Back to Journals » Clinical Ophthalmology » Volume 14
Screening for Predictive Parameters Requiring Psycho-Oncological Intervention via the National Comprehensive Cancer Network Distress Thermometer in the Follow-Up of Uveal Melanoma Patients
Authors Klingenstein A ![]() , Samel C, Garip-Kuebler A, Priglinger SG, Foerster PI
, Samel C, Garip-Kuebler A, Priglinger SG, Foerster PI
Received 17 August 2020
Accepted for publication 2 October 2020
Published 9 November 2020 Volume 2020:14 Pages 3813—3819
DOI https://doi.org/10.2147/OPTH.S276848
Checked for plagiarism Yes
Review by Single anonymous peer review
Peer reviewer comments 2
Editor who approved publication: Dr Scott Fraser
Annemarie Klingenstein,1 Christina Samel,2 Aylin Garip-Kuebler,1 Siegfried G Priglinger,1 Paul I Foerster1
1Department of Ophthalmology, Ludwig-Maximilians-University, Munich, Germany; 2Institute of Medical Statistics and Computational Biology, Faculty of Medicine, University of Cologne, Cologne, Germany
Correspondence: Annemarie Klingenstein
Department of Ophthalmology, Ludwig-Maximilians-University, Klinikum der Universität München, Campus Innenstadt, Mathildenstraße 8, Munich D-80336, Germany
Tel +49 89 44005 3811
Fax +49 89 44005 5160
Email [email protected]
Aim: To assess a profile of uveal melanoma patients at risk of requiring active psycho-oncological intervention by employing the National Comprehensive Cancer Network (NCCN) distress thermometer.
Methods: Multivariate correlation and multiple linear regression analysis of data collected retrospectively from 106 consecutive patients suffering from uveal melanoma.
Results: Distress levels correlated with practical (p = 0.01), emotional (p = 0.003) and physical problems (p = 0.001) as well as the total number of issues reported (p < 0.001; ANOVA, respectively). Emotional issues added up to 39% of influence on distress levels. Nervousness, worry and sadness as the most important emotional issues tested correlated significantly with anatomic stage, tumor T-category, metastatic status and time after primary diagnosis and were present more frequently in patients with higher distress levels (p < 0.001, p = 0.002, p = 0.004, respectively, Fisher’s exact test). Pre-existing psycho-oncological support was more frequent in metastatic patients and patients with higher anatomic stage tumors (p = 0.008 and p = 0.003; Fisher’s exact test).
Conclusion: The distress thermometer proved to be useful for rapid assessment of patients requiring active intervention. A higher number of distress items recorded correlated with elevated distress levels. Emotional issues were responsible for the majority of problems. A typical patient profile at risk of developing distress requiring close attention of caregivers includes high anatomic stage, high T-category, presence of metastases and early follow-up. Correct diagnosis and interpretation of distress-levels should help improve the quality of life of uveal melanoma survivors.
Trial Registration: Not applicable.
Keywords: quality of life, NCCN distress thermometer, uveal melanoma, psycho-oncological distress, cancer
Introduction
There is a current trend in the literature that emphasizes the need for psycho-oncological support focusing on patients’ quality of life (QoL) apart from successful medical treatment in uveal melanoma patients.1–4 Importantly, the effects of the treatment on the patients’ QoL should be taken into consideration.5 As uveal melanoma is a rare disease with a prevalence of 1–9/100.000,6 data on patients’ QoL are limited and to our knowledge, the NCCN distress thermometer has not yet been evaluated for uveal melanoma patients outside of our research.
A rapid psycho-oncological screening tool that can be integrated well into clinical practice would be invaluable because many uveal melanoma patients report reduced QoL as well as substantial emotional problems in comparison with other cancer entities and normative data.7–9 In our previous research, we focused on the development of QoL after stereotactic radiosurgery10 and compared patients’ QoL after enucleation and globe-preserving therapy with the Short-form (SF)-12 Health Survey.11 In our previous analysis with the NCCN distress thermometer, higher distress levels correlated with lower visual acuity.12
The NCCN distress thermometer is composed for rapid assessment of psychosocial stress, so-called distress. High patient acceptance, concision and good practicability could be shown in the literature.13 It is composed of a continuous scale visually measuring distress levels (0–10) and a problem list that includes practical, family, emotional, spiritual/religious and physical problems. The additional list of problems attached to the distress thermometer designates which area of life needs caregiving13 (in consequence, patients are referred to a social worker, minister, psycho-oncologist or oncologist). A distress threshold of ≥5 as advised in the literature calling for assistance13 proved to be sensible for our collective of uveal melanoma patients.12
We now statistically analysed specific patient characteristics enabling us to potentially identify uveal melanoma patients in danger of developing psycho-oncological distress requiring active intervention by their caregivers via the results of the NCCN distress thermometer.
