Back to Journals » Patient Preference and Adherence » Volume 11
Self-medication practice in Ethiopia: a systematic review
Authors Ayalew MB ![]()
Received 3 January 2017
Accepted for publication 7 February 2017
Published 1 March 2017 Volume 2017:11 Pages 401—413
DOI https://doi.org/10.2147/PPA.S131496
Checked for plagiarism Yes
Review by Single anonymous peer review
Peer reviewer comments 2
Editor who approved publication: Dr Johnny Chen
Mohammed Biset Ayalew
Department of Clinical Pharmacy, School of Pharmacy, College of Medicine and Health Sciences, University of Gondar, Gondar, Ethiopia
Background: Self-medication patterns vary among different populations, and are influenced by many factors. No review has been done that comprehensively expresses self-medication practice in Ethiopia. The aim of this study was to provide an overview of the literature on self-medication practice in Ethiopia.
Materials and methods: Databases (PubMed, Google Scholar, ResearchGate, and Hinari) were searched for published studies on the practice of self-medication in Ethiopia without restriction in the year of publication or methodology. Some studies were also identified through manual Google search. Primary search terms were “self medication”, “Ethiopia”, “self care”, “non-prescription”, “OTC drug use”, “drug utilization”, and “drug hoarding”. Studies that measured knowledge only or attitude only or beliefs only and did not determine the practice of self-medication were excluded.
Results: The database search produced a total of 450 papers. After adjustment for duplicates and inclusion and exclusion criteria, 21 articles were found suitable for the review. All studies were cross-sectional in nature. The prevalence of self-medication varied from 12.8% to 77.1%, with an average of 36.8%. Fever/headache, gastrointestinal tract diseases, and respiratory diseases were the commonest illnesses/symptoms for which self-medication was taken. The major reasons for practicing self-medication were previous experience of treating a similar illness and feeling that the illness was mild. Analgesics/antipyretics, antimicrobials, gastrointestinal drugs, and respiratory drugs were the common drug classes used in self-medication. Mainly, these drugs were obtained from drug-retail outlets. The use of self-medication was commonly suggested by pharmacy professionals and friends/relatives.
Conclusion: Self-medication practice is prevalent in Ethiopia and varies in different populations and regions of the country. Some of the self-medication practices are harmful and need prompt action. Special attention should be given to educating the public and health care providers on the types of illnesses that can be self-diagnosed and self-treated and the types of drugs to be used for self-medication.
Keywords: self-medication, self-care, OTC drug, Ethiopia
Introduction
Measures taken to achieve well-being and freedom from illness are different based on the attitudes and experiences of individuals. Beliefs, feelings, and thoughts of an individual significantly influence his/her understanding of an illness, which in turn affects the decision taken to address it.1 A small proportion, around 10%–30%, of symptoms experienced by an individual are brought to the attention of a physician. The majority of symptoms are either tolerated or self-medicated.2 According to the World Health Organization, self-medication is the selection and use of medicines by individuals to treat self-recognized illnesses or symptoms.3
Self-medication is a fairly widespread practice worldwide. Both developed and developing nations are giving due attention to self-medication as a component of their health care policy.4–9 Studies have revealed that increases in self-medication are due to a number of factors. These include socioeconomic factors, lifestyle, ready access to drugs, increased potential to manage certain illnesses through self-care, and greater availability of medicinal products. In most economically deprived countries, including Ethiopia, many drugs are dispensed over the counter (OTC), and the majority of health-related problems, nearly 60%–80%, are treated through self-medication as a lower-cost alternative.10–13
When practiced correctly, self-medication has a positive impact on individuals and health care systems. It allows patients to take responsibility and build confidence to manage their own health, thereby promoting self-empowerment. Furthermore, it can save time spent in waiting for a doctor and even lives in acute conditions, and may contribute to decreasing health care costs.14 If used appropriately, self-medication can lighten the demand on doctors and make people more health-conscious.15 The World Health Organization has also pointed out that responsible self-medication can help to prevent and treat ailments that do not require medical consultation, and provides a cheaper alternative for treating common illnesses.6
Regardless of the unquestionable benefits obtained from self-medication with nonprescription drugs, there are undesired outcomes that occur, due to improper usage. These have been indicated in studies where self-medication may have carried risks of misdiagnosis, use of too high a dose, incorrect duration of use, and adverse drug reactions related to the improper use of OTC drugs.16,17 Inappropriate self-medication results in irrational use of drugs, wastage of resources, increased risk of unwanted effects, and prolonged suffering.18 Irrational usage of antibiotics leads to the emergence of resistance pathogens worldwide.19 Furthermore, risks associated with self-medication also include potential delay in treating serious medical conditions, masking of symptoms of serious conditions through the use of nonprescription products, and increased polypharmacy and interaction with other regularly used medications.5 Even though self-medication is difficult to eliminate, interventions can be made to discourage the abnormal practice. Increasing self-medication practice requires more and better education of both the public and health professionals to avoid irrational use of drugs.10,20 All parties involved in self-medication should be aware of the benefits and risks of any self-medication product.6
Self-medication patterns vary among different populations, and are influenced by many factors, such as age, sex, income, expenditure, self-care orientation, education level, medical knowledge, satisfaction, and perception of illnesses.14 The type and extent of self-medication and the reasons for its practices may also vary from country to country.
Even though various studies have been conducted on self-medication practices in different parts of Ethiopia, there has not been any review done that comprehensively expresses self-medication practice in the country. Therefore, there is a need to know the overall situation of self-medication practice in the country, in order to devise appropriate educational, regulatory, and administrative measures in alleviating public health risks arising from improper practices of self-medication. The objective of this review was to provide an overview of the literature on self-medication practice among the Ethiopian population. It gives a comprehensive account of self-medication, more specifically its prevalence, common illnesses that cause the use of self-medication, commonly used drugs in self-medication, common reasons to practice self-medication, source of drugs for self-medication, and factors associated with the practice of self-medication.
