Back to Journals » Clinical, Cosmetic and Investigational Dermatology » Volume 19
Secukinumab-Induced Delayed Behçet-Like Reaction in a Patient with Plaque Psoriasis: A Case Report
Authors Wei Y, Zhang P, Chuan J ![]() , Ye J, Liu T
, Ye J, Liu T
Received 16 September 2025
Accepted for publication 18 December 2025
Published 8 January 2026 Volume 2026:19 567115
DOI https://doi.org/10.2147/CCID.S567115
Checked for plagiarism Yes
Review by Single anonymous peer review
Peer reviewer comments 2
Editor who approved publication: Prof. Dr. Rungsima Wanitphakdeedecha
Yanjie Wei,1,* Peilian Zhang,2,* Jintao Chuan,1 Jianzhou Ye,2 Tao Liu3
1Department of Dermatology, The First Affiliated Hospital of Yunnan University of Traditional Chinese Medicine, Kunming, People’s Republic of China; 2Department of Dermatology, Yunnan Provincial Hospital of Traditional Chinese Medicine, Kunming, Yunnan, People’s Republic of China; 3Department of Pathology, Yunnan Provincial Hospital of Traditional Chinese Medicine, Kunming, Yunnan, People’s Republic of China
*These authors contributed equally to this work
Correspondence: Peilian Zhang, Department of Dermatology, Yunnan Provincial Hospital of Traditional Chinese Medicine, Kunming, People’s Republic of China, Email [email protected]
Purpose: This report presents a rare paradoxical reaction manifesting as Behçet’s-like features, which developed three months following the initiation of secukinumab therapy for psoriasis.
Patients and Methods: A 38-year-old female with a 30-year history of plaque psoriasis achieved significant remission of psoriatic lesions following seven doses of secukinumab (cumulative dose: 2100 mg). However, she subsequently developed systemic adverse events, including pharyngodynia, painful tonsillar and genital ulcers, folliculitis-like papules on the trunk and extremities, and erythema nodosum-like lesions on the extensor surfaces of both lower limbs. Laboratory tests, including bacterial, viral, and fungal cultures, excluded infectious etiologies. Histopathological examination of a skin biopsy demonstrated superficial and deep perivascular and interstitial inflammation with dense infiltration of lymphocytes, neutrophils, and eosinophils. Consequently, a diagnosis of secukinumab-induced Behçet’s-like syndrome was established, as the patient did not fully meet the International Criteria for Behçet’s Disease (ICBD). Secukinumab was immediately discontinued, and the patient was initiated on thalidomide (50 mg, three times daily) and colchicine (0.5 mg, twice daily).
Results: Two weeks after treatment initiation, oral and genital ulcers resolved. Folliculitis-like papules and erythema nodosum-like lesions regressed significantly, leaving only residual post-inflammatory hyperpigmentation. The patient was subsequently switched to ustekinumab maintenance therapy at a standard dosage. Psoriasis remained well-controlled, with no recurrence of Behçet’s-like manifestations during a 4-year follow-up period.
Conclusion: This report underscores the critical need for vigilant patient monitoring during anti-IL-17 therapy to detect such uncommon yet clinically significant paradoxical reactions. Furthermore, precise characterization of the onset timing of such adverse events is crucial, as it enables clinicians to implement timely preventive measures, mitigate risks, and rapidly identify emerging adverse reactions.
Keywords: secukinumab, psoriasis, Behçet’s disease, adverse reaction, paradoxical reaction
Introduction
Psoriasis and Behçet’s disease (BD) are chronic immune-mediated inflammatory disorders with distinct clinical phenotypes but shared pathogenic mechanisms. Clinically, psoriasis presents with localized or generalized erythematous squamous plaques, whereas BD is characterized by recurrent oral and genital ulcers. Both conditions involve the aberrant activation of the T helper (Th) 17/Interleukin-17 (IL-17) pathway.1 Secukinumab, the first IL-17A inhibitor approved by the US Food and Drug Administration (FDA) for moderate-to-severe plaque psoriasis, is widely used as a first-line therapeutic option internationally.2 Furthermore, previous studies have reported that secukinumab can improve mucocutaneous and neurological manifestations in patients with refractory BD.1 Behçet’s-like paradoxical reactions during secukinumab therapy are rare. Paradoxical reactions are defined as the onset of a new disease or the exacerbation of a pre-existing condition during biologic therapy, despite the agent being therapeutically indicated for that specific condition.3 Such immune-mediated adverse events may represent a novel type of paradoxical reaction associated with IL-17 blockade. Herein, we report a case of a patient with long-standing plaque psoriasis, without any personal or family history of BD, who developed a late-onset Behçet’s-like reaction following the seventh dose of secukinumab (approximately three months after treatment initiation).
