Back to Journals » Local and Regional Anesthesia » Volume 16
Segmental Thoracic Spinal Anesthesia for Laparoscopic Cholecystectomy with the “Hypobaric” Technique: A Case Series
Authors Vincenzi P ![]() , Stronati M, Garelli P, Gaudenzi D
, Stronati M, Garelli P, Gaudenzi D ![]() , Boccoli G, Starnari R
, Boccoli G, Starnari R
Received 29 October 2022
Accepted for publication 19 January 2023
Published 8 May 2023 Volume 2023:16 Pages 31—40
DOI https://doi.org/10.2147/LRA.S395376
Checked for plagiarism Yes
Review by Single anonymous peer review
Peer reviewer comments 2
Editor who approved publication: Prof. Dr. Stefan Wirz
Paolo Vincenzi,1 Massimo Stronati,2 Paolo Garelli,3 Diletta Gaudenzi,4 Gianfranco Boccoli,3 Roberto Starnari2
1Department of General Surgery, Ospedali Riuniti Marche Nord, Pesaro, Italy; 2Department of Anesthesiology, IRCSS-INRCA, Ancona, Italy; 3Department of General Surgery, IRCSS-INRCA, Ancona, Italy; 4Department of Perioperative Services, AOU “Ospedali Riuniti di Ancona”, Ancona, Italy
Correspondence: Paolo Vincenzi, Department of General Surgery, Ospedali Riuniti Marche Nord, Piazzale Cinelli n 1, Pesaro, 61121, Italy, Tel +39 3394578495, Email [email protected]
Purpose: Several studies have applied lumbar spinal anesthesia (SA) with isobaric/hyperbaric bupivacaine and opioids in elective laparoscopic cholecystectomy (LC), documenting a superiority of the methodic over general anesthesia (GA) in terms of perioperative pain, nausea, and vomiting, though with a notable incidence of intraoperative right shoulder pain, potentially responsible for conversion to GA. This case series presents an opioid-free scheme of segmental thoracic spinal anesthesia (STSA) with hypobaric ropivacaine, reporting its benefits mainly in terms of shoulder pain occurrence.
Patients and Methods: Hypobaric STSA was performed in nine patients undergoing elective LC between May 1 and September 1, 2022. The level of the needle insertion was included between T8 and T9, via a median or a paramedian approach. Midazolam (0.03 mg/kg) and Ketamine (0.3 mg/kg) were used as adjuvants for intrathecal sedation, followed by the administration of hypobaric ropivacaine 0.25% at a dose of 5 mg and then isobaric ropivacaine at a dose of 10 mg. Patients were placed in anti-Trendelenburg position for the entire duration of surgery. LC was conducted through the standard 3 or 4 ports technique with pneumoperitoneum maintained at a pressure of 8– 10 mmHg.
Results: Mean patient age was 75.7 (± 17.5) years, with a mean ASA score and Charlson comorbidity index (CCI) of 2.7 (± 0.7) and 4.9 (± 2.7), respectively. STSA was completed without complications in all patients, with no need for conversion to GA. Mean operative time and SA duration were 37.5 (± 8.7) and 145.2 (± 21.8) min, respectively. Intraoperatively, no shoulder or abdominal pain and nausea were reported, with only four and two patients requiring vasopressor and sedative intravenous drugs, respectively. Postoperatively, overall mean VAS pain score and within the first 12 hafter surgery were 3 (± 2) and 4 (± 2), respectively. Median length of stay was 2 (range = 1– 3) days.
Conclusion: Hypobaric opioid-free STSA appears to be a promising approach for laparoscopic surgeries, with minimal to null occurrence of shoulder pain. Larger prospective studies are required to validate these findings.
Keywords: thoracic spinal anesthesia, laparoscopic cholecystectomy, hypobaric ropivacaine, intrathecal midazolam, intrathecal ketamine
Introduction
Since the first description in 2006 of a laparoscopic cholecystectomy (LC) conducted under the method of combined spinal-epidural anesthesia in a patient with severe chronic obstructive pulmonary disease awaiting lung transplantation,1 the safety and feasibility of neuraxial anesthesia (NA), ie, spinal, epidural or combined techniques, in laparoscopic surgeries, have been documented in several reports.2–9
Accordingly, prospective randomized studies comparing spinal anesthesia (SA) with general anesthesia (GA) in LC have reported significantly reduced rates of postoperative pain, nausea, and vomiting, making SA an optimal technique to apply in elective laparoscopic surgical procedures on low-risk patients [American Society of Anesthesiologists (ASA) score 1 or 2], allowing faster patient recovery, early discharge, and hence reduced costs.10–20
However, the concerns for possible serious cardiovascular and respiratory alterations consequent to pneumoperitoneum-increased intra-abdominal pressure levels and to the SA-induced sympathetic blockade together with the fears, though generally unjustified, of spinal cord damage and the high occurrence of intraoperative right shoulder pain, have considerably limited the routine application of SA in elective LC.21,22
In particular, shoulder tip pain, documented intraoperatively in 10–55% of cases, has been generally recognized as a seriously distressing factor by the awake patient and, though usually relieved with administration of opioids, it might be responsible for conversion to GA in up to 10% of cases, according to different series.11,21,22
Moreover, while most of the reports in the literature on the utilization of SA during elective LC have adopted the lumbar puncture,5–7,9–13,15–18 with only isolated reports describing the thoracic puncture,2–4,8,14 all these series have applied isobaric and/or hyperbaric bupivacaine as intrathecal local anesthetics and opioids as adjuvants, the first requiring a Trendelenburg (head-down) position to obtain the optimal sensory block, with further possible negative repercussions on the cardiovascular, respiratory, and central nervous systems, and the second potentially associated with adverse effects such as respiratory depression, nausea, vomiting, and urinary retention.