Materials and methods
Search strategy
Databases (PubMed, Google Scholar, ResearchGate, and Hinari) were searched for published studies done on the practice of self-medication in Ethiopia. Some studies were also identified through a manual Google search. Additional articles were also searched from the reference lists of retrieved articles. No restriction was applied on the year of publication, methodology, or study subjects. Primary search terms were “self medication”, “self care”, “non-prescription”, “OTC drug use”, “drug utilization”, “drug hoarding”, and “Ethiopia”.
Article selection
Studies were included in the review if they aimed to assess self-medication practice in Ethiopia. Studies that measured knowledge only or attitudes only or beliefs only and did not determine the practice of self-medication were excluded.
Assessment of methodological quality
Methodological validity of all the 21 studies was checked prior to inclusion in the review by undertaking critical appraisal using a standardized instrument adapted from Guyatt et al.21 The instrument has eleven criteria. Each study was evaluated for each criterion/question as “yes”, “cannot tell”, or “no”, with values of 2, 1, and 0 assigned, respectively. Studies with a total score of more than 90% were considered to be of high quality, 75%–90% medium quality, and below 75% low quality.
Data abstraction
The author screened the articles based on the inclusion/exclusion criteria. The following details were extracted from each study using an abstraction form: author, year of publication, study area, study subjects, sample size, study design, sampling technique, recall period, prevalence of self-medication, common illnesses that resulted in the use of self-medication, drugs used in self-medication, reasons to practice self-medication, and factors associated with self-medication.
Results
Literature search results
The search of the PubMed, Google Scholar, ResearchGate, and Hinari databases and Google provided a total of 450 studies. After adjustment for duplicates, 132 remained. Of these, 105 studies were discarded, since after review of their titles and abstracts, they did not meet the criteria. Four studies were discarded as their full text was not available. The full texts of the remaining 23 studies were reviewed in detail. Six studies were discarded after the full text had been reviewed, since they did not address much of the needed information. An additional four studies that met the criteria for inclusion were identified through searching the reference lists of retrieved papers. Finally, as shown in Figure 1, 21 studies were included in the review.
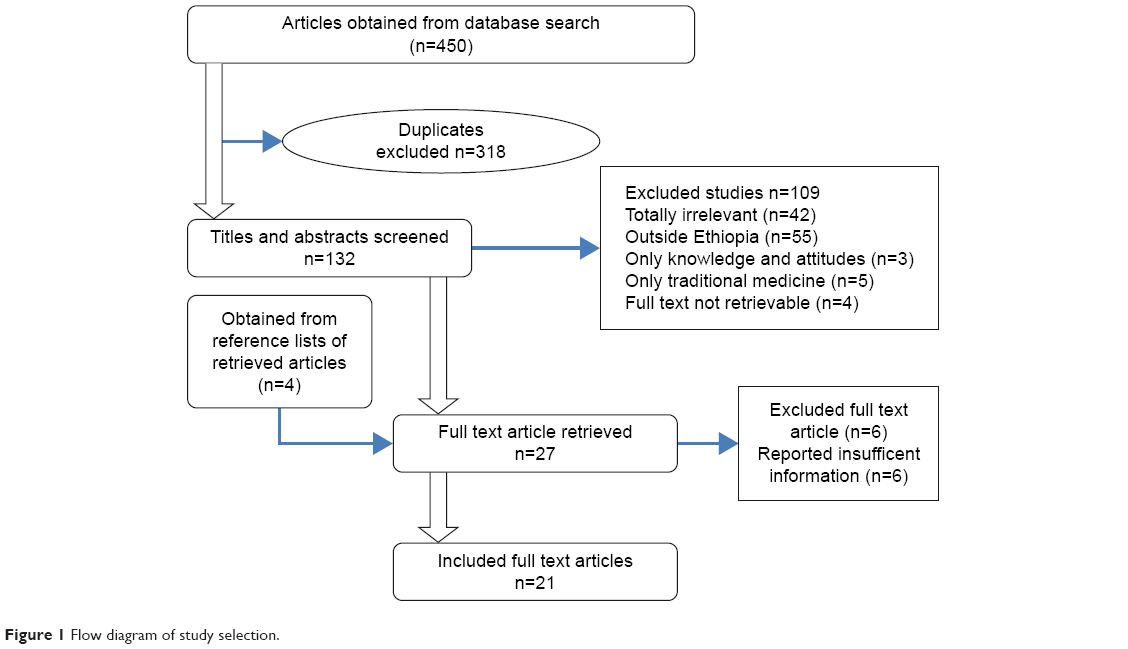 | Figure 1 Flow diagram of study selection. |
Study characteristics
The 21 studies differed substantially in sample size, recall period, and location. From these 21 articles, the majority were conducted to assess the self-medication practice of any drug or disease, while three studies focused on self-medication with antibiotics and antimalarials only. Ten studies assessed self-medication practices at the community level, five assessed self-medication practices of university students, and four assessed self-medication practices of drug-retail outlet customers. Two studies reported self-medication practices of pregnant women who were on antenatal care follow-up. The studies were conducted in different parts of the country on samples of 237–10,170 individuals. All the studies were cross-sectional in nature. The majority of the studies used stratification and random sampling to select study subjects. Detailed description of the characteristics of individual studies is provided in Table 1.