Materials and Methods
In the present study, medical and QoL data of 106 uveal melanoma patients were included. All patients gave informed consent for the completion of the NCCN distress thermometer (https://www.nccn.org/patients/resources/life_with_cancer/pdf/nccn_distress_thermometer.pdf; German version) at routine follow-up at our tumor consultation outpatient department as well as for inclusion of all relevant data from their medical files. In addition to the evaluation of the NCCN questionnaire, every patient underwent a complete ophthalmological examination including standardized A- and B-scan echography and widefield fundus photography. Data were assessed consecutively from April to December 2018. Details on descriptive patient data, best corrected visual acuity (BCVA) evaluation and calculation of the receiver operating characteristic (ROC)-threshold of the NCCN distress thermometer can be found in Klingenstein et al 2020.12 This study now adds the important calculation of concrete predictive risk factors of uveal melanoma patients to develop psycho-oncological distress in need of treatment by multivariate correlations and multiple linear regression analysis for clinical routine practice.
The current study has approval of the institutional review board of the Department of Ophthalmology and was waived by the ethics committee of Ludwig-Maximilians-University Munich, Germany. Tumor T-categorizing was performed employing the American Joint Committee on Cancer (AJCC) Staging Manual (7th ed New York, NY: Springer; 2009).
Statistical data collection was performed with Microsoft Excel (Microsoft Corporation, Redmond, WA, USA) for Mac 2011 and statistical analysis was performed with SPSS 25.0 (IBM Corporation; Armonk, NY, USA). In a first statistical model, descriptive analysis, cross-tabulations with chi-square and Fisher’s exact test were performed including calculation of correlation coefficients (Spearman’s rho). The dimensions of the