Back to Journals » Clinical Interventions in Aging » Volume 12
Searching for the relationship between the parameters of metabolic syndrome and the rs17782313 (T>C) polymorphism of the MC4R gene in postmenopausal women
Authors Brodowski J ![]() , Szkup M, Jurczak A, Wieder-Huszla S, Brodowska A, Laszczyńska M, Karakiewicz B, Kęcka K, Grochans E
, Szkup M, Jurczak A, Wieder-Huszla S, Brodowska A, Laszczyńska M, Karakiewicz B, Kęcka K, Grochans E ![]()
Received 10 December 2016
Accepted for publication 1 February 2017
Published 22 March 2017 Volume 2017:12 Pages 549—555
DOI https://doi.org/10.2147/CIA.S129874
Checked for plagiarism Yes
Review by Single anonymous peer review
Peer reviewer comments 2
Editor who approved publication: Dr Richard Walker
Jacek Brodowski,1 Małgorzata Szkup,2 Anna Jurczak,2 Sylwia Wieder-Huszla,2 Agnieszka Brodowska,3 Maria Laszczyńska,4 Beata Karakiewicz,5 Katarzyna Kęcka,1 Elżbieta Grochans2
1Primary Care Department, Pomeranian Medical University in Szczecin, 2Department of Nursing, Pomeranian Medical University in Szczecin, 3Clinic of Gynecology, Endocrinology, and Gynecologic Oncology, Pomeranian Medical University in Szczecin, 4Department of Histology and Developmental Biology, Pomeranian Medical University in Szczecin, 5Public Health Department, Pomeranian Medical University in Szczecin, Żołnierska, Szczecin, Poland
Abstract: Metabolic syndrome (MS) is widespread in the human population, and its incidence is continuously increasing, generating serious health problems. The purpose of this study was to find the relationship between the parameters of MS and the melanocortin type 4 receptor (MC4R) gene polymorphism in postmenopausal women. The study involved 344 healthy Polish women, who had their last menstrual cycle 1 year ago or earlier. The study included blood analysis, survey, and body measurements. The mean age was 58.5±6.6 years. An increased body mass index was observed in 65.7% and abdominal obesity in 80.3% of the study population. MS was diagnosed in 40.7% of all participants, including 39.3% of women with the T/T genotype and 44.7% of those with the C/X genotype (χ2 test; P>0.05). A logistic regression model showed that the probability of MS was higher in patients with the C/X genotype (odds ratio =1.25) (χ2 test; P>0.05). The study concluded that MS is a very common condition among postmenopausal women. The C/X genotype of the MC4R gene seems to predispose postmenopausal women to developing some MS symptoms.
Keywords: melanocortin type 4 receptor (MC4R), postmenopausal women, metabolic syndrome
Introduction
Metabolic syndrome (MS) is widespread in the human population, and its incidence is continuously increasing, generating serious health problems.1 A better understanding of genetic determinants of MS in postmenopausal women may be an interesting contribution to the knowledge of this problem, adding an important biological component to etiological environmental factors. The aim of this study was to find the relationship between the parameters of MS and the melanocortin type 4 receptor (MC4R) gene polymorphism in postmenopausal women. An attempt was made to answer the following research questions: What distinguishes a group of postmenopausal women in terms of characteristics typical of MS? What is the relationship between MC4R rs17782313 polymorphism and MS results in the group of women analyzed in this study?
Literature review
MS is a common condition, substantially contributing to the quality of life and the risk of untimely death. It is determined by the interaction between numerous environmental factors associated with lifestyle. Its etiology can be also related to the presence of MC4R polymorphism, which predisposes to this condition.
MS is a clinical condition characterized by the coexistence of risk factors for developing diabetes and cardiovascular diseases, such as carbohydrate and lipid metabolism disorders, central obesity, and raised blood pressure.2
In 2001, “The Third Report of the National Cholesterol Education Program Expert Panel on Detection, Evaluation, and Treatment of High Blood Cholesterol in Adults Treatment Panel III (NCEP-ATP III)” was published. Five elements of MS were established, namely abdominal obesity, hypertriglyceridemia, a decreased high-density lipoprotein cholesterol (HDL-C) level, hyperglycemia, and raised blood pressure, with three of these components necessary for MS to be diagnosed.3 In 2005, the International Diabetes Federation (IDF) proposed a new MS definition, based on the NCEP-ATP III criteria, but emphasizing that abdominal obesity classified by waist circumference is required for an MS diagnosis.4 Finally in 2009, several scientific societies, including the IDF, decided that there should be no obligatory criteria, still indicating the usefulness of waist measurements in screening for MS.