Case Description
A 38-year-old female presented to the dermatology outpatient clinic with a history of recurrent plaque psoriasis for over 30 years. Physical examination revealed widespread scaly papules and plaques on the scalp, trunk, and extremities, along with thimble-like pitting of the fingernails. No articular tenderness was noted. The Auspitz sign was positive. The affected Body Surface Area (BSA) was approximately 62%. Family history was unremarkable, and she denied any known allergies to drugs or food. Upon diagnosis of moderate-to-severe plaque psoriasis and exclusion of contraindications, secukinumab therapy was initiated at a dose of 300 mg weekly for five weeks, followed by 300 mg every four weeks (Q4W). Following the seventh dose of secukinumab (approximately three months after treatment initiation), psoriatic lesions resolved rapidly; however, she developed pharyngodynia and a millet-sized tonsillar ulcer, which she initially disregarded. After the eighth injection, pharyngodynia worsened, and multiple folliculitis-like papules with erythematous bases and central pustules appeared on the trunk and extremities (Figure 1a and b). Following the ninth injection, the patient experienced epigastric pain, which resolved after two weeks of treatment with omeprazole and aluminum-magnesium suspension (specific dosage unknown). No gastrointestinal endoscopy was performed. The patient did not exhibit arthralgia or uveitis. Subsequently, scattered erythematous papules and nodules appeared on the extensor surfaces of both lower limbs, accompanied by two painful ulcers on the external genitalia, measuring approximately the size of a rice grain to a broad bean (Figure 1c and d). The pathergy test was positive. Figure 2 summarizes the patient’s clinical timeline during secukinumab therapy. Laboratory investigations demonstrated normal blood counts, liver and kidney function, erythrocyte sedimentation rate (ESR), and C-reactive protein (CRP). Autoimmune screening, including antinuclear antibodies (ANA), anti-DNA antibodies, anti-Sm, anti-SSA, and complement levels, was within normal limits. Viral serology, including anti-HCV, anti-HIV, and HBsAg, was negative. Repeated bacterial, viral, and fungal cultures of the lesions and blood were negative, indicating no signs of infection. Histopathological examination of a lesion on the right leg revealed epidermal acanthosis, as well as superficial and deep perivascular and interstitial inflammatory infiltrates composed of dense lymphocytes, neutrophils, and eosinophils (Figure 3a and b). Although the patient did not fully meet the International Criteria for Behçet’s Disease (ICBD) for a definitive diagnosis, her cutaneous manifestations were consistent with the disease spectrum; thus, a diagnosis of Behçet’s-like syndrome was established. As secukinumab was the only recently introduced medication preceding the adverse events, the reaction was attributed to its administration.
