Back to Journals » Clinical, Cosmetic and Investigational Dermatology » Volume 15
Secondary Intention Healing of Nasal Ala and Tip Defects: A Simple and Valuable Treatment Option
Authors Wen G, Mao D, Zhu M ![]() , Hu J
, Hu J ![]() , Yao X, Zhang J
, Yao X, Zhang J
Received 10 February 2022
Accepted for publication 16 September 2022
Published 10 October 2022 Volume 2022:15 Pages 2165—2168
DOI https://doi.org/10.2147/CCID.S361662
Checked for plagiarism Yes
Review by Single anonymous peer review
Peer reviewer comments 3
Editor who approved publication: Dr Jeffrey Weinberg
Guangdong Wen, Dandan Mao, Mengyi Zhu, Jian Hu, Xueyan Yao, Jianzhong Zhang
Department of Dermatology, Peking University People’s Hospital, Beijing, People’s Republic of China
Correspondence: Jianzhong Zhang, Department of Dermatology, Peking University People’s Hospital, No. 11 Xizhimen South Street, Beijing, 100044, People’s Republic of China, Tel +86-10-88325472, Email [email protected]
Purpose: To investigate the cosmetic outcomes of secondary intention healing of small (< 1.5cm) nasal ala and tip defects.
Patients and Methods: From August 2017 to October 2020, 42 patients with nasal reconstructions using secondary intention healing were included. Defects after excision ranged from 0.5cm× 0.7cm to 1.2cm× 1.5cm in size. Foam dressing covering the wounds was changed every 3 to 5 days. Wound esthetic outcomes were graded as excellent, good, acceptable, and poor based on definitions described in the literature.
Results: All 42 wounds healed in 3 to 4 weeks, with uniform color, no obvious adverse reactions and high patient satisfaction. Esthetic evaluation: 16 excellent cases (38.1%), 19 good cases (45.2%), 7 acceptable cases (16.7%) and 0 poor cases.
Conclusion: Secondary intention healing of small nasal tip and ala defects in Chinese yielded satisfactory esthetic outcomes and should be an integral part of the surgeon’s reconstructive algorithm.
Keywords: nasal tip, ala, secondary intention healing, foam dressing
Introduction
Nose is located in the middle of the face, being a key aesthetic unit as it is subdivided into nine subunits.1 Reconstruction of defects involving the nasal ala and tip presents a substantial challenge to dermatologic surgeons, due to the three-dimensional projection of the ala, the thin dermis, limited overlying tissue mobility, the alar groove, and free margin distortion.2 A variety of approaches have been described for these defects, including skin grafts, free cartilage grafts, various flaps and secondary intention healing.3–5
In this study, 42 cases of nasal ala and tip defects were healed by secondary intention healing, which is simple and cosmetically satisfactory. The purpose of this study was to evaluate the cosmetic effectiveness of secondary intention healing of nasal ala and tip defects and provide the surgeon with a simple and valuable treatment option.
Materials and Methods
A retrospective review of 42 patients with nasal ala and tip defects (sizes ranged from 0.5cm×0.7cm to 1.2cm×1.5cm) who had undergone secondary intention healing after surgical excision was performed. For defects may take several weeks to close, and good wound care is imperative, we do not perform the secondary intention healing in patients who do not have time for follow-up visits. All surgeries were performed in the Department of Dermatology, Peking University People’s Hospital between August 2017 and October 2020. Of the 42 patients, 18 were men and 24 were women. They were 10 to 83 years old, with a mean age of 56.5 years. The lesions excised included 24 pigmented nevus, 17 basal cell carcinoma and 1 trichoblastoma. Of the 42 defects, 25 were located in nasal ala and 17 in nasal tip.
After local infiltration anesthesia, excision margin was determined according to the clinical diagnosis, including 1mm for benign lesions and 3 ~ 5mm for malignant tumors. Excision depths all reached the subcutaneous fat layer. Electrocoagulation or ligation of blood vessels was not routine unless substantial hemorrhage existed. After excision, the wounds were covered with alginate dressings, with bandages on top. 3 days later, wounds were cleaned with 3% hydrogen peroxide solution, disinfected with iodophor, cleaned with normal saline, and then covered with foam dressings. Afterwards, dressings were changed every 3 to 5 days, with crusts removed and new foam dressings replaced.
After healing, wound esthetic outcomes were divided into excellent, good, acceptable and poor. The evaluation criteria referred to previous literatures.6,7 Excellent was defined as a scar with no mismatch in edge contour and a good color match or only minor hypopigmentation to surrounding skin. Good was defined as little mismatch in edge contour and good color match or only minor hypopigmentation to surrounding skin. Acceptable was defined as a depressed or elevated scar with good color match or a clear color mismatch but with good edge contour. Poor was defined as a clearly depressed or elevated scar with severe color mismatch.
