Back to Journals » Infection and Drug Resistance » Volume 13
Self-Medication Practice and Associated Factors Among Health Professionals at the University of Gondar Comprehensive Specialized Hospital: A Cross-Sectional Study
Authors Simegn W ![]() , Dagnew B
, Dagnew B ![]() , Dagne H
, Dagne H ![]()
Received 10 April 2020
Accepted for publication 5 July 2020
Published 24 July 2020 Volume 2020:13 Pages 2539—2546
DOI https://doi.org/10.2147/IDR.S257667
Checked for plagiarism Yes
Review by Single anonymous peer review
Peer reviewer comments 4
Editor who approved publication: Professor Suresh Antony
Wudneh Simegn,1 Baye Dagnew,2 Henok Dagne3
1Department of Pharmaceutics, School of Pharmacy, University of Gondar, Gondar, Ethiopia; 2Department of Human Physiology, School of Medicine, University of Gondar, Gondar, Ethiopia; 3Department of Environmental and Occupational Health and Safety, Institute of Public Health, University of Gondar, Gondar, Ethiopia
Correspondence: Wudneh Simegn Email [email protected]
Background: Self-medication is the use of medication to treat self-diagnosed disorders or symptoms. In the current time, there has been an increasing tendency in self-medication in pharmacies and retail outlets in our country Ethiopia and alarmingly high in healthcare professionals. In spite of the adverse impacts, there were scarcity of data on self-medication practice among health professionals in Ethiopia. Therefore, this study aimed to determine the practice of self-medication and its determinant factors among health professionals at the University of Gondar Comprehensive Specialized Hospital, Northwest Ethiopia.
Methods: A Cross-sectional study design was employed using a simple random sampling technique to recruit the study participants. We used self-administered questionnaires to collect the data. Epi Info 7 and SPSS 20 were used for data entry and statistical analysis, respectively. Frequencies and mean with standard deviation were computed. Measure of association between self-medication and independent factors was determined using logistic regression. Variables with a p< 0.05 were declared as determinant factors of self-medication practice.
Results: Four hundred and twelve health professionals were involved in the study with a mean age of 29.9 years (± 5.43, range=20– 60). In this study, self-medication practice was 54.6% (95% CI: 49.8– 59.4). Health professionals who had worked less than 3 years after last graduation (AOR=1.67, 95% CI (1.02, 2.76)), those with 44– 55 working hours per week (AOR=2.44, 95% CI: 1.07,5.57), and who knew over-the-counter classification of drugs (AOR=1.75, 95% CI: 1.03,2.99) had significantly higher self-medication practice.
Conclusion: Self-medication practice was remarkably high in the current study which is a major public health problem. The findings suggest a cooperative implementation of pharmaceutical regulations particularly focusing on those health professionals with high working hours per week.
Keywords: self-medication, health professionals, Gondar
Background
Self-medication (SM) is the use of drugs to treat self-diagnosed disorders or symptoms or taking non-prescribed medicines.1–3 Currently, SM is increasing in Pharmacies or retail outlets.4 The practice of SM could have both benefits and risks in that appropriate use can save scarce medical resources from being wasted, reduce the burden on health-care facilities, and reduce the cost and time people spend visiting health care facilities for minor symptoms.5
Self-medication is an important concern for health authorities at global level and cannot be considered as entirely harmful.6 Despite the above-mentioned benefits, irrational use of medications (antibiotics) could lead to the emergence of resistant pathogens which is a major concern7,8 whereby inappropriate use of SM may lead to lack of public trust for the profession,9 serious health outcomes, and death.4,10 Drug resistance demands high cost and leads to greater morbidity and mortality.11 Due to the benefits and risks, SM practice requires better experience and education to the general population and the health professions to reduce inappropriate use.7
Self-medication practices are alarmingly high in health-care professionals which is associated with age, sex, income, expenditure, education level, medical knowledge, and perception of illnesses.4 It is known that health professionals are familiar with drugs so they are different from the general population in terms of drug use.12,13 It is considered due to a high level of professional education as a predictive factor for SM practice.14,15 Health professionals are more likely to be practicing SM due to the fact they believe that they are knowledgeable about the medicines used.16 In Ethiopia, SM has become a common phenomenon17 as described in different populations. Few studies conducted in Ethiopia have described SM practice among different populations particularly focusing on a specific profession.5 No such study had been conducted at the Comprehensive specialized hospital level. Therefore, the current study was designed to determine SM practice and its determinant factors among health professionals at the University of Gondar Comprehensive Specialized Hospital, Northwest Ethiopia.