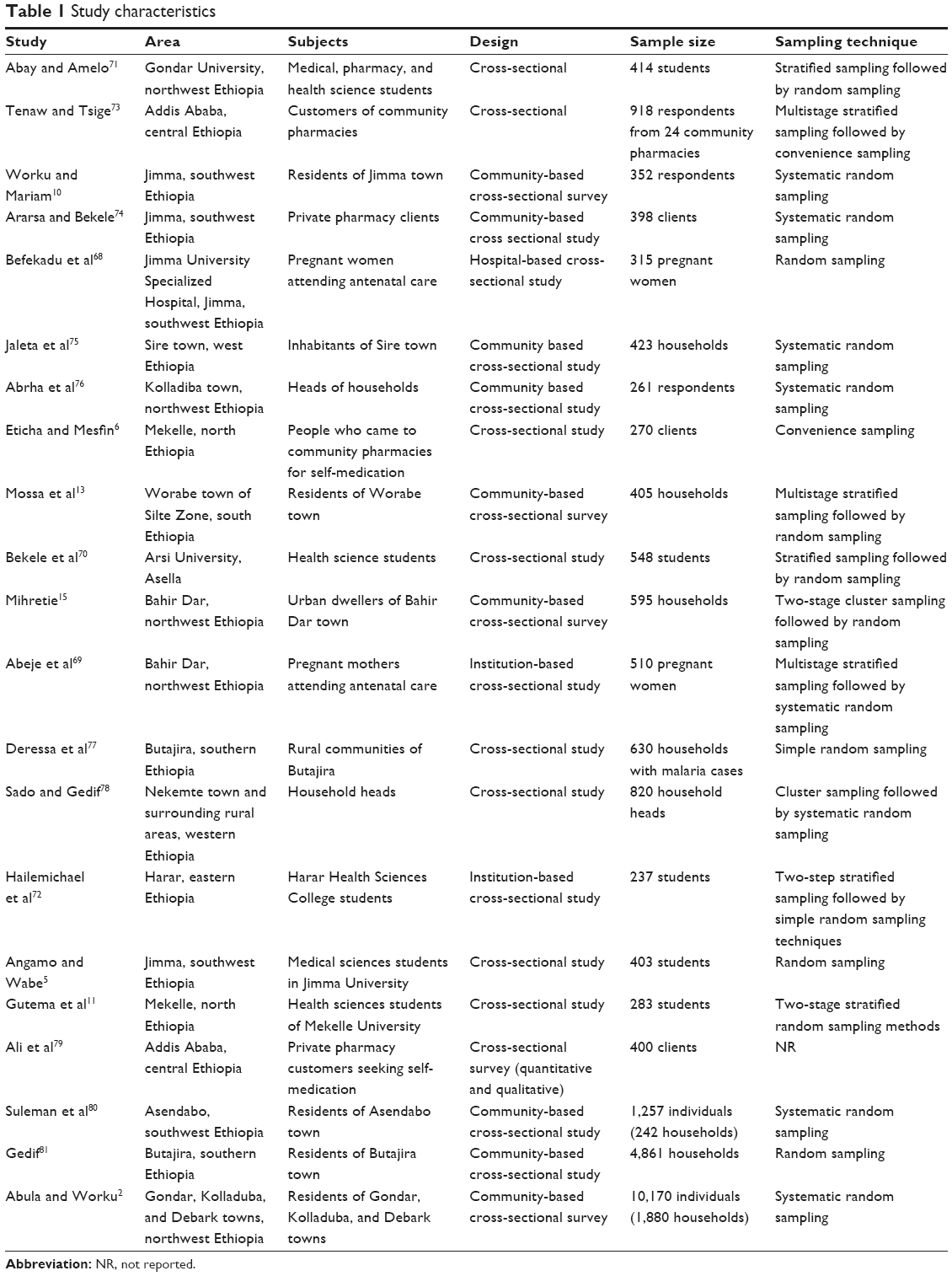 | Table 1 Study characteristics |
Methodological quality of included studies
Critical appraisal showed most studies were of high quality (n=18, 85.7%), whereas three (14.3%) were of medium quality. No difference was observed in terms of self-medication prevalence between high- and medium-quality studies.
Prevalence of self-medication
Of the 21 studies reviewed, 16 reported on prevalence of self-medication. Four studies did not calculate prevalence, since their subjects were community-pharmacy customers who came for self-medication. The reported prevalence of self-medication in the studies varied from 12.8% (Bahir Dar town residents) to 77.1% (Arsi University health science students), with an overall prevalence of 36.8%. The prevalence of self-medication in the studies was determined based on the illness history for different recall periods (2 weeks to 6 months). Two-week recall periods were used in many studies. There was no difference in the prevalence of self-medication in studies with small and large sample sizes. The prevalence of self-medication with respective recall period for each of the studies is indicated in Table 2.
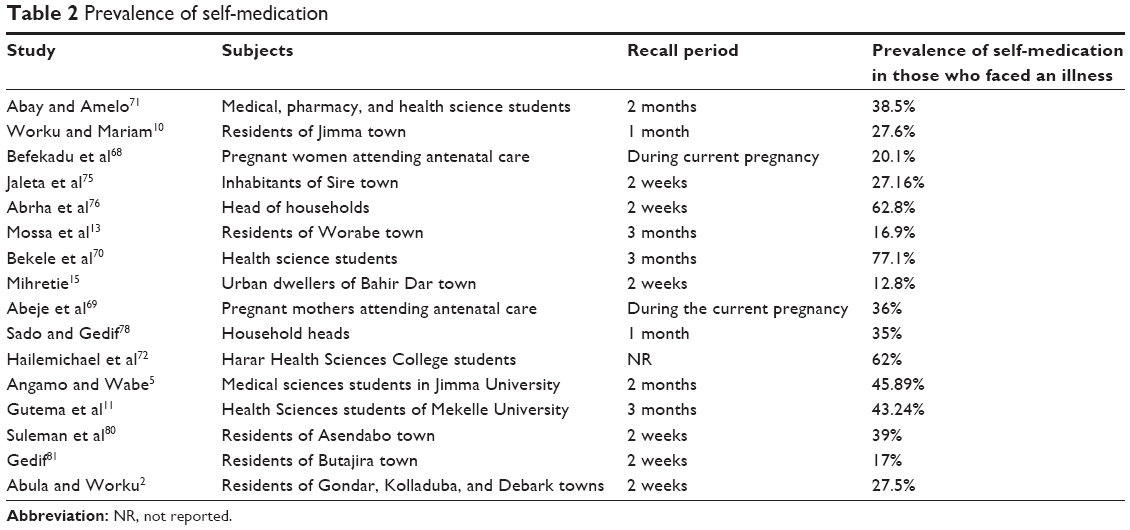 | Table 2 Prevalence of self-medication |
Common illnesses that cause self-medication, reasons to practice self-medication
Fever/headache, gastrointestinal (GI) tract diseases, and respiratory diseases were the commonest illnesses or symptoms for which self-medication was taken, accounting for an average of 30.5%, 19.7%, and 18.3% of self-medication use, respectively. The major reasons to practice self-medication were previous experience of treating a similar illness, feeling that the illness was mild and did not require the service of a physician, less expensive in terms of time and money, and need for emergency use. Table 3 shows the illnesses that resulted in self-medication and reasons that drove people to practice self-medication as reported in each study.