NCCN as well as the number of problems reported were then fitted to multiple linear regression analyses (including ANOVA (analysis of variance) and further analysis of correlation coefficients) after Kolmogorov Smirnov testing for normal distribution. For the comparison of the number of issues between subgroups (patient and tumor characteristics), Mann–Whitney U-test was performed. Statistical significance was noted at p < 0.05 with all confidence intervals being at 95% level. As all statistical procedures are of exploratory nature, no adjustment for multiple testing has been made.
Results
We analyzed the correlation of distress levels with practical, family issues, spiritual concerns, emotional and physical issues: The total number of issues reported by the patients correlated significantly with distress levels (p < 0.001 (ANOVA); Table 1; Figure 1).
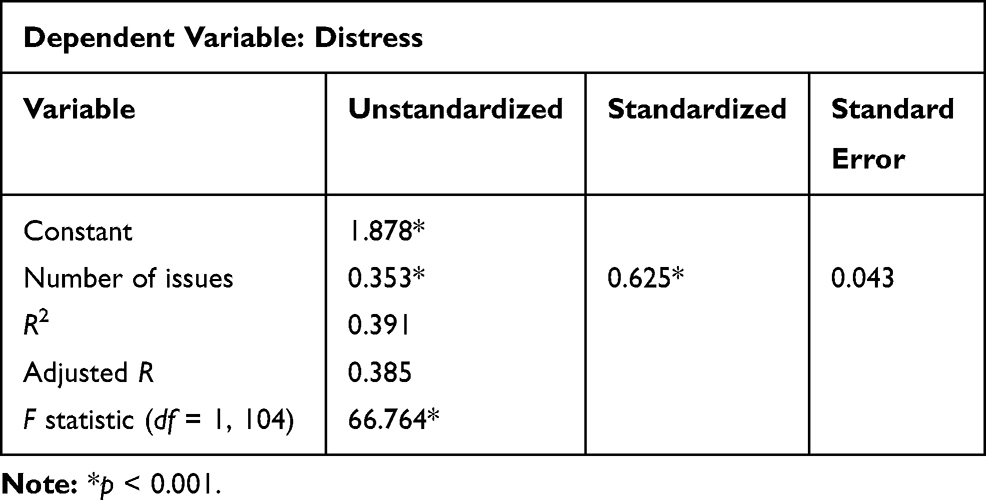 |
Table 1 Correlation of Distress and the Number of Issues on the NCCN Distress Scale |
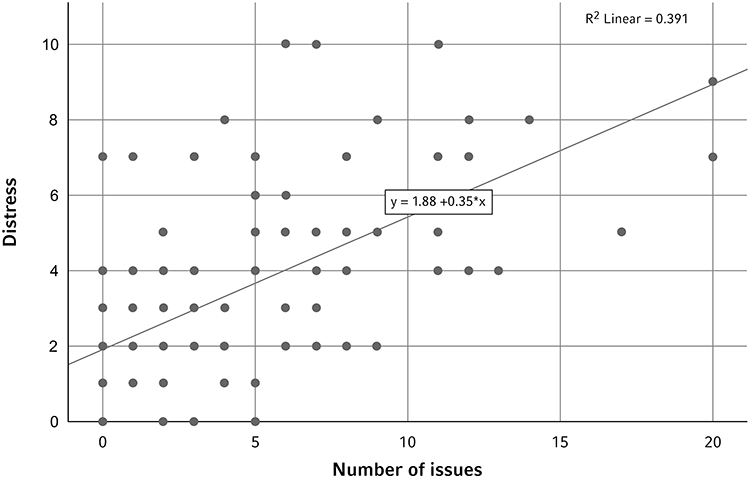 |
Figure 1 Scatterplot showing the level of distress on the NCCN distress thermometer and the total number of issues reported (practical and family, religious or spiritual, emotional and physical issues (n=106 patients)). |
Additionally, distress levels correlated significantly with the number of practical (p = 0.01), emotional (p = 0.003) and physical problems (p = 0.001) (Table 2).
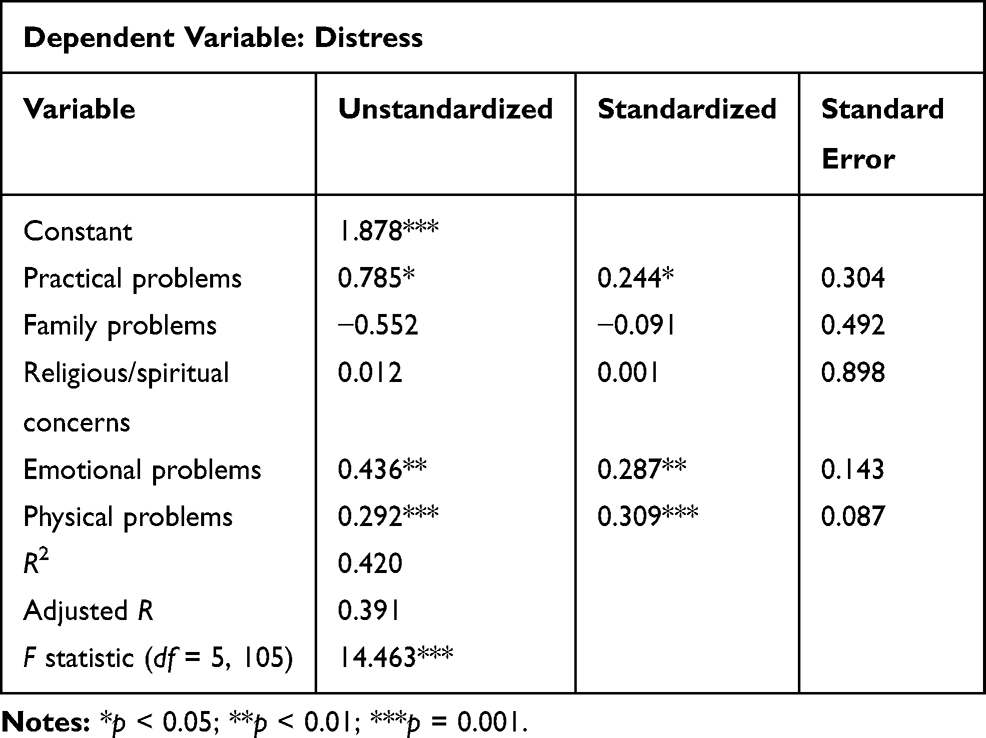 |
Table 2 Correlation of Distress and the Type of Problems on the NCCN Distress Scale |
In our correlation model, emotional issues added up to a total of 39% of influence on distress levels (adjusted R = 0.391; Table 2). When going further into detail, certain emotional issues were significantly higher in patients that reported higher distress levels (nervousness p < 0.001, worry p = 0.002, sadness p = 0.004, respectively, Fisher’s exact test; correlation p < 0.001, Spearman’s rho for all three items).