The incidence of MS in the population of Polish adults depends on sex – it noticeably rises with age; however, the increase is more apparent in women. In the 40–59 age bracket, MS affects 25.3% of women and 22.6% of men, and among 60 year olds it is diagnosed in nearly half of the female population and about one-third of the male population. Studies indicate major differences in the occurrence of MS in various regions of Poland. This syndrome is least common among female and male residents of southeastern Poland (16%–17%), and most prevalent in the western part of this country, affecting 33% of men in Wielkopolskie Province and 28% of men in Opolskie Province, as well as 26% of women in Opolskie Province and 25% of women in the Westpomeranian Province.5
According to the World Health Organization definition of 1996, menopause is the last menstrual bleeding in a woman’s life, resulting from the complete loss of ovarian follicles.6 In Poland, the average age for menopause is 43–55 years, and in the world 50.8 years.7
An increased risk of metabolic disorders in the perimenopausal period is also associated with hormonal changes. Nevertheless, most studies on the relationship between MS and postmenopausal androgen–estrogen imbalance provide inconsistent results, not explaining all metabolic disorders.8,9
Therefore, it is important to assess the contribution of genetic factors to the development of MS in postmenopausal women. Though it has not yet been fully elucidated, genetic background seems to play an important role in the predisposition to MS. Genes that may contribute to the development of this condition include MC4R. MS patients have also higher levels of markers of inflammation, such as C-reactive protein and tumor necrosis factor α. Inflammation aside, a certain role in MS genesis is also attributed to oxidative stress.10
MC4R is involved in regulating body mass through the control of food intake and energy expenditure.11 It was demonstrated in animal models that activation of MC4R lowers food intake and boosts energy expenditure, thus reducing the amount of adipose tissue.11,12 Obesity associated with an MC4R defect is the most common form of monogenic obesity. According to estimates, polymorphisms in this gene are responsible for 2.4%–4% of significant obesity. Studies conducted in Great Britain suggest that a defect in this gene is the most frequent autosomal dominant disease.13 There are also some variants in the MC4R gene, which may have preventive effects on obesity.13,14 The receptor gene for melanocortin is located on the 18th chromosome. Several variants in the MC4R gene have been identified, and rs17782313 polymorphism (T>C) is one of those frequently described.15–19 However, the role of the tested polymorphism in MS development remains unclear. Relatively few studies on these issues – only occasionally concerning postmenopausal women – have reported contradictory results.
The present research addresses the gap in the extant literature, particularly through the analysis of a specific study sample including women in the postmenopausal stage. What is more, it raises a crucial issue of MS etiology resulting from genetic predisposition, namely the presence of the MC4R polymorphism.
Material and methods
This study involved 344 healthy women, who had their last menstruation 1 year ago or earlier, from the area of the Westpomeranian Province in northwestern Poland. The criteria for inclusion in the study were nonuse of menopausal hormone therapy, lack of gynecological disorders (women had normal cytology and mammography/breast ultrasound results) and neoplastic diseases, and no psychiatric problems. The exclusion criteria were history of thyroid diseases, neoplastic diseases, cholestatic liver disease, chronic kidney disease, and chronic use of glycocorticosteroids. For the recruitment of patients, information about the program was disseminated in the local environment (local press, posters about the study were put up on noticeboards in public places, such as offices, shops, workplaces, outpatient clinics). Participants were nonrandomly selected by the snowball method. All the participants provided written informed consent to be a part of this study.
The study was conducted in accordance with the Declaration of Helsinki, and the protocol was approved by the Bioethical Commission of the Pomeranian Medical University in Szczecin (permit number KB-0012/104/11).
The study was conducted using the following methods.
