Back to Journals » International Journal of Women's Health » Volume 17
Screening for Cervical Intraepithelial Lesions with TCT and HPV DNA: A Triage Strategy
Authors Song M, Mao M, Zhao H, Chen C
Received 4 September 2025
Accepted for publication 10 December 2025
Published 16 December 2025 Volume 2025:17 Pages 5487—5495
DOI https://doi.org/10.2147/IJWH.S565280
Checked for plagiarism Yes
Review by Single anonymous peer review
Peer reviewer comments 2
Editor who approved publication: Dr Everett Magann
Meiyu Song, Minhong Mao, Huirong Zhao, Chen Chen
Department of Obstetrics and Gynecology, Beijing Chaoyang Hospital, Capital Medical University, Beijing, 100043, People’s Republic of China
Correspondence: Meiyu Song, Department of Obstetrics and Gynecology, Beijing Chaoyang Hospital, Capital Medical University, No. 5, Jingyuan Road, Shijingshan District, Beijing, 100043, People’s Republic of China, Email [email protected]
Objective: To explore the value of the ThinPrep cytology test (TCT) combined with human papillomavirus (HPV) DNA detection in the screening and triage of cervical lesions.
Methods: A total of 1671 patients with cervical inflammation or lesions who underwent colposcopy and biopsy between April 2020 and December 2022 were analyzed. The data included TCT, HPV DNA, and pathological findings.
Results: The incidence of high-grade squamous intraepithelial lesions (HSILs) or above significantly increased with TCT severity: 25.9% in the negative for intraepithelial lesion or malignancy (NILM) group, 39.4% in the atypical squamous cells of undetermined significance (ASCUS) and low-grade SIL (LSIL) groups, and 76.5% in the HSIL+ group (P< 0.001 for all pairwise comparisons). The incidence also varied significantly by HPV status: 58.2% in the HPV 16 or 18 group, 28.6% in the other high-risk groups, and 17.6% in the low-risk and negative groups (P< 0.001 for all pairwise comparisons). Multivariate analysis revealed independent risk factors for HSIL+: younger age (OR=0.972), HSIL and above cytology (OR=10.154), ASCUS and LSIL cytology (OR=2.250), HPV 16/18 infection (OR=8.061), and other high-risk HPV infections (OR=2.578). Patients with concurrent HPV 16/18 infection and HSIL or above cytology presented a substantially elevated risk (OR=41.517). Among the cohort, 35 cases of cervical squamous cell carcinoma were identified.
Conclusion: TCT combined with HPV DNA testing provides an effective strategy for risk stratification in cervical screening. Our findings support that patients with HPV16 or 18 should be referred directly for colposcopy, and patients with other high-risk HPV types and TCT results of ASCUS and above are also recommended for colposcopy referrals. These referral suggestions warrant further validation in larger, multicenter studies.
Keywords: cervical cancer, precancerous lesions, ThinPrep cytology test, HPV DNA detection, colposcopy referral, risk stratification
Introduction
Cervical cancer poses a serious threat to women’s health and remains a significant global health challenge.1,2 According to the latest global cancer statistics (GLOBOCAN 2022), there were an estimated 660,000 new cases of cervical cancer and over 340,000 deaths worldwide in 2022,3 a figure that underscores the persistent global burden also highlighted in earlier reports.4 The burden of cervical cancer is particularly heavy in China, which has faced a continuous challenge because of its increasing incidence and mortality rates.5,6 Persistent infection with high-risk human papillomavirus (HR-HPV) is a necessary condition for the development of cervical cancer.7 This understanding has made cervical cancer a preventable disease through effective screening and early intervention, with prophylactic vaccination serving as another cornerstone of prevention.8 Therefore, optimizing screening strategies is crucial for eliminating cervical cancer.1,9
Over the past two decades, cervical cancer screening strategies have undergone a fundamental shift, moving from traditional cytology-based screening (eg, Pap smear or liquid-based cytology, TCT) to primary screening, which is based on the detection of HR-HPV. A large-scale real-world study in China confirmed that the sensitivity of HPV testing for detecting high-grade squamous intraepithelial lesions (CIN2+) was 96.7%, which was significantly greater than the 64.9% sensitivity of cytology.10 On the basis of such evidence, the World Health Organization (WHO) and various national expert consensuses now recommend primary HPV testing as the preferred screening method.9,11
Despite the advantage of high sensitivity, the relatively low specificity of primary HPV screening remains a major challenge. Since most HR-HPV infections are transient and can be cleared by the immune system within 1–2 years, lower specificity leads to the detection of numerous HPV-positive results with no clinical risk of progression. This not only increases unnecessary colposcopy referrals, causing psychological anxiety and financial burdens for women but also strains healthcare resources.10,11 Thus, the effective triage of the HPV-positive population to accurately identify individuals at high risk of progression has become a central issue in modern cervical cancer screening.
To address this, risk-based triage strategies have emerged. These strategies assess risk by combining cytology, HPV genotyping (especially identifying HPV 16/18), or novel molecular biomarkers such as p16/Ki-67 dual staining.12 HPV16 and HPV18 are the main high-risk genotypes responsible for approximately 70% of cervical cancers worldwide. A recent meta-analysis revealed that women positive for HPV16 or HPV18, even those with negative cytology, face a significantly greater immediate risk of CIN3+ than those with other HR-HPV genotypes.13 Consequently, guidelines from authoritative bodies such as the American Cancer Society (ACS) emphasize individualized management on the basis of risk factors, recommending direct colposcopy referrals for HPV 16/18-positive individuals to maximize screening benefits.14 This review aims to systematically summarize the core strategies, challenges, and future directions in cervical cancer screening.
