Back to Journals » Clinical Ophthalmology » Volume 20
Segmentation Errors of Two Modern Biometers in 100 Eyes with Phakic Intraocular Lenses
Authors Monteiro S ![]() , Marques JH
, Marques JH ![]() , Abreu AC
, Abreu AC ![]() , Menéres P, Melo Beirão J
, Menéres P, Melo Beirão J ![]() , Pinto MDCB
, Pinto MDCB ![]()
Received 25 November 2025
Accepted for publication 17 February 2026
Published 5 June 2026 Volume 2026:20 579977
DOI https://doi.org/10.2147/OPTH.S579977
Checked for plagiarism Yes
Review by Single anonymous peer review
Peer reviewer comments 3
Editor who approved publication: Dr Bharat Gurnani
Sílvia Monteiro,1,2 João Heitor Marques,1,2 Ana Carolina Abreu,1,2 Pedro Menéres,1,2 João Melo Beirão,1,2 Maria do Céu Brochado Pinto1
1Refractive Surgery Unit of Ophthalmology Department, Centro Hospitalar Universitário de Santo António, Oporto, Portugal; 2Medical Sciences Department, Instituto de Ciências Biomédicas Abel Salazar, Oporto, Portugal
Correspondence: Sílvia Monteiro, Email [email protected]
An accurate calculation of intraocular lens (IOL) power is crucial for satisfactory refractive outcomes. The percentage of patients with a prediction error within ±0.5D after cataract surgery is only 73.7%, according to data from de European Registry of Quality Outcomes for Cataract and Refractive Surgery. In addition to the error in calculating the effective lens position, this may be due to errors in biometric measurements such as anterior chamber depth (ACD), axial length, and keratometry.1 All modern IOL power calculation formulas take into account the measured ACD and lens thickness (LT). The IOL Master 700® (Zeiss, Germany) – biometer 1 – and the ANTERION® (Heidelberg Engineering, Germany) – biometer 2 – are devices that use the swept-source optical coherence tomography (SS-OCT). Both identify all optical interfaces inside the eye and allow visualization of the segmentation lines.2
On the other hand, the increasing number of patients with cataract and that had been previously implanted with a phakic IOL pose an additional challenge.2 The accuracy in measuring ACD and LT seem to be prone to error in patients with phakic IOLs.3–5 The results are variable in the literature. In the study by Ribeiro et al, the anterior surface of the crystalline lens was misidentified in 194% of eyes.3 In another work the crystalline lens surface was misidentified in 75% of eyes.4 It remains unclear if any device is superior is measuring or segmenting eyes with phakic IOLs.
Our purpose was to analyze the automatic segmentation performed by the two devices on 100 eyes with implanted phakic IOLs (iris-fixated, posterior chamber and angle-supported phakic IOLs). The eyes were chosen at random from a list of patients implanted with phakic lenses. This study was performed according to the principles of the Declaration of Helsinki. Moreover, all exams performed are considered non-invasive. Eligible participants were enrolled after obtaining their acceptance and written informed consent for the study and for publication. The study was approved by our institutional review board and ethics committee – “Departamento de Ensino, Formação e Investigação” (DEFI), no: 2023–147(124-DEFI/118-CE). All data was saved and shared anonymously. The examinations were checked by two independent investigators and the cases in which the segmentation line misclassified the anterior or the posterior surface of the phakic IOL as the anterior surface of the crystalline lens were identified. Regarding the biometer 2, the cases in which no segmentation was assumed by the device were also signaled. The results are shown in the Table 1.
