Back to Journals » Clinical Ophthalmology » Volume 20
Selenium Supplementation in Graves’ Orbitopathy: Effects on Blood Concentrations and Clinical Outcomes
Authors Lumyongsatien M, Vejsitthangkul K, Treebuppachatsakul T, Sintuwong S, Nimitwongsakul O, Pongpirul K
Received 23 September 2025
Accepted for publication 23 January 2026
Published 9 February 2026 Volume 2026:20 569805
DOI https://doi.org/10.2147/OPTH.S569805
Checked for plagiarism Yes
Review by Single anonymous peer review
Peer reviewer comments 2
Editor who approved publication: Dr Scott Fraser
Mingkwan Lumyongsatien,1 Kittiphum Vejsitthangkul,1 Thitipon Treebuppachatsakul,1 Sunisa Sintuwong,1 Ornvenus Nimitwongsakul,1 Krit Pongpirul2
1Department of Ophthalmology, Metta Pracharak (Wat Rai Khing) Hospital, Nakhon Pathom, Thailand; 2Center of Excellence in Preventive and Integrative Medicine (CE-PIM), Chulalongkorn University, Bangkok, Thailand
Correspondence: Mingkwan Lumyongsatien, Department of Ophthalmology, Metta Pracharak (Wat Rai Khing) Hospital, 52 Moo 2 Rhikhing, Nakhon Pathom, 73210, Thailand, Email [email protected]
Objective: To evaluate changes in blood selenium concentrations and associated clinical outcomes following selenium supplementation in patients with Graves’ orbitopathy (GO) with varied severity.
Study Design: A retrospective study.
Patients and Methods: We retrospectively reviewed the medical records of patients with GO who received selenium supplementation with a total daily dose of 210 μg for six months at a single tertiary care center between January 2019 and January 2021. Clinical parameters, including visual acuity, exophthalmos, eyelid aperture, Clinical Activity Score (CAS), GO severity, Graves’ Ophthalmopathy Quality of Life (GO-QoL) scores, and selenium concentrations were assessed at baseline and post-treatment. Subgroup analysis was performed for patients who received no concurrent GO treatment.
Results: Forty-eight patients (52.1% female, mean age 46.33± 11.47 years) were included, with disease severity classified as mild (22.9%), moderate-to-severe (70.8%), and sight-threatening (6.3%). The mean selenium concentrations increased from 90.46± 16.40 μg/L to 113.67± 19.64 μg/L (mean difference: 23.21± 24.75 μg/L; 95% CI: 16.02– 30.39, P< 0.001). Of 37 patients who did not receive other GO treatments, CAS improved significantly in 13 (35.13%; P=0.02), and the prevalence of eyelid edema decreased from 22.2% to 5.6% (P=0.03). GO-QoL appearance subscale scores significantly improved (mean change: 8.16± 23.14; 95% CI: 0.33– 15.99; P=0.04), while the changes in visual function scores were not statistically significant.
Conclusion: Selenium supplementation was associated with a significant increase in selenium concentrations and clinically significant improvements in CAS, eyelid edema, and quality of life among patients with GO. These findings support the potential role of selenium therapy in GO management. However, larger randomized controlled trials are warranted to confirm these observations and guide dosage recommendations.
Keywords: selenium supplementation, blood concentration, Graves’ orbitopathy
Introduction
Graves’ orbitopathy (GO) is an inflammatory autoimmune disorder affecting approximately 25–50% of patients with Graves’ hyperthyroidism (GH).1 The pathogenesis involves cross-reactivity between antigens shared by thyroid follicular cells and orbital fibroblasts. Infiltrating lymphocytes in orbital and perivascular tissues initiate an inflammatory cascade mediated by cytokines, growth factors and reactive oxygen species (ROS).1,2 These mediators stimulate orbital fibroblasts to proliferate and differentiate into adipocytes and myofibroblasts, leading to excessive production of hydrophilic glycosaminoglycans. The resulting expansion of orbital tissue contributes to the characteristic clinical signs and symptoms of GO.