Though recent series from our institution already illustrated the advantages of a segmental thoracic spinal anesthesia (STSA) technique in abdominal, urological, breast, and axillary surgery,23,24 maintaining at the same time the safety profile of lumbar anesthesia (LA), with the few sporadic reports existing in literature confirming these findings in LC,4,14 no previous studies have focused their attention on investigating potential alternative intrathecal local anesthetics and adjuvants that might reduce the drawbacks of the currently applied methods of NA in LC.
For these reasons, we present our initial experience of an opioid-free STSA with hypobaric ropivacaine used as local intrathecal anesthetic in LC.
Materials and Methods
Study Design and Population
All cases of elective LC conducted for cholelithiasis under the technique of STSA at the Italian National Research Center on Aging (INRCA) between May 1, 2022, and September 1, 2022, were reviewed, aiming at conducting a case series on this specific topic.
Exclusion criteria included acute cholecystitis, previous upper abdominal surgery, and previous episodes of acute pancreatitis.
Both anesthesia and surgery were performed by the same anesthesiologist and surgical team.
The study was approved by the INRCA Hospital Institutional Review Board, in accordance with the Helsinki Declaration.
All patients received extensive and detailed explanation of the procedure including the possibility of intraoperative conversion to GA if needed.
Written informed consent for publication of medical data and image material was obtained from all subjects or a legal surrogate.
Segmental Thoracic Spinal Anesthesia Technique
Colloid (500 mL) was administered before the procedure.
Under a fully aseptic technique with the patient in a sitting position, the correct intervertebral space, located between T8 and T9, was identified and the skin of the puncture site infiltrated with 3 mL of 2% lidocaine. The puncture was performed via a median or a paramedian approach using a 25-gauge Whitacre needle (B. Braun Medical Inc., Melsungen, Germany), as shown in Figure 1.
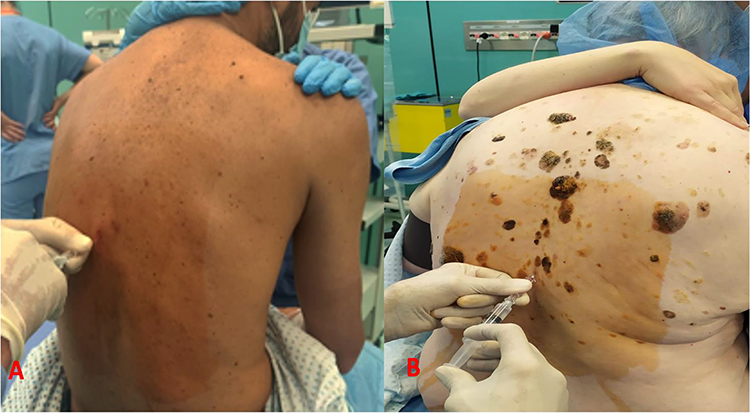 |
Figure 1 Insertion of the needle at T8–9: (A) paramedian approach. (B) median approach. |
Once clear flow of cerebrospinal fluid was established, preservative free midazolam (Accord Healthcare, Milan, Italy) at a dose of 0.03 mg/kg and preservative free ketamine (Molteni Pharmaceuticals, Florence, Italy) at a dose of 0.3 mg/kg were injected as adjuvants for intrathecal sedation, followed by the administration of hypobaric ropivacaine 0.25% (Bioindustria Pharmaceuticals, Novi Ligure, Italy) at a dose of 5 mg (1 mL of ropivacaine 1% diluted with 3 mL of distilled water for a total volume given equal to 2 mL) and isobaric ropivacaine 0.25% at a dose of 10 mg (1 mL of ropivacaine 1% diluted with 3 mL of saline for a total volume given equal to 4 mL).
Procedure-related paresthesias, pain, or any difficulty during spinal puncture were documented in each case.
The patients were then placed supine in a slight (5°) anti-Trendelenburg (head-up) position, then increased to 20° combined with modest rotation to the patient's left side after induction of pneumoperitoneum; this position was maintained for the entire duration of surgery until carbon dioxide insufflation was discontinued.
