Back to Journals » Clinical Ophthalmology » Volume 19
Scoping Review of the Role of Accommodation and Binocular Coordination in Myopia Onset and Progression
Authors Evans BJW ![]() , Shah R, Vlasak N
, Shah R, Vlasak N ![]()
Received 13 September 2025
Accepted for publication 27 November 2025
Published 15 December 2025 Volume 2025:19 Pages 4665—4688
DOI https://doi.org/10.2147/OPTH.S567456
Checked for plagiarism Yes
Review by Single anonymous peer review
Peer reviewer comments 3
Editor who approved publication: Dr Scott Fraser
Bruce John William Evans,1 Rakhee Shah,1 Natalia Vlasak2
1Optometry and Visual Sciences, City St George’s, University of London, London, EC1V 0HB, UK; 2HOYA Vision Care, Amsterdam, 1043 NX, the Netherlands
Correspondence: Bruce John William Evans, Optometry and Visual Sciences, City St George’s, University of London, London, EC1V 0HB, UK, Email [email protected]
Background: The predominant theory, underlying most optical myopia control interventions, is that relative peripheral hyperopic defocus (RPHD) is a cause of myopia progression. However, interventions that reduce RPHD only slow myopia progression on average by ~50%, so other factors are likely to be involved.
Objective: To explore the literature on accommodation and binocular coordination as possible factors in myopia development and progression.
Methods: PubMed was searched for relevant keywords in September 2025. Non-human and non-English reports were excluded.
Results: (1) Concerning myopia onset, the CLEERE study found changes in the interaction between accommodation and convergence (increasing AC/A ratio) from four years before myopia onset. This is thought to indicate compromised accommodation, supported by reduced positive relative accommodation before myopia onset in other longitudinal studies. (2) Regarding myopia progression, the magnitude of accommodative lag is not strongly correlated with rate of myopia progression. The validity of clinical measurements of accommodative lag has been questioned. Tests of eye alignment during near vision show a more convergent posture (esophoria) in some myopes around the time of myopia onset, probably secondary to increased AC/A ratio. If compromised accommodation and/or near esophoria are relevant to myopia progression, prescribing a near addition should be helpful. However, myopia control trials of bifocal and progressive addition lens spectacles show poor efficacy. Despite early indications of greater efficacy in cases with higher accommodative lag and/or near esophoria, poor treatment effects in this sub-group were subsequently found. Nonetheless, some individual cases with symptomatic convergence excess esophoria are likely to benefit from bifocal spectacles for symptomatic relief.
Conclusion: Although accommodative dysfunction seems likely to play some role in myopia onset, accommodative and binocular factors are unlikely to be major causal factors in myopia progression. An additive risk factor risk-resilience model is presented and suggestions are made for further research.
Plain Language Summary: Myopia (short-sightedness) has become much more common in recent years, and is predicted to affect half the world’s population by 2050. Treatments are available that slow the progression of myopia by approximately 50% on average, including special spectacle lenses, contact lenses, and eye drops. To better understand why these approaches are not 100% effective we need to know more about the various factors that may play a causal role in myopia. The purpose of this review is to assess the evidence for two such factors: the ability to focus close to (ocular accommodation) and to use the two eyes as a team (binocular coordination). The review reveals research that has found abnormalities in ocular accommodation several years before a child develops myopia. However, there is less evidence that myopia or binocular coordination play a role during myopia progression. A risk-resilience model of myopia is presented. This highlights various factors that may play a causal role in myopia and others that may protect some children against developing myopia.
Keywords: myopia onset, myopia progression, accommodation, binocular vision, AC/A ratio, accommodative lag
Introduction
Background
In recent years, myopia has emerged as a serious public health issue, with a major impact on eye health and quality of life.1 Approximately one third of the world population are myopic and the prevalence is estimated to reach nearly 50% by 2050, when approximately 1 billion people are likely to have high myopia.1 Myopia, especially high myopia, increases the risk of sight loss from ocular pathology2 and therefore there is considerable interest in myopia control interventions. As advocated by the International Myopia Institute, in this manuscript myopia control refers to interventions to slow myopia progression and/or associated axial elongation and myopia management describes the overall care that clinicians provide for myopic patients, including prevention and correction.3
The most commonly used contemporary myopia control interventions are atropine eye drops and optical interventions that provide, via a variety of approaches, additional plus power in the periphery of the lens.2 These optical interventions are designed to correct relative peripheral hyperopic defocus (RPHD), which is believed to be a factor in myopia aetiology.4 A reduction in contrast in the peripheral image is another possible mechanism.5,6 Optical interventions that correct RPHD are effective, typically slowing myopia progression on average by approximately 50%.7 Within the data from clinical trials there is considerable variation in individual responses.8–10 Therefore, other factors are likely to be involved in the aetiology of myopia and better understanding of these is essential for developing more comprehensive approaches to myopia control. For many years, ocular accommodation11 and binocular coordination12 have been suggested as other factors that may be involved in myopia aetiology.
Accommodation
Ocular accommodation can be assessed in various ways. The maximum accommodation that can be exerted is the amplitude of accommodation, typically measured using a target that approaches the eye or by introducing negative lenses until the patient reports blur.13 When negative lenses are used, measurements of the amplitude of accommodation must be carried out monocularly because if the patient fixates the target binocularly then the link between accommodation and convergence confounds the measurement.14 If negative lenses are added whilst the patient fixates on a target binocularly until blur occurs, the amount of accommodation that can be exerted is much less than the total amplitude and is called the positive relative accommodation (PRA). If positive lenses are introduced to relax accommodation under binocular viewing conditions, the maximum lens power that can be added indicates the negative relative accommodation (NRA).
Accommodative facility describes the ability to rapidly change accommodation. The accuracy of accommodation is indicated by accommodative lag, which is typically measured clinically by retinoscopy or in the laboratory with instruments that record the accommodative response.
If accommodative lag genuinely occurs (see Discussion), since the retinal image falls behind the retina hyperopic defocus will occur. The feedback loop hypothesis of myopia posits that in the presence of hyperopic defocus the eyeball grows, as if trying to move the retina towards the focal point of the eye, causing myopia.15 If accommodative lag persists, then the eye continues to elongate. According to this hypothesis, higher levels of accommodative lag cause increased hyperopic defocus leading to more rapid myopia progression.16 The evidence for this accommodative lag induced hyperopic defocus hypothesis has been described as equivocal at best, perhaps due to difficulties in the precise measurement of accommodative lag,17 as discussed later.
An alternative hypothesis relates to the finding that the act of accommodation results in transient increases in axial length.18,19 Schmid and Strang speculated that these transient changes might translate to permanent axial length increases, causing myopia progression.20
Cheng et al described the hypothesis that accommodative stress induces myopia progression and that relaxing accommodation would therefore inhibit axial elongation.17 These authors obtained data rejecting this hypothesis.
Another hypothesis attempts to link accommodation and intraocular pressure (IOP). Yan et al found that, compared with emmetropes, progressing myopes had a significant increase in intraocular pressure but only during ocular accommodation.21 They speculated that this may be related to myopia progression. A recent Mendelian randomisation study did not find a direct causal link between IOP and the development of myopia,22 but there is some evidence of an increase in IOP with accommodation in progressing myopes.23
In a theoretical paper, Hargrave argued that the extraocular muscles play a role in ocular accommodation and in the aetiology of myopia.24 This opinion has received very limited support25 and does not seem to have received further consideration by myopia researchers.