Results
All 42 patients healed in about 3 to 4 weeks. The aesthetic evaluation after healing was excellent in 16 cases (38.1%), good in 19 cases (45.2%), acceptable in 7 cases (16.7%) and poor in 0 cases. Detailed information is shown in Table 1. Typical cases are shown in Figure 1 (excellent), Figure 2 (good) and Figure 3 (acceptable).
 |
Table 1 Aesthetic Outcomes in Secondary Intention Healing |
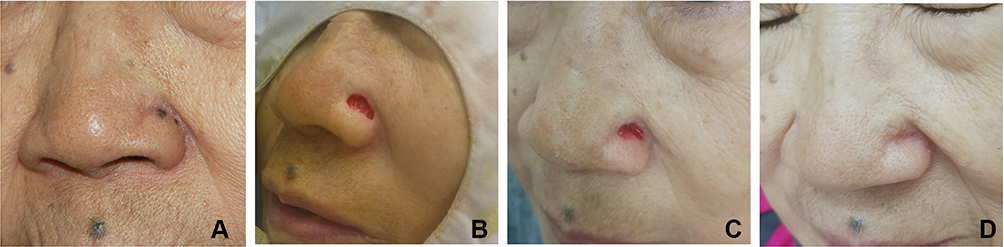 |
Figure 1 Defects involving lateral ala healed by secondary intention of a 77-year-old female trichoblastoma patient, with excellent outcome: (A) before surgery; (B) immediately after surgery; (C) 3 days after surgery and (D) 3 weeks after surgery. |
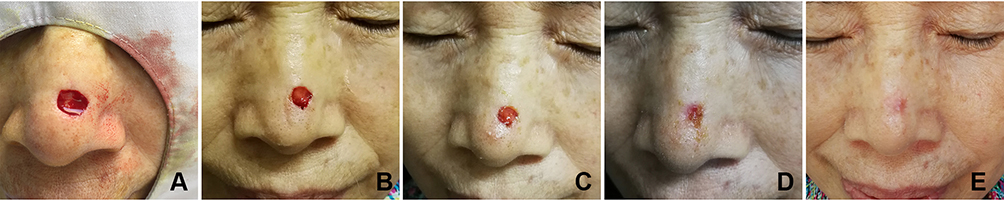 |
Figure 2 Defects involving anterior tip healed by secondary intention of a 62-year-old female basal cell carcinoma patient, with good outcome: (A) immediately after surgery; (B) 3 days after surgery; (C) 1 week after surgery and (D) 2 weeks after surgery and (E) 1 month after surgery. |
 |
Figure 3 Defects involving anterior tip healed by secondary intention of a 74-year-old male basal cell carcinoma patient, with acceptable outcome: (A) before surgery; (B) immediately after surgery; (C) 10 days after surgery and (D) 1 month after surgery. |
Discussion
A multitude of reconstructive options exist for patients with nasal defects, including primary closure, skin grafts, local, regional or free flaps, and secondary intention healing. Given the vital functions of the nose in everyday life, it is extremely important that the reconstruction of defects preserves the integrity of complex facial functions and expressions, as well as facial symmetry and a pleasing aesthetic outcome. As a result, decision-making based on aesthetic subunit and defect size before reconstruction is critical. A detailed subunit-based classification of the reconstructive armamentarium is offered by Losco et al.1 However, healing by secondary intention was not included, which is overlooked and underused today.
In our observation, secondary intention healing is an effective method to repair the defect in nasal tip and alar less than 1.5cm in diameter, with limited complications. Jin et al also showed that secondary intention healing yields satisfactory cosmetic results for the nasal ala and dorsum defects less than 1 cm in diameter in Asians.8 This approach is ideal for fragile patients unable or unwilling to have complex repairs. Besides, it allows wounds to be monitored for tumor recurrence. For the cosmetic outcome, location by subunit remains the critical determinant, followed by size and depth of the wound.9,10 For the nose, the best esthetic outcomes were seen in wounds located on the nasal ala, a concave surface, and poorer results were seen on the nasal tip, a convex surface.7 Statistical evidence has also shown that concave areas of the face are prone to heal excellently, especially if these wounds are small, superficial, and located near the medial canthus and medial cheek.6 Furthermore, on concave surfaces secondary intention healing produces cosmetic results that are superior to those produced by flaps or grafts.11 In addition, the choice of patients is also very important, as patients need to change dressings regularly for a long time and need good compliance to optimize the aesthetic effect.
In our practice, all defects were covered with alginate dressing and pressured bandage after excision. With the alginate dressing, wounds rarely bled or adhered to the dressing, making the dressing change easy. Three days later, the alginate dressing was removed and foam dressing was covered, which was changed every 3–5 days. It can provide a moist occlusive healing environment for wound and promote the healing process. The wound healed in around 3 to 4 weeks, with patients’ good satisfaction. In our patients, the esthetic effect of nasal alar and tip is both good, which may be related to the application of the foam dressing, as it is best studied as an alternative for gauze and appears to be preferable as to pain reduction, patient satisfaction and nursing time.12
The primary disadvantage of secondary intention healing is that it requires dressing change and care for an open wound for a prolonged period. In addition, it may produce a poor cosmetic outcome if used in the wrong setting.13 Therefore, before applying the secondary intention healing method, it is necessary to choose the right condition and fully communicate with the patient.