The level of the sensory blockade was tested using pinprick tests. When an adequate sensory block from the supraclavicular area (C3–C4) to the hypogastric region (T11–12) was achieved, the surgery was allowed to start.
In the case of patient anxiety and discomfort, an intravenous ketamine (0.4–0.5 mg/kg) and/or midazolam (0.02–0.05 mg/kg) bolus were administered.
All patients were spontaneously breathing in Venturi masks on 28–40% FiO2 and during surgery, another 500 mL of colloid was administered.
Standard hemodynamic and clinical monitoring, particularly the level of sensory blockade, were applied to all patients.
Hypotension, defined as a decrease in mean arterial blood pressure of more than 20% of the basal pre-anesthetic value,25 was managed with boluses of ephedrine at a dose of 6 mg.
Laparoscopic cholecystectomy was performed using the standard three or four-port technique and the open umbilical access to create the pneumoperitoneum; the intraperitoneal pressure was maintained between 8 and 10 mmHg.
At the end of the surgical procedure, patients were admitted to the recovery area, where they were monitored for at least 30 minutes and then transferred to the Surgical Unit.
Measurements
The Charlson Comorbidity Index (CCI)26 and the ASA score27 were used to determine the burden of comorbidities and the patient’s physiological status, respectively.
Preoperatively, patients were taught how to evaluate their own pain intensity using the visual analogue scale (VAS), scored from 0 to 10 (where 0=no pain and 10=the worst pain imaginable). Pain was assessed intraoperatively and postoperatively every 3 h for the first 12 h and then every 6 h until discharge of the patient. Any request for intravenous painkillers was noted. Only VAS pain scores greater than 4 were considered notable, and intravenous analgesics (Paracetamol 1 g or NSAIDs) were administered.
The level of sedation during surgery was assessed on a 5-point scale (modified Ramsay Sedation Scale): 0=alert, 1=easily arousable, 2=awakens after tactile stimulation, 3=awakens after verbal stimulation, and 4=not arousable,28 while the level of motor block was evaluated at the end of surgery on a 4-point scale (Bromage Scale): 1=able to lift extended legs, 2=just able to flex knees, full ankle movement, 3=no knee movement, some ankle movement, 4=complete paralysis.29
Overall duration of SA was defined as the period (min) included between the onset and the complete regression of the sensory block.
Respiratory depression was defined as a respiratory rate <10 breaths/min, oxygen saturation <90% by pulse oximetry lasting at least 3 min, hypercapnia (pCO2>50 mm Hg) or a change from baseline end-tidal CO2 >10 mmHg.30
Any intraoperative incidents, particularly those related to STSA, ie, right shoulder or abdominal pain, headache, discomfort, nausea, anxiety, hypotension and hemodynamic changes, or the necessity for a nasogastric tube, were recorded.
All patients were visited daily to assess any nerve root injury (radiculopathy, back pain, cauda equina), central nervous system complications (meningitis, spinal abscess, spinal hematoma), and post-dural puncture headache (PDPH).
At the outpatient clinic, 1 week after surgery, patients were asked to assess their degree of satisfaction (high, fair, bad) with the procedure. The same question was put to the first surgeon at the end of each surgical procedure.
Statistical Analysis
Frequency distributions were determined for baseline categorical variables, and the mean along with standard error (±SE) were calculated for baseline continuous variables. All of the statistical analysis was performed using the Statistical Analysis System (SAS) software, Version 9.4 (SAS Institute, Inc., Cary, NC).
Results
Nine cases were identified and described in Table 1, of whom 22.2% (2/9) were referred to our institution because of their deliberate and reiterated refusal of GA.
 |
Table 1 Baseline Characteristics of the Case-Series |
Overall, mean patient age was 75.7 (±17.5) years; the percentage of male patients being 44.4% (4/9), with a mean BMI of 26.6 (±4.8). Regarding the patient’s physiological status and comorbidities, mean ASA score and mean CCI were 2.7 (±0.7) and 4.9 (±2.7).
During all anesthetic and surgical procedures no major complications and no need for conversion from STSA to GA were reported, with 0% of patients describing right shoulder pain, abdominal discomfort, headache, and nausea, as shown in Table 2.
 |
Table 2 Operative Variables |
Intraoperative hypotension was documented exclusively in four cases (44.4%), with 25% (1/4) of these requiring more than one bolus of ephedrine, whereas intraoperative anxiety was recorded in two patients (22.2%) and resolved with a single bolus of ketamine and/or midazolam (Table 2).
The level of sedation recorded during surgery was: 2–3 for the whole duration of surgery in five cases (55.5%) and three for the entire operation in the other four (44.5%), while the level of motor block evaluated at the end of surgery was minimal, between 0 and 1 in all cases (100%, 9/9).
From the surgical point of view, it should be noted that in all cases (100%, 9/9) the muscular relaxation of the abdominal wall was complete and without interruptions.