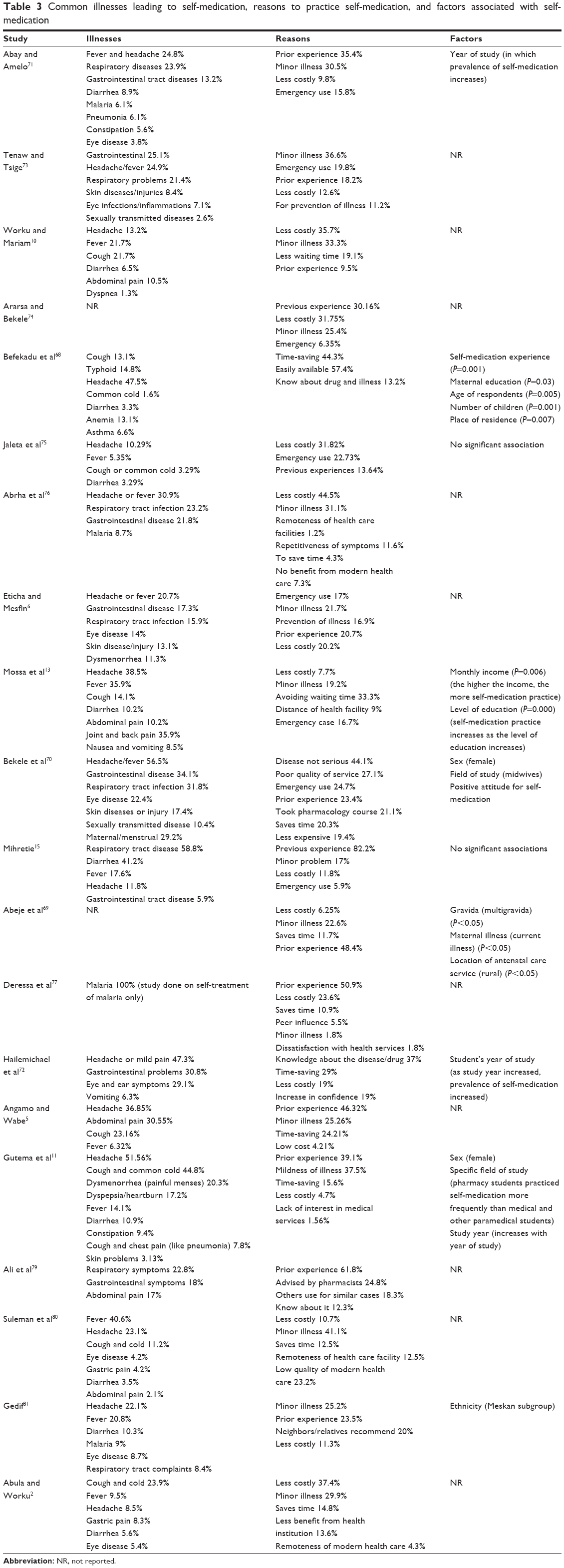 | Table 3 Common illnesses leading to self-medication, reasons to practice self-medication, and factors associated with self-medication |
Drugs used in self-medication, where they are obtained, and who suggested their use
As indicated in Table 4, analgesics/antipyretics, antimicrobials, GI drugs, and respiratory drugs were the common drug classes used in self-medication. On average, 38.7%, 30.8%, 16.7%, and 7.3% of people who practice self-medication used these drugs, respectively. Mainly, these drugs were obtained from drug-retail outlets (66.6%), shops (10.3%), relatives/friends (9.3%), and left over from previous use (6.5%). The use of self-medication was commonly suggested by pharmacy professionals, friends/relatives, and clinicians, but without formal prescriptions.
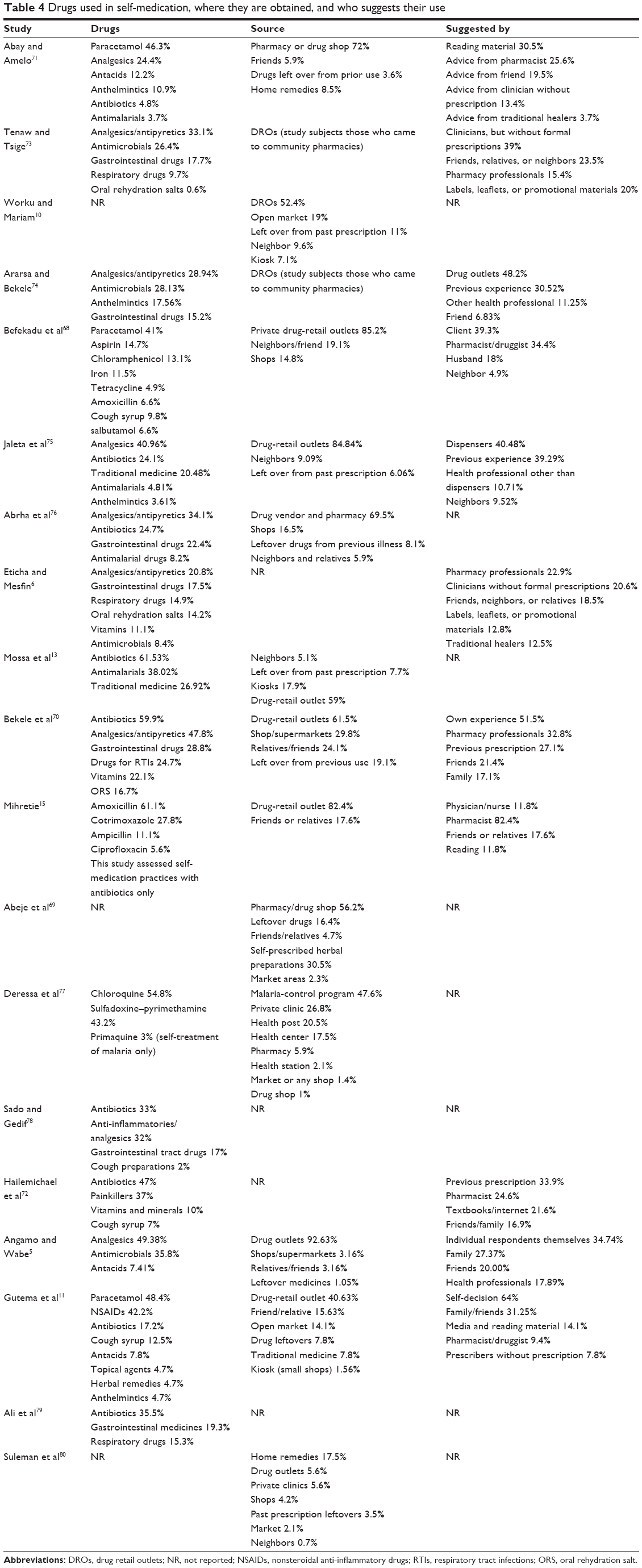 | Table 4 Drugs used in self-medication, where they are obtained, and who suggests their use |
Factors associated with practice of self-medication
Even though most of the studies reviewed did not address factors associated with self-medication, some checked the presence of association between sociodemographic characteristics and self-medication practice. As shown in Table 3, age, place of residence, sex, educational status, occupation, income, ethnicity, prior self-medication experience, attitude toward self-medication, year of study, and field of study of students were some of the factors identified in the reviewed studies.