The number of physical issues seems to correlate with metastatic status (p = 0.06, Mann–Whitney U-test; Figure 2), while we could not prove this statistically due to the small number of metastatic patients. The number of emotional issues correlated with tumor T-category (p < 0.05, Spearman’s rho; Figure 3) and anatomic stage (p = 0.02, Spearman’s rho).
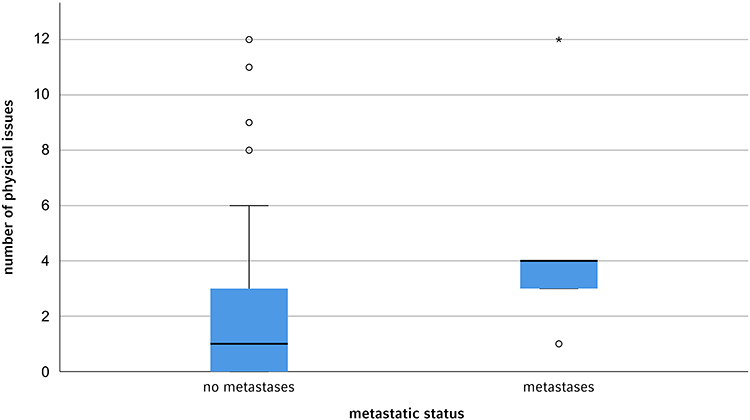 |
Figure 2 Box plot showing a higher number of physical issues in metastatic patients (n=5; outliers (at least 1.5 box lengths from the median) depicted as circles, extremes (at least 3 box lengths from the median as asterisks); p = 0.06, Mann–Whitney U-test). |
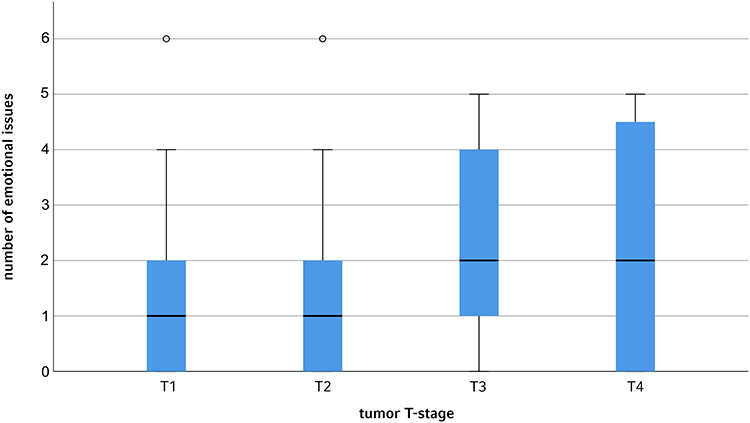 |
Figure 3 Box plot showing significantly more emotional issues in patients with higher tumor T-category (n T1/2/3/4 = 43/38/21/4). |
These factors being identified for causing psycho-oncological distress, we asked ourselves which further patient characteristics are associated with elevated levels of practical, emotional and physical issues: Patients diagnosed with higher anatomic T-category reported significantly more worries (p = 0.02, Fisher’s exact test; correlation p = 0.03, Spearman’s rho). Nervousness was marked significantly more often in patients suffering from higher T-category tumors (p = 0.04, Fisher’s exact test; correlation p = 0.03, Spearman’s rho) and a shorter time interval of assessment of the NCCN distress thermometer after primary diagnosis (0 to 6 months, n = 11 (10,4%); 6 to 36 months, n = 40 (37.7%) and greater than 36 months, n = 55 (51.9%); p = 0.04, Fisher’s exact test). Sadness was reported significantly more often in patients with higher tumor T-category as well as higher anatomic stage (p = 0.04 and p = 0.03, Fisher’s exact test; correlation p = 0.03 and p = 0.02, Spearman’s rho).
Patients with known metastases and higher anatomic stage tumors had significantly more pre-existing support due to their existent oncological guidance (p = 0.008 and p = 0.003; Fisher’s exact test, respectively). There was a positive correlation between metastatic status and pre-existing help (p = 0.008; Spearman’s rho).