Selenium (Se) is an essential micronutrient with potent antioxidant and anti-inflammatory properties. It plays a key role in thyroid hormone metabolism through the activity of 25 known selenoproteins that incorporate selenocysteine at their active center.3 The highest Se concentration in the human body is found in the thyroid gland, where selenoenzymes—including glutathione peroxidase (GPX), thioredoxin reductase, and iodothyronine deiodinase—help neutralize ROS generated during thyroid hormone synthesis.4
Serum selenium and circulating selenoprotein concentrations are commonly used to assess Se status. Se deficiency has been associated with various thyroid disorders, such as hypothyroidism, subclinical hypothyroidism, autoimmune thyroiditis, goitre, and Graves’ disease.5–7 Patients with GO tend to have lower Se concentrations than those with Graves’disease (GD) without orbitopathy.8,9 Se insufficiency has also been linked to more severe manifestation of GO.8,9
The potential benefits of Se supplementation in GD and GO have drawn increasing attention. A systematic review of 10 randomized trials found that Se improved thyroid function at both 3 and 6 months.10 Another meta-analysis of four randomized controlled trials (RCT) demonstrated that Se supplementation improved clinical outcomes and quality of life of patients with GO relative to placebo.11 However, it remains unclear whether Se should be used exclusively in patients with Se deficiency or also in those with optimal Se intake. Moreover, the narrow therapeutic window poses safety concerns, as excessive intake may approach toxic levels.4 Plasma Se concentrations higher than 122 μg/L before supplementation have been associated with an increased risk of cancer and type-2 diabetes.3 Se levels above 150 μg/L are linked to a moderate increase in mortality.12 Clinical presentations of Se toxicity include nausea, vomiting, nail brittleness, nail discoloration, hair loss, fatigue, irritability and garlic breath odor.13
Changes in serum Se concentrations following supplementation in GO patients have been rarely documented in the literatures. Previous trials have employed variable dosages and durations, often without coordinated assessment of both clinical outcomes and Se concentrations.14
This study aimed to assess the changes in blood Se concentrations following six months of supplementation and to evaluate corresponding clinical outcomes in Thai patients with GO. Our findings may contribute to a more personalized and evidence-based approach to Se therapy in this population.
Materials and Methods
Study Design and Ethics Approval
The retrospective observational study was conducted at the thyroid eye disease clinic of Metta Pracharak (Wat Rai Khing) Hospital. It was approved by the Institutional Review Board of the Metta Pracharak (Wat Rai Khing) hospital (IRB approval number: 024/2566) and adhered to the principles of the Declaration of Helsinki. Patients were identified through electronic medical records from January 2019 to January 2021. Informed consent was obtained from all included patients after providing a detailed explanation of the study and the use of their data for the research purposes.
The Sample Size Calculation
The sample size was calculated using the formula for dependent means (paired t-test). Based on our pilot study, the mean selenium concentration in patients with GO before supplementation was 97.99 ± 20.45 μg/L, while the predicted post-supplementation concentration was 106.95 μg/L, similar to levels observed in a healthy Thai population.9 A clinically significant difference was set at 0.05 (type I error = 0.05, two-sided), with a type II error of 0.2 and a power of 80%. To account for a 20% dropout rate, a total sample size was calculated to be 48 participants.
Participants
The inclusion criteria were patients aged ≥ 18 years who were diagnosed with GO and completed six months of selenium supplementation. The exclusion criteria included eating disorders, gastrointestinal absorption disorders, selenium allergy, pregnancy, breastfeeding, chronic kidney disease, Se concentration ≥ 120 μg/L or vision loss unrelated to GO.
Data Collection
Demographic data collected included age, sex, smoking history, underlying comorbidities, thyroid disease diagnosis, thyroid status at enrolment, and prior treatments for thyroid disease and GO. The clinical parameters were recorded at baseline and after six months of Se supplementation, and they included serum Se concentration, visual acuity (VA), exophthalmos measurements, eyelid aperture width, Clinical Activity Score (CAS), disease severity according to the EUGOGO classification, and Graves’ ophthalmopathy quality of life (GO-QoL) scores.