Discussion
The prevalence of self-medication varied across the studies reviewed, ranging from 12.8% to 77.1%. This variation was found to depend on recall periods used in each study. Average prevalence rates of 31%, 31.3%, 42.2%, and 45.7% were reported for studies that assessed self-medication practice with 2-week, 1-month, 2-month, and 3-month recall periods, respectively. The main reasons for the wide variation in the prevalence of self-medication practice may be differences in social determinants of health, beliefs, and culture of the population, as Ethiopia is a country of multiple “nations”. The difference in approaches used to collect information about self-medication may also have contributed to this variation in prevalence of self-medication. Similarly, review article by Shehnaz et al reported that the overall prevalence of self-medication varied from 2% to 92%.22
Higher self-medication use was reported in studies conducted on health science students than the general population. This may be because health science students have better knowledge of disease and drugs, so have less inclination to seek physicians help to treat their illnesses. Other studies conducted on health science students in different parts of the world have also reported higher prevalence of self-medication practice.23–25 Martins et al also reported community members with a high level of education were more likely to use antimicrobial self-medication, possibly due to the exposure and increased focus on health.26
The most common reasons for self-medication in Ethiopia were previous experience of treating a similar illness, feeling that the illness was mild, less costly, and less time-consuming. Similarly, the patient’s assessment of their ailment as minor was identified as one of the major factors in self-medication in many studies conducted outside Ethiopia.27–35 Prior experience of treating the same condition by self-medication has also been mentioned as the main reason for practicing self-medication.34,35 Studies conducted in other developing countries also mention lack of time to visit the physician and economic problems as the main reason to use self-medication.23,33
Fever/headache, GI-tract diseases, and respiratory diseases were the commonest illnesses/symptoms for which self-medication was taken. Fever and headache were indicated as the most frequent health complaint that led to self-medication in different studies.22–24,35–37 There were also studies that reported respiratory diseases23,34,35,37–39 and GI-tract diseases23,40 as common illnesses for which self-medication was used. This may be because these illnesses are very common and occur frequently in individuals with experience of treating them. The mild and self-limiting nature of these illnesses may also prevent patients from seeking physician consultation. However, patients should not forget that when these illnesses/symptoms occur repeatedly or for prolonged periods, they should be investigated further by physicians, as they may be manifestations of serious illnesses.
Analgesics/antipyretics, antimicrobials, GI drugs, and respiratory drugs were the most frequently used drug classes in self-medication. Multiple studies conducted to assess the practice of self-medication outside Ethiopia also reported analgesics as the most widely consumed OTC drugs in self-care.22,23,35,40–43 Antimicrobials were also reported in many studies as commonly used drugs in self-medication.23,34,37,44–46 One review article indicated that the overall estimate of antimicrobial self-medication in low- and middle-income countries was 38.8%.47 Even though every medication used in self-care needs responsibility, the high rate of antimicrobial use in self-medication needs special emphasis. Despite their prescription-only legal status in most countries, antibiotic use as an OTC medication occurs globally.48 This practice poses great risks, like antibiotic resistance. The practice of self-medication should be conducted only insofar as the benefits outweigh the risks. It should also be understood that the potential benefits of self-medication will only be obtained if it is practiced responsibly.49 Responsible government and nongovernment organizations should work hard to ensure the rational use of antimicrobials.
Common sources of drug recommendation included pharmacy professionals, friends/relatives, and clinicians, but without formal prescriptions. It was also mentioned in different studies that community drug sellers were commonly used as a source of advice or information for the drugs used in self-medication.23,34,35,47,50,51 The advice of friends or family was also reported as a commonly used source to identify drugs used for self-medication.23,24,34,51 As most of the self-medication users take drugs after consulting drug dispensers, the main role of assuring the rationality of self-medication practice will primarily lay on them. As such, they should be well trained to respond to symptoms. They should also have professional conduct, and abide by the rules and regulations of the drug-control authority of the country. They should avoid the nonprescription sale of prescription-only drugs. The community should also be educated on which illnesses they can seek drugs without the advice of a physician and for which they have to seek a clinician’s consultation.