Methods
Study Design
This institution-based cross-sectional study was carried out on health professionals working at the University of Gondar Comprehensive Specialized Hospital, Northwest Ethiopia, which is located 728 Km away from Addis Ababa, the capital city of Ethiopia. The Hospital serves as a referral center for the nearby general hospitals and provides clinical services for over 5 million inhabitants in the northwest region of Ethiopia. The data collection period was from June to August, 2019.
Study Questions
The current study was intended to answer the following questions. First, what was the practice of SM among health professionals? Secondly, what were the associated factors of SM practice among health professionals at the University of Gondar Comprehensive Specialized Hospital?
Sample and Sampling Method
The sample size (n) was calculated using single population proportion formula with the assumptions of the proportion =0.5, 95% uncertainty interval (UI), and margin of error (d) = 5%. After adding a non response rate of 10%, the final sample size was 423. Stratification was done by department (profession). Samples were determined by proportional allocation for each profession. Then, we applied a lottery method for recruiting study units (health professionals) using a simple random sampling technique. A questionnaire was provided to each consented participant. All health professionals who had been working for more than 1 year at the University of Gondar Comprehensive Specialized Hospital were included. The health professionals under study were nurses, pharmacists, medical doctors, midwives, and laboratory technologists. Health professionals who were severely ill during the data collection period, those who were unwilling, and those who were not present at the time of data collection were excluded.
Instrument
The questionnaire was composed of four sections. The first section was about sociodemographic variables (age, sex, marital status, work experience, profession etc.). The second section of the tool comprised of 22 items to assess knowledge. Respondents were asked 22 knowledge questions about whether they knew about antimicrobial resistance, the SM mean, that medication administration requires basic knowledge about drug action, that changing the time when taking a drug is hazardous, that antihypertensive drugs could not be discontinued when blood pressure returns to the normal range, that overuse of paracetamol will cause liver toxicity, that antacid should be chewed before swallowing, that improper use of medication can result in antimicrobial resistance, that not taking the full dose of a medication can have an effect, that SM can mask signs and symptoms, that drug use during pregnancy should be used with care, that all medications have their own adverse effects, that taking medicine with food, drink, tea, or alcohol can interfere with the effect of the medicine, that antibiotics often have side effects such as diarrhea, that antibiotics cause negative effects on the body’s own bacterial flora, that they should terminate a therapy immediately if they feel better after only taking a partial course of antibiotics, that bacteria can become resistant to antibiotics, that people can become resistant to antibiotics, that antibiotics use for animals can reduce the possibility of effective antibiotics treatment for humans, that antibiotics resistance can spread from animals to humans and that antibiotics resistance can spread from person to person. The fourth section was related to practice of self medication among health professionals: whether they ever took SM or not, reasons for SM practice, diseases most frequently encountered to use SM, source of information for SM practice, and frequently used drugs for SM. The third was about attitude towards SM with 11 items (whether they perceive that SM is part of self-care; if they believe pharmacists are a good source of information for minor medical problems); the course of medicines should be complete although the symptoms subside; do all health-care workers have good ability to treat symptoms; whether they believe that SM is acceptable for health-care workers; whether they believe that health-care workers have good ability to diagnose the symptoms after SM; if they think that SM would be harmful if they are taken without proper knowledge of drugs and disease; whether a medical license should be essential for better administration of drugs; wether they thought that they should be careful with non-prescribed over-the-counter medicines; if they think that health-care workers should check the accompanying medication leaflet; whether they think SM is not acceptable at all and it would be harmful regarding attitude of SM with a four-point Likert-scale from 0 (strongly disagree) to 3 (strongly agree). We used semi-structured, pretested self-administered questionnaire to collect the required data after preparing the questionnaire by reviewing the different literature. In this study, SM was considered when a person used medicines by his/her own decision without a prescription from another health professional to treat self-diagnosed illnesses or symptoms.18 The overall reliability of the items used for knowledge and attitude of SM was performed and we found a Cronbach’s alpha of 0.84 which is good reliability.19 Content validity was assured by delivering the questionnaire to two epidemiologists and then we included the comments from them.