GO Assessment Criteria
The CAS was calculated using a seven-item scale, included: (1) spontaneous retrobulbar pain, (2) pain on eye movement, (3) eyelid redness, (4) conjunctival redness, (5) eyelid swelling, (6) caruncle or plica swelling, and (7) chemosis. A CAS of ≥ 3 denoted active disease. GO severity was categorized as follows: (1) mild: eyelid retraction of < 2 mm, mild soft tissue involvement, exophthalmos of < 3 mm above race- and sex-adjusted norms, intermittent diplopia, and corneal exposure responsive to lubricants; (2) moderate-to-severe: eyelid retraction of ≥ 2 mm, moderate/severe soft tissue involvement, exophthalmos of ≥ 3 mm and or persistent diplopia; and (3) sight-threatening: dysthyroid optic neuropathy or corneal breakdown. All clinical assessments were conducted by trained ophthalmologists using the GO Clinical Evaluation Atlas and confirmed by a single oculoplastic surgeon for consistency at the thyroid eye disease clinic.
Quality of Life Assessment
Quality of life was evaluated using the validated Thai version of the GO-QoL questionnaire,15 which consists of 16 items across two subscales: visual function and appearance. A change of ≥ 6 points for either subscale was considered the minimal clinically important difference (MCID).16
Se Supplementation and Laboratory Analysis
All patients at the thyroid eye disease clinic underwent routine assessments of their Se status at baseline. Patients with baseline blood Se concentrations below 120 μg/L received Se amino acid complex tablets (The British Dispensary (L.P). Co., Ltd, Samut Prakan, Thailand), with a total daily dose of 210 µg (3 tablets of 70 µg each) for six months, based on previous clinical trials data.11 Blood samples were collected at baseline and six months. Serum was separated by centrifugation and analysed at the Faculty of Medical Technology, Mahidol University, using graphite furnace atomic absorption spectrophotometry (SpectrAA 600, Varian, Victoria, Australia) with a selenium-specific electrode discharge lamp.
Statistical Analyses
Descriptive statistics were used to summarize the demographic and clinical characteristics. Categorical variables were presented as frequencies and percentages. Continuous variables were expressed as mean ± standard deviation or median with interquartile range, depending on data distribution. For inferential analysis, paired t-test was used to assess the changes in normally distributed continuous variables, whereas Wilcoxon signed-rank test was used for non-normally distributed data. McNemar’s or exact tests were applied to paired categorical data, as appropriate. To evaluate changes in clinical outcomes specifically attributable to Se supplementation, a subgroup analysis was conducted for patients who did not receive other GO treatments during the six-month supplementation. A 95% confidence interval (CI) was calculated for each comparison. P value of < 0.05 denoted statistically significance. All statistical analyses were performed using SPSS version 28.0 (IBM Corp., Chicago, IL, USA).
Results
Participant Characteristics
Forty-eight patients were included in this study. Their baseline demographic data and clinical characteristics are summarized in Table 1. Their mean age was 46.33 ± 11.47 years, and 52.1% (n=25) were female. Most participants (93.8%) were diagnosed with GD, and 79.2% were in a euthyroid state at the time of enrolment. GO severity was classified as mild for 11 patients (22.9%), moderate-to-severe for 34 patients (70.8%), and sight-threatening for 3 patients (6.3%). The mean CAS at baseline was 0.73 ± 0.96 (range: 0–3), indicating that most cases were inactive. During the six-month period of Se supplementation, 11 patients (22.91%) received other treatments for GO: systemic steroid alone in 1 case (2.08%), surgery alone in 7 cases (14.58%), and combined steroid and surgery in 3 cases (6.25%). Two patients (4.1%) reported mild side effects, including nausea and flatulence. No severe adverse reactions or toxicity were observed.