Antimuscarinic agents (eg, atropine) slow myopia progression. Initially, the mechanism was thought to be by eliminating accommodation, but this was disproven.26 The precise mechanism is still unknown,27 although the recent finding of reduced accommodation induced biomechanical forces during atropine use has been suggested as a possible mechanism, together with increased near vision viewing distance.28 A review by Horn et al concluded that multiple mechanisms are likely to be involved.29
Excessive near vision, particularly at close viewing distances, can be a trigger for myopia.30 Queiros et al investigated whether the effect of accommodation on the pattern of peripheral refraction is atypical in myopia.31 In young adult myopes, they found similar changes in peripheral refraction for both myopes and emmetropes with accommodation, even to very close near targets. In contrast, like other authors they found that for their most distant target (2 m), in the temporal retinal periphery there is hyperopic defocus in myopes (when wearing spectacle correction) compared with myopic defocus in emmetropes. The findings of this study support the RPHD theory but do not support theories directly implicating accommodation in myopia aetiology. A recent review argued that colour vision mediates hyperopic defocus signals and accommodative lags to facilitate myopia, but noted the need for further research.32
Nowadays, hypotheses implicating accommodation in myopia aetiology are a minority view and the RPHD hypothesis appears to be predominant. Nonetheless, there is a growing acceptance that the RPHD hypothesis cannot fully explain myopia onset and progression. Myopia aetiology is likely to be multifactorial so that, in addition to genetic factors, there are probably several mechanisms contributing to the development and progression of myopia, considered further in the Discussion.33 The first aim of the present review is to re-evaluate the evidence concerning the possible role of accommodation in myopia development and progression.
Binocular Coordination (Binocular Vision)
The term binocular coordination is used here to describe the ability of the eyes to work together as a coordinated team. In normal binocular coordination, the eyes are directed at the object of regard. For about two percent of the population the eyes are misaligned (strabismus).31 Most people with normal binocular alignment (no strabismus) have, during near vision, a latent tendency for the eyes to turn outwards (exophoria). Less commonly, the opposite is observed, an esophoria.
Good near vision requires both accommodation and convergence and these functions are linked.14 It is possible that in some individuals the visual system over-stimulates accommodation in an attempt to overcome a high accommodative lag, and excessive innervation to the accommodative system triggers excessive convergence, resulting in esophoria. Conversely, a patient with an esophoria that is causing symptoms may relax their accommodation to cause an associated reduction in convergence to reduce the esophoria. In this scenario, the esophoria may lead to excessive accommodative lag.14 The relationship between accommodation and convergence is quantified by the accommodative-convergence to accommodation (AC/A) ratio. This is the amount of convergence that is induced by each dioptre of accommodation. The second aim of this review is to evaluate the evidence concerning the possible role of binocular coordination in myopia development and progression.
A scoping review is considered appropriate to address the aims for the following reasons. The review seeks to determine the scope of a broad body of literature, including different types of evidence, to identify and analyse knowledge gaps.34 Rather than addressing a specific intervention the review seeks to explore a broad range of literature.35 For example, the review includes clinical trials, observational studies, laboratory studies, and theoretical papers.
Methods
The review protocol was not pre-published. A PubMed search was carried out for the terms in Table 1, first on 26 October 2024 and last updated on 7 September 2025. After duplicates were removed, all publications were screened for relevance by title and abstract. Additional references were identified from article reference lists and the authors’ bibliographies. Full reports were studied, and selection criteria applied (Table 1). A supplementary search was carried out for papers with “heterophoria” in the title and “myopia” in any field.
 |
Table 1 Search Terms Used in Literature Search |
In view of the broad research questions and wide range of literature considered (eg, clinical trials, observational studies, laboratory studies, theoretical papers) a standardised data charting form was not appropriate. Instead, all manuscripts were reviewed for relevant information. The key tools used in handling and synthesizing results were Endnote and Microsoft Excel.
Non-human studies were excluded because reviews of animal work36 reveal differences between species in the relationship between accommodation, binocular coordination, and myopia.20,36
Results
Literature Search
The output of the literature search is summarised in Figure 1. Most research has studied early (juvenile; aged under 18 years)37 onset myopia rather than late (adult) onset and this review refers to early onset myopia unless otherwise stated. The literature was divided into that relevant to myopia onset and to myopia progression.
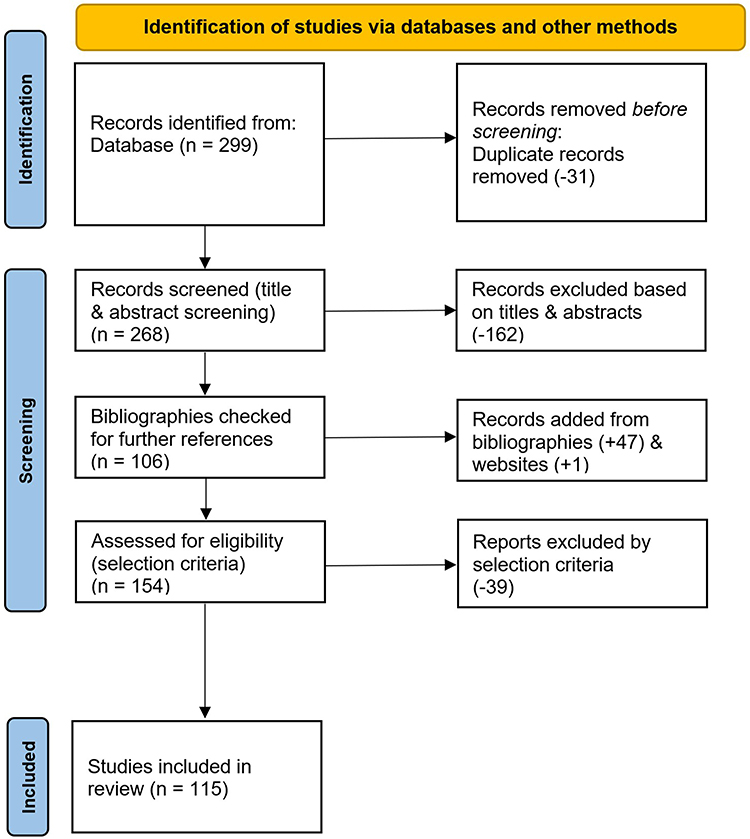 |
Figure 1 PRISMA flowchart of paper selection. |
Myopia Onset
Accommodation
A summary paper by Schmid and Strang20 reports reasonable agreement that higher lags of accommodation occur in some groups of progressing myopes,38,39 especially with challenging stimulus conditions, but consider that it is less clear whether higher lags of accommodation occur in emmetropes who go on to develop myopia. In adults, Rosenfield et al found that emmetropes who went on to develop myopia had significantly lower accommodative lag than young adults who remained emmetropic or were myopic already.40 These authors stressed that they measured accommodative function under natural viewing conditions (ie, the usual proximal, convergent, and blur-driven cues to accommodation were present) and that this may account for opposite results in other studies.
To determine the optometric functions involved in the development of myopia, the strongest research design is a longitudinal study, where large groups of non-myopic children are tested and followed over time to determine, when some children become myopic, which optometric parameters best predict the development of myopia. An early study that took this approach, Goss, was a retrospective review of clinical records from four optometry practices.41 PRA was significantly lower in the children who went on to become myopic than in those who remained emmetropic.
Goss and Jackson reported a longitudinal study of a cohort of initially emmetropic children who were examined for three years.42 Lag and amplitude were not reported, but the mean PRA was significantly lower in the group who became myopic. Measurements were taken with patients viewing through their refractive corrections, so this finding is likely to be accurate.