Object and Method
Research Subjects
This study enrolled 1671 patients with cervical inflammation or lesions who underwent colposcopy-guided biopsy at Beijing Chaoyang Hospital (Shijingshan Campus), Capital Medical University, between April 2020 and December 2022. The inclusion criteria were as follows: (1) ASCUS or higher-grade cytology (TCT) or high-risk HPV positivity requiring colposcopic biopsy; (2) histopathological classification into chronic cervicitis (CC), low-grade squamous intraepithelial lesions (LSILs), high-grade squamous intraepithelial lesions (HSILs), or squamous cell carcinoma (SCC); and (3) complete clinical documentation. The decision for colposcopy-guided biopsy was based on 2019 ASCCP Risk-Based Management Consensus Guidelines for Abnormal Cervical Cancer Screening Tests and Cancer Precursors,15 where patients with abnormal TCT results (ASCUS or higher) or positive HR-HPV tests are referred for further evaluation to exclude high-grade lesions, even in cases of cervical inflammation. This approach ensures comprehensive assessment of potential precancerous changes, as inflammation alone may not preclude underlying neoplasia. The exclusion criteria were as follows: (1) pregnancy or lactation and (2) prior cervical surgery, conization, hysterectomy, or pelvic radiotherapy.
Research Methods
Specimen Collection
The collection of samples from patients is the responsibility of our hospital’s gynecologists. Sexual activity is prohibited 24 hours before the examination, and vaginal flushing or medication is prohibited 72 hours before the examination to avoid menstruation. TCT was performed on the collected cervical cell samples (Haoluo Jie Medical Technology Beijing Co., Ltd), and thin layer cell images were prepared. The results were interpreted according to the Bethesda System (TBS) cervical cytology classification:16 negative for intraepithelial lesion or malignancy (NILM), atypical squamous epithelial cells of unknown significance (ASCUS), highly squamous intraepithelial neoplasia (ASC-H), LSILs, HSILs, and SCC cannot be ruled out. ASCUS and above lesions are diagnosed as TCT positive. The samples were divided into three groups: the NILM group, the ASCUS and LSIL groups, and the HSIL and above (HSIL+) group.
HPV DNA Testing
The patient’s cervix was fully exposed through a speculum, excess secretions around the cervical opening were cleansed, and a professional HPV collector was used to collect exfoliated cells from the patient’s cervical opening and cervical canal. After collection, the sample is collected in a dedicated specimen storage bottle, labeled in a standardized manner, and isolated for storage. Using the HR-HPV typing nucleic acid assay kit produced by Chaozhou Kaipu Biochemical Co., Ltd. (batch number: C230403A), PCR+membrane hybridization technology was used to detect 18 HR-HPV gene subtypes, including HPV16, 18, 26, 31, 33, 35, 39, 45, 51, 52, 53, 56, 58, 59, 66, 68, 73, and 82 types, in the cervical cells of patients. The instructions of the reagent kit were followed according to the manufacturer’s instructions. According to the HPV typing results, the patients were divided into 16- or 18-type groups: high-risk, low-risk, and negative.
Colposcopic Examination and Pathological Diagnosis Protocol
After informed consent is obtained from patients undergoing pathological examination, the same senior vaginal colposcopy physician should perform a vaginal colposcopy examination on high-risk, HPV-positive individuals with TCT results of ASCUS or above. Abnormal patterns on colposcopy include white epithelium, punctate blood vessels, coarse and fine inlays, atypical blood vessels, etc. Patients with positive results should undergo regional multipoint positioning biopsy. The biopsy samples under the microscope were fixed, embedded, sliced, and stained with conventional HE using 4% neutral formaldehyde. Pathological diagnosis will be made by pathologists after reviewing the film and will be reviewed by senior doctors. The pathological diagnoses included CC, LSIL, HSIL, and SCC. The patients were divided into three groups: the inflammation group, low-grade squamous intraepithelial lesion (LSIL) group, HSIL group, and cervical cancer group.
Statistical Methods
Data management utilized Excel 2020, with statistical analyses performed in SPSS 20.0. Continuous variables are presented as the means ± standard deviations (SDs), whereas categorical data are reported as frequencies and percentages. Intergroup comparisons were performed via independent samples t tests or χ2-tests. Univariate logistic regression identified variables associated with high-grade cervical lesions (P<0.1 for multivariate inclusion). Stepwise multivariate logistic regression was used to determine independent risk factors, with statistical significance defined as P<0.05.
Results
Basic Information
A total of 1671 patients were selected, with 1067 patients in the group with inflammation and low-grade lesions detected by vaginal biopsy pathology, with an average age of 44.86 ± 11.58 years, and 604 patients in the group with high-grade lesions or above, with an average age of 40.51 ± 11.06 years. The high-grade lesion group was significantly younger than the inflammation/low-grade lesion group was (P=0.001; Table 1). Among the research subjects, 501 postmenopausal patients were included, including 370 patients in the group with inflammation and low-grade lesions detected by vaginal biopsy pathology and 131 patients in the group with high-grade lesions or above. There were a total of 1170 premenopausal patients, including 697 patients in the group with inflammation and low-grade lesions detected by vaginal biopsy pathology and 473 patients in the group with high-grade lesions or above. The proportion of postmenopausal women was significantly lower in the high-grade lesion group than in the inflammation/low-grade lesion group (P=0.001; Table 1). A total of 35 patients with cervical squamous cell carcinoma were screened, including 14 patients aged 30--39 years, accounting for 40%, and 10 patients aged 45--54 years, accounting for 28.6%.