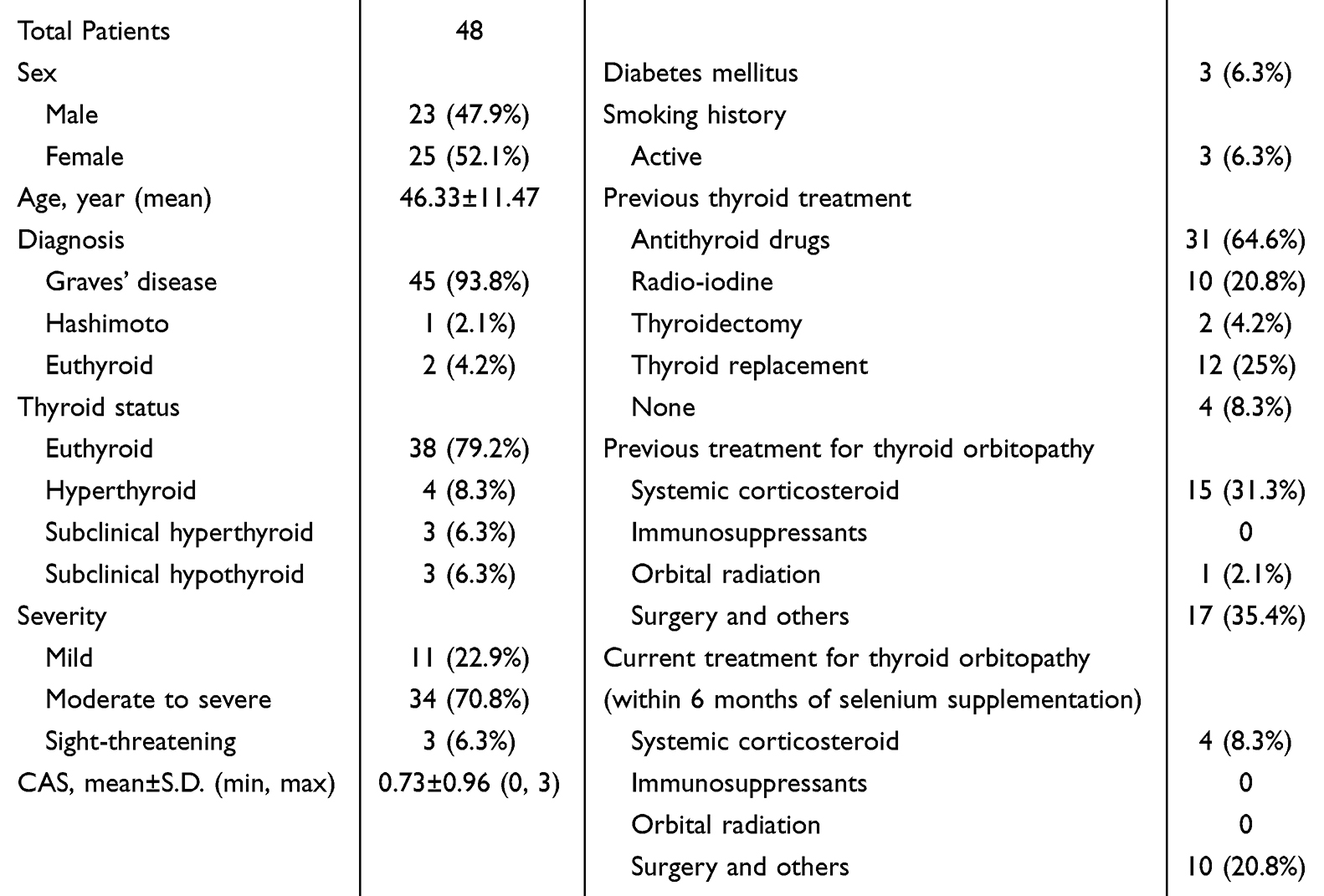 |
Table 1 Demographic Data of the Patients |
Change in Se Concentrations
The serum Se concentrations significantly increased after supplementation. The mean Se concentration increased from 90.46 ± 16.40 µg/L at baseline to 113.67 ± 19.64 µg/L at six months (mean difference: 23.21 ± 24.75 µg/L; 95% CI: 16.02–30.39, P<0.001) (Figure 1). Most individual patients demonstrated an upward trend in Se concentrations (Figure 2).
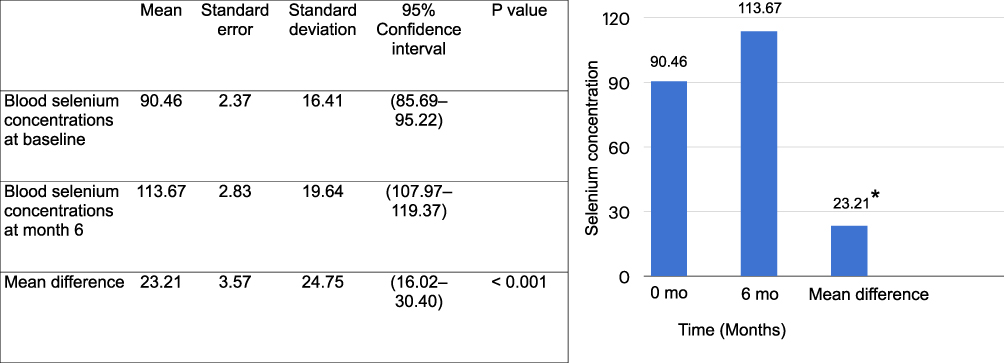 |
Figure 1 Blood selenium concentrations (µg/L) before and after treatment. * p-value < 0.05. |
 |
Figure 2 Scattered plot of individual blood selenium concentrations before and after therapy. |
Clinical Outcomes After Se Supplementation
Subgroup analysis was performed for 37 patients who did not receive concurrent GO treatment during the study period. Improvements in several clinical parameters were observed. CAS significantly improved in 13 patients (35.13%) at six months (P=0.02), with no deterioration observed in others. The number of patients with eyelid edema significantly decreased from 8 (22.2%) at baseline to 2 (5.6%) at six months (P=0.03).