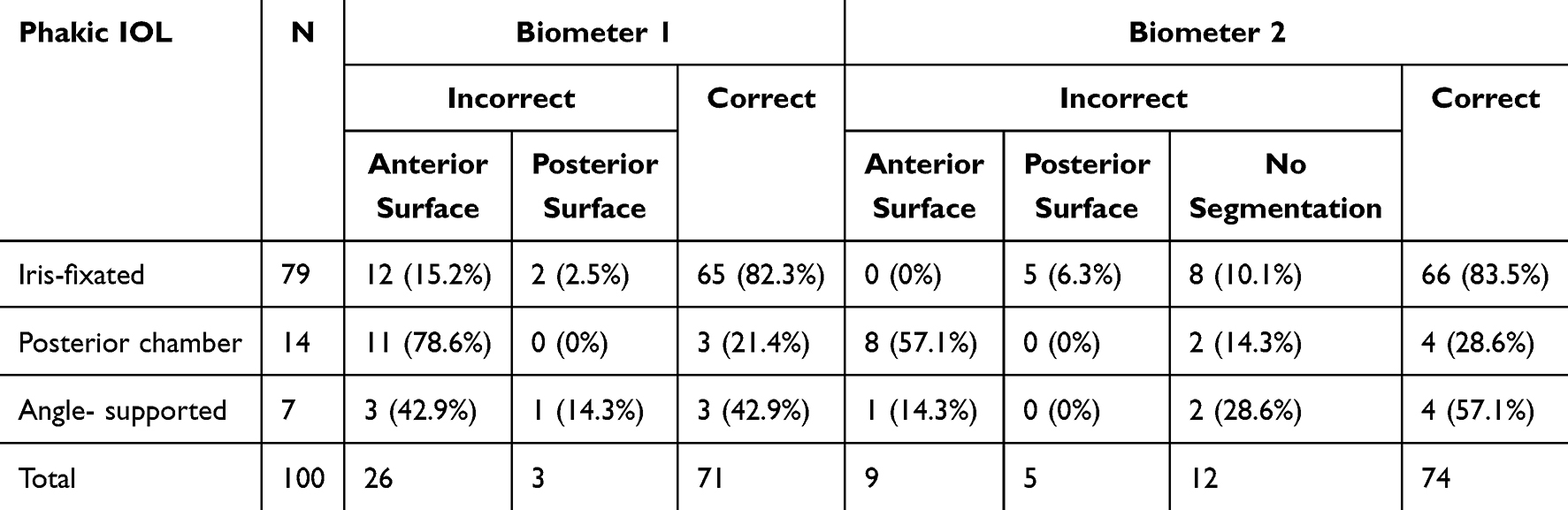 |
Table 1 Results of Segmentation Data with the Two Biometers. IOL – Intraocular Lens |
The percentage of doubtful segmentation cases was high with both devices: 26% and 29% with biometer 2 and 1, respectively (Figure 1). In all the incorrectly segmented eyes, there was an underestimation of ACD and an overestimation of LT. The segmentation with biometer 2 is more conservative: not only because it incorrectly segmented fewer eyes, but also because the device does not automatically segment some of these cases, forcing the operator to analyze the image and validate the segmentation manually. The biometer 1 is more prone to error as it always takes over either the anterior or posterior surface of the phakic IOL. The possibility of manually correcting the segmentation is also an advantage of biometer 2 over 1, which does not have this feature.