Laboratory analysis
Blood for analysis was taken on an empty stomach in accordance with binding procedures, using the BD Vacutainer system (Becton Dickinson, Poland). For each patient, standard enzymatic methods were employed to determine the levels of glycemia on an empty stomach, total cholesterol, low-density lipoprotein cholesterol (LDL-C) and HDL-C, and triglycerides. Insulin levels were determined by the ELISA method using a commercial kit (DRG MedTek, Warszawa, Poland), and the levels of apolipoprotein B was determined by the immunoturbidimetric method using reagents of Dade Behring (Marburg, Germany). The analyses were performed in a certified laboratory (ISO 9001:2008 certified). The laboratory norms assumed in the study were as follows: glucose 74–99 mg/dL, total cholesterol <180 mg/dL, HDL >50 mg/dL, LDL <130 mg/dL, triglycerides (TG) <150 mg/dL, apolipoprotein B 60–117 mg/dL (the level assumed in the study was <100), and insulin 2.6–24.9 μIU/mL.
For each patient, insulin resistance (IR) (homeostatic model assessment [HOMA-IR]) index was calculated according to the formula: serum glucose level (mg/dL) × insulin level (μIU/mL) divided by 405; it was assumed in the study that women had IR if HOMA-IR index ≥2.5.
The next stage of the study was based on genetic analysis, in which DNA was isolated from whole blood by a salting-out method according to Miller.20
Genotyping of the MC4R gene rs17782313 (T>C)
Genomic DNA was isolated from whole blood according to standard procedures. All genotyping was performed with the fluorescence resonance energy transfer method real time using the Light Cycler System 1.0 (Roche Diagnostic, Poland). For polymorphism in the MC4R gene, the following conditions were applied: polymerase chain reaction was performed with 50 ng DNA in a total volume of 20 mL containing 2 mL reaction mix, 0.5 mM of each primer, 0.2 mM of each hybridization probe, and 2 mM MgCl2 according to the manufacturer’s instructions for 35 cycles of denaturation (95°C for 10 min), annealing (60°C for 10 s), and extension (72°C for 15 s). After amplification, a melting curve was generated by holding the reaction at 40°C for 20 s and then heating slowly to 85°C. The fluorescence signal was plotted against temperature to give melting curves for each sample. Peaks were obtained at 49.5°C for the T allele and at 58.23°C for the C allele.
Survey
The study involved a survey of women based on a questionnaire of the authors’ own design, concerning sociodemographic data (age, education level, place of living, marital status, and employment status).
Measurement
Height and weight as well as waist measurement were taken in a standing position. The waist was measured between the lower rib margin and the upper margin of the iliac crest at the end of a gentle exhalation. It was assumed that values ≥80 cm reflected the central distribution of adipose tissue – I0 obesity, and values ≥88 cm – II0 obesity. The body mass index (BMI, kg/m2) was calculated for each patient. Normal weight was assumed at 18.5–24.9 kg/m2, overweight at 25–29.9 kg/m2, I0 obesity at 30–34.9 kg/m2, II0 obesity at 35–39.9 kg/m2, and III0 obesity ≥40 kg/m2.
Statistical analysis
Statistical analysis was performed using Statistica 7.1 PL software package (StatSoft, OK, USA). Quantitative variables were characterized by minimum and maximum values, arithmetic mean, upper and lower quartiles, median, and standard deviation. The distribution of the quantitative variables was assessed by means of the Shapiro–Wilk test. Student’s t-test for independent variables and its nonparametric equivalent, the Mann–Whitney U test, were used to determine the significance of the difference between two groups. Based on the logistic regression model, the odds ratio (OR) with a 95% confidence interval (CI) was calculated. The relationship between qualitative variables was assessed using the chi-square (χ2) test of independence. The level of significance (α) was assumed to be 0.05.
Results
The mean age of the participants were 58.5±6.6 years, the youngest woman was 46 years old and the oldest was 65 years. The majority of the participants (53.9%) had secondary education, lived in a city with the population of >100,000 (64.2%), were married (74.8%), and were employed (67.2%). There was no relationship between the sociodemographic data and the incidence of metabolic disorders (χ2 test; P>0.05).
MS was diagnosed on the basis of the IDF criteria of 2005 in 40.7% of the whole group analyzed.
An increased BMI (≥25 kg/m2) was observed in 65.7% of the participants – overweight in 40.7% and obesity in 25%. The mean BMI was 27±4.4 kg/m2. Abdominal obesity diagnosed on the basis of waist circumference cutoffs was found in 80.3% of all women, 34% of whom had I0 obesity and 46.3% II0 obesity. In accordance with the definition proposed by the IDF in 2005, each woman with MS had abdominal obesity.