Quality of Life (GO-QoL) Scores
Quality of life improved for both GO-QoL subscales (Table 2 and Figure 3). The mean appearance subscale score increased from 65.97 ± 27.85 to 74.13 ± 23.91 (mean difference: 8.16 ± 23.14; 95% CI: 0.33–15.99, P=0.04). The mean visual functioning subscale score improved from 54.69 ± 30.33 to 61.81 ± 29.08, but the difference did not reach statistical significance (mean difference: 7.12 ± 30.00; 95% CI: −3.03–17.27, P=0.16).
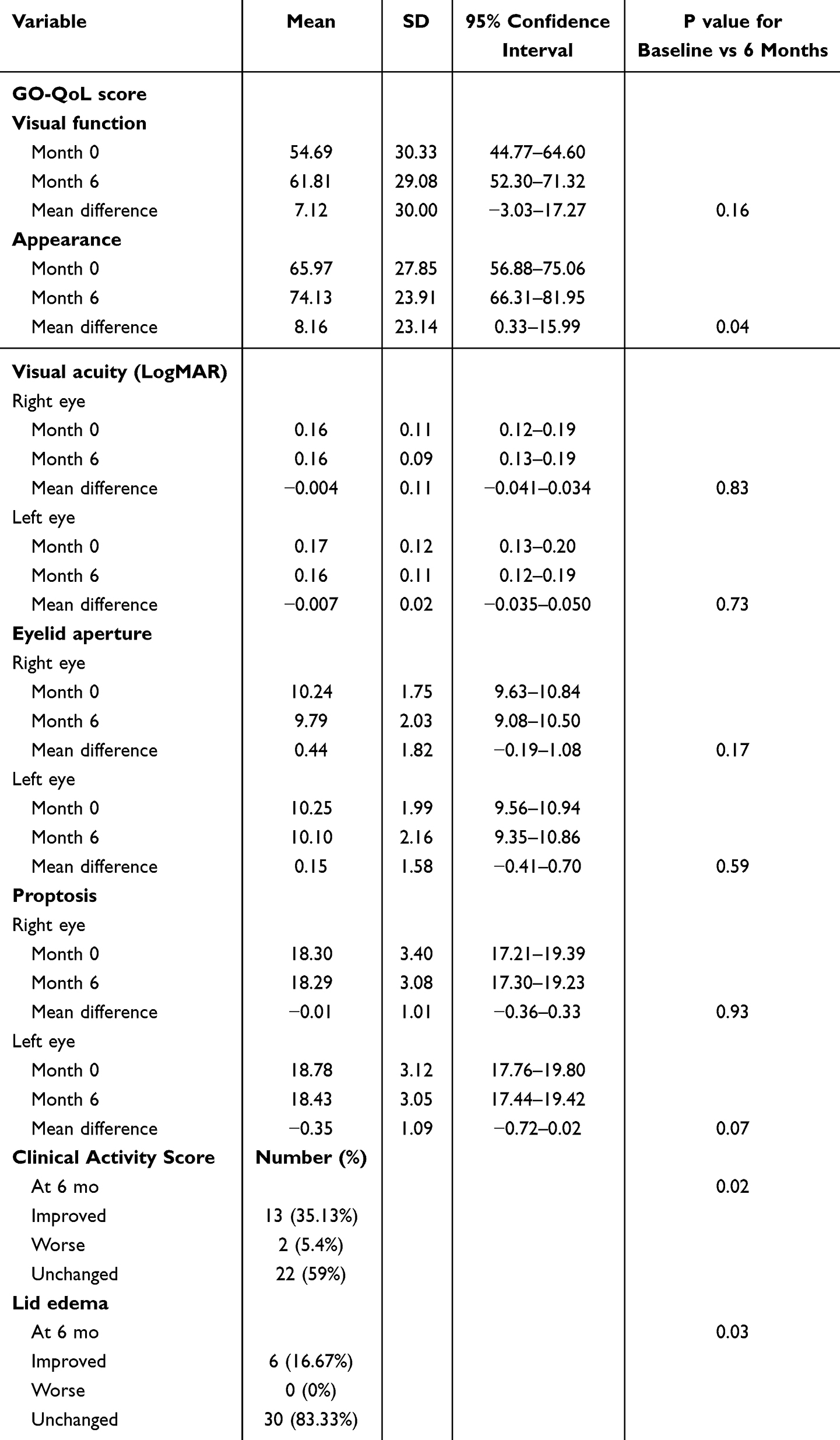 |
Table 2 GO-QoL Score and Clinical Parameters Before and After Treatment |
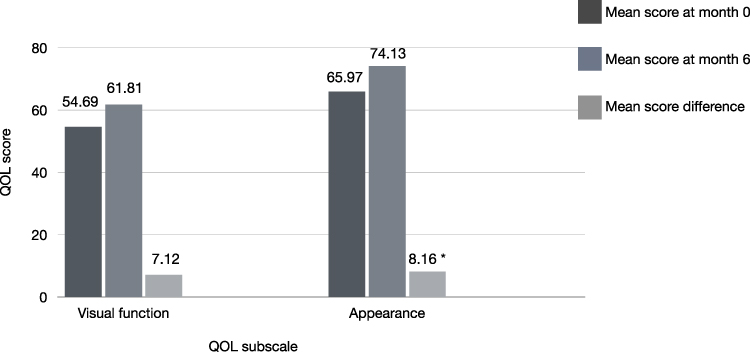 |
Figure 3 GO-QoL scores for functional and appearance subscales. * p-value < 0.05. |
Other Ocular Parameters
No statistically significant changes were observed in visual acuity (LogMAR), eyelid aperture width, or exophthalmos measurements in either eye (P > 0.05 for all comparisons) (Table 2).
Discussion
This retrospective study evaluated the effect of Se supplementation on serum Se concentrations and clinical outcomes in Thai patients with GO. Our findings demonstrate that a six-month supplementation regimen with 210 µg/day of Se significantly increased serum Se concentrations and was associated with clinical improvements, especially in CAS, eyelid edema, and quality of life as measured by GO-QoL scores.
The optimal range for serum Se is estimated to be between 90–120 μg/L, which is considered sufficient for maximal selenoprotein expression.17 In our study, the baseline Se concentrations were within or near this optimal range, but supplementation still led to significant increments (mean difference: 23.21 µg/L; P<0.001), indicating