Mean operative time was 37.5 (±8.7) min, while the mean duration of SA was 145.2 (±21.8) min (Table 2). A fourth port (epigastric) was used in three cases (33.3%) during the operation.
Postoperative course was uneventful in all cases (100%, 9/9) with a median length of stay of 2 (range 1–3) days; no patient (0%, 0/9) needed mechanical ventilation or presented any neurologic consequences related to SA and no episodes of post-operative nausea and vomiting (PONV) or urinary retention were reported, as detailed in Table 3.
 |
Table 3 Post-Operative Variables |
Regarding the analgesia, the overall mean postoperative VAS score and the mean VAS score registered within the first 12 h after surgery were 3 (±2) and 4 (±2), respectively; in 55.5% (5/9) of patients at least one dose of non-opioid rescue analgesics was administered at a median time lapse of 4 (range =2–20) h after completion of surgery, of whom 40% (n=2) and 20% (n=1) required a total of two and three doses, respectively (Table 3).
At outpatient clinic appointment, all patients expressed a high level of satisfaction on the anesthesiologic method, except one patient (11.1%) who judged her experience with SA to be fair, while surgeons totally approved the method, mainly surprised by the optimal anterior abdominal wall relaxation achieved during surgery, as shown in Table 3.
Discussion
As far as we are aware, this is the first study to report the use of an opioid-free hypobaric STSA approach to LC, confirming its potential role as a primary anesthesiologic method alternative to GA in laparoscopic surgical procedures.
Though applied in a small series, our initial experience shows that this regimen may have remarkable perioperative advantages, mainly in the field of right shoulder pain, that, carrying a high occurrence and representing a potential reason for conversion to GA, has been acknowledged as one of the main limits of the technique.21,22
Indeed, over the past 15 years, several series have described the utilization of SA in LC,1–9 with older reports documenting its application mainly in comorbid patients who would be at high risk of perioperative morbidity with GA1,7 and more recent reports supporting its adoption in low-risk patients (ASA 1–2) undergoing elective surgeries.2,4,5
Accordingly, prospective randomized controlled trials conducted on the latter group of patients scheduled for elective LC described several benefits of SA when compared to GA, in terms of perioperative pain management and PONV, leading to faster patient recovery, a smoother postoperative course, and possible same-day discharge,10–20 reinforcing the concept of LC as routine ambulatory surgery, with reduced overall health-care costs and waiting lists, as recent evidence encourages.31,32
Nevertheless, the negative impact of combining NA and laparoscopy on the cardiovascular and respiratory system and the high occurrence of intraoperative right shoulder pain have represented the main obstacles to an extensive utilization of SA in laparoscopic procedures.21,22
Indeed, regarding the first point, the increased intra-abdominal pressure caused by the artificial pneumoperitoneum may worsen the hypotension secondary to the extensive sympathetic block of SA, whose effects of reducing systemic vascular resistance and inducing venous dilatation of lower limbs might eventually lead to a significant reduction in cardiac output.21,22
Moreover, the Trendelenburg (head-down) position, generally necessary to obtain an optimal surgical anesthesia, facilitating the cranial diffusion of local hyperbaric anesthetics, may have further negative repercussions on the cardiac output, on the ventilation, and on the intracranial pressure.22
Regarding the second point, the not negligible incidence of severe right shoulder pain during LC requiring intravenous administration of opioids, ranging between 10 and 55% of cases, with up to 10% requiring conversion to GA,11,21 has led to the implementation of various strategies aimed at preventing this pain from occurring or, at least, reducing its severity and minimizing the consequent risk of SA failure.21,22 Actions adopted intraoperatively, such as lowering the intra-abdominal pressure of pneumoperitoneum to 8–10 mmHg or spraying the diaphragm with 2% lidocaine solution, relied on diaphragmatic irritation by carbon dioxide as the main underlying cause of shoulder-related pain, though definitive evidence on their effectiveness is still missing.10,22
According to our previous successful experiences24 and aiming at overcoming the above-mentioned issues, we applied a different and promising method of SA in our series of LC, based on an association of hypobaric ropivacaine as intrathecal local anesthetic, ie, the “hypobaric” technique, and midazolam and ketamine as adjuvants, replacing the commonly used isobaric/hyperbaric bupivacaine and opioids, respectively.
Indeed, the demonstrated advantages of ropivacaine over bupivacaine, in delivering an enhanced sensory and motor differentiation with a similar sensory block, improved motor recovery, and minor toxicity, were the main reasons justifying our choice.33–36 A highly selective blockage of the sensory roots of C3–C4 and C5 innervating the diaphragm, while sparing the motor counterpart and thus without affecting the ventilation, might explain the main clinical effects and benefits of ropivacaine, when applied in STSA, with regard to the shoulder pain.