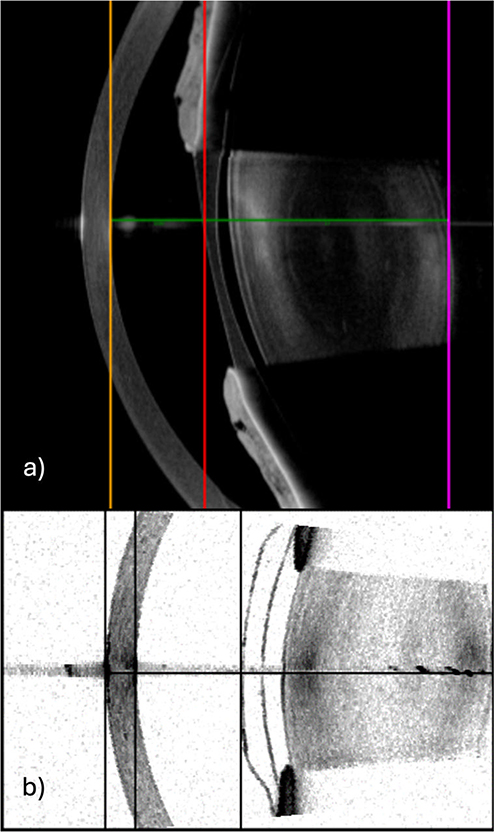 |
Figure 1 (a) Incorrect segmentation of a posterior chamber phakic IOL with biometer 2. Misidentification of the anterior surface of the crystalline lens as the anterior surface of the phakic IOL (red line). Yellow line: posterior corneal surface. Purple line: posterior surface of crystalline lens. Green line: line of sight. (b) Incorrect segmentation of an anterior chamber phakic IOL with biometer 1. Misidentification of the anterior surface of the crystalline lens as the anterior surface of the phakic IOL (third vertical line). First vertical line: anterior corneal surface. Second vertical line: posterior corneal surface. Horizontal line: line of sight. |
Even modern biometers may inaccurately estimate ACD and LT measurements, which highlights the importance of always check the quality of biometric measurements. In patients with phakic IOLs, it is important to validate the segmentation irrespectively of the biometer used. We emphasize the clinical importance of these results when choosing a biometer in patients with phakic IOLs. We recommend that is better to perform biometry with the biometer 2 in patients with phakic IOLs.
Funding
The authors received no funding.
Disclosure
The authors have no financial or proprietary interest in any material or method mentioned for this work.
References
1. Stopyra W, Langenbucher A, Grzybowski A. Intraocular lens power calculation formulas – a systematic review. Ophthalmol Ther. 2023;12(6):2881–3. doi:10.1007/s40123-023-00799-6
2. Aramberri J, Hoffer KJ, Olsen T, Savini G, Shammas HJ. Intraocular lens calculations. In: Essentials in Ophthalmology. Cleveland, OH, USA: Springer; 2024:17,22.
3. Ribeiro B, Monteiro S, Marques JH, Abreu AC, Pinto MC. Impact and correction of an anterior phakic intraocular lens on swept-source optical coherence tomography biometry. J Refract Surg. 2024;40(8):e562–e568. doi:10.3928/1081597X-20240716-01
4. Ouchi M. Evaluation of impact of posterior phakic IOL implantation on biometry and effectiveness of concomitant use of anterior segment OCT on IOL power calculation for cataract surgery. J Cataract Refract Surg. 2022;48(6):657–662. doi:10.1097/j.jcrs.0000000000000811
5. Zhang J, Xia J, Han X, et al. Accuracy of intraocular lens calculation formulas in patients undergoing combined phakic intraocular lens removal and cataract surgery. Am J Ophthamol. 2022;234:241–249. doi:10.1016/j.ajo.2021.09.035
 © 2026 The Author(s). This work is published and licensed by Dove Medical Press Limited. The
full terms of this license are available at https://www.dovepress.com/terms
and incorporate the Creative Commons Attribution
- Non Commercial (unported, 4.0) License.
By accessing the work you hereby accept the Terms. Non-commercial uses of the work are permitted
without any further permission from Dove Medical Press Limited, provided the work is properly
attributed. For permission for commercial use of this work, please see paragraphs 4.2 and 5 of our Terms.
© 2026 The Author(s). This work is published and licensed by Dove Medical Press Limited. The
full terms of this license are available at https://www.dovepress.com/terms
and incorporate the Creative Commons Attribution
- Non Commercial (unported, 4.0) License.
By accessing the work you hereby accept the Terms. Non-commercial uses of the work are permitted
without any further permission from Dove Medical Press Limited, provided the work is properly
attributed. For permission for commercial use of this work, please see paragraphs 4.2 and 5 of our Terms.