that additional Se may provide therapeutic benefits even for individuals who are not overtly deficient. However, excessive Se intake can pose risks, including disturbances in endocrine function, and has been associated with increased incidence of type 2 diabetes and certain cancers.17,18 These findings underscore the need for individualized dosing and careful monitoring of Se status before and during supplementation.9
Consistent with reports of previous randomized controlled trials,11,19–21 we observed clinical benefits of Se therapy in patients with GO. CAS improved significantly in over one-third of patients without concurrent GO treatment (P=0.02), and the prevalence of eyelid edema was significantly reduced (P=0.03). While we did not observe significant changes in proptosis or eyelid aperture, our findings support the hypothesis that Se may primarily influence soft tissue inflammation and activity rather than structural changes in GO such as proptosis, diplopia, and eyelid retraction. Although Se mainly reduces oxidative stress and inflammation, it is less effective in addressing structural changes due to the several reasons: it predominantly targets inflammation rather than tissue remodeling and fibrosis; structural alterations result from complex interactions among fibroblasts, adipocytes, and cytokines, which Se does not directly affect; by the time these structural changes become apparent, GO may have progressed to an inactive phase with minimal inflammation; and Se does not significantly influence fibroblast proliferation or preadipocyte differentiation, which contribute to orbital structural alterations.