A key longitudinal study is the Collaborative Longitudinal Evaluation of Ethnicity and Refractive Error (CLEERE) study, which started as the Orinda Longitudinal Study of Myopia. This tested a large population of children from age 6 years. The first paper that reported on accommodation, Mutti et al, found that increased accommodative lag occurred in children only after the onset of myopia.43 It was concluded that increased hyperopic defocus from accommodative lag may be a consequence rather than a cause of myopia.
A later paper on the CLEERE study by Zadnik et al evaluated 13 candidate risk factors for their ability to predict the onset of myopia.44 In multivariate models, eight factors retained an association with the risk of myopia onset: spherical equivalent refractive error at baseline, parental myopia, axial length, corneal power, crystalline lens power, AC/A ratio, horizontal/vertical astigmatism magnitude, and reported near vision activity. Accommodative lag was not found to be a significant predictor of myopia development, even in univariate models.
Mutti et al reported further analysis of the CLEERE study, concentrating on the AC/A ratio in 698 children who went on to become myopic compared with 430 children who remained emmetropic.45 The mean response AC/A ratio was not significantly different between the two groups five years before myopia onset, but four years before onset it was significantly higher in those who subsequently became myopic (Figure 2). The mean AC/A ratio then increased monotonically in children who became myopic until reaching a plateau at myopia onset of ~7 PD/D compared to ~4 PD/D for children who remained emmetropic (p < 0.01). A higher AC/A ratio was associated with greater accommodative lag but not with the rate of myopia progression regardless of the level of near work. The authors conclude that an increasing AC/A ratio appears to play a role in the process of becoming myopic, although they note that nothing predicts myopia better than a child’s current low hyperopic or emmetropic refractive error. The authors hypothesise that the increase in AC/A ratio results from compromised accommodation requiring an increased neural effort per dioptre of accommodation. Interestingly, RPHD only started to differ significantly between the groups two years before myopia onset in contrast to four years for the AC/A ratio.
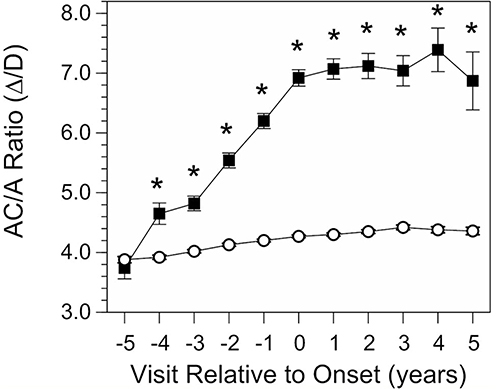 |
Figure 2 The response AC/A ratio as a function of annual visit relative to the onset of myopia (−5 years before to +5 years after onset, which is designated as visit 0). Data are from children who became myopic (solid squares) and from emmetrope model values (clear circles). All error bars are ± standard error of the mean. Error bars for the emmetrope model values are smaller than the symbols. *Significant differences between groups (p < 0.01). Reproduced from Mutti et al45 under Creative Commons Licence. |
The WEPrOM longitudinal study in China found that the predictors of myopia included lower PRA, less hyperopic refractive error, longer axial length, and female sex.46 The first two of these were the top single predictors. The authors suggest that reduced accommodative functions may be associated with difficulty in increasing blur-driven accommodation in pre-myopes. A later study by this group found that low PRA at baseline (mean age 7.8y) had a moderate predictor power for myopia onset at mean age 11.7 years (area under the receiver-operator curve, 0.59). The authors considered that reduced ability to accommodate at close distances for prolonged periods of near work may be linked to myopia onset.
The third major prospective longitudinal study is the Lhasa Childhood Eye Study.47 This evaluated the habitual accommodative tone (HAT), defined as the difference between non-cycloplegic and cycloplegic automated refraction. The authors argue that HAT describes long-term, age-related changes of habitual accommodative tone. For hyperopic children, the HAT was significantly associated with the incidence of myopia over two years indicating that lower HAT was potentially associated with myopia development. The authors noted that further research is required to determine whether the reduction in HAT is a consequence of the eye tending toward myopia or the cause of it.
Sun et al also studied the difference between non-cycloplegic and cycloplegic spherical equivalent refraction (SER).48 These authors concentrated on cases for whom non-cycloplegic SER was −0.50D or worse and cycloplegic SER was better than −0.50D, which was considered to represent pseudo-myopia or over-accommodation (cyclospasm).14 A total of 2328 children were followed for six months. After adjusting for multiple myopia risk factors, including baseline cycloplegic SER, near work and time outdoors, pseudo-myopia was found to be an independent risk factor for myopia onset. Pseudo-myopic children with a higher amplitude of accommodation had an increased risk of myopia development. A limitation of this study48 is that the pseudo-myopia and over-accommodation could in some cases have been an artefact from testing with autorefractors (instrument myopia). This view is supported by normal uncorrected visual acuity in over 80% of the pseudo-myopia group.
Binocular Coordination
The study described above by Goss,41 found that the mean near heterophoria was low esophoria in children who went on to become myopic, but was low exophoria in those who remained emmetropic.
The longitudinal study by Goss and Jackson found that the near heterophoria was more convergent (more eso/less exo) in the group who became myopic, who demonstrated an eso-shift (a decrease in exophoria or increase in esophoria) over time.49 There were also proportionately more cases of high exophoria in the group that became myopic, causing the authors to comment that a near heterophoria that is not close to orthophoria appears to be a risk factor for youth onset myopia. This study also found an eso-shift in the midpoint of the near fusional reserve range (zone of clear binocular single vision).42
In the CLEERE study (described above), the proportion of children with near esophoria increased among those who became myopic compared to children who remained emmetropic.45 This was consistent with the main finding of the study, increasing AC/A ratio during a period of stable accommodative lag for several years before the onset of myopia. Multivariate analysis indicated that the near esophoria may be driven more by the AC/A ratio than the level of accommodative lag.
Myopia Progression
Accommodation
Accommodative Function in Individuals with Myopia
Table 2 summarises research on accommodative function in individuals with myopia. Particularly instructive studies are elaborated below the table.