The incidence of particular MS elements was analyzed. An increased glucose level on an empty stomach was observed in 20.7% of the women, an abnormal HDL-C level was noticed in 30.2%, a TG level ≥150 mg/dL was found in 26.8%, a cholesterol level >180 mg/dL was observed in 86.6%, an LDL level >130 mg/dL in 60.4%, and apolipoprotein B ≥100 mg/dL in 48.9%.
The T/T genotype was found in 66% (227 subjects) of the total number of 344 women, 31.6% (109 subjects) had the C/T genotype, and 2.4% (8 subjects) had the C/C genotype. Considering a small number of those with the C/C genotype, further statistical analysis was conducted in two subgroups of women. The first comprised women with the T/T genotype of MC4R, and the second consisted of those with the C/X genotype, where ‘x’ denoted the C or T allele (117 subjects). The incidence of MS among patients with specific polymorphisms in the MC4R gene was gauged. In the subgroup with the T/T genotype, MS diagnosed on the basis of the IDF criteria of 2005 was found in 39.3%, and in the subgroup with the C/X genotype in 44.7%. The differences, however, were not statistically significant (χ2 test; P>0.05).
To assess the relationship between particular polymorphisms and the incidence of MS more accurately, a logistic regression model was employed. The probability of MS was higher in patients with the C/X genotype (OR =1.25), but the test value was not statistically significant (OR: 1.25; 95% CI: 0.74–2.04; P=0.42). The frequency of particular polymorphisms was also determined in women with and without an MS diagnosis. In the group of women without MS, 68.5% had the T/T genotype, which was insignificantly more than in the group with MS – 63.3% (χ2 test; P>0.05). There was also no significant difference in the frequency of the C/X genotype in the groups analyzed (χ2 test; P>0.05).
As the next step, the levels of selected metabolic parameters were assessed depending on the tested polymorphisms in the MC4R gene. There were statistically significant differences in average total cholesterol levels in serum between the groups. The group with the T/T genotype had significantly lower total cholesterol levels (218.8±41.4 mg/dL vs 227.1±44.8 mg/dL; Mann–Whitney U test; P=0.006). Analysis of the mean LDL-C levels demonstrated a significant difference between the groups. The mean LDL-C level was lower in the group with the T/T genotype (133.5±37.7 mg/dL vs 144.9±36.3 mg/dL; Student’s t-test; P=0.01). Analysis of the mean serum TG levels demonstrated that they were significantly lower in the group with the T/T genotype (118.7±52.1 mg/dL vs 131.3±72.8 mg/dL; Mann–Whitney U test; P=0.008). Analysis of the mean apolipoprotein B levels in serum revealed significant differences between the groups: levels of this protein were significantly higher in the C/X genotype group (103.7±25.5 mg/dL vs 97.2±24.1 mg/dL; Student’s t-test; P=0.03).
In the case of other MS parameters (average levels of glucose, HDL-C, and HOMA-IR [Mann–Whitney U test], and waist size and BMI [Student’s t-test]) (Table 1), no statistically significant differences were found between the groups.