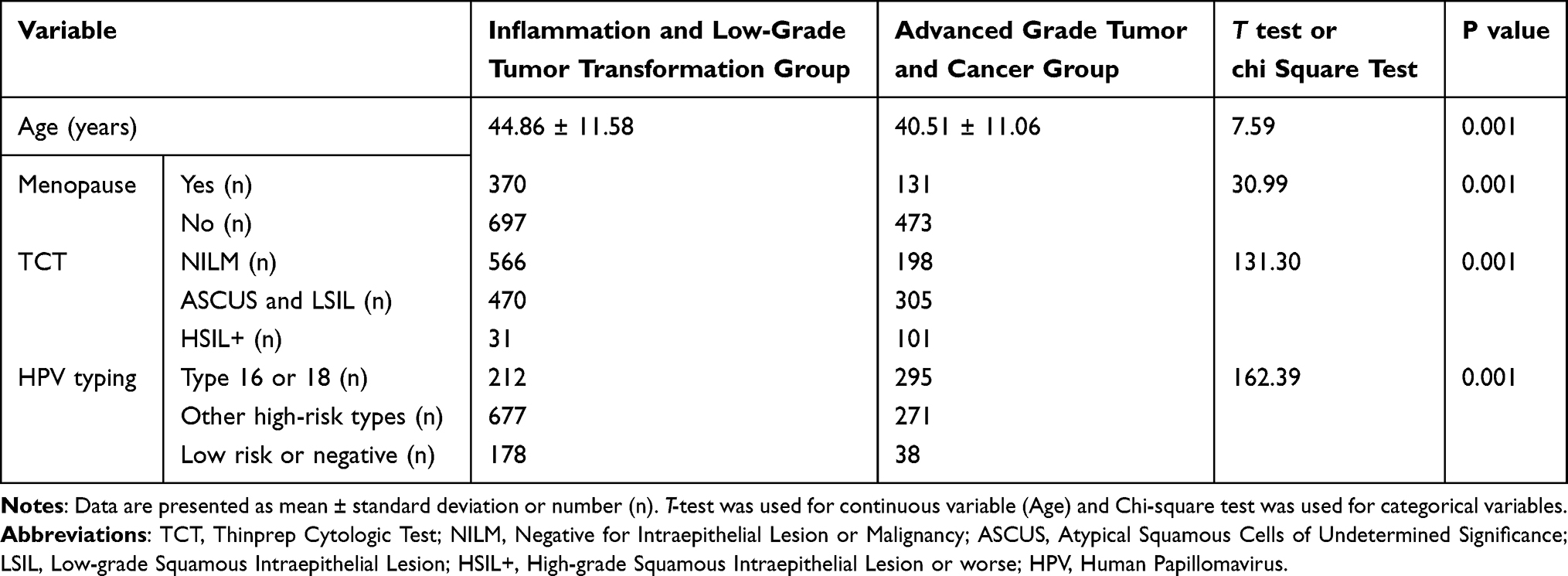 |
Table 1 Comparison of Variables Between the Inflammation or Low-Grade Tumor Transformation Group and the High-Grade Tumor Transformation or Cancerous Transformation Group According to Pathology |
Distribution of Cervical Lesions by TCT Category
The distribution of TCT categories differed significantly between the pathological outcome groups (P<0.001, Table 1). Consistent with these findings, the incidence of high-grade lesions significantly increased with increasing severity of cytological abnormalities: 25.9% (198/764) in the NILM group, 39.4% (305/775) in the ASCUS/LSIL group, and 76.5% (101/132) in the HSIL+ group (P<0.001 for trend). Post hoc pairwise comparisons confirmed that the differences in the incidence of high-grade lesions between every two TCT categories were statistically significant (all P<0.001, Table 2).