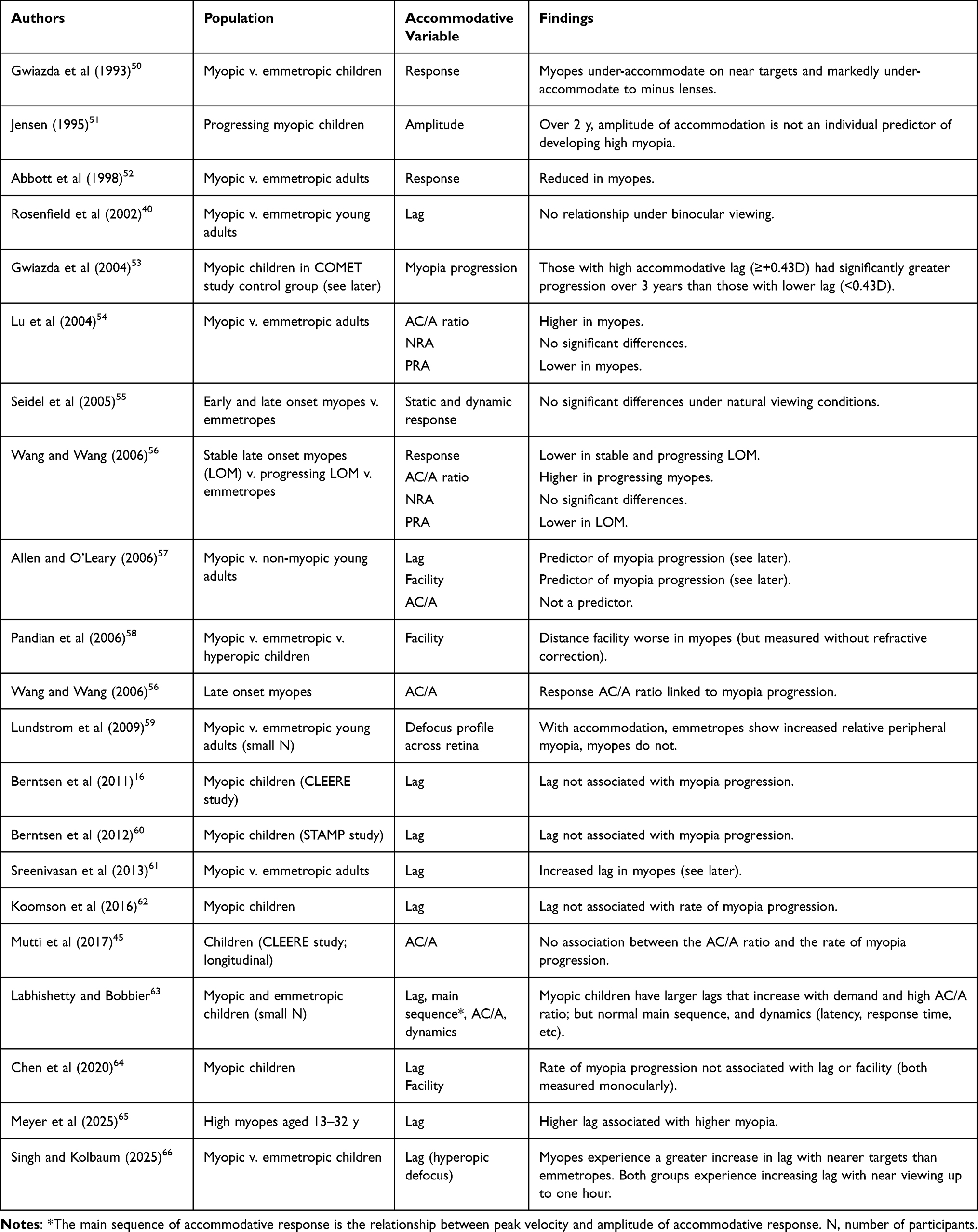 |
Table 2 Summary of Research Evaluating Relationship Between Accommodative Function and Myopia |
Gwiazda et al measured accommodative responses with an autorefractor in myopic and emmetropic children.50 Myopic children accommodated significantly less (increased lag) than emmetropic children for real targets at near distance, and much less for blur induced by minus lenses. However, with positive lenses, requiring relaxation of accommodation, there was no significant difference between the groups. The researchers concluded that blur is not an effective stimulus for accommodation in myopic children.
In young adults with progressing myopia, Rosenfield et al found no evidence of a relationship between accommodative lag and myopia progression.40 These authors stressed that they measured accommodative function under natural viewing conditions, with the usual proximal, convergent, and blur-driven cues to accommodation all present.
Seidel et al noted that previous research had found progressing myopia to be associated with abnormal accommodative dynamics, including accommodative microfluctuations.55 They found it surprising that myopes do not report symptoms from these problems and noted that previous research had been carried out under artificial experimental conditions of viewing targets monocularly and not in free-space. Like Rosenfield et al,67 Seidel et al investigated accommodation under natural conditions and found no significant differences in the accuracy of static and dynamic accommodation responses among emmetropes, early onset myopes, and late onset myopes.
Allen and O’Leary found accommodative lag and accommodative facility (but not AC/A ratio) to be predictors of myopia progression.57 Allen and O’Leary noted that both these factors affect retinal defocus. However, there was considerable scatter in the relationships.16
Sreenivasan et al investigated the retinal image quality during accommodation in adult myopic eyes.61 These authors used binocular viewing, creating the more natural viewing conditions recommended by Rosenfield et al.40 Sreenivasan et al found increased accommodative lag in myopes compared with emmetropes, but noted that acuity was not measurably worse in myopes. The authors proposed three explanations. First, they found higher positive spherical aberration in myopes which is likely to provide increased depth of focus. This could reduce sensitivity to retinal image blur, allowing the accommodative system to exert the minimum necessary accommodation to bring the target into focus. Second, other researchers have found increased adaptation to blur in myopes, probably from habitual adaptation to uncorrected blur. A third explanation relates to larger than usual accommodative micro-fluctuations in myopes. There may be a burst of accommodative effort just long enough to clear the image even in the presence of significant accommodative lag.
Schmid and Strang20 reviewed research on differences in accommodative response between myopes and emmetropes since their 1998 study.52 Like Rosenfield et al,40 they note that in general, studies have shown higher accommodative lags in myopic children, but have used artificial conditions of viewing monocularly through an optical lens system.
Labhishetty and Bobbier compared six myopic with six emmetropic children, aged 8–13 years, under monocular viewing conditions.63 Myopic children typically exhibited significantly larger response lags that increase with demand but their main sequence relationship was similar to emmetropes. Other dynamic characteristics such as latency and response time were not different between the two refractive groups for both accommodation and relaxation of accommodation. The authors considered models of accommodative function, proposing that the reduced blur sensitivity seen in myopic children is compensated by a motor recalibration wherein the gain of the accommodative convergence crosslink is increased. They noted that a larger gain of the crosslink would be necessary to maintain sufficient levels of vergence given the reduced accommodation.
A study by Labhishetty et al in 2021 is not specifically about myopia but raises important questions about the consensus view, that accommodative errors (lags and leads) are a by-product of the accommodative system changing state only by as much as is required to bring an image into acceptable focus.68 These authors note that this view is difficult to reconcile with the decline in visual acuity with small amounts of defocus and the smallest change in stimulus distance that drives accommodative response. They simultaneously measured accommodation (objectively) and visual acuity (subjectively) at a range of optical distances. A limitation of the work is that readings were obtained monocularly and without proximal cues. Participants were six pre-presbyopic adults whose refractive errors were not described, but were corrected during the experiments.
The subjective measure found much smaller errors than objective measurements. Specifically, a wavefront sensor indicated median lags of ∼1D for stimuli at 1–6D and the autorefractor results found lags of ∼0.5–1.5D. In contrast, subjective measurements (the distances at which acuity was maximized) indicate little to no accommodative lag except at the nearest distances of 5D and 6D, which were at the limits of accommodative amplitude of the participants.68 The authors posit that some or most of the difference they observed is due to a greater contribution of spherical aberration to the objective measures, with negative spherical aberration likely to cause an apparent lag. Noting that young adult myopes exhibit higher negative spherical aberration than emmetropes,69 Labhishetty et al’s findings raise the possibility that the increased accommodative lag that many authors have associated with myopia may be an artefact. If further research validates these findings, they bring into doubt the utility of measuring lag of accommodation routinely in myopia management, which in one survey was reported by over 40% of clinicians.70
Near work-induced transient myopia (NITM) is a small and transient myopic shift induced by a period of sustained near work.71 This can be conceptualised as a slowness of accommodation to relax after near vision. It has been proposed that NITM may be a near work factor that contributes to permanent myopia. NITM is larger in myopes than in emmetropes,72 and is manifest during the progressive phase of myopia development.73 However, the three-year report from the Beijing Myopia Progression Study found that NITM was only significantly associated with the progression of a myopic refractive shift among hyperopes, not myopes.71
In a theoretical paper that considers a large body of literature, Liu et al noted that there is growing evidence that chromatic sensitivity is preserved partially in the peripheral retina.74 These authors considered that longitudinal chromatic aberration plays a key role in the feedback loop to ensure accurate focussing by indicating the necessary direction and magnitude of the accommodative response. Liu et al argue that the ratio of long- to medium-wavelength (L-M) cone contrast produces a pronounced direction signal for accommodation.