Moreover, to compare these findings with the natural course of the disease, a placebo group in a teprotumumab study showed a 21% reduction in CAS at six months.22 In a series of untreated thyroid eye disease (TED) patients in the UK, 22% experienced substantial improvement, 42.4% showed minimal change, 22% remained stable and 14% deteriorated.22,23
Improvements in quality of life were evident, especially for the appearance subscale of the GO-QoL questionnaire. This aligns with previous studies showing that Se supplementation enhances patient-reported outcomes.11,19 The visual function subscale showed a trend toward improvement, but the change did not reach statistical significance, similar to findings in a Thai population,21 possibly due to the low baseline CAS and relatively inactive disease status of most participants.
Our study adds to the growing body of literature by demonstrating real-world changes in Se concentrations along with clinical outcomes. It is among the first in Thailand to assess the biochemical response to Se therapy in patients with GO and provides region-specific data to support clinical decision-making.
However, several limitations should be acknowledged. The relatively small sample size may have limited the power to detect changes in certain outcomes. The absence of a control group and reliance on retrospective data may have introduced bias. Additionally, subgroup analysis was performed to isolate the effect of Se, and residual confounding from unmeasured variables cannot be excluded.
Conclusion
This study demonstrates that Se supplementation significantly increased serum Se concentrations, with a mean difference of 23.21 ± 24.75 µg/L, and may support the concept of individualized Se dosing. Clinically significant benefits were observed across patients with varying severities of inactive GO, especially in the improvement of CAS, reduction of eyelid edema, and enhancement of GO-QoL appearance scores. These findings suggest that Se supplementation may serve as a valuable adjunctive therapy in GO management while ensuring safety. However, further research involving larger sample sizes and randomized controlled trials is necessary to validate these outcomes and develop evidence-based guidelines for Se use in patients with GO.
Funding
This study received research funding from Metta Pracharak (Wat Rai Khing) Hospital, Department of Medical Service, Ministry of Public Health, Thailand.
Disclosure
All authors report no conflicts of interest in this work.
References
1. Bahn RS. Current insights into the pathogenesis of Graves’ ophthalmopathy. Horm Metab Res. 2015;47(10):773–9. doi:10.1055/s-0035-1555762
2. Marinò M, Menconi F, Rotondo Dottore G, et al. Selenium in Graves hyperthyroidism and orbitopathy. Ophthalmic Plast Reconstr Surg. 2018;34(4S):S105–S110. doi:10.1097/IOP.0000000000001136
3. Rayman MP. Selenium and human health. Lancet. 2012;379(9822):1256–1268. doi:10.1016/S0140-6736(11)61452-9
4. Gorini F, Sabatino L, Pingitore A, et al. Selenium: an element of life essential for thyroid function. Molecules. 2021;26(23):7084. doi:10.3390/molecules26237084
5. Wu Q, Rayman MP, Lv H, et al. Low population selenium status is associated with increased prevalence of thyroid disease. J Clin Endocrinol Metab. 2015;100(11):4037–4047. doi:10.1210/jc.2015-2222
6. Bülow Pederson I, Knudsen N, Carlé A, et al. Serum selenium is low in newly diagnosed Graves’ disease: a population-based study. Clin Endocrinol. 2013;79(4):584–590. doi:10.1111/cen.12185
7. Wertenbruch T, Willenberg HS, Sagert C, et al. Serum selenium levels in patients with remission and relapse of graves’ disease. Med Chem. 2007;3(3):281–284. doi:10.2174/157340607780620662
8. Khong JJ, Goldstein RF, Sanders KM, et al. Serum selenium status in Graves’ disease with and without orbitopathy: a case–control study. Clin Endocrinol. 2014;80(6):905–910. doi:10.1111/cen.12392
9. Lumyongsatien M, Bhaktikamala U, Thongtong P, et al. Relative selenium insufficiency is a risk factor for developing severe Graves’ orbitopathy: a case-control study. BMJ Open Ophthalmol. 2021;6(1):e000713. doi:10.1136/bmjophth-2021-000713