Moreover, the utilization of a hypobaric agent, ie, with a relative density lower than that of CSF, differently from hyperbaric anesthetics, requires an anti-Trendelenburg (head-up) position to diffuse cranially, hence avoiding the related risks of hypotension while allowing to adopt, since the induction of anesthesia, the definitive position required to perform a LC, which might, concurrently, contribute to a minor diaphragmatic irritation by carbon dioxide pneumoperitoneum.37,38
The combination of these aspects, ie, use of ropivacaine, low baricity, and patient positioning, might explain the reason why in our initial experience, even if with a limited number of cases, no patient experienced this type of pain, compared to the high rates reported in literature,11,21 and therefore a conversion to GA was never required.
Regarding the use of adjuvants in SA, since the use of intrathecal opioids might be associated with adverse effects such as respiratory depression, urinary retention, pruritus, nausea, and vomiting,39–41 we decided to extend the benefits of an opioid-free STSA, demonstrated in our previous series,23,24 to laparoscopic surgeries, emphasizing the role of midazolam and ketamine in improving the duration and quality of SA, in reducing the onset time of sensory block, in providing a mild intraoperative sedative effect, in assuring a prolonged perioperative analgesia due to delayed recovery time of sensory block and in decreasing the incidence of PONV without negative effects on perioperative hemodynamics, significant side-effects, and neurotoxicity.41–43
In particular, an adequate intrathecal sedation allows the patient to remain cooperative and able to report any discomfort or pain he might experience during the surgery, maintaining at the same time valid swallowing and cough reflexes and preserving him from consequences related to a lack of airway protection as in GA.24
Lastly, the decision to employ the STSA in the field of minimally invasive surgeries derived from our consolidated experience with this method,23,24 whose benefits, secondary to a highly selective neuraxial blockade, consist in improved control over both induction and surgical anesthesia, minor negative repercussions on the cardiovascular and respiratory systems, reduced doses of local anesthetics used and limited caudal spread with concomitant decreased sympathomimetic blockade, vasodilatation and hypotension, in comparison to LA,4 that has represented the main technique applied in nearly all the series described so far in the literature.5–7,9–13,15–18
Concurrently, the safety of thoracic puncture has been established by magnetic resonance imaging investigations on the anatomy of the thoracic spinal cord and by large clinical series reporting similar rates of paresthesia during STSA compared to LA, without any neurologic sequelae.44,45
Similarly, severe direct complications of the technique (eg, spinal hematomas or PDPH) were not recorded in our cases as well as in our previous works on STSA,23,24 validating its security.
Moreover, our results indicate that, with this method, in addition to not reporting any occurrence of shoulder pain and any need for conversion to GA, satisfying intraoperative hemodynamics were generally maintained and, if needed, assured by the administration of low doses of vasopressor amines; besides an optimal perioperative analgesia was observed in all cases as stated by all parameters used to evaluate this outcome after surgery: incidence of pain, VAS score, and administration of intravenous non-opioid analgesics.
Conversely, since our institute is specifically focused on geriatric care and hence explained our remarkable background in applying this anesthesiologic approach to the comorbid elderly,23,24 it has been difficult to extend the concept of ambulatory LC to our series, having a median length of in-hospital stay of 2 days, in relation to the mean age, CCI, and ASA scores recorded, the last one approaching the number 3.
Another potential advantage of NA is currently related to its potential use in surgeries involving confirmed or only suspected COVID-19 patients by limiting airway manipulation, reducing exposure to patient respiratory droplets, and reducing the risk of virus spread in operating rooms.46,47 Accordingly, all major scientific societies have recommended RA, whenever possible, in COVID-19-infected patients.47
Future approaches may imply the association of NA techniques with fascial plane blocks such as the paravertebral and the erector spinae plane block. Fusion anesthesia, as it was named by the developing authors Starnari and Pullano, is based on the innovative concept of blocking the same afferent pathway in different parts, granting a major exposure to local anesthetic, with the main plus-points of reduced neuraxial loading doses, shorter onset time, longer duration of single-shot SA, minor hemodynamic impact, decreased motor block and lower incidence of patchy or missing segment blocks.48
There are several limitations to this study. First, the limited number of patients in this case series might bias the outcomes analyzed. In addition, although the data were prospectively collected, the analysis was retrospective in nature and lacks a control group undergoing GA to compare our findings, suggesting the need for prospective studies with a larger number of patients undergoing laparoscopic surgeries to validate and confirm these findings.
Conclusions
Our small series confirms STSA as a safe, reliable, and adequate anesthesiologic method in elective LC, representing a reasonable alternative to GA.
Use of hypobaric ropivacaine and non-opioid adjuvants might present important additional advantages over the classical scheme described in the literature, mainly in the intraoperative management of shoulder pain.
Abbreviations
ASA, American Society of Anesthesiologists; BMI, body mass index; CCI, Charlson comorbidity index; COVID-19, coronavirus disease 2019; GA, general anesthesia; INRCA, Italian National Research Center on Aging; LA, lumbar anesthesia; LC, laparoscopic cholecystectomy; NA, neuraxial anesthesia; NSAIDs, non-steroidal anti-inflammatory drugs; PACU, post-anesthesia care unit; PDPH, post-dural puncture headache; PONV, postoperative nausea and vomiting; RA, regional anesthesia; SA, spinal anesthesia; STSA, segmental thoracic spinal anesthesia; VAS, visual analogue scale.