Myopia Control Trials Designed to Influence Accommodation
If prolonged accommodation during near vision is a causal factor in myopia progression, then multifocal (bifocal or progressive addition lens) spectacle lenses (MFSL) should slow myopia progression because the near addition reduces the need for accommodation.52 Also, if increased accommodative lag contributes to myopia progression, then MFSL should slow progression by reducing accommodative lag.52 A recently updated Cochrane network meta-analysis shows that MFSL have a negligible treatment effect at slowing myopia progression and axial elongation (Figure 3).
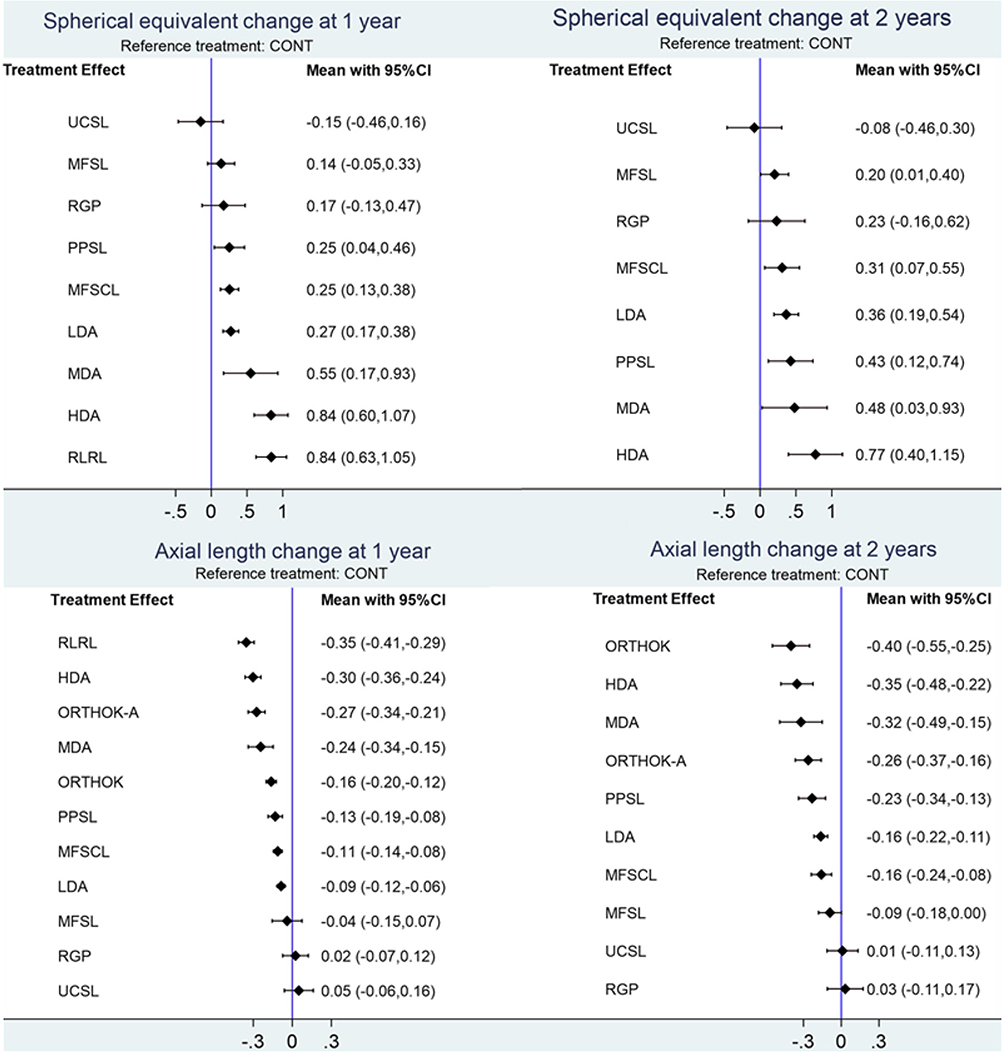 |
Figure 3 Estimates of effect from network meta-analyses for all treatments versus control for progression of myopia (based on SER and axial length) at 1 and 2 years. Reproduced with permission from Lawrenson et al Interventions for myopia control in children: a living systematic review and network meta-analysis for Cochrane Collaboration.75 Abbreviations: CONT, control; RLRL, repeated low intensity red light; HDA, high-dose atropine; LDA, low-dose atropine; MDA, medium-dose atropine; MFSCL, multifocal soft contact lenses; MFSL, multifocal spectacle lenses (bifocal and progressive addition lenses); ORTHOK, orthokeratology; ORTHOK-A, combined orthokeratology and atropine; PPSL, peripheral plus spectacle lenses; RGP, rigid gas-permeable contact lenses; UCSL, under-corrected spectacle lenses. |
It should be noted that, by introducing extra plus power in a portion of the lens, MFSL will have an effect at creating myopia defocus and/or reducing hyperopic defocus. The hypothesis that this mechanism might account for some of the myopia control effect of MFSL is supported by the observation that the studies demonstrating greatest treatment effect tend to be those using larger near vision segments.76,77
In the COMET study of MFSL, the experimental group (who wore progressive addition lens, PAL, spectacles) exhibited slower progression than the control group (who wore single vision spectacles) but the difference between the groups only reached statistical significance in the 114 participants with high accommodative lag.53 Therefore, the COMET2 study specifically targeted myopic children with high accommodative lag and near esophoria, who were randomly assigned to single vision lens (SVL) spectacles or PAL with a +3.00 addition.78 There was significantly slower myopia progression in the PAL group, but the treatment effect (0.28D over three years) was not clinically significant. Interestingly, the treatment effect increased over the three years, which is different to other myopia control interventions.79
Berntsen et al reported on the Study of Theories about Myopia Progression (STAMP) trial. This was a two-year trial to investigate whether (a) high accommodative lag during near work produces hyperopic retinal blur that accelerates axial growth or (b) mechanical tension created by the crystalline lens or ciliary body restricts equatorial ocular expansion, thereby causing accelerated axial elongation.60 In the latter theory, high accommodative lag is a consequence rather than a cause of myopia. These hypotheses were investigated by studying 85 myopic children with high accommodative lag, who wore either PALs or control SVL for one year. After one year, there was significantly slower myopia progression (by 0.18D) in the group wearing PALs. All participants then wore SVLs for a further year, with similar myopia progression in the two groups (no rebound effect in the PAL group). The absence of a rebound effect was interpreted as supporting theories relating to hyperopic defocus. However, the lack of significant correlation between accommodative lag and myopia progression was considered to be inconsistent with the benefit from PAL being due to decreased foveal blur during near work.
Multifocal soft contact lenses (MFSCL), like MFSL, have the potential to reduce the need for accommodation during near vision and to reduce accommodative lag. A key difference between MFSL and MFSCL is that with MFSL the eyes rotate to look through the appropriate segment of the lens for distance or near vision. Therefore, MFSCL may be less effective at reducing the need for accommodation, may have an unpredictable effect on accommodative lag, but may be more effective at reducing peripheral hyperopic defocus or increasing peripheral myopic defocus.