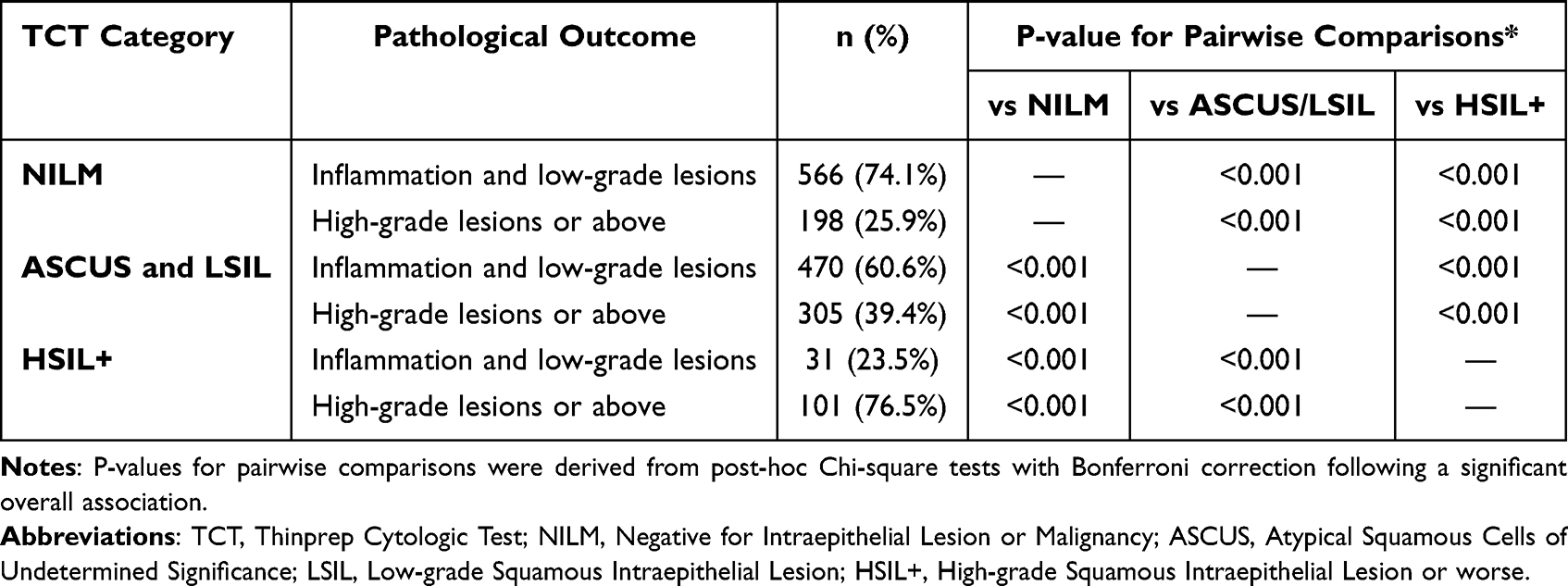 |
Table 2 Pairwise Comparisons of Pathological Outcomes Across TCT Categories |
High-Grade Lesion Incidence Stratified by HPV Genotype
A significant association was also observed between HPV genotyping risk groups and pathological outcomes (P<0.001, Table 1). The incidence of high-grade lesions varied markedly by HPV status, being highest in the HPV 16/18 group (58.2%, 295/507), intermediate in the other high-risk HPV group (28.6%, 271/948), and lowest in the low-risk/negative group (17.6%, 38/216). Pairwise comparisons revealed statistically significant differences in the incidence of high-grade lesions across all three HPV risk groups (all P<0.001, Table 3).
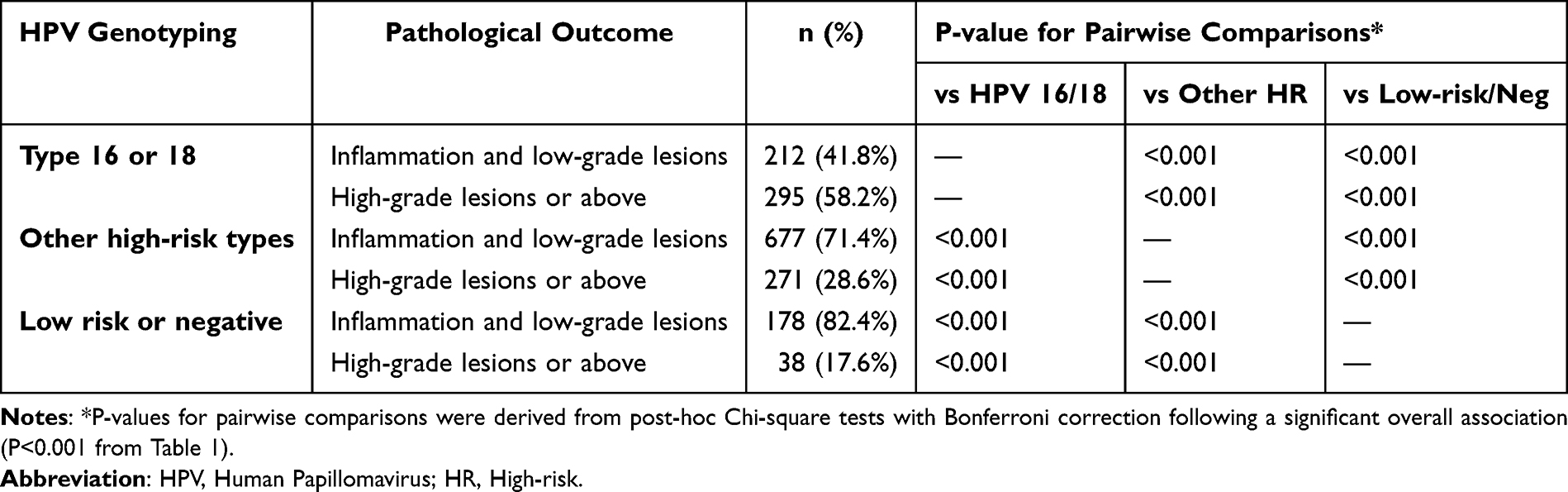 |
Table 3 Pairwise Comparisons of Pathological Outcomes Across HPV Genotyping Risk Groups |
Screening of Independent Risk Factors
Univariate logistic regression of the variables in Table 1 identified candidate variables (P<0.1, listed in Table 4) for multivariate analysis. The multivariate model established the following independent risk factors for high-grade cervical lesions: age (OR=0.972, 95% CI: 0.962–0.982; P=0.001), HSIL+ pathology (OR=10.154, 95% CI: 6.297–16.374; P=0.001; note: OR magnitude contradicts the CI direction), ASCUS/LSIL cytology (OR=2.250, 95% CI: 1.778–2.847; P=0.001), HPV 16/18 infection (OR=8.061, 95% CI: 5.293–12.278; P=0.001), and other high-risk HPV types (OR=2.578, 95% CI: 1.729–3.844; P=0.001). Crucially, patients with concurrent HPV 16/18 infection and HSIL+ cytology presented a substantially elevated risk of high-grade histopathological lesions (OR=41.517, 95% CI: 14.538–118.595; P=0.001).