Author Contributions
All authors made a significant contribution to the work reported, whether that is in the conception, study design, execution, acquisition of data, analysis and interpretation, or in all these areas; took part in drafting, revising, or critically reviewing the article; gave final approval of the version to be published; have agreed on the journal to which the article has been submitted; and agree to be accountable for all aspects of the work.
Funding
This research did not receive any specific grants from funding agencies in the public, commercial, or not-for-profit sectors.
Disclosure
The authors report no conflicts of interest in this work.
References
1. van Zundert AAJ, Stultiens G, Jakimowicz JJ, van den Borne BEEM, van der Ham WGJM, Wildsmith JAW. Segmental spinal anaesthesia for cholecystectomy in a patient with severe lung disease. Br J Anaesth. 2006;96(4):464–466. doi:10.1093/bja/ael036
2. Kejriwal A, Begum S, Krishan G, Agrawal R. Laparoscopic cholecystectomy under segmental thoracic spinal anesthesia: a feasible economical alternative. Anesth Essays Res. 2017;11(3):781. doi:10.4103/0259-1162.174467
3. Stultiens G, Wildsmith JAW, Korsten HHM, et al. Laparoscopic cholecystectomy under segmental thoracic spinal anaesthesia: a feasibility study. Br J Anaesth. 2007;98(5):682–686. doi:10.1093/bja/aem058
4. Imbelloni L. Spinal anesthesia for laparoscopic cholecystectomy: thoracic vs. Lumbar Technique. Saudi J Anaesth. 2014;8(4):477–483. doi:10.4103/1658-354X.140853
5. Imbelloni LE, Sant’Anna R, Fornasari M, Fialho JC. Laparoscopic cholecystectomy under spinal anesthesia: comparative study between conventional-dose and low-dose hyperbaric bupivacaine. Local Reg Anesth. 2011;4(1):41–46. doi:10.2147/lra.s19979
6. Sinha R, Gurwara AK, Gupta SC. Laparoscopic cholecystectomy under spinal anesthesia: a study of 3492 patients. J Laparoendosc Adv Surg Tech. 2009;19(3):323–327. doi:10.1089/lap.2008.0393
7. Yi JW, Choi SE, Chung JY. Laparoscopic cholecystectomy performed under regional anesthesia in patient who had undergone pneumonectomy - A case report. Korean J Anesth. 2009;56(3):330. doi:10.4097/kjae.2009.56.3.330
8. Pedullà G, Santoro E, Colace L, Pullano C. Spinal and epidural anesthesia for laparoscopic abdominal surgery: 84 procedures. World J Surg Surg Res. 2021;4:1–6.
9. Bayrak M, Altintas Y. Comparing laparoscopic cholecystectomy in patients with chronic obstructive pulmonary disease under spinal anesthesia and general anesthesia. BMC Surg. 2018;18:1. doi:10.1186/s12893-018-0396-1
10. Imbelloni LE, Fornasari M, Fialho JC, Sant’Anna R, Cordeiro JA. General anesthesia versus spinal anesthesia for laparoscopic cholecystectomy. Rev Bras Anestesiol. 2010;60(3):217–227. doi:10.1016/S0034-7094(10)70030-1
11. Kalaivani V, Pujari VS, Sreevathsa MR, Hiremath BV, Bevinaguddaiah Y. Laparoscopic cholecystectomy under spinal anaesthesia vs. general anaesthesia: a prospective randomised study. J Clin Diagnostic Res. 2014;8(8). doi:10.7860/JCDR/2014/9829.4700
12. Tzovaras G, Fafoulakis F, Pratsas K, Georgopoulou S, Stamatiou G, Hatzitheofilou C. Spinal vs general anesthesia for laparoscopic cholecystectomy interim analysis of a controlled randomized trial. Arch Surg. 2008;143(5):497–501. doi:10.10001/archsurg.143.5.497