Data Collection Method
The data collection was using self-administered semistructured questionnaires. First, we prepared the questionnaire after reviewing previous literature.4,20,21 After obtaining Ethical approval from the School of Pharmacy, University of Gondar, four BSc Nurses were recruited to distribute and return the questionnaire and facilitate the collection process. Before conducting the actual study, orientation was given to facilitators about the purpose of the study and ethical issues. Pretest was done among 20 health professionals outside of the study area and we amended the questionnaire after obtaining feedback from pretest results. The purpose of the study was explained to each study participant to assure their willingness. Any possible identifiers were eliminated from the questionnaire to ascertain confidentiality. Finally, facilitators provided the questionnaire to each participant and then returned after completion.
Statistical Analysis
After checking for the completeness and consistency, data were entered into the Epi-info 7.1 and then exported into SPSS version 20 for computing, recoding, and further analysis. We used chi-square test to compare each independent variable by SM. Continuous variables were described using mean standard deviation (SD) whereas categorical variables were presented using frequency with percent. Point prevalence and its 95% UI were used to describe the practice of self-medication. Binary logistic regression model was used to find out possible candidate variables for the final model. An independent variable with a p-value of <0.2 was entered into a multivariable binary logistic regression. In the final model, a variable with a p-value of ≤0.05 with 95% uncertainty interval was treated as a significant factor for self-medication practice. The strength of association between independent factors and SM was measured using odds ratio with its 95% UI.
Results