 |
Table 4 Univariate and Multivariate Logistic Regression Analysis of Risk Factors for High-Grade Cervical Lesions or Above |
Prediction of High-Grade Cervical Lesions and Above by Combining HPV DNA Testing and TCT
The positive predictive values (PPVs) for high-grade lesions based on the combination of TCT and HPV genotyping are summarized in Table 5. In this study, the incidence of high-grade cervical lesions and above was 45.5% in patients with HPV genotypes of 16 or 18 and TCT results of NILM. When the TCT results were ASCUS or LSIL, the incidence of high-grade cervical lesions and above was 64.6%. When the TCT result was HSIL or above, the incidence of high-grade cervical lesions or above was 83.6% (Table 5).
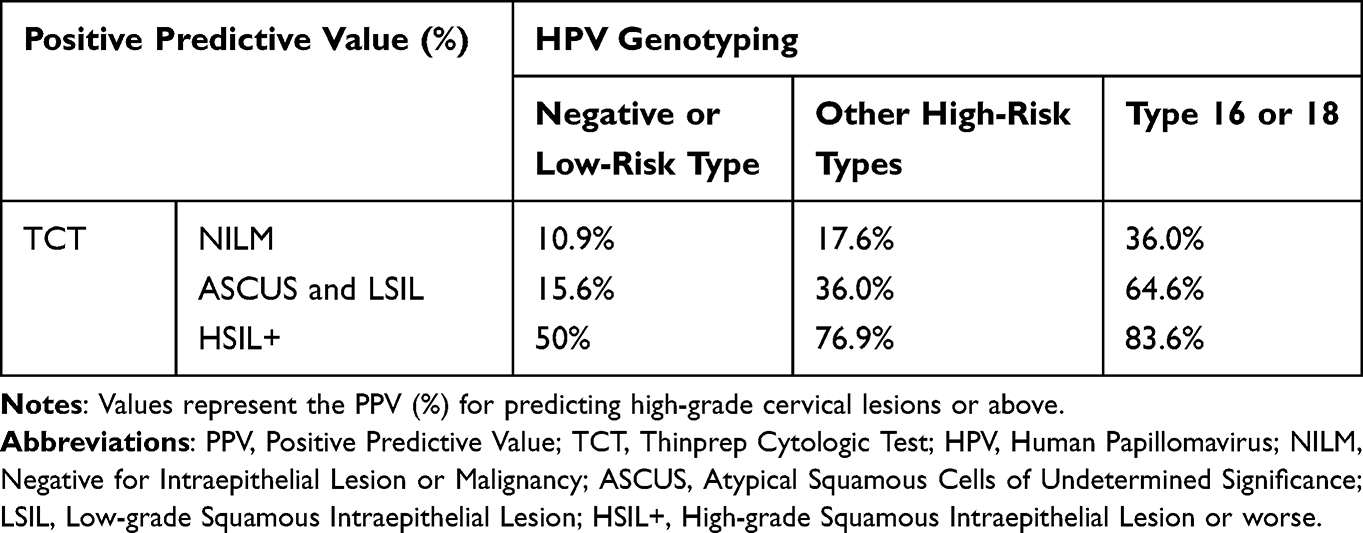 |
Table 5 Positive Predictive Value (PPV, %) of Different Combinations of TCT Results and HPV Genotyping for Predicting High-Grade Cervical Lesions or Above |
Discussions
Cervical cancer is currently the sole malignancy with a definitively established etiology that enables early detection and effective prevention.17 The pathogenic continuum spanning initial HPV infection through cervical intraepithelial neoplasia to invasive carcinoma development represents an extended multistage process. The prolonged duration of precancerous manifestations provides critical opportunities for cervical cancer screening. Consequently, the development of refined cotesting methodologies and evidence-based referral algorithms is essential for the timely identification and therapeutic intervention of cervical precancerous states, thereby effectively reducing disease incidence and mortality.
Within our investigation, histopathological stratification of 1671 colposcopy patients delineated inflammation/low-grade lesions versus high-grade lesions/carcinoma cohorts. Compared with the inflammation/low-grade cohort, the high-grade lesion group presented a significantly lower mean age and a lower menopausal incidence, potentially reflecting the earlier age of onset of cervical cancer. Among the 35 identified squamous cell carcinomas, 40.0% were aged 30–39 years, and 28.6% were aged 45–54 years, establishing a bimodal pattern with a heightened initial peak magnitude—consistent with established epidemiological trends.16
Liquid-based cytology (TCT) maintains widespread utilization for detecting cervical precancer lesions.18 Categorization by TCT findings (NILM, ASCUS/LSIL, HSIL+) revealed progressively increasing biopsy-confirmed high-grade lesion frequencies: 25.9% (NILM), 39.4% (ASCUS/LSIL), and 76.5% (HSIL+), with statistically significant intergroup differences. Multivariate regression confirmed that cytological abnormality severity was directly correlated with histopathological risk escalation, showing a maximum likelihood of progression for HSIL+ patients and an intermediate risk for ASCUS/LSIL (OR=2.250) when referenced against NILM.19
For patients identified with high-grade lesions requiring treatment, both cold knife conization and carbon dioxide (CO2) laser conization are well-established therapeutic options. A recent large-scale analysis by Ferrari et al20 demonstrated that while CO2 laser conization achieved a significantly lower overall rate of positive margins than cold knife conization did (4.3% vs 13.3%, p=0.015), both techniques provided equivalent oncological outcomes for patients with incidental cervical cancer. These findings underscore the importance of accurate screening and diagnosis in guiding appropriate therapeutic interventions.