Drugs used in self-medication were mostly obtained from drug-retail outlets (66.6%), shops (10.3%), relatives/friends (9.3%), and left over from previous use (6.5%). According to the current study, more than 10% of self-medication users in Ethiopia take drugs from shops. This is another important issue that needs due attention. Drugs should not be allowed to be present in shops, since they need special storage conditions, special handling, and advice from a pharmacy professional who is knowledgeable on dispensing. Even though Ethiopian law forbids the availability of drugs in shops, the implementation of regulation is weak. Ethiopian food, medicine, and health care control authorities need to enforce this law more judiciously.
There were several studies that reported significant associations between self medication practice and sociodemographic characteristics such as age,52–59 sex,34,52,56,57,60–63 educational status,58,62,64–66 income,58,62,64–66 and prior self-medication experience.62,67 Similarly, the current review identified some sociodemographic factors to affect the prevalence of self medication. These were age,68 place of residence,68,69 sex,11,70 educational status,13,68 income,13 prior self-medication experience,68 attitude toward self-medication,70 student’s year of study,11,71,72 field of study,11,70 and ethnicity.81
Limitations
Even though this review has its own strengths, such as inclusion of both published and unpublished research works and critically appraising the selected studies, it is not without limitations. As all of the studies reviewed were cross-sectional, the limitation of this type of study will be reflected. Some information was not reported in some of the studies. The recall periods used to assess the practice of self-medication varied across the studies, which made difficult to compare among prevalence rates. There was also high heterogeneity among the studies reviewed. This may have been due to a lack of standardized criteria for data-collection tools.
Conclusion
Self-medication practice is prevalent in Ethiopia and varied in different populations and regions of the country. Some of the self-medication practices are harmful and need prompt action. Implementation of laws that regulate drug dispensing should be emphasized. Special attention should be given to educating the public and health care providers on the type of illnesses that can be self-diagnosed and self-treated and the type of drugs to be used for self-medication.
Disclosure
The author reports no conflicts of interest in this work.
References
Leyva-Flore R, Kageyama ML, Ervitin-Erice J. How people respond to illness in Mexico: self-care or medical care? Health Policy. 2001;57:15–26. | ||
Abula T, Worku A. Self-medication in three towns of north west Ethiopia. Ethiop J Health Dev. 2001;15:25–30. | ||
World Health Organization. The role of the pharmacist in self-care and self-medication. Available from: http://apps.who.int/medicinedocs/pdf/whozip32e/whozip32e.pdf. Accessed October 26, 2016. | ||
Sleath B, Rubin RH, Campbell W, Gwyther L, Clark T. Physician-patient communication about over-the-counter medications. Soc Sci Med. 2001;53:357–369. | ||
Angamo MT, Wabe NT. Knowledge, attitude and practice of self-medication in southwest Ethiopia. Int J Pharm Sci Res. 2012;3:1005–1010. | ||
Eticha T, Mesfin K. Self-medication practices in Mekelle, Ethiopia. PLoS One. 2014;9:e97464. | ||
Chang FR, Trivedi PK. Economics of self medication: theory and evidence. Health Econ. 2003;12:721–739. | ||
World Health Organization. The benefits and risks of self-medication. WHO Drug Inf. 2000;14:1–2. | ||
World Health Organization. The role of the pharmacist in the health care system. 1994. Available from: http://apps.who.int/medicinedocs/pdf/h2995e/h2995e.pdf. Accessed February 8, 2017. | ||
Worku S, Mariam AG. Practice of self-medication in Jimma town. Ethiop J Health Dev. 2003;17:111–116. | ||
Gutema GB, Gadisa DA, Kidanemariam ZA, et al. Self-medication practices among health sciences students: the case of Mekelle University. J Appl Pharm Sci. 2011;1:183–189. | ||
Khan RA. Self-Medication with Antibiotics: Practices among Pakistani Students in Sweden and Finland [master’s thesis]. Huddinge (Sweden): Södertörns University; 2011. | ||
Mossa DA, Wabe NT, Angamo MT. Self-medication with antibiotics and antimalarials in the community of Silte Zone, south Ethiopia. Turk Silahli Kuvvetleri Koruyucu Hekim Bul. 2012;11:529–536. | ||
Almasdy D, Sharrif A. Self-medication practice with nonprescription medication among university students: a review of the literature. Arch Pharm Pract. 2011;2:95–100. | ||
Mihretie TM. Self-Medication Practices with Antibiotics among Urban Dwellers of Bahir Dar Town, North West Ethiopia [master’s thesis]. Addis Ababa: Addis Ababa University; 2014. | ||
Hughes CM, McElnay JC, Fleming GF. Benefits and risks of self-medication. Drug Saf. 2001;24:1027–1037. | ||
Ruiz ME. Risks of self-medication practices. Curr Drug Saf. 2010;5:315–323. | ||
Buck M. Self-medication by adolescents. J Pediatr Pharm. 2007;13:1–4. | ||
Pagane D. Self-medication and health insurance coverage in Mexico. Health Policy. 2007;75:170–177. | ||
Saleem TK, Sankar C, Dilip C, Azeem AK. Self-medication with over the counter drugs: a questionnaire based study. Pharm Lett. 2011;3:91–98. | ||
Guyatt GH, Sackett DL, Cook DJ. Users’ guides to the medical literature II: how to use an article about therapy or prevention. JAMA. 1994;271:59–63. | ||
Shehnaz SI, Agarwal AK, Khan N. A systematic review of self-medication practices among adolescents. J Adolesc Health. 2014;55:467–483. | ||