A total of 423questionnaires were distributed to the participants and 412 health professionals voluntarily agreed to participate in this study representing a response rate of 97.4%. The mean age of respondents was 29.9 years (±5.43) which ranged from 20–60 years. From the participants 220 (53.4%) participants were males, 339 (82.3%) participants attended educational level of Bachelor’s degree. Overall, 142 (34.5%) participants had a minimum of 2 years work experienceand 196 (47.6%) professionals were nurses. A total of 172 (41.7%) participants reported that they had a high work load and 117 (28.4%) participants reported having a high work load outside of the hospital (Table 1).
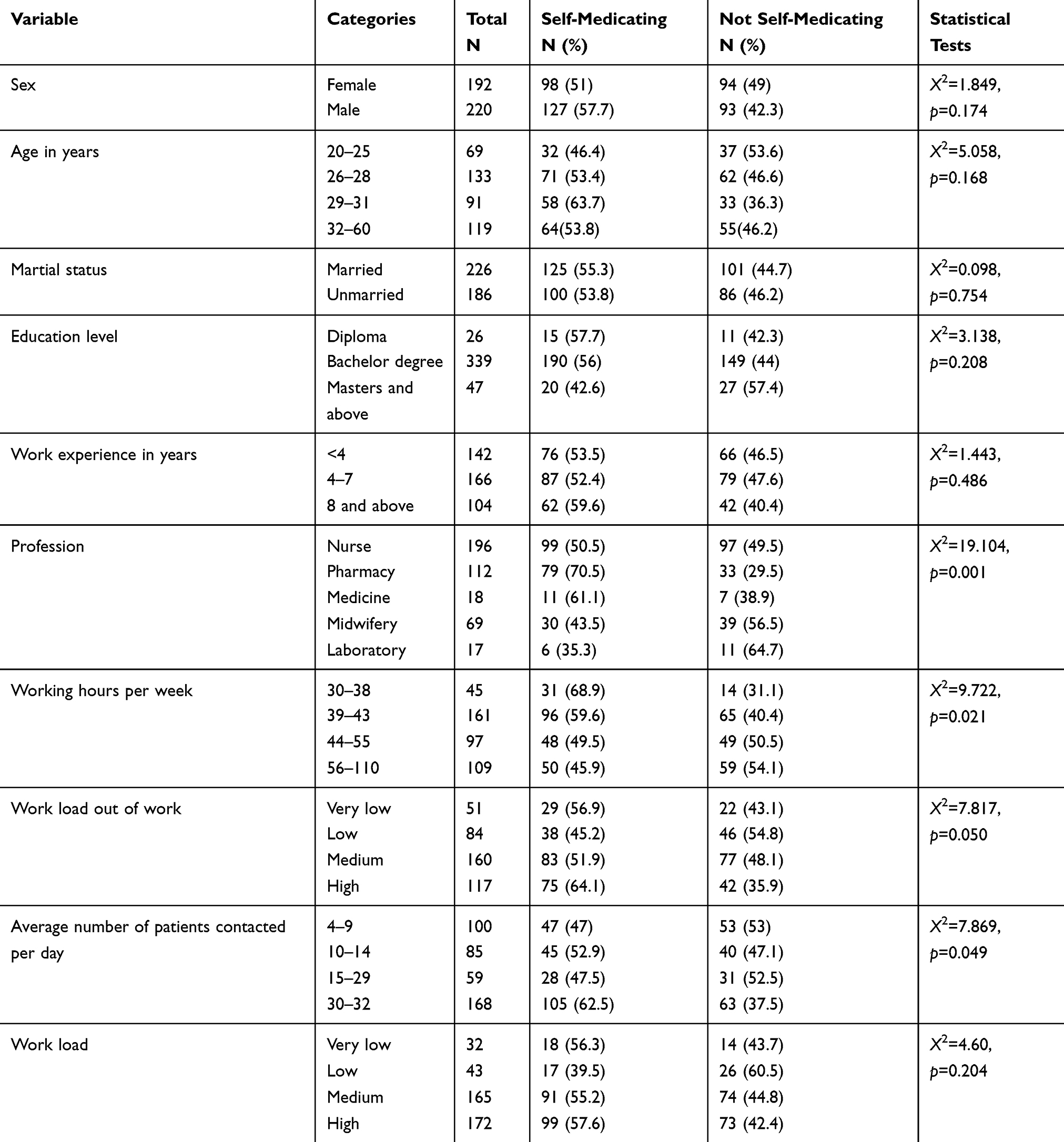 |
Table 1 Sociodemographic Characteristics of Study Participants from the University of Gondar Comprehensive Specialized Hospital, Gondar, Ethiopia, 2019 (n=412) |
Self-Medication Practice and Associated Factors
From a total of 412 respondents, 225 (54.6%, 95% CI:49.8–59.4) reported SM practice in their life to treat self recognized illnesses/symptoms. A total of 311 (75.5%) health professionals revealed they knew the OTC drugs classification. Overall, 138 (61.3%) claimed non-seriousness of illness as a reason for SM, drugs related to antipain were frequently used by 78.4% of health professionals, and 67.2% participants practice SM for headache (Table 2).
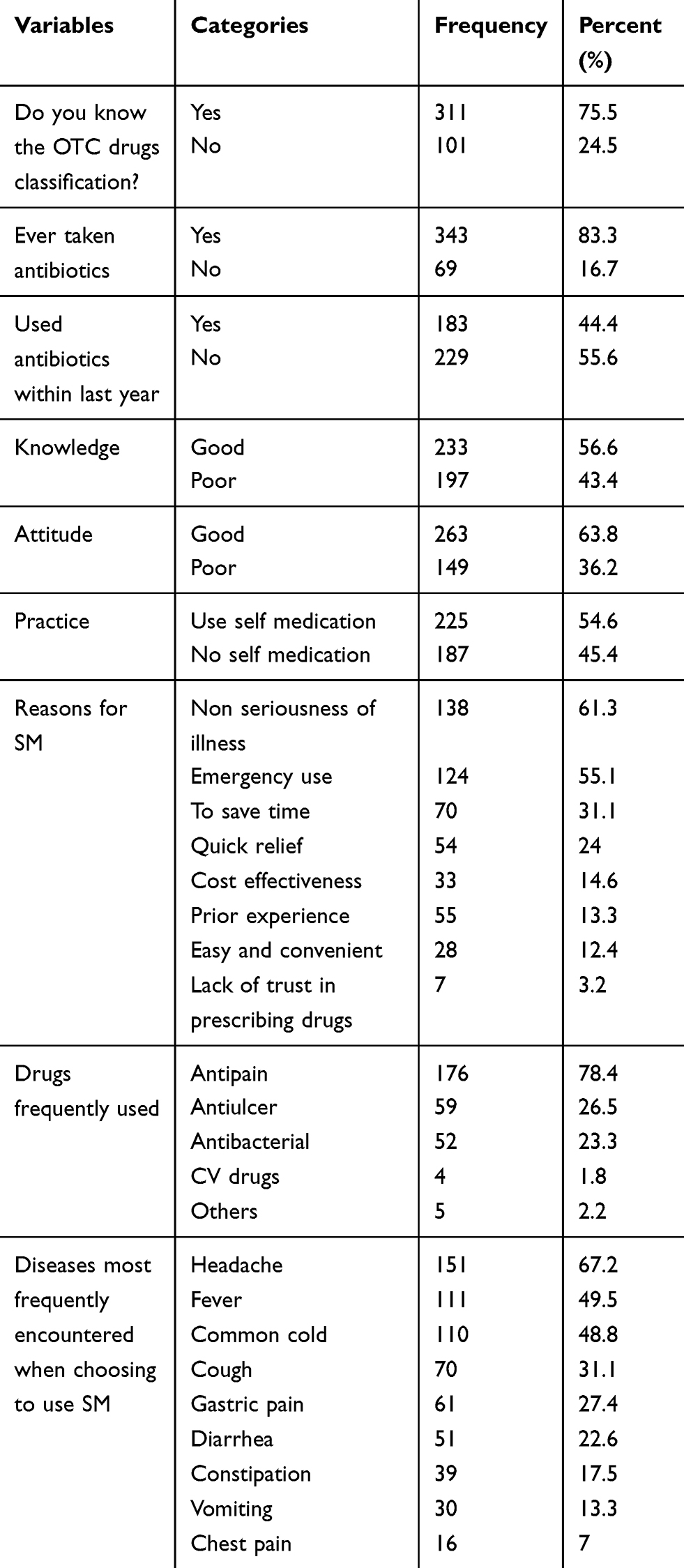 |
Table 2 Self-Medication Practice and Related Characteristics Among Health Professionals at the University of Gondar Comprehensive Specialized Hospital, Northwest Ethiopia, 2019 (n=412) |
We checked bivariable association of all independent factors with SM using binary logistic regression. Sex, profession, years after last graduation, working hours per week, average patients contacted per day, work load, knowledge about OTC classification of drugs, and ever taking antibiotics were candidate variables for the final model and entered into the multivariable logistic regression. In the final model; participants with less than 3 years after last graduation had 1.5-fold (AOR=1.67, 95% UI (1.02, 2.76)) higher practice of SM than their counterparts. The odds of having SM practice was 2.5 times higher (AOR=2.44, 95% UI: (1.07,5.57)) among respondents who had 44–55 working hours per week than those with 56–110 working hours per week. Furthermore, health professionals who had knowledge of OTC classification of drugs had 1.75 times (AOR=1.75, 95% UI: (1.03,2.99)) higher SM practice than their counterparts (Table 3).