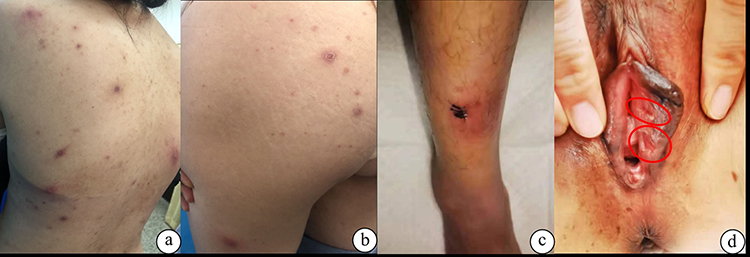 |
Figure 1 (a and b) Clinical images showing a cutaneous delayed-type hypersensitivity (Type IV) reaction to secukinumab. Multiple folliculitis-like papules with erythematous bases and central pustules appeared on the trunk and extremities. (c and d) Scattered erythematous papules and nodules appeared on the extensor surfaces of right lower limbs, accompanied by two painful ulcers on the external genitalia, measuring approximately the size of a rice grain to a broad bean. |
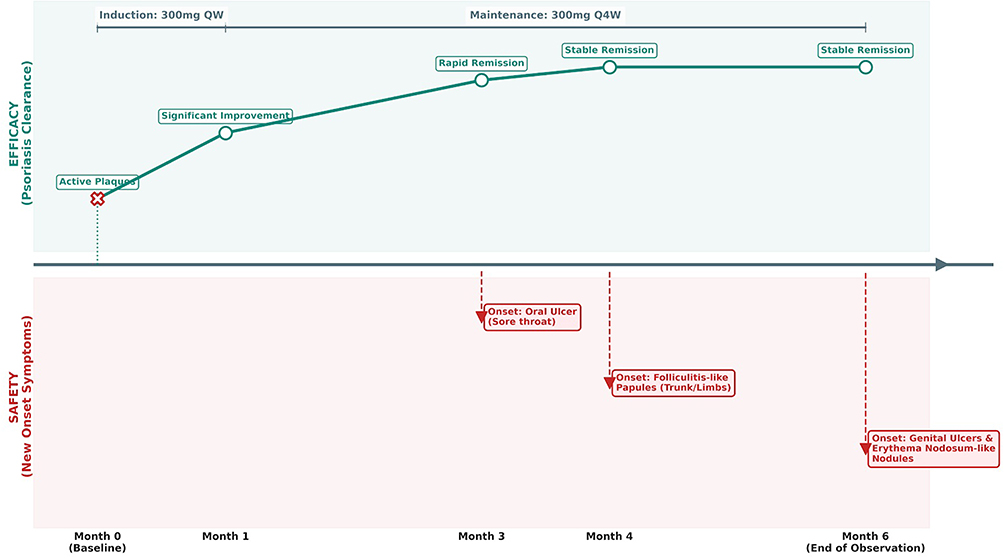 |
Figure 2 Clinical Timeline of Psoriasis Resolution and Behçet-Like Reaction during Secukinumab Therapy. The central axis indicates months following secukinumab initiation. The upper panel (green) illustrates the rapid resolution of plaque psoriasis, progressing from baseline plaques to stable remission. The lower panel (red) details the delayed onset and sequential emergence of the secukinumab-induced Behçet-like reaction, beginning at Month 3. Top bars denote the dosage regimen. Abbreviation: QW, once weekly; Q4W, every 4 weeks. |
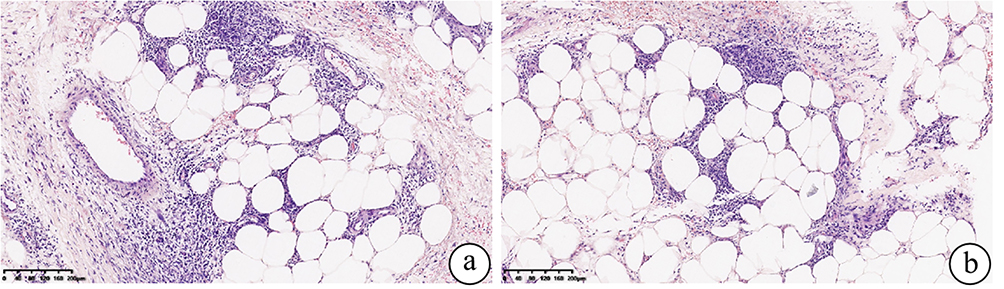 |
Figure 3 (a and b) Histopathological examination of a lesion on the right leg revealed epidermal acanthosis, as well as superficial and deep perivascular and interstitial inflammatory infiltrates composed of dense lymphocytes, neutrophils, and eosinophils. |
Results
Secukinumab was immediately discontinued. In accordance with the 2021 Guidelines for the Diagnosis and Treatment of Behçet’s Syndrome issued by the Chinese Medical Association,4 which recommend targeted interventions for the prevention of mucocutaneous recurrence and for cases characterized primarily by oral/genital ulcers and pseudofolliculitis, the patient was treated with thalidomide (50 mg, three times daily) and colchicine (0.5 mg, twice daily). Two weeks after treatment initiation, oral and genital ulcers resolved. Folliculitis-like papules on the trunk and extremities, as well as the erythema nodosum-like lesions, showed significant improvement, leaving only residual post-inflammatory hyperpigmentation. Studies have indicated that IL-12/23 and IL-23 inhibitors are associated with a lower incidence of paradoxical reactions compared to IL-17 inhibitors.5 Consequently, upon psoriasis recurrence, the patient was switched to the IL-12/23 inhibitor ustekinumab at a standard maintenance dosage. Psoriasis was well-controlled, and no recurrence of Behçet’s-like cutaneous manifestations was observed during a 4-year follow-up period.