13. Tiwari S, Chauhan A, Chaterjee P, Alam MT. Laparoscopic cholecystectomy under spinal anaesthesia: a prospective, randomised study. J Minim Access Surg. 2013;9(2):65–71. doi:10.4103/0972-9941.110965
14. Ellakany M. Comparative study between general and thoracic spinal anesthesia for laparoscopic cholecystectomy. Egypt J Anaesth. 2013;29(4):375–381. doi:10.1016/j.egja.2013.05.004
15. Bessa SS, Katri KM, Abdel-Salam WN, El-Kayal ESA, Tawfik TA. Spinal versus general anesthesia for day-case laparoscopic cholecystectomy: a prospective randomized study. J Laparoendosc Adv Surg Tech. 2012;22(6):550–555. doi:10.1089/lap.2012.0110
16. Bessa SS, El-Sayes IA, El-Saiedi MK, Abdel-Baki NA, Abdel-Maksoud MM. Laparoscopic cholecystectomy under spinal versus general anesthesia: a prospective, randomized study. J Laparoendosc Adv Surg Tech. 2010;20(6):515–520. doi:10.1089/lap.2010.0041
17. Donmez T, Erdem VM, Uzman S, et al. Laparoscopic cholecystectomy under spinal-epidural anesthesia vs. general anaesthesia: a prospective randomised study. Ann Surg Treat Res. 2017;92(3):136–142. doi:10.4174/astr.2017.92.3.136
18. Kisa A, Koruk S, Kocoglu H, Leblebici İM. Comparison of general anesthesia with spinal anesthesia in laparoscopic cholecystectomy operations. Medeni med J. 2019;34(4):346–353. doi:10.5222/MMJ.2019.37929
19. Wang XX, Zhou Q, Pan DB, et al. Comparison of postoperative events between spinal anesthesia and general anesthesia in laparoscopic cholecystectomy: a systemic review and meta-analysis of randomized controlled trials. BioMed Res Int. 2016;2016. doi:10.1155/2016/9480539
20. Yu G, Wen Q, Qiu L, Bo L, Yu J. Laparoscopic cholecystectomy under spinal anaesthesia vs. general anaesthesia: a meta-analysis of randomized controlled trials. BMC Anesth. 2015;15(1). doi:10.1186/s12871-015-0158-x
21. Longo MA, Cavalheiro BT, de Oliveira Filho GR. Laparoscopic cholecystectomy under neuraxial anesthesia compared with general anesthesia: systematic review and meta-analyses. J Clin Anesth. 2017;41:48–54. doi:10.1016/j.jclinane.2017.06.005
22. Bajwa SJS, Kulshrestha A. Anaesthesia for laparoscopic surgery: general vs regional anaesthesia. J Minim Access Surg. 2016;12(1):4–9. doi:10.4103/0972-9941.169952
23. Vincenzi P, Starnari R, Faloia L, et al. Continuous thoracic spinal anesthesia with local anesthetic plus midazolam and ketamine is superior to local anesthetic plus fentanyl in major abdominal surgery. Surg Open Sci. 2020;2(4):5–11. doi:10.1016/j.sopen.2020.07.002
24. Vincenzi P, Stronati M, Isidori P, et al. Opioid-free segmental thoracic spinal anesthesia with intrathecal sedation for breast and axillary surgery: report of four cases. Local Reg Anesth. 2022;15:23–29. doi:10.2147/LRA.S358157.
25. Guarracino F, Bertini P. Perioperative hypotension: causes and remedies. J Anaesth Analog Crit Care. 2022;2:1. doi:10.1186/s44158-022-00045-8
26. Charlson ME, Pompei P, Ales KL, MacKenzie R. Charlson comorbidity index. J Chronic Dis. 1987;40(5):373–383. doi:10.1016/0021-9681(87)90171-8
27. Doyle DJ, Garmon EH. American Society of Anesthesiologists Classification (ASA Class). Stat Pearls Publishing; 2018. doi:10.1097/00132582-198203000-00028
28. Sheahan CG, Mathews DM. Monitoring and delivery of sedation. Br J Anaesth. 2014;113:ii37–ii47. doi:10.1093/bja/aeu378