Discussion
International guidelines prioritize introducing routine emotional distress screening in cancer care to accurately identify patients who need psycho-oncological treatment most, and ensure that patients can access appropriate supportive care.14
As uveal melanoma severely threatens patients with early death, visual handicap, and potential loss of the eye,1,3 we wanted to distinguish specific patient characteristics that may result in an elevated risk of distress. These relevant patient characteristics having a direct influence on psycho-oncological needs could be of great value for the treating clinician in everyday practice: Early intervention has been proven crucial to improve patients’ QoL and decrease psychiatric and psychosocial distress in meta-analyses.15–17
On the one hand, distress levels correlated significantly with the total amount of issues reported in this patient collective. We derive from this observation that overall, the QoL issues reported seem to have an additive effect on the distress level perceived by the patients. On the other hand, emotional issues could be attributed to have especially high impact (accounting for 39% in total) on psycho-oncological distress. Different meta-analyses proved improvement of QoL by psychosocial interventions as well as relaxation trainings in emotionally distressed patients.16,17 Therefore, screening and early intervention is crucial for these patients.
In a recent US American study, only a small percentage of uveal melanoma patients reported an existing offer of psychological support and there was vast dissatisfaction with psychological counseling.3 The percentage of patients that reported pre-existing psychological support was similar to our study (13.3% versus 10.4% of patients12). Yet, reportedly, only a limited number of patients suffering from distress accepts referrals to or turns to psycho-oncological support services with predictors and barriers to psycho-oncological support service utilization being under-studied.14 Providing psycho-oncological support seems to be much more integrated into the clinical routine of general practitioners and oncologists than ophthalmologists: Patients with positive metastatic status and higher anatomic stage tumors reported significantly more pre-existing help by their caregivers (p = 0.008 and p = 0.003) with a positive correlation between metastatic status and pre-existing help (p = 0.008). Of course, these patients represent the most seriously affected patient subgroup, so their adequate counseling is of utmost importance. Yet, ophthalmologists should take this observation as a leading example for uveal melanoma patients in general, especially, as uveal melanoma is for the most part treated in a single-session or hypo-fractionated therapy and patients consequently are left alone soon after therapy when ocular adverse effects develop after a certain latency. After successful local tumor therapy, monitoring and all related issues lie within the responsibility of the treating ophthalmologist.12
A recent study polling uveal melanoma patients found that at 1 and 3 months after primary diagnosis, health information and psychological needs were most relevant and associated psychosocial factors should be identified for proactive supportive intervention.1 In a first evaluation of the five problem fields attached to the distress thermometer, time after diagnosis had no significant impact on distress levels.12 Yet, when going further into detail, we could now prove that the emotional sub-items nervousness, worry and sadness were indeed more frequent early on. This can be seen in accordance with the literature, where critical points throughout the course of cancer include the primary diagnosis, treatment endpoint, recurrence as well as disease progression and the palliative stage.18
The threshold value of distress ≥5 demanding active intervention that is proposed in the guidelines of the NCCN distress thermometer13 fits our own ROC analysis.12 Yet, this cut-off could be reconsidered and support could be offered proactively to patients that fit certain characteristics found above that are especially susceptible to psycho-oncological distress at a lower threshold, e.g. ≥4.
As distress could be correlated with a higher mortality rate in patients that developed cancer in a recent large multicenter study,19 early detection and treatment of distress could be secondarily preventive for further diseases giving screening with the NCCN distress thermometer utmost importance.
Of course, a multitude of questionnaires for assessment of patients’ QoL have been developed (e.g. the SF-36 or −12 Health Survey or the European Organisation for Research and Treatment of Cancer (EORTC) QLQ-C30), some even with additional modules for uveal melanoma,20 whereas the NCCN distress thermometer was not specifically developed for uveal melanoma patients. We have discussed the advantages of the NCCN distress thermometer in comparison with the SF-12 Health Survey previously.12 In brief, the NCCN distress thermometer enables both rapid completion as well as fast visualization and interpretation of the data acquired. Additionally, for basic screening, the NCCN distress thermometer requires no further scoring software for interpretation.
We are aware that psycho-oncological items are very complex, not always equally weighed and thus difficult to evaluate in statistical (metric) terms. The NCCN distress thermometer pictures a scaled thermometer as a continuous visual analog scale from 0 to 10 with the same distances between each calibration line. In order to avoid haphazard grouping in ordinal and extreme coarsening of graduate data in logistic regression, we thus treated distress as a metric variable employing a linear regression for statistical analysis of the correlation of distress and the number of issues reported as well as the five items of the distress thermometer.