Discussion
Sacchelli et al6 previously reported a case of a patient with moderate plaque psoriasis who developed recurrent bacterial folliculitis two months following secukinumab therapy. In contrast, in the present case, the patient presented with concurrent oral and genital ulcers, and bacterial cultures were negative, supporting a diagnosis of Behçet’s-like syndrome as the primary consideration. According to current literature,1 increasing numbers of reports in the literature describe Behçet’s-like paradoxical reactions following treatment with IL-17A inhibitors. IL-17A is a critical mediator of these paradoxical reactions, contributing not only to pathogenic inflammation but also to the immunopathogenesis of Behçet’s disease. Notably, IL-17 levels are significantly elevated in patients with Behçet’s disease compared to healthy controls, particularly during active disease stages.3 The pathogenesis underlying these paradoxical reactions is complex and has not yet been fully elucidated. Recent studies suggest that cytokine imbalance induced by IL-17 blockade may precipitate paradoxical Behçet’s-like symptoms.1 As a key cytokine produced by Th17 cells, IL-17 drives neutrophil activation and migration. Upon its blockade by secukinumab, compensatory upregulation of other IL-17 isoforms, along with related pathogenic cytokines such as IL-22 and IL-23, may occur. This shift may trigger neutrophil activation and the onset of paradoxical reactions, while simultaneously impairing the mucosal barrier, thereby contributing to these adverse events.7 Furthermore, IL-17 inhibitor therapy can significantly alter the gut microbiota composition in psoriasis patients. Dysbiosis of the gut or oral microbiota may disrupt the balance between regulatory T cells (Tregs) and Th1/Th17 cells through metabolic processes, thereby inducing Behçet’s disease immunopathology.8
Despite the immunopathogenic similarities and the known comorbidity between Behçet’s disease and psoriasis, controversy persists as to whether secukinumab’s role in such cases represents a true paradoxical reaction or merely a precipitating factor.8 However, the constellation of typical clinical manifestations, the timing of the rash onset, histopathological findings, and lesion resolution following the withdrawal of the offending agent suggests that the patient experienced a Type IV delayed-type hypersensitivity reaction, rather than a concurrent manifestation of psoriasis. Most drug-induced adverse reactions typically occur within 4–28 days of initiation, making our case’s timeline noteworthy: the patient developed a late-onset Behçet’s-like paradoxical reaction at three months (after the seventh dose) of secukinumab therapy. This latency is consistent with prior literature reporting an average onset of 3.4 months for Behçet’s disease following IL-17A inhibitor therapy,1 and cases of secukinumab-induced delayed cutaneous hypersensitivity (Type IV reaction) have previously been documented.9 Biologics, including monoclonal antibodies such as secukinumab, inherently carry immunogenic potential, which may induce anti-drug antibodies (ADAs) that contribute to adverse events ranging from reduced therapeutic efficacy to drug hypersensitivity reactions. The latency of such paradoxical reactions is likely multifactorial, involving not only the immunogenicity of the biologic but also factors such as drug-specific properties (eg, half-life, accumulation kinetics) and individual host factors (eg, genetic polymorphisms, baseline immune status). Although the incidence of clinical immunogenicity associated with secukinumab is lower than that reported for other biologics,10 clinicians must remain cognizant of the potential for delayed reactions. The complexity of adverse events associated with secukinumab indicates that severe cutaneous reactions may still occur, highlighting the need for high vigilance to enable early detection, prompt discontinuation, and appropriate intervention to mitigate adverse outcomes.
Conclusion
In this case, a patient with moderate-to-severe plaque psoriasis developed a Behçet’s-like paradoxical reaction induced by secukinumab, manifesting as a Type IV delayed-type hypersensitivity reaction. These findings underscore the importance of vigilant patient monitoring during clinical management to identify potentially rare or previously unreported paradoxical reactions. Furthermore, precisely defining the onset timing is crucial for the timely implementation of preventive and mitigative strategies, as well as for the prompt recognition of adverse events.