Conclusion
In conclusion, secondary intention healing of nasal defects has satisfactory aesthetic outcome. In an era of sophisticated reconstruction for large defects, secondary intention healing is often overlooked. However, when considering surgical options for reconstruction of nasal defects, secondary intention healing should still be a choice in mind.
The limitation of this paper is that the observed defects were less than 1.5cm in diameter, only reaching the subcutaneous fat layer, not the periosteum. Therefore, whether secondary intention healing is suitable for larger and deeper defects in Chinese patients still needs further research.
Ethics Approval and Informed Consent
Informed consent was obtained from participants and the patients in the images have provided informed consent for the images to be published. This study was approved by the Institutional Ethics Committee of the Peking University People’s Hospital, Beijing, China. The study was conducted in accordance with the Declaration of Helsinki.
Funding
This study was supported by the National Natural Science Foundation of China (Nos. 81402588 and 82103750).
Disclosure
The authors report no conflicts of interest in this work.
References
1. Losco L, Bolletta A, Pierazzi DM, et al. Reconstruction of the nose: management of nasal cutaneous defects according to aesthetic subunit and defect size. A review. Medicina. 2020;56(12):639. doi:10.3390/medicina56120639
2. Meirson DH. Nasal anatomy and reconstruction. Dermatol Clin. 1998;16(1):91–108. doi:10.1016/S0733-8635(05)70489-7
3. Neuhaus IM, Yu SS. Second-intention healing of nasal alar defects. Dermatol Surg. 2012;38(4):697–702. doi:10.1111/j.1524-4725.2011.02233.x
4. Salgarelli AC, Bellini P, Multinu A, et al. Reconstruction of nasal skin cancer defects with local flaps. J Skin Cancer. 2011;2011:181093. doi:10.1155/2011/181093
5. van der Eerden PA, Verdam FJ, Dennis SC, Vuyk H. Free cartilage grafts and healing by secondary intention: a viable reconstructive combination after excision of nonmelanoma skin cancer in the nasal alar region. Arch Facial Plast Surg. 2009;11(1):18–23. doi:10.1001/archfaci.2008.501
6. van der Eerden PA, Lohuis P, Hart AAM, Mulder WC, Vuyk H. Secondary intention healing after excision of nonmelanoma skin cancer of the head and neck: statistical evaluation of prognostic values of wound characteristics and final cosmetic results. Plast Reconstr Surg. 2008;122(6):1747–1755. doi:10.1097/PRS.0b013e31818a9aaa
7. Liu KY, Silvestri B, Marquez J, Huston TL. Secondary intention healing after mohs surgical excision as an alternative to surgical repair evaluation of wound characteristics and esthetic outcomes. Ann Plas Surg. 2020;85:S28–S32. doi:10.1097/SAP.0000000000002330
8. Jin W, Jin S, Li Z, Jin Z, Jin C. Second intention healing of nasal ala and dorsum defects in Asians. J Dermatolog Treat. 2021;32(4):465–468. doi:10.1080/09546634.2019.1666204
9. Donaldson MR, Coldiron BM. Scars after second intention healing. Facial Plast Surg. 2012;28(5):497–503. doi:10.1055/s-0032-1325643
10. Becker GD, Adams LA, Levin BC. Nonsurgical repair of perinasal skin defects. Plast Reconstr Surg. 1991;88(5):768–776;discussion 777–768. doi:10.1097/00006534-199111000-00003
11. Zitelli JA. Secondary intention healing: an alternative to surgical repair. Clin Dermatol. 1984;2(3):92–106. doi:10.1016/0738-081X(84)90031-2
12. Vermeulen H, Ubbink D, Goossens A, de Vos R, Legemate D, Dressings and topical agents for surgical wounds healing by secondary intention. Cochrane Database Syst Rev. 2004;2:CD003554. doi:10.1002/14651858.CD003554.pub2
13. Lam TK, Lowe C, Johnson R, Marquart JD. Secondary intention healing and purse-string closures. Dermatol Surg. 2015;41(Suppl 10):S178–186. doi:10.1097/DSS.000000000000048
 © 2022 The Author(s). This work is published and licensed by Dove Medical Press Limited. The
full terms of this license are available at https://www.dovepress.com/terms
and incorporate the Creative Commons Attribution
- Non Commercial (unported, 3.0) License.
By accessing the work you hereby accept the Terms. Non-commercial uses of the work are permitted
without any further permission from Dove Medical Press Limited, provided the work is properly
attributed. For permission for commercial use of this work, please see paragraphs 4.2 and 5 of our Terms.
© 2022 The Author(s). This work is published and licensed by Dove Medical Press Limited. The
full terms of this license are available at https://www.dovepress.com/terms
and incorporate the Creative Commons Attribution
- Non Commercial (unported, 3.0) License.
By accessing the work you hereby accept the Terms. Non-commercial uses of the work are permitted
without any further permission from Dove Medical Press Limited, provided the work is properly
attributed. For permission for commercial use of this work, please see paragraphs 4.2 and 5 of our Terms.