For example, in the BLINK study Walline et al investigated the effects of MFSCL at slowing myopia.80 The centre-distance lenses they used were selected for their hypothesised effect at correcting RPHD, rather than through any effect on accommodation. However, most peripheral defocus metrics and defocus at most peripheral retinal loci accounted for little to no variance in the treatment effect of the +2.50D addition lens.81 Thus, the mechanism of the treatment effect does not appear to be peripheral defocus.81 This raises the possibility of an accommodative mechanism. Indeed, after three years the participants who had worn MFSCL had reduced accommodative response (when not wearing the lenses), suggesting some effect on accommodation (see later).82
Allen et al carried out a two-year study of myopic adolescents comparing two interventions to improve accommodative function.83 These were a contact lens designed to reduce accommodative lag by controlling spherical aberration and vision training designed to improve accommodative dynamics. The treatments had no statistically significant effect, in isolation or combined. This may have resulted from a low myopia progression rate (−0.33D over two years), attributed to the participants’ age (mean 16 years). Also, one third of the participants dropped out of the trial.
Zhu et al (only abstract available in English) measured the amplitude of accommodation in 49 children fitted with OrthoK.84 The myopia control effect was greatest in children with a low amplitude of accommodation, who demonstrated a clinically significant increase in accommodation after treatment.
Lv et al reported reduced myopia progression and axial elongation and improved accommodative facility in a group of children receiving binocular vision perceptual training.85 However, this finding could be attributable to methodological limitations: participants were not randomly allocated to treatment groups, follow-up was three months, accommodative facility was only measured in the group receiving vision therapy, and the intention-to-treat principle86 was not followed.
Binocular Coordination
Binocular Coordination in Patients with Myopia
In the 1980s, Rosenfield and Gilmartin noted that early onset myopia (before age 15 years) is associated with a higher AC/A ratio than late onset myopia or emmetropia.87
In a longitudinal study of Swedish myopic children described above, Jensen studied the optometric variables that predicted, over two years, which children would develop high myopia.51 Neither the type of heterophoria, or near point of convergence were individual predictors of which cases would develop high myopia. A limitation is that heterophoria was only considered as a categorical variable (orthophoria, exophoria, or esophoria).
Allen et al found that the CA/C ratio did not contribute significantly to myopia progression.57 Ma et al reported a retrospective analysis of myopia progression patients wearing DIMS, dividing participants by the type of heterophoria. Those with convergence excess progressed most rapidly and those with divergence excess progressed least rapidly.88 Since there was no control group, it is unknown whether this was related to DIMS or whether a similar differentiation would have been present in myopes wearing single vision spectacle lenses.
Table 3 summarises studies investigating the type of heterophoria in children with myopia compared to emmetropia. These data are cross-sectional and therefore provide a different perspective to the information described above, of longitudinal studies that indicate an eso-drift at myopia onset.
 |
Table 3 Summary of Studies Evaluating Relationship Between Heterophoria and Myopia |
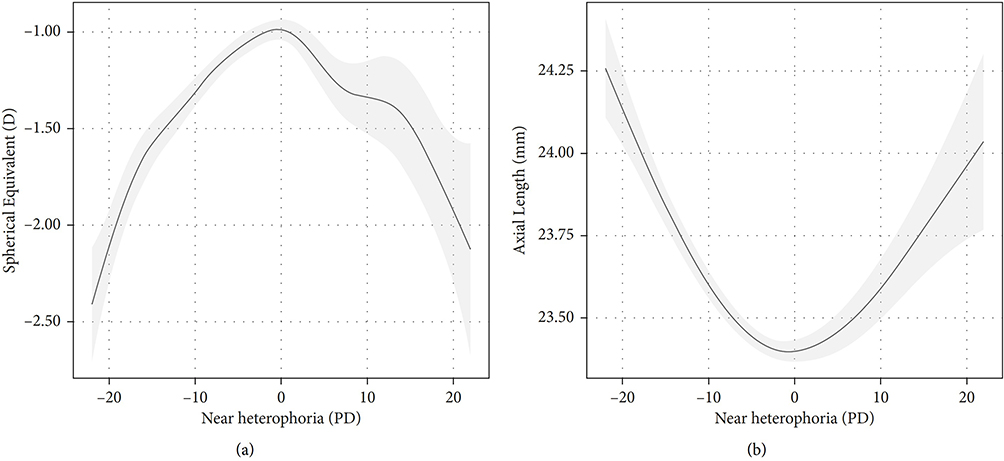 |
Figure 4 Relationship between heterophoria and (a) myopia and (b) axial length derived from a generalised additive model. Heterophoria is in prism dioptres (PD), and negative values are exophoria. The grey areas represent the 95% confidence intervals. Reproduced, under Creative Commons Licence, from Chen et al.93 |
Chen et al assessed near heterophoria in 11,000 Chinese children aged 6 to 13 years.93 Exophoria was most common (65%). Interestingly, children with larger near heterophoria, regardless of whether exophoria or esophoria, tended to exhibit a higher degree of myopia and longer axial length than those with lower levels of near heterophoria (Figure 4). Children who had spectacles were assessed when wearing these, and others were assessed without any refractive correction. Therefore, the results may have been confounded by uncorrected and under-corrected refractive errors. However, the findings in Figure 4 are so marked that they seem unlikely to be explained by this limitation. The study highlights that the relationship between heterophoria and myopia is non-linear. Most of the studies reviewed in this section have evaluated the number of individuals with exophoria or esophoria and Figure 4 reveals such analyses would obscure the real relationship between myopia and heterophoria. Similarly, measures of central tendency of heterophoria may be confounded by compensating errors (see Discussion).
Owing to the link between accommodation and convergence, it has been suggested that MFSL or MFSCL may slow myopia progression by reducing accommodative demand, which in turn reduces the stimulus to converge, reducing esophoria.
When Goss and Grosvenor95 reanalysed a study of bifocal spectacles to restrict the sample to those with near esophoria, they obtained a treatment effect close to 40%, better than the treatment effect in non-esophoric populations. Similarly, with MFSCL an unusually strong treatment effect at slowing myopia progression was obtained by Aller et al,96 who corrected participants with a near esophoria with MFSCL having a near addition individually selected to neutralise the near eso-fixation disparity (see later).
In the COMET study (2004), both high accommodative lag and near esophoria were associated with increased myopia progression when wearing SVL and with the most marked benefit from PAL.53 However, the correlation between accommodative lag and near heterophoria was low (r = −0.16), so that it is unlikely that the mechanism of this finding is that esophoric children were relaxing accommodation to reduce accommodative convergence.14
The COMET2 study was specifically designed to investigate the effect of PAL spectacles on the progression of myopia in children with low baseline myopia, high accommodative lag, and near esophoria.78 The myopia control effect was only 24%, which although statistically significant was not considered to be clinically significant. Two other studies that tested the effect of MFSL on myopia progression in children with near esophoria produced disappointing results, with treatment effects below 20%.97,98
An unexpected finding in the CLEERE study (2011) is that exophoria at near was associated with myopia progression, although the effect was not clinically significant.16 In further analysis of this study, Berntsen et al noted that the mild slowing of myopia progression from MFSL does not require a mechanism that relates to binocular coordination or accommodation.16 By decreasing the accommodative lag during near work, this will also decrease the amount of hyperopic defocus.
In the STAMP study (2012), 64% of participants were esophoric at near.60 However, near heterophoria was not associated with myopia progression or the magnitude of the PAL treatment effect.