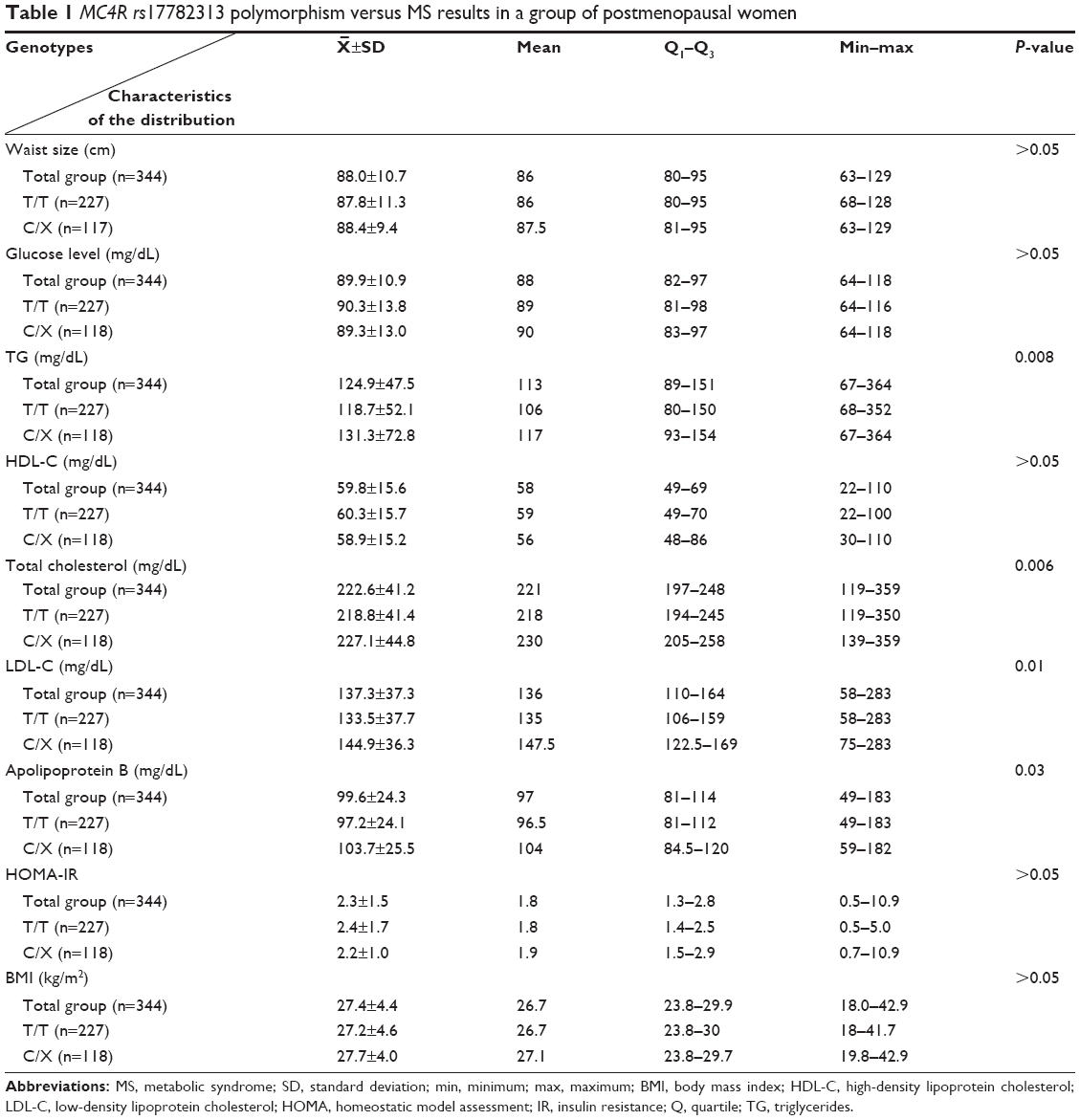 | Table 1 MC4R rs17782313 polymorphism versus MS results in a group of postmenopausal women |
Discussion
Interactions between genetic and environmental factors play an important part in the etiology of MS and obesity.21 MS diagnosed on the basis of the IDF criteria of 2005 was observed in 39.3% of women with the T/T genotype. It was slightly more common in the subgroup with the C/X genotype (44.7%); however, the difference was not statistically significant. The logistic regression model showed that the C allele raises the risk of MS (OR: 1.25), but the test value was not statistically significant. The average frequency of the C/C genotype does not exceed 5%, the C/T genotype is found in about 40% and the T/T genotype in ~55% of the population.22 Literature concerning associations between the tested polymorphism and the incidence of MS is very scanty. Even fewer are those publications that describe metabolic disorders in postmenopausal women. This present study did not provide evidence for a significant relationship between BMI and the tested polymorphism in women after menopause. Nonetheless, Chinese authors have demonstrated a substantial association between the MC4R rs17782313 polymorphism and obesity, finding a significant correlation between this polymorphism and BMI (P=0.0012).15 Similarly, Belgian authors revealed a strong connection between the MC4R rs17782313 polymorphism and obesity in the general population (OR: 1.42; 95% CI: 1.14–1.77; P=0.002).23 In an American study of >5,700 women, the authors scrutinized how the presence of the above mentioned polymorphism was related to the type of food consumed, changes in body mass, and the risk of type 2 diabetes. They found that the MC4R rs17782313 polymorphism was markedly associated with high energy expenditure (P=0.028), as well as the total fat and protein content in the diet (P=0.008 and 0.003, respectively). When assessed with reference to age and body mass, this relationship was significant. There was also a close connection between the single nucleotide polymorphism (SNP) in this gene and an increased BMI (P=0.002), and it was largely independent of the type of food intake. The BMI of the C allele carriers was higher by 0.2 kg/m2 on average. It was additionally established that the risk of diabetes in carriers of the C allele increased by 14% regardless of the BMI.24 This study did not provide evidence for the substantial influence of the risk allele on waist circumference and the development of IR. Comparable results were reported by German authors, who claimed that the presence of the C allele entailed a considerably higher BMI (P=0.0013), but had no influence on waist circumference, glucose tolerance, or insulin sensitivity. They showed that the tested SNP had an impact on the total mass of adipose tissue (P=0.022) and subcutaneous compartment (P=0.017). Such a relationship was not found in the case of visceral adipose tissue. The authors emphasized that obesity associated with polymorphism in the MC4R gene is metabolically favorable, as it is associated with accumulating fat mainly in the subcutaneous compartment, which does not contribute to IR as much as visceral adipose tissue. Since lower sensitivity to insulin is the most important pathophysiological element of MS, the above mentioned findings also suggest that this polymorphism has no impact on the development of type 2 diabetes.22,25 In the present study, the presence of the risk allele did not entail a higher glucose level on an empty stomach. Also, authors from Great Britain