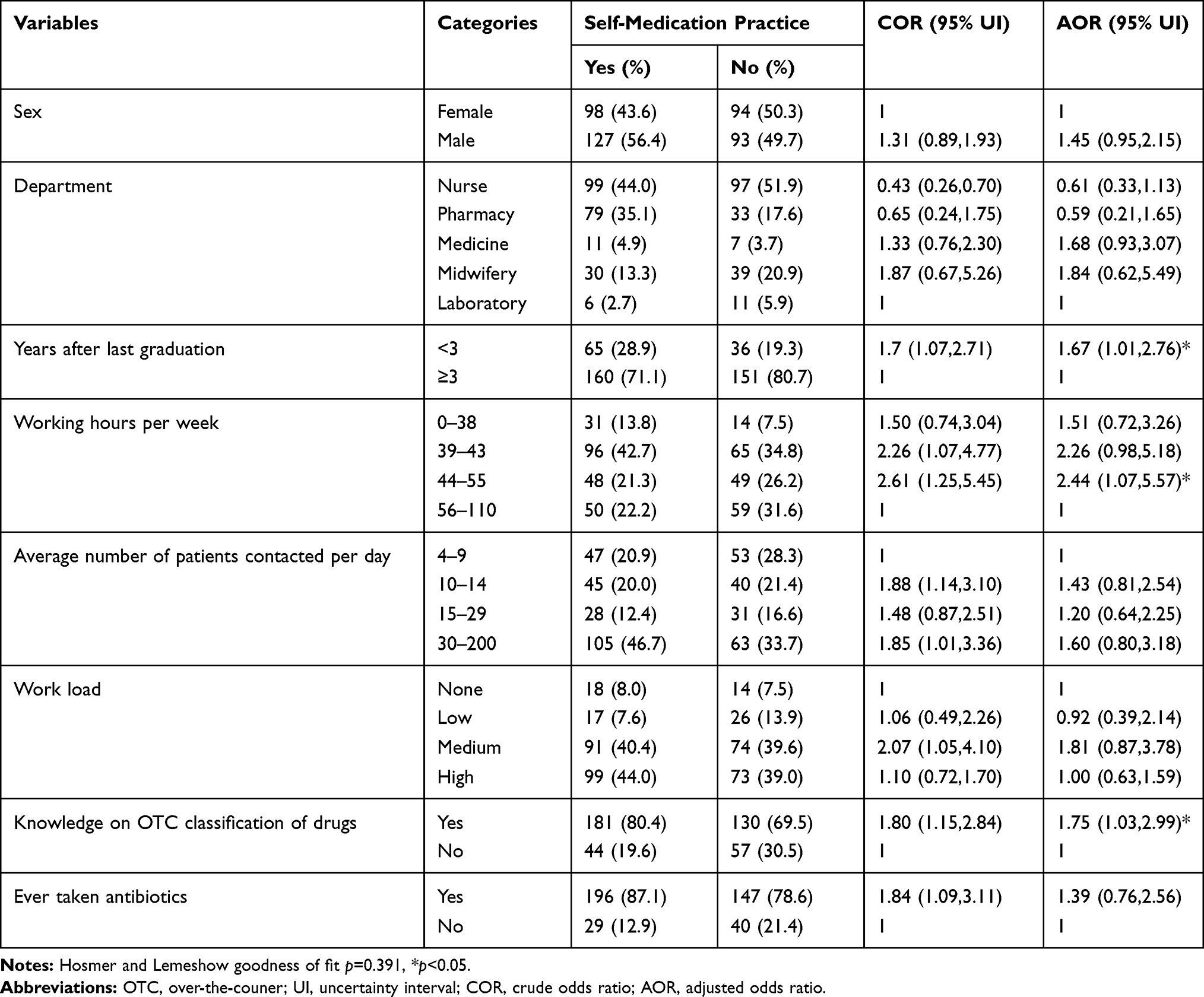 |
Table 3 Associated Factors of SM Practice Among Health Professionals at the University of Gondar Comprehensive Specialized Hospital, Gondar, Northwest Ethiopia, 2019 (n=412) |
Discussion
Self-medication practice is higher in developing countries like Ethiopia and exerts huge health impacts particularly on the emergence of drug-resistant pathogens.3,5 The current study aimed to describe the practice of SM and associated factors among health professionals at the University of Gondar Comprehensive Specialized Hospital, northwest Ethiopia. In the current study, the prevalence of SM practice among health professionals was 54.6% (95% UI: 49.80–59.40%). The period since last graduation, working hours per week, and knowledge on over-the-counter classification of drugs were significantly associated factors of SM practice.
The prevalence of SM in our study is consistent with a previous study in Nigeria (52.1%).22 However, our findings disclosed a lower self-medicaton practice than studies in Nekemte town, Western Ethiopia (67.5%),12 UAE (96.6%),23 Nigeria (73%),24 India (87.5%),16 and Malaysia (77.6%).4 This difference might be due to differences in sample size, setting, socioeconomic gaps, sampling method, and law enforcement. On the other hand, the current study revealed a higher prevalence of self-medication than other studies as observed in Brazil (24.2%).25 This might be because the study in Brazil only used nurses as study population and also sample size, methods used, and economic differences might be accountable for the variation.
In this study the pharmacy professionals had higher indications of self-medication practice (70.5%) followed by physicians (61.1%), and nurses (50.5%). This is supported by other findings in Jamaica where pharmacists practiced higher SM.26 It may be due to the fact that pharmacists can access the drugs easily as they are front-line workers of drugs and drug products.27 As observed in this study “non seriousness of the illness“ was among the main reasons for SM practice which is