An early myopia control spectacle lens design comprised E-segment bifocal spectacles with a +1.50D addition combined with 3 PD base in prism. Cheng et al compared this intervention with a +1.50D add E-segment bifocal without the prism and with single vision spectacles.99 The rationale underlying the use of base in prism is that when children with near orthophoria or exophoria use an add, this is likely to result in an exophoric shift (by relaxing accommodative convergence) which may cause problems from the higher demand for fusional convergence. Cheng et al’s study population were Chinese-Canadian children with progressing myopia. Over three years, both interventions slowed myopia progression, by 39% for just bifocals and by 51% for bifocals with prism. For children with high lags of accommodation, the treatment effect of both types of bifocal was similar, but for those with low lags, the prismatic bifocals had a greater treatment effect than the normal bifocals. The treatment effect of both types of bifocal was independent of the type of near heterophoria, disconfirming the theories of Hargrave24 and Bayramlar et al.25
Aller et al reported on a randomised controlled trial of centre-distance MFSCL on children with myopia progression of −0.50D or more per annum and with a near eso-fixation disparity.96 Bifocal adds were selected to neutralise the fixation disparity. This approach was associated with stronger treatment effects than in other studies which could be attributable to the targeted approach of treating to correct near esophoria or due to other differences between studies. Alternatively, or additionally, the fact that this subgroup of myopes is likely to obtain symptomatic relief of the binocular vision anomaly may encourage wear of the intervention, contributing to its success.100
Discussion
Compensatory Mechanisms in Accommodative and Binocular Function
The complex inter-relationship between binocular, accommodative, and sensory factors means that these systems may compensate for each other in various ways for different individuals. If there is compromised accommodation then some individuals may attempt to overcome this by exerting excessive neural effort to accommodate resulting in a high AC/A ratio.45 If this mechanism is successful, the individual may have normal or lower than normal accommodative lag. If this is only partly successful at overcoming the compromised accommodation, the individual may have slightly increased accommodative lag. Other cases may not attempt to overcome the compromised accommodation via exerting extra effort, possibly causing higher accommodative lag. Looking at a group of individuals, some of whom adopt each strategy, mean accommodative lag may be close to normal, despite an underlying accommodative deficit.
Another type of compensatory mechanism is that some people with a decompensated heterophoria may develop sensory suppression to prevent symptoms.14 Individuals differ in their ability to develop suppression,101,102 and suppression may be easier to develop when there is a constant or large heterophoria.14 Therefore, for some individuals, who can develop suppression, a high esophoria may be less problematic whereas for those who cannot develop suppression a larger esophoria may be more problematic.
The complexity associated with these mechanisms may account for an interesting finding by researchers investigated the effects of myopia control interventions (OrthoK and MFSCL) on a variety of accommodative and binocular functions.103,104 There were negligible differences in the mean of these variables, but a common finding was that the standard deviation of the study populations reduced with myopia control interventions. This finding is compatible with the considerations outlined above.
For those researching this topic, this observation highlights the dangers of over-reliance on measures of central tendency (eg, mean, median). It is essential to plot raw data to see whether a measure of central tendency is valid. An example is in the data of Goss and Jackson, where many children who became myopic exhibited an esophoric shift but a subset had increasing exophoria. The usual approach of scoring esophoria as positive values and exophoria as negative values will lead to a compensating error, where the mean may remain stable despite marked changes in the variable under consideration (see Figure 4).
Summary and Synthesis of Main Findings
First, the roles of accommodative function and binocular coordination in myopia development (onset) are summarised. The multifactorial nature of myopia means that no one parameter is likely to be a very strong predictor of myopia onset. This may in part explain inconclusive findings of an earlier review on the role of accommodative function in myopia development.105 The fact that accommodative, binocular, and sensory functions interact and to some extent may compensate for one another further reduces the likely strength of any one variable at predicting myopia, even if the variable plays some causal role. The imperfect sensitivity and specificity of clinical tests, especially in young children, is another factor that will limit their predictive power.
The CLEERE study found that as early as four years before myopia onset, children who would become myopic had a significantly higher AC/A ratio then children who remained emmetropic.45 The AC/A ratio increased monotonically in the years approaching myopia onset. This seems to be strong evidence supporting involvement of ocular motor factors in myopia onset. The finding that RPHD only started to differentiate the groups two years before myopia onset could challenge the predominance of the RPHD hypothesis. However, there are difficulties in measuring peripheral refraction, especially in young children, so further research is required to confirm these findings.106
Longitudinal studies also find low PRA to be a predictor of myopia onset.41,46 The WEPrOM publication states that PRA was measured with vision correction using a phoropter,46 so the results should not have been confounded by the degree of hyperopia. PRA measures the accommodation that can be exerted without changing convergence. Therefore, PRA can be considered to be the “accommodation in reserve”, and a low PRA can be indicative of accommodative insufficiency.107
Both low PRA and high AC/A ratio are signs of convergence excess,107,108 and therefore the findings of Goss and the WEPrOM study may be consistent with those of the CLEERE study. An alternative explanation lies in the conclusions of the WEPrOM authors, that they had detected “reduced accommodative functions”,46 which agree with the CLEERE study conclusion of “compromised accommodation”.45 This is supported by the Lhasa Childhood Eye Study47 finding that lower habitual accommodative tone is somewhat predictive of myopia onset.
Considering binocular coordination, on average (but by no means always) myopia onset is preceded by a shift in the near heterophoria in the eso direction, which is likely to be secondary to the increase in AC/A ratio and is consistent with convergence excess.14 The finding of an increased tendency for near esophoria in children who progress to develop myopia41,45 is most likely to be a consequence of the high AC/A ratio that precedes myopia onset.45
A weakness of the argument that accommodative dysfunction is an aetiological factor in myopia progression is the disappointing results of studies of myopia control trials with bifocal/PAL spectacles. An early study indicated that the myopia control effects of bifocal/PAL spectacles may be more substantial in participants with a near esophoria.95 However, subsequent studies failed to provide strong support for the initial findings.97,98 Berntsen et al found that when children with a high accommodative lag (mean, +1.76D) were prescribed a near add (+2.00) the lag decreased by less than 25% of the add (to a mean of +1.26D).109 Therefore, it may be unsafe to assume that bifocal/PAL spectacles will necessarily correct the “compromised accommodation” implicated by Mutti et al.45
Taken together, the findings of changes to accommodation as an early predictor of myopia onset increases the likelihood that accommodation may be one of the factors involved in myopia aetiology. This conclusion refers to early onset myopia, but probably not late onset myopia because only the former is associated with a high AC/A ratio.87
Although the analysis by Mutti et al of the CLEERE data implicates a high AC/A ratio as predictive of myopia onset, the study found no association between the AC/A ratio and the rate of myopia progression regardless of the level of near work activity.45 The present review also indicates that there is much less evidence for any relationship between abnormal accommodation and myopia progression. Although several studies have argued that progressing myopes have increased accommodative lag, some authors have attributed this finding to artefacts induced by measuring accommodation under artificial conditions. In particular, the findings of Labhishetty et al68 questions the concept of clinically significant accommodative lag, as highlighted by Brennan et al.110
This raises an apparent paradox, with evidence suggesting that accommodative dysfunction may be a factor involved in myopia aetiology without also being a factor involved in myopia progression. Although this may seem counter-intuitive, it is analogous to another factor that has a role in myopia development, lack of time outdoors, which appears to have little or no relationship with myopia progression.111,112 Further research is required to determine whether these are examples of the rare situation of mechanistic factors that contribute to the development of a condition but not to its progression.
This difference between myopia onset and myopia progression may help to partially explain an apparent contradiction in this review. Longitudinal studies indicate an eso-drift at myopia onset but cross-sectional studies that have compared children with myopia with emmetropes find, on average, that myopia is associated with exophoria. The non-linear relationship in Figure 4 additionally may partially explain this. Also, not all myopes will exhibit the esophoric shift around the time of myopia onset.