Bollu M, Vasanthi B, Chowdary PS, Chaitanya DS, Nirojini PS, Nadendla RR. Prevalence of self medication among the pharmacy students in Guntur: a questionnaire based study. World J Pharm Pharm Sci. 2014;3:810–826. | ||
Johnson D, Sekhar HS, Alex T, Kumaraswamy M, Chopra RS. Self-medication practice among medical, pharmacy and nursing students. Int J Pharm Pharm Sci. 2016;8:1–5. | ||
Patil SB, Vardhamane SH, Patil BV, Santoshkumar J, Binjawadgi AS, Kanaki AR. Self-medication practice and perceptions among undergraduate medical students: a cross-sectional study. J Clin Diagn Res. 2014;8:20–23. | ||
Martins AP, Miranda AC, Mendes Z, Soares MA, Ferreira P, Nogueria A. Self-medication in a Portuguese urban population: a prevalence study. Pharmacoepidemial Drug Saf. 2002;11:409–414. | ||
Hebeeb GE, Gearhart JG. Common patient symptoms: patterns of self-treatment and prevention. J Miss State Med Assoc. 1993;34:179–181. | ||
Sharma R, Verma U, Sharma CL, Kapoor B. Self-medication among urban population of Jammu city. Indian J Pharmacol. 2005;37:40–43. | ||
Omolase CO, Adeleke OE, Afolabi AO, Afolabi OT. Self medication amongst general outpatients in a Nigerian community hospital. Ann Ib Postgrad Med. 2007;5:64–67. | ||
Shankar PR, Partha P, Shenoy N. Self-medication and non-prescription practices in Pokhara Valley, western Nepal: a questionnaire-based study. BMC Fam Pract. 2002;3:17. | ||
Zaki IA. Self-medication practices among Malaysia undergraduate pharmacy students. 2010. Available from: http://malrep.uum.edu.my/rep/Record/uitm.ir.2218/Details. Accessed February 8, 2017. | ||
Sawalha AF. Assessment of self-medication practice among university students in Palestine: therapeutic and toxicity implications. Islam Univ J. 2007;15:67–82. | ||
Yousef AM, Al-Bakri AG, Bustanji Y, Wazaify M. Self-medication patterns in Amman, Jordan. Pharm World Sci. 2008;30:24–30. | ||
Jasim AL, Fadhil TA, Taher SS. Self-medication practice among Iraqi patients in Baghdad city. Am J Pharmacol Sci. 2014;2:18–23. | ||
Flaiti MA, Badi KA, Hakami WO, Khan SA. Evaluation of self-medication practices in acute diseases among university students in Oman. J Acute Dis. 2014;3:249–252. | ||
Gaddamdamodar; Assessment of self-medication practices among medical, pharmacy and nursing students at a tertiary care teaching hospital. Indian J Hosp Pharm. 2012;49:79–83. | ||
Patil SB, Vardhamane SH, Patil BV, Jeevangi S, Ashok SB, Anand RK. Self-medication practice and perceptions among undergraduate medical students: a cross-sectional study. J Clin Diagn Res. 2014;8:20–23. | ||
Banerjee I, Bhadury T. Self-medication practice among undergraduate medical students in a tertiary care medical college, West Bengal. J Postgrad Med. 2012;58:127–131. | ||
Badiger S, Kundapur R, Jain A, et al. Self-medication patterns among medical students in South India. Australas Med J. 2012;5:217–220. | ||
Ali SE, Ibrahim MI, Palaian S. Medication storage and self-medication behaviour amongst female students in Malaysia. Pharm Pract (Granada). 2010;8:226–232. | ||
Sharif SI, Ibrahim OH, Mouslli L, Waisi R. Evaluation of self-medication among pharmacy students. Am J Pharmacol Toxicol. 2012;7:135–140. | ||
James H, Handu SS, Al Khaja KA, Otoom S, Sequeira RP. Evaluation of the knowledge, attitude and practice of self-medication among first-year medical students. Med Princ Pract. 2006;15:270–275. | ||
Mitka M. When teens self-treat headaches, OTC drug misuse is frequent result. JAMA. 2004;292:424–425. | ||
Syed NZ, Reema S, Sana W, Akbar JZ, Talha V. Self medication amongst university students of Karachi: prevalence, knowledge and attitudes. J Pak Med Assoc. 2008;58:214–217. | ||
Khan RA. Self-medication with antibiotics: practices among Pakistani students in Sweden and Finland. 2011. Available from: http://sh.diva-portal.org/smash/record.jsf?pid=diva2%3A452461&dswid=−2995. Accessed February 8, 2017. | ||
Awad AI, Eltayeb IB, Capps PA. Self-medication practices in Khartoum State, Sudan. Eur J Clin Pharmacol. 2006;62:317–324. | ||
Ocan M, Obuku EA, Bwanga F, et al. Household antimicrobial self-medication: a systematic review and meta-analysis of the burden, risk factors and outcomes in developing countries. BMC Public Health. 2015;15:742. | ||
Morgan DJ, Okeke IN, Laxminarayan R, Perencevich EN, Weisenberg S. Non-prescription antimicrobial use worldwide: a systematic review. Lancet Infect Dis. 2011;11:692–701. | ||
Radyowijati A, Haak H. Improving antibiotic use in low-income countries: an overview of evidence on determinants. Soc Sci Med. 2003;57:733–744. | ||
Moraes AC, Delaporte TR, Molena-Fernandes CA, Falcão MC. Factors associated with medicine use and self-medication are different in adolescents. Clinics (Sao Paulo). 2011;66:1149–1155. | ||
Patel MM, Singh U, Sapre C, Salvi K, Shah A, Vasoya B. Self-medication practices among college students: a cross sectional study in Gujarat. Natl J Med Res. 2013;3:257–260. | ||
da Silva C, Giugliani ER. Consumo de medicamentos em adolescentes escolares: uma preocupação. [Consumption of medicines among adolescent students: a concern]. J Pediatr (Rio J). 2004;80:326–332. Portuguese. | ||
Du Y, Knopf H. Self-medication among children and adolescents in Germany: results of the National Health Survey for Children and Adolescents (KiGGS). Br J Clin Pharmacol. 2009;68:599–608. | ||
Pereira FS, Bucaretchi F, Stephan C, Cordeiro R. Self-medication in children and adolescents. J Pediatr (Rio J). 2007;83:453–458. | ||
Abahussain NA, Taha AZ. Knowledge and attitudes of female school students on medications in eastern Saudi Arabia. Saudi Med J. 2007;28:1723–1727. | ||
McCabe SE, Boyd CJ, Young A. Medical and nonmedical use of prescription drugs among secondary school students. J Adolesc Health. 2007;40:76–83. | ||