analyzed the connection between the presence of >10 polymorphisms (including rs17782313) and obesity. They demonstrated that the OR for obesity in carriers of this polymorphism was 1.14 (95% CI: 1.067–1.23; P<0.001), and the presence of the risk allele resulted in an increase in BMI by 0.18 kg/m2, and waist circumference by 0.43 cm.26 Chinese authors, on the other hand, conducted a meta-analysis, being a sort of summing up of the reports described above. They showed that the MC4R rs17782313 polymorphism was significantly related with a risk of obesity in the general population (OR: 1.18; 95% CI: 1.15–1.21; P<0.001).27
The relationship between the rs17782313 polymorphism and body mass was also confirmed by Danish authors – the MC4R risk allele caused an increase in the BMI by 0.25 kg/m2 and in waist circumference by 0.67 cm. There were no significant associations with the level of glucose on an empty stomach, the levels of total cholesterol, triglycerides, HDL-C, and HOMA-IR index.28 Although, in this study, the tested polymorphism did not contribute to the development of abdominal obesity, it was found that women with the C/X genotype had higher levels of total cholesterol, TG, LDL-C, and apolipoprotein B.
Different results concerning effects of the tested polymorphism on MS parameters were reported by Tao et al, who did not notice any connection between the rs17782313 polymorphism and BMI or the risk of obesity in a Chinese population. However, similar to this study, they observed a significant relationship between the risk allele and increased levels of LDL-C (P=0.003) and triglycerides (P=0.001).18 Correspondingly, Hotta et al did not demonstrate any relation between the rs17782313 polymorphism and BMI or the mass of subcutaneous and visceral adipose tissue.19 Also, Cheung et al neither provided evidence for a significant influence of the tested SNP on body mass (including the mass of visceral adipose) and the risk of obesity, nor for a significant connection between rs17782313 and the risk of MS. It is true that OR was 1.12, but likewise in this study, the test value was not statistically significant.15 Nevertheless, recent reports indicate a noteworthy association between SNP rs17782313 and MS. The authors demonstrated that the presence of C allele was a crucial risk factor for developing MS, especially when combined with nicotine addiction; yet, they analyzed premenopausal women.29
Summing up, MS is a group of coexisting risk factors for diabetes and cardiovascular diseases that are especially common in postmenopausal women. Detection of one MS component should induce active search and treatment of other elements, which is to prevent atherosclerosis and its complications. The most common MS element found in the women analyzed in this study (aside from obligatory abdominal obesity) was lower HDL-C level. MS is a multifactorial disorder determined by numerous environmental and genetic factors, hormonal changes, and genetic–environmental interactions (being of critical importance). MC4R SNPs may increase the risk of MS, but their phenotypic expression is affected by environmental factors, such as quantitative and qualitative composition of diet and physical activity. Awareness of the presence of selected mutations in the predisposing genes may improve MS prevention, and better understanding of the complex relations between genetic and environmental influences will allow targeted therapeutic interventions. The first-choice management in MS is modification of lifestyle supplemented with pharmacotherapy in selected clinical situations.