Persistent high-risk HPV (HRHPV) infection constitutes the principal etiological driver for advanced cervical lesions and carcinoma.21 HPV DNA testing provides methodological advantages, including high sensitivity, robust negative predictive value, and analytical reproducibility,22 with contemporary guidelines endorsing it as the primary cervical screening modality.9,11 Carcinogenic risk stratification classifies HPV into high-risk and low-risk categories, where HPV16/18 confers maximal high-grade lesion risk, whereas 12 additional HRHPV types demonstrate variable oncogenic potential. HRHPV-negative individuals exhibit minimal HSIL+ progression risk,23 with HPV 16/18 accounting for more than 70% of cervical carcinomas. Our virological stratification revealed a decrease in the prevalence of high-grade lesions: HPV 16/18-positive (58.2%), other HRHPV types (28.6%), and HPV-negative (17.6%). There was a significant difference between any two groups (P=0.001). Multivariate logistic regression analysis revealed that, compared with the low-risk and negative groups, the HPV 16 or 18 group had the highest risk of developing high-grade lesions or above (OR=8.061), followed by the other high-risk groups (OR=2.578), which is consistent with previous research results.24–26
TCT examination has several disadvantages, such as low sensitivity and poor reproducibility, and relies more on the subjective experience of cell pathologists.27 HPV DNA testing has high sensitivity and objective results but low specificity. Single HPV DNA testing can lead to excessive vaginal colposcopy referrals.28 The combination of TCT and HPV DNA testing can improve screening sensitivity and specificity and reduce false positive and missed diagnosis rates.29,30 In this study, the risk of developing high-grade cervical lesions in patients was predicted on the basis of the degree of cytological abnormalities detected by TCT and the HPV genotype. Even in the absence of abnormalities detected by TCT, patients with HPV16 or 18 still have a considerable risk of developing high-grade cervical lesions, and the greater the TCT abnormality is, the greater the risk of developing high-grade cervical lesions. These findings suggest that for patients positive for HPV16 or 18, consideration could be given to direct colposcopy referral and cervical pathological biopsy, regardless of TCT results, to potentially reduce missed diagnoses of high-grade cervical lesions. However, the clinical implementation of such a strategy requires validation in broader populations.23,26 In the other high-risk groups, patients with TCT results of ASCUS and LSIL or HSIL and above had positive predictive values of 36.0% and 76.9% for biopsy pathology of high-grade cervical lesions and above, respectively. Colposcopy referrals may also be warranted for these patients. For patients with TCT results of NILM, the positive predictive value is 17.6%, and close follow-up rather than immediate colposcopy might be a reasonable approach.23,31,32 In the low-risk and negative HPV groups, the positive predictive value of TCT results for patients with HSIL or above and biopsy pathology for high-grade cervical lesions or above was 50%. It would also be advisable to refer these patients for colposcopy. The TCT results for ASCUS and LSIL patients have a positive predictive value of 15.6%, and close follow-up is recommended.33 In addition to secondary prevention through screening, primary prevention via HPV vaccination represents a crucial strategy for eliminating cervical cancer. Despite public concerns regarding vaccine safety, a recent systematic review and meta-analysis by Ferrari et al34 encompassing over 8 million individuals revealed no significant association between HPV vaccination and the development of autoimmune diseases. This robust evidence further supports the favorable benefit‒risk profile of HPV vaccination programs. Importantly, the number of patients included in this study was relatively small, and more clinical studies and the inclusion of more patients are needed to further validate the above results.
Conclusion
Our findings demonstrate a strong association between the severity of cytological abnormalities on TCT and the risk of high-grade cervical lesions. The synergistic use of TCT and HPV DNA testing shows promise for optimizing cervical cancer screening protocols. On the basis of our data, a stratified referral strategy appears feasible: direct colposcopy referral is highly justified for patients with HPV 16/18 genotypes, whereas patients with other high-risk HPV types coupled with TCT results of ASCUS or above may also benefit from colposcopic evaluation. However, these findings, which were derived from a single-center cohort, necessitate further validation in larger, multicenter populations. Future research should focus on refining this strategy, potentially through the development of integrated risk-prediction models that incorporate additional variables such as age-specific risks and novel molecular biomarkers, to increase precision and cost-effectiveness before widespread clinical adoption can be recommended.
Data Sharing Statement
The datasets used and analyzed during the current study are available from the corresponding author upon reasonable request.
Ethics Approval and Consent to Participate
This study was approved by the Ethics Committee of Beijing Chaoyang Hospital, Capital Medical University (Approval No. 2024-Ke-570). Informed consent was obtained from all the participants. All methods were carried out in accordance with the Declaration of Helsinki.