In conclusion, special attention that may cause higher distress levels should be paid to the following patient characteristics: Patients suffering from higher T-category and anatomic stage tumors, metastatic patients and patients who report worry, nervousness, and sadness amongst emotional issues.
In this study, we could show that the NCCN distress thermometer is a rapid tool for screening psycho-oncological distress in uveal melanoma patients. It can be applied well not only by the treating ophthalmologists, but equally important also by the patients’ oncologists or general practitioners. Our preliminary results can give clinicians insights into patient profiles that need access to psycho-oncological interventions and should be validated in further studies to support these findings and improve the QoL of uveal melanoma survivors. Furthermore, the characteristics found to be predictive of developing distress requiring psycho-oncological intervention in uveal melanoma patients could be applicable for patients suffering from other tumor entities, giving us large potential for future interdisciplinary studies.
Availability of Data and Materials
The datasets used and/or analysed during the current study are available from the corresponding author upon reasonable request.
Abbreviations
EORTC, European Organisation for Research and Treatment of Cancer; NCCN, National Comprehensive Cancer Network; QoL, quality of life.
Ethics Approval and Consent to Participate
The study was waived by the ethics committee of Ludwig-Maximilians-University, Munich, Germany (project number 20-462 KB), giving their “declaration of no objection” and approving “no consulting obligation” regarding the assessment of uveal melanoma patients’ quality of life via the validated survey. All patients gave informed consent for the completion of the NCCN distress thermometer at follow-up.
Author Contributions
AK conducted the design of the study and wrote the manuscript. CS performed statistical data analysis. AGK and SGP contributed in writing the manuscript. PIF collected clinical patient data and contributed in writing the manuscript. All authors made a significant contribution to the work reported, whether that is in the conception, study design, execution, acquisition of data, analysis and interpretation, or in all these areas; took part in drafting, revising or critically reviewing the article; gave final approval of the version to be published; have agreed on the journal to which the article has been submitted; and agree to be accountable for all aspects of the work.
Funding
There is no funding to report.
Disclosure
The authors report no conflicts of interest for this work. The abstract of this paper has been presented at the 38th ESOPRS Annual Meeting 12–14 September 2019 in Hamburg, Germany, under the following title: Profiling for Distress Requiring Intervention via the National Comprehensive Cancer Network Distress Thermometer in Uveal Melanoma Patients.
References
1. Williamson TJ, Jorge-Miller A, McCannel TA, Beran TM, Stanton AL. Sociodemographic, medical, and psychosocial factors associated with supportive care needs in adults diagnosed with uveal melanoma. JAMA Ophthalmol. 2018;136(4):356–363. doi:10.1001/jamaophthalmol.2018.0019
2. Frenkel S, Rosenne H, Briscoe D, et al. Long-term uveal melanoma survivors: measuring their quality of life. Acta Ophthalmol. 2018;96(4):e421–e426. doi:10.1111/aos.13655
3. Afshar AR, Deiner M, Allen G, Damato BE. The patient’s experience of ocular melanoma in the US: a survey of the ocular melanoma foundation. Ocul Oncol Pathol. 2018;4(5):280–290. doi:10.1159/000485189
4. van Beek JGM, Buitendijk GHS, Timman R, et al. Quality of life: fractionated stereotactic radiotherapy versus enucleation treatment in uveal melanoma patients. Acta Ophthalmol. 2018;96(8):841–848. doi:10.1111/aos.13823
5. Foss AJE, Lamping DL, Schroter S, Hungerford J. Development and validation of a patient based measure of outcome in ocular melanoma. Br J Ophthalmol. 2000;84:347–351. doi:10.1136/bjo.84.4.347