similar wth other studies.4,12,23,28 This study found headache was the major condition that subjected health professionals to SM that is similar with other studies.4,28 Antipain and antiulcer (gastrointestinal drugs) were the two most frequently used drugs for SM practice in this study. The first group of drugs (analagesics) were in line with the study done in Nekemte.12,16 This might be because the analgesics are dominantly available as over-the-counter.
In the current study, study participants who had less than 3 years after last graduation were 1.7-fold more likely to practice SM than their counterparts. The association might be due to the fact that new professionals are not familier with health risks that can occur if inappropriate SM has been used. It is a new finding since similar findings were not found for comparison. And also it might be related with work experience as newer graduates may have less work experience29 and hence were susceptible for SM practice as was observed by another study.4 Health professionals with 44–55 working hours per week had 2.4 times greater SM practice than those participants with 56–110 working hours per week. This could be explained as health professionals with low working time may have free time to read materials like leaflets, books, and to access information on drug use thereby they could have high ability and confidence to select drugs for themselves. However, no study incorporated this variable and so we were not able to compare it with others. The odds of having SM was 1.75 times higher among health professionals who reported that they knew the classifications of OTC drugs than who those who did not know the classification of OTC drugs. This finding is clearly understandable whereby knowledge of OTC drugs can help respondents to consider self-medication practice.4
Limitations of the Study
The possible limitations in the current study includes social desirability and recall bias. In addition, the cause-effect relationship cannot be established as this is a cross-sectional study. The use of binary logistic instead of poisson regression may lead to overestimation of association between the outcome and covariates.