Author Contributions
All authors made a significant contribution to the work reported, whether in the conception, study design, execution, acquisition of data, analysis and interpretation, or in all these areas; took part in drafting, revising or critically reviewing the article; gave final approval of the version to be published; agreed on the journal to which the article has been submitted; and agreed to be accountable for all aspects of the work.
Funding
The work was supported by the Clinical Research Special Fund of Wu Jieping Medical Foundation (Grant 320.6750.17023).
Disclosure
The authors declare that they have no conflicts of interest regarding this work.
References
1. Cohen PA, Jhingran A, Oaknin A, Denny L. Cervical cancer. Lancet. 2019;393(10167):169–182. doi:10.1016/S0140-6736(18)32470-X
2. Ferlay J, Colombet M, Soerjomataram I, et al. Estimating the global cancer incidence and mortality in 2018: GLOBOCAN sources and methods. Int J Cancer. 2019;144(8):1941–1953. doi:10.1002/ijc.31937
3. Bray F, Laversanne M, Sung H, et al. Global cancer statistics 2022: GLOBOCAN estimates of incidence and mortality worldwide for 36 cancers in 185 countries. CA Cancer J Clin. 2024;74(3):229–263. doi:10.3322/caac.21834
4. Sung H, Ferlay J, Siegel RL, et al. Global cancer statistics 2020: GLOBOCAN estimates of incidence and mortality worldwide for 36 cancers in 185 countries. CA Cancer J Clin. 2021;71(3):209–249. doi:10.3322/caac.21660
5. Lu Y, Li P, Luo G, et al. Cancer attributable to human papillomavirus infection in China: burden and trends. Cancer. 2020;126(16):3719–3732. doi:10.1002/cncr.32986
6. Wu S, Zhou J, Li M, Yang Y, Liu Y. Cervical cancer incidence, mortality, and burden in China. Cancer Med. 2024;13(4):e6994. doi:10.1002/cam4.6994
7. Okunade KS. Human papillomavirus and cervical cancer. J Obstet Gynecol. 2020;40(5):602–608. doi:10.1080/01443615.2019.1634030
8. Chinese Preventive Medicine Association Vaccine and Immunization Branch. Expert consensus on immunoprophylaxis of papillomavirus related diseases such as cervical cancer. Zhonghua Yu Fang Yi Xue Za Zhi. 2019;53(8):761–803. doi:10.3760/cma.j.issn.0253-9624.2019.08.001
9. World Health Organization. WHO guideline for screening and treatment of cervical precancer lesions for cervical cancer prevention, second edition. 2021. Available from: https://www.who.int/publications/i/item/9789240030824.
10. Jiang W, He Y, Chen W, et al. Real-world effectiveness of cytology and HPV-based screening strategies for cervical cancer in Chengdu, China. PLoS One. 2024;19(3):e0299651. doi:10.1371/journal.pone.0299651
11. Vaginal Endoscopy and Cervical Lesions Professional Committee of the Obstetrics and Gynecology Branch of the Chinese Medical Association. Expert consensus on the application of HPV DNA testing in the initial screening of cervical cancer in healthy individuals. Chin J Health Manag. 2022;16(10):665–672. doi:10.3760/cma.j.cn115624-20220810-00599
12. Sepodes B, Barata PC, Teixeira PF, Ramalho C, Felix A. Optimization of HPV-positive women triage with p16/Ki67 dual-staining cytology: a systematic review and meta-analysis. Arch Gynecol Obstet. 2024;302:111–115. doi:10.1007/s00404-024-07584-6
13. Dai W, Chen J, Li J, Kong Y. Immediate risk of cervical intraepithelial neoplasia and cancer in women with cytology-negative, high-risk HPV-positive screening results: a systematic review and meta-analysis. Am J Obstet Gynecol. 2024;231(2):e80. doi:10.1016/j.ajog.2024.04.039
14. Fontham ETH, Wolf AMD, Church TR, et al. Cervical cancer screening for individuals at average risk: 2020 guideline update from the American Cancer Society. CA Cancer J Clin. 2020;70(5):321–346. doi:10.3322/caac.21628
15. Perkins RB, Guido RS, Castle PE, et al. 2019 ASCCP risk-based management consensus guidelines for abnormal cervical cancer screening tests and cancer precursors. J Low Genit Tract Dis. 2020;24(2):102–131. doi:10.1097/LGT.0000000000000525
16. Hu X, Meng L, Gao Y, et al. A study on the current status of human papillomavirus infection and cervical cytological abnormalities in a female physical examination population in Shenzhen. Chin J Epidemiol. 2021;42(7):1205–1212. doi:10.3760/cmaj.cn112338-20210106-00007
17. Xia C, Qiao Y, Zhang Y, et al. WHO global strategy for eliminating cervical cancer and the challenges and response strategies faced by China. Chin Med J. 2020;100(44):3484–3488. doi:10.3760/cmaj.cn112137-20200909-02606
18. Ji W, Lou W, Hong Z, et al. Genomic amplification of HPV, h-TERC and c-MYC in liquid-based cytological specimens for screening of cervical intraepithelial neoplasia and cancer. Oncol Lett. 2019;17(2):2099–2106. doi:10.3892/ol.2018.9825
19. Luo H, Du H, Liu Z, et al. Risk assessment of cervical intraepithelial neoplasia grade 2 or 3 and above in patients with different subtypes of human papillomavirus infection and cytological abnormalities. Chin J Oncol. 2018;40(3):232–238. doi:10.3760/cma/j.issn.0253-3766.2018.03.015
20. Ferrari F, Bonetti E, Oliveri G, et al. Cold knife versus carbon dioxide for the treatment of preinvasive cervical lesion. Medicina. 2024;60(7):1056. doi:10.3390/medicina60071056
21. Tangjitgamol S, Kantathavorn N, Kittisiam T, et al. Prevalence and associated factors of abnormal cervical cytology and highrisk HPV DNA among Bangkok Metropolitan women. Asian Pac J Cancer Prev. 2016;17(7):3147–3153.