29. Bromage PR. Epidural Analgesia. Philadelphia: Ed Saunders; 1978.
30. Apfelbaum J, Horlocker T, Agarkar M, Connis R, Hebl J, Nickinovich D. Practice guidelines for the prevention, detection, and management of respiratory depression associated with neuraxial opioid. Anesthesiology. 2016;124(3):535–552. doi:10.1097/ALN.0000000000000975
31. Gurusamy K, Junnarkar S, Farouk M, Davidson BR. Meta-analysis of randomized controlled trials on the safety and effectiveness of day-case laparoscopic cholecystectomy. Br J Surg. 2008;95(2):161–168. doi:10.1002/bjs.6105
32. Manzia TM, Quaranta C, Filingeri V, et al. Feasibility and cost effectiveness of ambulatory laparoscopic cholecystectomy. A retrospective cohort study. Ann Med Surg. 2020;55:56–61. doi:10.1016/j.amsu.2020.04.036
33. Mcclellan KJ, Faulds D, Binning AR, Casati A, Scott DA. Ropivacaine an update of its use in regional anaesthesia. Drugs. 2000;60(5):1065–1093. doi:10.2165/00003495-200060050-00007
34. Malhotra R, Johnstone C, Halpern S, Hunter J, Banerjee A. Duration of motor block with intrathecal ropivacaine versus bupivacaine for caesarean section: a meta-analysis. Int J Obstet Anesth. 2016;27:9–16. doi:10.1016/j.ijoa.2016.03.004
35. Hansen T. Ropivacaine: a pharmacological review. Expert Rev Neurother. 2004;4(5):781–791. doi:10.1586/14737175.4.5.781
36. Yadav N, Chaudhary S, Gahlot D, Salhotra R. Comparison of intrathecal hyperbaric bupivacaine, isobaric levobupivacaine and isobaric ropivacaine with fentanyl as adjuvant in knee arthroscopy: a randomised controlled study. Indian J Clinic Anaesth. 2020;7(4):594–599. doi:10.18231/j.ijca.2020.108
37. Aydemir Ö, Aslan FE, Karabacak Ü, Akdaş Ö. The effect of exaggerated lithotomy position on shoulder pain after laparoscopic cholecystectomy. Pain Manag Nurs. 2018;19(6):663–670. doi:10.1016/j.pmn.2018.04.012
38. Zeeni C, Chamsy D, Khalil A, et al. Effect of postoperative Trendelenburg position on shoulder pain after gynecological laparoscopic procedures: a randomized clinical trial. BMC Anesthesiol. 2020;20(1):27. doi:10.1186/s12871-020-0946-9
39. Sultan P, Gutierrez MC, Carvalho B. Neuraxial morphine and respiratory depression: finding the right balance. Drugs. 2011;71(14):1807–1819. doi:10.2165/11596250-000000000-00000
40. Raffaeli W, Marconi G, Fanelli G, Taddei S, Borghi GB, Casati A. Opioid-related side-effects after intrathecal morphine: a prospective, randomized, double-blind dose-response study. Eur J Anaesthesiol. 2006;23(7):605–610. doi:10.1017/S026502150600038X
41. Yegin A, Sanli S, Dosemeci L, Kayacan N, Akbas M, Karsli B. The analgesic and sedative effects of intrathecal midazolam in perianal surgery. Eur J Anaesthesiol. 2004;21(8):658–662. doi:10.1017/S0265021504008129
42. Abd El-Rahman AM, Mohamed AA, Mohamed SA, Mostafa MAM. Effect of intrathecally administered ketamine, morphine, and their combination added to bupivacaine in patients undergoing major abdominal cancer surgery a randomized, double-blind study. Pain Med. 2018;19(3):561–568. doi:10.1093/pm/pnx105
43. Shama AA, Ng KT, Shahen MM, Abosamak MF. Effect of adding midazolam to intrathecal bupivacaine in children undergoing lower abdominal surgeries: a randomised controlled trial. Indian J Anaesth. 2022;66(3):200–206. doi:10.4103/ija.ija_466_21
44. Imbelloni LE, Quirici MB, Ferraz Filho JR, Cordeiro JA, Ganem EM. The anatomy of the thoracic spinal canal investigated with magnetic resonance imaging. Anesth Analg. 2010;110(5):1494–1495. doi:10.1213/ANE.0b013e3181d5aca6
45. Imbelloni LE, Pitombo PF, Ganem EM. The incidence of paresthesia and neurologic complications after lower spinal thoracic puncture with cut needle compared to pencil point needle. Study in 300 patients. J Anesth Clin Res. 2010;1(02). doi:10.4172/2155-6148.1000106
46. Uppal V, Sondekoppam RV, Landau R, El-Boghdadly K, Narouze S, Kalagara HKP. Neuraxial anaesthesia and peripheral nerve blocks during the COVID-19 pandemic: a literature review and practice recommendations. Anaesthesia. 2020;75(10):1350–1363. doi:10.1111/anae.15105
47. Cappelleri G, Fanelli A, Ghisi D, et al. The role of regional anesthesia during the SARS-CoV2 pandemic: appraisal of clinical, pharmacological and organizational aspects. Front Pharmacol. 2021;12. doi:10.3389/fphar.2021.574091
48. Starnari R, Pullano C. Fascial plane blocks and neuraxial blocks: two planets not so far apart. In: Edra A, editor. Ultrasound Guided Nerve Blocks of the Trunk and Abdominal Wall. Vol. 1. Edra Publishing; 2022:205–213.
 © 2023 The Author(s). This work is published and licensed by Dove Medical Press Limited. The
full terms of this license are available at https://www.dovepress.com/terms
and incorporate the Creative Commons Attribution
- Non Commercial (unported, 3.0) License.
By accessing the work you hereby accept the Terms. Non-commercial uses of the work are permitted
without any further permission from Dove Medical Press Limited, provided the work is properly
attributed. For permission for commercial use of this work, please see paragraphs 4.2 and 5 of our Terms.
© 2023 The Author(s). This work is published and licensed by Dove Medical Press Limited. The
full terms of this license are available at https://www.dovepress.com/terms
and incorporate the Creative Commons Attribution
- Non Commercial (unported, 3.0) License.
By accessing the work you hereby accept the Terms. Non-commercial uses of the work are permitted
without any further permission from Dove Medical Press Limited, provided the work is properly
attributed. For permission for commercial use of this work, please see paragraphs 4.2 and 5 of our Terms.