Conclusion
MS is a very common condition among postmenopausal women. The presence of the T allele of MC4R rs17782313 polymorphism noticeably reduces the incidence of lipid metabolism disorders in postmenopausal women and seems to protect against metabolic disorders in this group of women.
Acknowledgment
Financial resources for the project and funds for covering the costs to publication were provided exclusively by the Pomeranian Medical University of Szczecin.
Author contributions
JB and AB conceived and designed the experiments; JB, MS, AJ, SW-H, KK performed the experiments; JB, ML, BK analyzed the data; JB, EG, AB contributed reagents/materials/analysis tools; and JB, MS, AJ, EG wrote the paper. All authors contributed toward data analysis, drafting and revising the paper and agree to be accountable for all aspects of the work.
Disclosure
The authors report no conflicts of interest in this work.
References
Wyrzykowski B, Bandosz P, Zdrojewski T. Ocena częstoŚci występowania zespołu metabolicznego w Polsce [Evaluation of the incidence of the metabolic syndrome in Poland]. Kardioprofil. 2006; 4:3–11. | ||
Mamcarz A, Podolec P, Kopeć G, et al. Konsensus grupy roboczej PFP dotyczące zespołu metabolicznego [The consensus of the PFP working group for the metabolic syndrome]. Forum Profil. 2009;2:1–8. | ||
Wyrzykowski B. Zespół metaboliczny w praktyce klinicznej [Metabolic syndrome in clinical practice]. Gdańsk, Poland: Via Medica; 2010. | ||
Alberti KG, Zimmet PZ, Shaw JE. The metabolic syndrome – a new worldwide definition. Lancet. 2005;366:1059–1062. | ||
Zdrojewski T, Bandosz P, Szpakowski P. Rozpowszechnienie głównych czynników ryzyka chorób układu sercowo naczyniowego w Polsce. Wyniki badania NATPOL PLUS [The prevalence of major risk factors for cardiovascular diseases in Poland. The results of the NATPOL PLUS study]. Kardiol Pol. 2004;61(Suppl IV):5–26. | ||
Skałba P. Endokrynologia ginekologiczna [Gynecological endocrinology]. Warszawa, Poland: PZWL; 2005. | ||
Pertyński T, Stachowiak G, Stetkiewicz T. Rola ginekologa w okresie pre- i okołomenopauzalnym [The role of the gynecologist during the pre- and perimenopausal period]. Prz Menopauz. 2007;2:64–65. | ||
Gaspard U. Hyperinsulinaemia, a key factor of the metabolic syndrome in postmenopausal women. Maturitas. 2009;62:362–365. | ||
Golden SH, Ding J, Szklo M, Schmidt MI, DuncanBB, Dobs A. Glucose and insulin components of the metabolic syndrome are associated with hyperandrogenism in postmenopausal women: the atherosclerosis risk in communities study. Am J Epidemiol. 2004;160:540–548. | ||
Stachowiak G, Zając A, Pertyński T. Zespół metaboliczny u kobiet w okresie menopauzy [Metabolic syndrome in women during menopause]. Przegl Menopauz. 2009;1:6–10. | ||
Valassi E, Scacchi M, Cavagnini F. Neuroendocrine control of food intake. Nutr Metab Cardiovasc Dis. 2008;18:158–168. | ||
Balthasar N, Dalgaard LT, Lee CE, et al. Divergence of melanocortin pathways in the control of food intake and energy expenditure. Cell. 2005;123:493–505. | ||
Proneth B, Xiang Z, Pogozheva ID, et al. Molecular mechanism of the constitutive activation of the L250Q human melanocortin 4 receptor polymorphism. Chem Biol Drug Des. 2006;67:215–229. | ||
Alharbi KK, Spanakis E, Tan K, et al. Prevalence and functionality of paucimorphic and private MC4R mutations in a large, unselected European British population, scanned by meltMAD-GE. Hum Mutat. 2007;28:294–302. | ||
Cheung CY, Tso AW, Cheung BM, et al. Obesity susceptibility genetic variants identified from recent genome-wide association studies: implications in a Chinese population. J Clin Endocrinol Metab. 2010;95:1395–1403. | ||
Beckers S, Zegers D, de Freitas F, Mertens IL, Van Gaal LF, Van Hul W. Association study of MC4R with complex obesity and replication of the rs17782313 association signal. Mol Genet Metab. 2011;103:71–75. | ||
