moulton C-AE, Dubrowski A, MacRae H, Graham B, Grober E, Reznick R. Teaching surgical skills: what kind of practice makes perfect?: a randomized, controlled trial. Ann Surg. 2006;244(3):400–409. doi:10.1097/01.sla.0000234808.85789.6a
 © 2019 The Author(s). This work is published and licensed by Dove Medical Press Limited. The
full terms of this license are available at https://www.dovepress.com/terms
and incorporate the Creative Commons Attribution
- Non Commercial (unported, 3.0) License.
By accessing the work you hereby accept the Terms. Non-commercial uses of the work are permitted
without any further permission from Dove Medical Press Limited, provided the work is properly
attributed. For permission for commercial use of this work, please see paragraphs 4.2 and 5 of our Terms.
© 2019 The Author(s). This work is published and licensed by Dove Medical Press Limited. The
full terms of this license are available at https://www.dovepress.com/terms
and incorporate the Creative Commons Attribution
- Non Commercial (unported, 3.0) License.
By accessing the work you hereby accept the Terms. Non-commercial uses of the work are permitted
without any further permission from Dove Medical Press Limited, provided the work is properly
attributed. For permission for commercial use of this work, please see paragraphs 4.2 and 5 of our Terms.