Hansen EH, Holstein BE, Due P, Currie CE. International survey of self-reported medicine use among adolescents. Ann Pharmacother. 2003;37:361–366. | ||
Al-Azzam SI, Al-Husein BA, Alzoubi F, Masadeh MM, Al-Horani S. Self-medication with antibiotics in Jordanian population. Int J Occup Med Environ Health. 2007;20:373–380. | ||
Sanjana P, Barans MJ, Bangs MJ, et al. Survey of community knowledge, attitudes and practices during a malaria epidemic in central Java, Indonesia. Am J Trop Med Hyg. 2006;75:783–789. | ||
Stoelben S, Krappweis J, Rössler G, Kirch W. Adolescents’ drug use and drug knowledge. Eur J Pediatr. 2000;159:608–614. | ||
Furu K, Skurtveit S, Rosvold EO. Selvrapportert legemiddelbruk hos 15–16-åringer i Norge. [Self-reported medical drug use among 15–16 year-old adolescents in Norway]. Tidsskr Nor Laegeforen. 2005;125:2759–2761. Norwegian. | ||
Chowdhury N, Matin F, Chowdhury SF. Medication taking behavior of students attending a private university in Bangladesh. Int J Adolesc Med Health. 2009;21:361–370. | ||
Alghanim SA. Self-medication practice among patients in a public health care system. East Mediterr Health J. 2011;17:409–416. | ||
Awad A, Eltayeb I, Matowe L, Thalib L. Self-medication with antibiotics and antimalarials in the community of Khartoum State, Sudan. J Pharm Pharm Sci. 2005;8:326–331. | ||
Sapkota AR, Coker ME, Goldstein RE, et al. Self-medication with antibiotics for the treatment of menstrual symptoms in southwest Nigeria: a cross-sectional study. BMC Public Health. 2010;10:610. | ||
Osemene KP, Lamikanra A. A study of the prevalence of self-medication practice among university students in southwestern Nigeria. Trop J Pharm Res. 2012;11:683–689. | ||
Shehnaz SI, Sreedharan J, Khan N, et al. Factors associated with self-medication among expatriate high school students: a cross-sectional survey in United Arab Emirates. Epidemiol Biostatist Public Health. 2013;10:e8724. | ||
Befekadu A, Dekama NH, Mohammed AM. Self-medication and contributing factors among pregnant women attending antenatal care in Ethiopia: the case of Jimma University Specialized Hospital. Med Sci. 2014;3:969–981. | ||
Abeje G, Admasie C, Wasie B. Factors associated with self-medication practice among pregnant mothers attending antenatal care at governmental health centers in Bahir Dar city administration, northwest Ethiopia, a cross sectional study. Pan Afr Med J. 2015;20:276. | ||
Bekele SA, Argaw MD, Yalew AW. Magnitude and factors associated with self-medication practices among university students: the case of Arsi University, College of Health Science, Asella, Ethiopia: cross-sectional survey based study. Open Access Libr J. 2016;3:e2738. | ||
Abay SM, Amelo W. Assessment of self-medication practices among medical, pharmacy, and health science students in Gondar University, Ethiopia. J Young Pharm. 2010;2:306–310. | ||
Hailemichael W, Sisay M, Mengistu G. Assessment of the knowledge, attitude, and practice of self-medication among Harar Health Sciences College students, Harar, eastern Ethiopia. J Drug Deliv Ther. 2016;6:31–36. | ||
Tenaw A, Tsige GM. Self-medication practices in addis ababa: a prospective study. Ethiop J Health Sci. 2004;14(1):1–11. | ||
Ararsa A, Bekele A. Assessment of self-medication practice and drug storage on private pharmacy clients in Jimma town, Oromia, South west Ethiopia. AJPS. 2015;1(1):20–32. | ||
Jaleta A, Tesema S, Yimam B. Self-medication practice in Sire town, West Ethiopia: a cross-sectional study. Cukurova Med J. 2016;41(3):447–452. | ||
Abrha S, Molla F, Melkam W. Self-medication practice: the case of Kolladiba Town, North West Ethiopia. IJPSR. 2014;5(10):670–677. | ||
Deressa W, Ali A, Enqusellassie F. Self-treatment of malaria in rural communities, Butajira, southern Ethiopia. Bulletin of the World Health Organization. 2003;81:261–268. | ||
Sado E, Gedif T. Drug Utilization at Household Level in Nekemte Town and Surrounding Rural Areas, Western Ethiopia: A Cross-Sectional Study. Open Access Library Journal. 2014;1:e651. | ||
Ali H. Self-medication practices in private pharmacies of Kolfe Keraneo Sub-city, Addis Ababa, Ethiopia. Harar Bulletin of Health Sciences. 2012;5:390–409. | ||
Suleman S, Ketsela A, Mekonnen Z. Assessment of self-medication practices in Assendabo town, Jimma zone, southwestern Ethiopia. Research in Social and Administrative Pharmacy. 2009;5:76–81. | ||
Gedif T. Self medication and its determinants in Butajira, southern Ethiopia. [master’s thesis]. Addis Ababa: Addis Ababa University; 1995. |
 © 2017 The Author(s). This work is published and licensed by Dove Medical Press Limited. The
full terms of this license are available at https://www.dovepress.com/terms
and incorporate the Creative Commons Attribution
- Non Commercial (unported, 3.0) License.
By accessing the work you hereby accept the Terms. Non-commercial uses of the work are permitted
without any further permission from Dove Medical Press Limited, provided the work is properly
attributed. For permission for commercial use of this work, please see paragraphs 4.2 and 5 of our Terms.
© 2017 The Author(s). This work is published and licensed by Dove Medical Press Limited. The
full terms of this license are available at https://www.dovepress.com/terms
and incorporate the Creative Commons Attribution
- Non Commercial (unported, 3.0) License.
By accessing the work you hereby accept the Terms. Non-commercial uses of the work are permitted
without any further permission from Dove Medical Press Limited, provided the work is properly
attributed. For permission for commercial use of this work, please see paragraphs 4.2 and 5 of our Terms.