Li S, Zhao JH, Luan J, et al. Cumulative effects and predictive value of common obesity-susceptibility variants identified by genome-wide association studies. Am J Clin Nutr. 2010;91:184–190. | ||
Tao L, Zhang Z, Chen Z, et al. A common variant near the melanocortin 4 receptor is associated with low-density lipoprotein cholesterol and total cholesterol in the Chinese Han population. Mol Biol Rep. 2012;39:6487–6493. | ||
Hotta K, Nakamura M, Nakamura T, et al. Polymorphisms in NRXN3, TFAP2B, MSRA, LYPLAL1, FTO and MC4R and their effect on visceral fat area in the Japanese population. J Hum Genet. 2010;55:738–742. | ||
Miller S, Dykes D, Plesky H. A simple salting out procedure for extracting DNA from human nucleated cells. Nucl Acids Res. 1988;16:1215. | ||
Park S, Daily JW, Zhang X, Jin HS, Lee HJ, Lee YH. Interactions with the MC4R rs17782313 variant, mental stress and energy intake and the risk of obesity in Genome Epidemiology Study. Nutr Metab (Lond). 2016;21(13):38. | ||
Haupt W, Thamer C, Heni M, et al. Impact of variation near MC4R on whole-body fat distribution, liver fat, and weight loss. Obesity. 2009;17:1942–1945. | ||
Beckers S, Zegers D, de Freitas F, Mertens IL, Van Gaal LF, Van Hul W. Association study of MC4R with complex obesity and replication of the rs17782313 association signal. Mol Genet Metab. 2011;103:71–75. | ||
Qi L, Kraft P, Hunter DJ, Hu FB. The common obesity variant near MC4R gene is associated with higher intakes of total energy and dietary fat, weight change and diabetes risk in women. Hum Mol Genet. 2008;17:3502–3508. | ||
Tran TT, Yamamoto Y, Gesta S, Kahn CR. Beneficial effects of subcutaneous fat transplantation on metabolism. Cell Metab. 2008;7:410–420. | ||
Van Pelt RE, Evans EM, Schechtman KB, Ehsani AA, Kohrt WM. Contributions of total and regional fat mass to risk for cardiovascular disease in older women. Am J Physiol Endocrinol Metab. 2002;282:1023–1028. | ||
Xi B, Takeuchi F, Chandak GR, et al. Common polymorphism near the MC4R gene is associated with type 2 diabetes: data from a meta-analysis of 123,373 individuals. Diabetologia. 2012;55:2660–2666. | ||
Zobel DP, Andreasen CH, Grarup N, et al. Variants near MC4R are associated with obesity and influence obesity-related quantitative traits in a population of middle-aged people: studies of 14,940 Danes. Diabetes. 2009;58:757–764. | ||
Yang CW, Li CI, Liu CS, et al. The joint effect of cigarette smoking and polymorphisms on LRP5, LEPR, near MC4R and SH2B1 genes on metabolic syndrome susceptibility in Taiwan. Mol Biol Rep. 2013;40:525–533. |
 © 2017 The Author(s). This work is published and licensed by Dove Medical Press Limited. The
full terms of this license are available at https://www.dovepress.com/terms
and incorporate the Creative Commons Attribution
- Non Commercial (unported, 3.0) License.
By accessing the work you hereby accept the Terms. Non-commercial uses of the work are permitted
without any further permission from Dove Medical Press Limited, provided the work is properly
attributed. For permission for commercial use of this work, please see paragraphs 4.2 and 5 of our Terms.
© 2017 The Author(s). This work is published and licensed by Dove Medical Press Limited. The
full terms of this license are available at https://www.dovepress.com/terms
and incorporate the Creative Commons Attribution
- Non Commercial (unported, 3.0) License.
By accessing the work you hereby accept the Terms. Non-commercial uses of the work are permitted
without any further permission from Dove Medical Press Limited, provided the work is properly
attributed. For permission for commercial use of this work, please see paragraphs 4.2 and 5 of our Terms.