Conclusion
The current study showed that SM practice is common among health professinals. Non-seriousness of the illness, was the main reason to practice SM. Period since last graduation, working hours per week, and knowledge on over-the-counter classification of drugs were significantly associated factors of SM practice. It is better to create awareness on the risk of SM especially on newly graduated health professionals and there is a need for the government to tailor restrictions on drug use without prescription.
Abbreviations
AOR, adjusted odds ratio; COR, crude odds ratio; OTC over-the-counter; SD, standard deviation; SM, self-medication.
Data Sharing Statement
The dataset can be obtained from the corresponding author upon reasonable request.
Ethical Approval and Consent to Participate
Ethical approval was gained from the ethical committee of the School of Pharmacy, University of Gondar with ethical review protocol number: SOP/559/2019. All participants were informed about the purpose of the study. Written informed consent was obtained from each participant to assure their willingness of participation and no identifiers were listed in the questionnaire to make it confidential.
Acknowledgments
The authors are grateful to the study participants, the Academic Committee of the School Of Pharmacy, University of Gondar and the data collectors.
Author Contributions
All authors made a significant contribution to the work reported, in the conception, study design, execution, acquisition of data, analysis and interpretation, and in all these areas; took part in drafting, revising or critically reviewing the article; gave final approval of the version to be published; have agreed on the journal to which the article has been submitted; and agree to be accountable for all aspects of the work.
Disclosure
The authors report no conflicts of interest in this work.
References
1. Lukovic JA, Miletic V, Pekmezovic T, et al. Self-medication practices and risk factors for self-medication among medical students in Belgrade, Serbia. PLoS One. 2014;9(12):e114644. doi:10.1371/journal.pone.0114644
2. Chouhan K, Prasad SB. Self-medication and their consequences: a challenge to health professional. Asian J Pharm Clin Res. 2016;9(2):314–317.
3. Ayalew MB. Self-medication practice in Ethiopia: a systematic review. Patient Prefer Adherence. 2017;11:401. doi:10.2147/PPA.S131496
4. Ali AN, Kai JTTK, Keat CC, et al. Self-medication practices among health care professionals in a Private University, Malaysia. Int Curr Pharm J. 2012;1(10):302–310. doi:10.3329/icpj.v1i10.11846
5. Beyene A, Getachew E, Doboch A, et al. Knowledge, attitude and practice of self medication among pharmacy students of Rift Valley University, Abichu campus, Addis Ababa, Ethiopia. J Health Med Inform. 2017;8(03):2. doi:10.4172/2157-7420.1000269
6. Selvaraj K, Kumar SG, Ramalingam A. Prevalence of self-medication practices and its associated factors in Urban Puducherry, India. Perspect Clin Res. 2014;5(1):32. doi:10.4103/2229-3485.124569
7. Ocan M, Bwanga F, Bbosa GS, et al. Patterns and predictors of self-medication in northern Uganda. PLoS One. 2014;9(3):e92323. doi:10.1371/journal.pone.0092323
8. Jain S, Malvi R, Purviya JK. Concept of self medication: a review. Int J Pharm Biol Arch. 2011;2(3):831–836.
9. Montgomery A, Bradley C, Rochfort A, et al. A review of self-medication in physicians and medical students. Occup Med (Chic Ill). 2011;61(7):490–497. doi:10.1093/occmed/kqr098
10. Murray MD, Callahan CM. Improving medication use for older adults: an integrated research agenda. Ann Intern Med. 2003;139(5_Part_2):425–429. doi:10.7326/0003-4819-139-5_Part_2-200309021-00009
11. Stansfield SK, Walsh J, Prata N, Evans T. Information to improve decision making for health. Dis Control Priorities Dev Countries. 2006;2.