10. Zheng H, Wei J, Wang L, et al. Effects of selenium supplementation on Graves’ disease: a systematic review and meta-analysis. Evid Based Complement Alternat Med. 2018;2018(1):3763565. doi:10.1155/2018/3763565
11. Sharabati I, Qafesha RM, Hindawi MD, et al. The efficacy and safety of selenium supplementation versus placebo in the treatment of Graves’ orbitopathy: a systematic review and meta-analysis of randomised controlled trials. Clin Endocrinol. 2024;101(6):669–681. doi:10.1111/cen.15128
12. Bleys J, Navas-Acien A, Guallar E. Serum selenium levels and all-cause, cancer, and cardiovascular mortality among US adults. Arch Intern Med. 2008;168(4):404–410. doi:10.1001/archinternmed.2007.74
13. MacFarquhar JK, Broussard DL, Melstrom P, et al. Acute selenium toxicity associated with a dietary supplement. Arch Intern Med. 2010;170(3):256–261. doi:10.1001/archinternmed.2009.495
14. Lanzolla G, Marinò M, Marcocci C. Selenium in the treatment of Graves’ hyperthyroidism and eye disease. Front Endocrinol. 2021;11:608428. doi:10.3389/fendo.2020.608428
15. Lumyongsatien M, Keeratidamkerngsakul B, Pornpanich K, et al. Development and psychometric properties of the Thai Graves’ ophthalmopathy quality of life (GO-QOL) questionnaire. J Patient Rep Outcomes. 2019;4(1):1. doi:10.1186/s41687-019-0164-8
16. Terwee CB, Dekker FW, Mourits MP, et al. Interpretation and validity of changes in scores on the Graves’ ophthalmopathy quality of life questionnaire (GO-QOL) after different treatments. Clin Endocrinol. 2001;54(3):391–398. doi:10.1046/j.1365-2265.2001.01241.x
17. Radomska D, Czarnomysy R, Radomski D, et al. Selenium as a bioactive micronutrient in the human diet and its cancer chemopreventive activity. Nutrients. 2021;13(5):1649. doi:10.3390/nu13051649
18. Kim J, Chung HS, Choi MK, et al. Association between serum selenium level and the presence of diabetes mellitus: a meta-analysis of observational studies. Diabetes Metab J. 2019;43(4):447–460. doi:10.4093/dmj.2018.0123
19. European Group on Graves’ Orbitopathy; Marcocci C, Kahaly GJ, Krassas GE, et al. Selenium and the course of mild Graves’ orbitopathy. N Engl J Med. 2011;364(20):1920–1931. doi:10.1056/NEJMoa1012985
20. Almanza-Monterrubio M, Garnica-Hayashi L, Dávila-Camargo A, et al. Oral selenium improved the disease activity in patients with mild Graves’ orbitopathy. J Fr Ophtalmol. 2021;44(5):643–651. doi:10.1016/j.jfo.2020.08.029
21. Potita P, Pruksakorn V, Srichomkwun P, et al. Selenium supplementation in inactive moderate to severe Graves’ orbitopathy patients: a randomized controlled trial. Orbit. 2024;43(3):329–336. doi:10.1080/01676830.2024.2315566
22. Bartalena L, Gallo D, Tanda ML, et al. Thyroid eye disease: epidemiology, natural history, and risk factors. Ophthalmic Plast Reconstr Surg. 2023;39(6S):S2–S8. doi:10.1097/IOP.0000000000002467
23. Perros P, Cromblie A, Kendall-Taylor P. Natural history of thyroid associated ophthalmopathy. Clin Endocrinol. 1995;42:45–50.
 © 2026 The Author(s). This work is published and licensed by Dove Medical Press Limited. The
full terms of this license are available at https://www.dovepress.com/terms
and incorporate the Creative Commons Attribution
- Non Commercial (unported, 4.0) License.
By accessing the work you hereby accept the Terms. Non-commercial uses of the work are permitted
without any further permission from Dove Medical Press Limited, provided the work is properly
attributed. For permission for commercial use of this work, please see paragraphs 4.2 and 5 of our Terms.
© 2026 The Author(s). This work is published and licensed by Dove Medical Press Limited. The
full terms of this license are available at https://www.dovepress.com/terms
and incorporate the Creative Commons Attribution
- Non Commercial (unported, 4.0) License.
By accessing the work you hereby accept the Terms. Non-commercial uses of the work are permitted
without any further permission from Dove Medical Press Limited, provided the work is properly
attributed. For permission for commercial use of this work, please see paragraphs 4.2 and 5 of our Terms.