22. Zhao Y, Ma L, Ren W, et al. Analysis of cervical cancer examination project data for rural women in China from 2009 to 2018. Chin Med J. 2021;101(24):1863–1868. doi:10.3760/cmaj.cn112137-20210111-00075
23. The Tumor Prevention and Control Professional Committee of the Chinese Preventive Medicine Association, the Vaginal Endoscopy and Cervical Disease Professional Committee of the Obstetrics and Gynecology Branch of the Chinese Medical Association, and the Vaginal Endoscopy and Cervical Pathology Branch of the Chinese Eugenics Association. Chinese expert consensus on human papillomavirus nucleic acid testing for cervical cancer screening (2022). Chin Med J. 2023;103(16):1184–1195. doi:10.3760/cmaj.cn112137-20230117-00096
24. Falcaro M, Castañon A, Ndlela B, et al. The effects of the national HPV vaccination programme in england, uk, on cervical cancer and grade 3 cervical intraepithelial neoplasia incidence: a register-based observational study. Lancet. 2021;398(10316):2084–2092. doi:10.1016/S0140-6736(21)02178-4
25. Koc S, Yuksel D, Kinay T, Burkankulu D, Kayikcioglu F. Histological results of HPV genotyping from a colposcopy center. Arch Gynecol Obstet. 2023;308(1):193–200. doi:10.1007/s00404-022-06879-5
26. Ruan Y, Wei Y, Hou J, et al. Characteristics of cervical lesions in 1080 patients with abnormal TCT and HPV double screening colposcopy biopsy in Shihezi area. Chin J Physicians. 2022;24(1):29–34. doi:10.3760/cmaj.cn431274-2021006-00018
27. Zhang M, Bao H, Wang L, et al. Analysis of the current status and related factors of cervical cancer screening in China in 2015. Chin Med J. 2021;101(24):1869–1874. doi:10.3760/cmaj.cn112137-20210108-00054
28. Ruan Y, Li H, Liu M, et al. A retrospective analysis of human papillomavirus (HPV) prevalence and genotype distribution among 25,238 women in Shanghai, China revealed the limitations of current HPV-based screening and HPV vaccine. Cancer Epidemiol. 2023;84:102372. doi:10.1016/j.canep.2023.102372
29. Qi W, Li Q, Yang X, et al. Clinical analysis of screening and diagnosis of cervical lesions in 1337 postmenopausal women. Chin J Geriatr. 2023;42(7):804–809. doi:10.3760/cma/j.issn.0254-9026.2023.07.010
30. Husaiyin S, Jiao Z, Yimamu K, et al. ThinPrep cytology combined with HPV detection in the diagnosis of cervical lesions in 1622 patients. PLoS One. 2021;16(12):e0260915. doi:10.1371/journal.pone.0260915
31. Jia X, Jiang M, Li Y, et al. Value analysis of referral to colposcopy for high-risk cervical human papillomavirus positive women. Chin J Physicians. 2022;24(11):1620–1624. doi:10.3760/cmaj.cn431274-20220104-00005
32. Wang X, Wu S, Li Y. Risks for cervical abnormalities in women with non-16/18 high-risk human papillomavirus infections in south Shanghai, China. J Med Virol. 2021;93(11):6355–6361. doi:10.1002/jmv.27185
33. Li X, Xiang F, Zhao Y, et al. Detection of cervical high-grade squamous intraepithelial lesions and assessing diagnostic performance of colposcopy among women with oncogenic HPV. BMC Womens Health. 2023;23(1):411. doi:10.1186/s12905-023-02538-2
34. Ferrari FA, Ciminello E, Ceccaroni M, et al. No increased risk of autoimmune diseases following HPV vaccination: a systematic review and meta-analysis. Vaccines. 2025;13(4):391. doi:10.3390/vaccines13040391
 © 2025 The Author(s). This work is published and licensed by Dove Medical Press Limited. The
full terms of this license are available at https://www.dovepress.com/terms
and incorporate the Creative Commons Attribution
- Non Commercial (unported, 4.0) License.
By accessing the work you hereby accept the Terms. Non-commercial uses of the work are permitted
without any further permission from Dove Medical Press Limited, provided the work is properly
attributed. For permission for commercial use of this work, please see paragraphs 4.2 and 5 of our Terms.
© 2025 The Author(s). This work is published and licensed by Dove Medical Press Limited. The
full terms of this license are available at https://www.dovepress.com/terms
and incorporate the Creative Commons Attribution
- Non Commercial (unported, 4.0) License.
By accessing the work you hereby accept the Terms. Non-commercial uses of the work are permitted
without any further permission from Dove Medical Press Limited, provided the work is properly
attributed. For permission for commercial use of this work, please see paragraphs 4.2 and 5 of our Terms.