12. Sado E, Kassahun E, Bayisa G, et al. Epidemiology of self-medication with modern medicines among health care professionals in Nekemte town, western Ethiopia. BMC Res Notes. 2017;10(1):533. doi:10.1186/s13104-017-2865-5
13. Boateng DP, Self-medication among doctors and pharmacists at the Korle Bu Teaching Hospital. 2009.
14. Kalyan VS, Padma T, Pratap K, et al. Evaluation of self-medication practices among undergraduate dental students of tertiary care teaching dental hospital in South India. J Educ Ethics Dent. 2013;3(1):21. doi:10.4103/0974-7761.126939
15. Paula Martins A, da Costa Miranda A, Mendes Z, et al. Self‐medication in a Portuguese urban population: a prevalence study. Pharmacoepidemiol Drug Saf. 2002;11(5):409–414. doi:10.1002/pds.711
16. Sajith M, Suresh SM, Roy NT, et al. Self-medication practices among health care professional students in a tertiary care hospital, Pune. Open Public Health J. 2017;10(1):63–68. doi:10.2174/1874944501710010063
17. Sisay M, Mengistu G, Edessa D. Epidemiology of self-medication in Ethiopia: a systematic review and meta-analysis of observational studies. BMC Pharmacol Toxicol. 2018;19(1):56. doi:10.1186/s40360-018-0248-8
18. Abay S, Amelo W. Assessment of self-medication practices among medical, pharmacy, health science students in Gondar University, Ethiopia. J Young Pharm. 2010;2(3):306–310. doi:10.4103/0975-1483.66798
19. Dagnew B, Dagne H, Andualem Z. Depression and its determinant factors among University of Gondar medical and health science students, Northwest Ethiopia: institution-based cross-sectional study. Neuropsychiatr Dis Treat. 2020;16:839. doi:10.2147/NDT.S248409
20. Dilie A, Tenaw G, Dessalegn H, et al. Knowledge, attitude and practice of self-medication among health science students at Debre Markos university, Northwest Ethiopia. J Public Health Epidemiol. 2017;9(5):106–113. doi:10.5897/JPHE2017.0926
21. Patel P, Prajapati A, Ganguly B, et al. Study on impact of pharmacology teaching on knowledge, attitude and practice on self-medication among medical students. Int J Med Sci Public Health. 2013;2(2):181–186. doi:10.5455/ijmsph.2013.2.173-178
22. Babatunde OA, Fadare JO, Ojo OJ, et al. Self-medication among health workers in a tertiary institution in South-West Nigeria. Pan Afr Med J. 2016;24.
23. Sharif SI, Bugaighis LM, Sharif RS. Self-medication practice among pharmacists in UAE. Pharmacol Pharm. 2015;6(09):428. doi:10.4236/pp.2015.69044
24. Bamgboye E, Amoran O, Yusuf O. Self medication practices among workers in a tertiary hospital in Nigeria. Afr J Med Med Sci. 2006;35(4):411–415.
25. Barros ARR, Griep RH, Rotenberg L. Self-medication among nursing workers from public hospitals. Revista Latino-Americana De Enfermagem. 2009;17(6):1015–1022. doi:10.1590/S0104-11692009000600014
26. Balbisi EA, Ambizas EM. Self-prescribing of noncontrolled substances among pharmacists. Am J Health Syst Pharm. 2005;62(23):2508–2511. doi:10.2146/ajhp050007
27. Chiarello E. The war on drugs comes to the pharmacy counter: frontline work in the shadow of discrepant institutional logics. Law Social Inq. 2015;40(1):86–122. doi:10.1111/lsi.12092
28. Abdi A, Faraji A, Dehghan F, et al. Prevalence of self-medication practice among health sciences students in Kermanshah, Iran. BMC Pharmacol Toxicol. 2018;19(1):36. doi:10.1186/s40360-018-0231-4
29. Haider S, Thaver IH. Self-medication or self-care: implication for primary health care strategies. J Pak Med Assoc. 1995;45:297.
 © 2020 The Author(s). This work is published and licensed by Dove Medical Press Limited. The
full terms of this license are available at https://www.dovepress.com/terms
and incorporate the Creative Commons Attribution
- Non Commercial (unported, 3.0) License.
By accessing the work you hereby accept the Terms. Non-commercial uses of the work are permitted
without any further permission from Dove Medical Press Limited, provided the work is properly
attributed. For permission for commercial use of this work, please see paragraphs 4.2 and 5 of our Terms.
© 2020 The Author(s). This work is published and licensed by Dove Medical Press Limited. The
full terms of this license are available at https://www.dovepress.com/terms
and incorporate the Creative Commons Attribution
- Non Commercial (unported, 3.0) License.
By accessing the work you hereby accept the Terms. Non-commercial uses of the work are permitted
without any further permission from Dove Medical Press Limited, provided the work is properly
attributed. For permission for commercial use of this work, please see paragraphs 4.2 and 5 of our Terms.