Ethics Statement
Written informed consent has been obtained from the patient for the publication of the case details and related images. Publication of details of the case does not require the agency’s approval.
Consent Statement
The patient had given written informed consent for the publication of her clinical details.
Funding
This work was supported by the Xingdian Talents Support Program (Grant No. XDYC-YLWS-2023-0093), the Yunnan Provincial Clinical Medical Center of Traditional Chinese Medicine (Dermatology) (Grant No. Yun Cai She [2024] 12), and the Sixth Batch of Master-Apprentice Projects for Traditional Chinese Medicine of Yunnan Province (Grant No. Yun Wei Zhong Yi Fa Zhan Fa [2025] 1).
Disclosure
The authors report no conflicts of interest in this work.
References
1. Ren YK, Ren L, Sun W, et al. Paradoxical Behçet’s disease after ixekizumab: a case report and literature review. Indian J Dermatol. 2025;70(1):42–5. doi:10.4103/ijd.ijd_719_24
2. Frieder J, Kivelevitch D, Menter A. Secukinumab: a review of the anti-IL-17A biologic for the treatment of psoriasis. Ther Adv Chronic Dis. 2018;9(1):5–21. doi:10.1177/2040622317738910
3. Algarra AC, Miguel RA, Lencina JJA, et al. Behçet’s-like disease during secukinumab treatment: new paradoxical reaction. J Dtsch Dermatol Ges. 2021;19(1):116–118. doi:10.1111/ddg.14196
4. Zheng W, Zhang N, Zhu X, et al. Diagnosis and treatment guidelines for Behçet’s syndrome. Zhonghua Nei Ke Za Zhi. 2021;60(10):860–867. doi:10.3760/cma.j.cn112138-20210604-00398
5. Murphy MJ, Cohen JM, Vesely MD, et al. Paradoxical eruptions to targeted therapies in dermatology: a systematic review and analysis. J Am Acad Dermatol. 2022;86(5):1080–1091. doi:10.1016/j.jaad.2020.12.010
6. Sacchelli L, Ferrara F, Tartari F, et al. Recalcitrant and recurrent bacterial folliculitis during anti-IL 17 therapy in a psoriatic patient. G Ital Dermatol Venereol. 2020;155(2). doi:10.23736/S0392-0488.18.05993-X
7. Avcı C, Akın G, Akarsu S, et al. Pyoderma gangrenosum and Behcet’s-like disease induced by secukinumab: a paradoxical drug reaction. J Dermatol Treat. 2023;34(1):2235040. doi:10.1080/09546634.2023.2235040
8. Liu K, Sun J. Behcet’s-like disease induced by secukinumab in a patient with psoriasis: a case report and literature review. J Dermatol Treat. 2024;35(1):2347440. doi:10.1080/09546634.2024.2347440
9. Konda S, Shetty N, Friedman B, et al. Delayed drug hypersensitivity reaction to secukinumab in a patient with hidradenitis suppurativa. Drug Ther Bull. 2024;62(5):77–79. doi:10.1136/dtb.2023.249684rep
10. Wong SCT, Chung HY. Secukinumab-induced delayed-type drug hypersensitivity reactions. J Clin Rheumatol. 2020;26(6):e197–e198. doi:10.1097/RHU.0000000000001065
 © 2026 The Author(s). This work is published and licensed by Dove Medical Press Limited. The
full terms of this license are available at https://www.dovepress.com/terms
and incorporate the Creative Commons Attribution
- Non Commercial (unported, 4.0) License.
By accessing the work you hereby accept the Terms. Non-commercial uses of the work are permitted
without any further permission from Dove Medical Press Limited, provided the work is properly
attributed. For permission for commercial use of this work, please see paragraphs 4.2 and 5 of our Terms.
© 2026 The Author(s). This work is published and licensed by Dove Medical Press Limited. The
full terms of this license are available at https://www.dovepress.com/terms
and incorporate the Creative Commons Attribution
- Non Commercial (unported, 4.0) License.
By accessing the work you hereby accept the Terms. Non-commercial uses of the work are permitted
without any further permission from Dove Medical Press Limited, provided the work is properly
attributed. For permission for commercial use of this work, please see paragraphs 4.2 and 5 of our Terms.