6. Orphanet [homepage on the Internet]. Available from: https://www.orpha.net/consor/cgibin/Disease_Search.
7. Brandberg Y, Kock E, Oskar K, Af Trampe E, Seregard S. Psychological reactions and quality of life in patients with posterior uveal melanoma treated with ruthenium plaque therapy or enucleation: a one year follow-up study. Eye. 2000;14(6):839–846. doi:10.1038/eye.2000.233
8. Brandberg Y, Månsson-Brahme E, Rindborg U, Sjödén PO. Psychological reactions in patients with malignant melanoma. Eur J Cancer. 1995;31:157–162. doi:10.1016/0959-8049(94)00333-Z
9. Hjermstad MJ, Fayers PM, Bjørdal K, Kaasa S. Health related quality of life in the general Norwegian population assessed by the European Organization for research and treatment of cancer core Quality of Life Questionnaire: the QLQ-C30 (+3). J Clin Oncol. 1998;16:1188–1196. doi:10.1200/JCO.1998.16.3.1188
10. Klingenstein A, Fürweger C, Nentwich MM, et al. Quality of life in the follow-up of uveal melanoma patients after CyberKnife treatment. Melanoma Res. 2013;23(6):481–488. doi:10.1097/CMR.0000000000000023
11. Klingenstein A, Fürweger C, Mühlhofer AK, et al. Quality of life in the follow-up of uveal melanoma patients after enucleation in comparison to CyberKnife treatment. Graefes Arch Clin Exp Ophthalmol. 2016;254(5):1005–1012. doi:10.1007/s00417-015-3216-7
12. Klingenstein A, Samel C, Garip-Kuebler A, et al. The national comprehensive cancer network distress thermometer as a screening tool for the evaluation of quality of life in uveal melanoma patients. Acta Ophthalmol. 2020;98(3):e381–e287. doi:10.1111/aos.14277
13. Mehnert A, Müller D, Lehmann C, Koch U. Die deutsche Version des NCCN Distress-Thermometers. Empirische Prüfung eines Screening-Instruments zur Erfassung psychosozialer Belastung bei Krebspatienten. Z Klin Psychol Psychopathol Psychother. 2006;54(3):213–223. doi:10.1024/1661-4747.54.3.213
14. Zwahlen D, Tondorf T, Rothschild S, et al. Understanding why cancer patients accept or turn down psycho-oncological support: a prospective observational study including patients’ and clinicians’ perspectives on communication about distress. BMC Cancer. 2017;17(1):385. doi:10.1186/s12885-017-3362-x
15. Meyer TJ, Mark MM. Effects of psychosocial interventions with adult cancer patients: a meta-analysis of randomized experiments. Health Psychol. 1995;14:101–108. doi:10.1037/0278-6133.14.2.101
16. Lübbert K, Dahme B, Hasenbring M. The effectiveness of relaxation training in reducing treatment-related symptoms and improving emotional adjustment in acute non-surgical cancer treatment: a meta-analytical review. Psychooncology. 2001;10(6):490–502. doi:10.1002/pon.537
17. van’t Spijker A, Trijsburg RW, Duivenvoorden HJ. Psychological sequelae of cancer diagnosis: a meta-analytical review of 58 studies after 1980. Psychosom Med. 1997;59:280–293.
18. McCormick TR, Conley BJ. Patients’ perspectives on dying and on the care of dying patients. West J Med. 1995;163:236–243.
19. Batty GD, Russ TC, Stamatakis E, Kivimäki M. Psychological distress in relation to site specific cancer mortality: pooling of unpublished data from 16 prospective cohort studies. BMJ. 2017;356:j108. doi:10.1136/bmj.j108
20. Brandberg Y, Damato B, Kivelä T, Kock E, Seregard S. The EORTC ophthalmic quality of life questionnaire module (EORTC QLQ-OPT30). Development and pre-testing (Phase I-III). Eye. 2004;18(3):283–289.
 © 2020 The Author(s). This work is published and licensed by Dove Medical Press Limited. The
full terms of this license are available at https://www.dovepress.com/terms
and incorporate the Creative Commons Attribution
- Non Commercial (unported, 3.0) License.
By accessing the work you hereby accept the Terms. Non-commercial uses of the work are permitted
without any further permission from Dove Medical Press Limited, provided the work is properly
attributed. For permission for commercial use of this work, please see paragraphs 4.2 and 5 of our Terms.
© 2020 The Author(s). This work is published and licensed by Dove Medical Press Limited. The
full terms of this license are available at https://www.dovepress.com/terms
and incorporate the Creative Commons Attribution
- Non Commercial (unported, 3.0) License.
By accessing the work you hereby accept the Terms. Non-commercial uses of the work are permitted
without any further permission from Dove Medical Press Limited, provided the work is properly
attributed. For permission for commercial use of this work, please see paragraphs 4.2 and 5 of our Terms.