The feedback loop theory of myopia development and progression is that hyperopic defocus from near vision leads to axial elongation.113 According to this model, myopia is simply an adaptation to the environment. Hyperopic defocus may be a mechanism and accommodative lag a contributory factor because it increases hyperopic defocus. Berntsen et al investigated this hypothesis and found only partial support.60 There are some difficulties with this theory. Most importantly, the finding of Labhishetty et al raises serious questions about the veracity of clinical measurements of accommodative lag68 and therefore about theories based on this.110
Even if accommodative lag is relevant in some cases, another weakness of the feedback loop hypothesis is that it would predict that under-correcting myopia should slow myopia progression, and most studies indicate that under-correction is not an effective myopia control strategy.26,114–117 Medina, a leading advocate of the feedback loop hypothesis, argues that the level of under-correction in these studies is too low and the typical approach, of under-correcting by a fixed amount, is inappropriate.113 Medina posits that myopia should be under-corrected by a proportion of the refractive error. A study by Sun et al that used a greater degree of under-correction, did find significantly slower myopia progression in the uncorrected group.118 Further support comes from a study with an even higher degree of under-correction monocularly, achieved by monovision.119
This monovision study, by Phillips in 2005, is particularly important for the present review. Phillips measured accommodation and showed that all his participants accommodated to read with the dominant, distance focussed, eye,119 which is as expected from previous research.120 In other words, the slower myopia progression he found in the near vision eye is not attributable to an accommodative mechanism, but more likely to be due to a reduction of hyperopic defocus or increase in myopic defocus. This supports the feeback loop hypothesis.
A third potential weakness of the feedback loop hypothesis is that bifocal and PAL lenses might be expected to have a greater effect at myopia control than revealed in Figure 3.79 However, accommodative lag only decreases by less than 25% of the near addition,109 so hyperopic defocus will not be reduced by as much as might be anticipated.
Comparison with Previous Reviews
An early review by Goss and Zhai concluded that myopia is associated with abnormal results at some accommodative functions and near esophoria.121 Prousali et al reviewed the role of accommodative function in myopia development.105 They summarised research findings as inconclusive, but nonetheless recommended measuring AC/A ratio as “it may show a rise preceding myopia onset”.
The two most thorough reviews to have considered this topic are a 2021 review by the International Myopia Institute (IMI; Logan et al)122 and a 2024 review by the USA National Academy of Sciences (NAS).79 The conclusions of the IMI review are not supportive of a role for accommodation and binocular coordination: “Current evidence does not point toward a role for accommodation and binocular vision in myopia development and progression”. In other places, the findings are summarised more positively:
Further research is critical to understanding the factors underlying accommodative and binocular mechanisms that may be involved in myopia development and its progression and to guide recommendations for targeted interventions to slow myopia progression.
Concerning accommodative lag, the IMI review (p. 3) cites references supporting the view that children and adults with myopia tend to have higher accommodative lags than emmetropes and that higher lags are associated with faster myopia progression.122 However, later in the review (p. 13) they cite the study by Chen et al64 as evidence that “Lag of accommodation has not been found to be associated with myopia progression”. The review’s conclusion, that high accommodative lag is more likely to represent a consequence rather than a stimulus for myopia, seems to rely on one paper but was perhaps prescient in view of the publication later that year by Labhishetty et al.68 The review suggests that near esophoria in myopia is a compensation for deficient accommodation rather than a causative factor for myopia progression.
The other major review, by the USA National Academy of Sciences (NAS) in 2024, is more positive about a role for accommodation.79 The authors comment that both young and adult myopes consistently show increased accommodative lag, and the accommodative response function decreases as myopia progresses. On the other hand, the review notes that “If near work and hyperopic defocus were as detrimental to the eye as assumed from animal models, bifocal spectacles would have solved the problem long ago”. The NAS review authors note that effects of accommodation and near work may be overstated in childhood and underappreciated at earlier ages. Since most infants are hyperopic, the review points out that infants are either experiencing defocus or they are accommodating and experiencing less defocus.
The NAS review stresses that our current ability to explain why people develop refractive errors and in particular high myopia is very limited. The review suggests that environmental factors may play a greater role than evidenced to date, because most studies have used coarse methods of assessing these variables (eg, parental questionnaires).79 It notes the high preponderance of near objects indoors compared with outdoors. Concerning the mechanism of current myopia control interventions, the NAS review considers that one potential mechanism is chronic relaxation of accommodation.79 The review notes that it is unclear whether the myopia control effect of optical interventions is achieved via RPHD, reduced contrast, or an accommodative mechanism.
Brennan et al noted that the most dramatic differences between refractive groups in terms of accommodative lag were obtained under contrived, unnatural viewing conditions, (ie, monocular distance viewing with lens-induced blur), with much more modest differences observed under binocular viewing of near targets.110 Brennan et al went on to cite the research by Labhishetty et al68 and other evidence that questions the existence of clinically significant accommodative lag as a correlate of myopia. Brennan et al conclude that there is little evidence to support the proposition that accommodative lag is involved in myopia development. They noted, however, that the broader role of accommodation in myopia onset and progression should not be completely dismissed. For example, they cited a study17 which found that failure to accommodate fully when wearing a myopia control soft contact lens was associated with greater myopia progression.
Limitations
A limitation of the present review is that the search was restricted to PubMed, although this was supplemented by detailed searching of bibliographies (Figure 1). Another limitation is that animal studies were excluded. The challenge with animal studies is always the question of whether findings in other species apply to humans. Additional limitations are the exclusion of non-English studies and that the review protocol was not published.
Causes of Myopia: A Multifactorial Risk-Resilience Model
Most myopia is attributable to environmental and genetic factors,79 with over 500 genetic loci for myopia.123 An exception is myopic anisometropia, when the two eyes will have the same genotype and are likely to have very similar environmental experiences.124 More generally, myopia development and progression is likely to be multifactorial: there is no single cause of myopia, but rather several causative factors. The risk of myopia developing or progressing in an individual may be proportional to the number of risk factors: an additive risk factor model. The present authors propose that myopia aetiology is best conceptualised as a risk-resilience model. This is illustrated in Figure 5, which includes evidence-based and speculative risk and protective factors for myopia.125–127
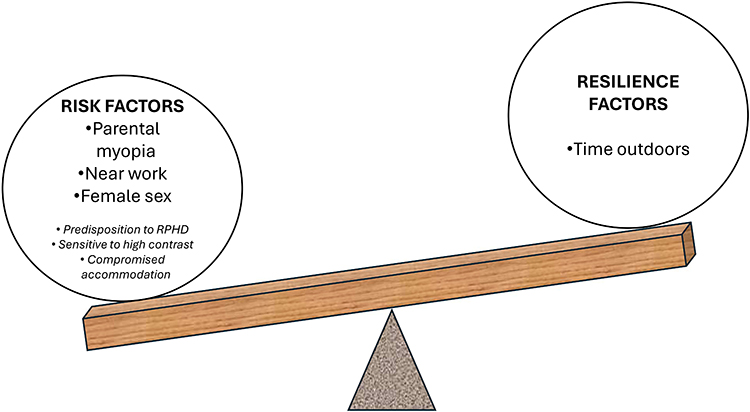 |
Figure 5 The authors’ proposed multifactorial risk-resilience model of myopia. Risk factors and resilience factors in normal font are taken from the umbrella review of risk factors for myopia by Ying et al127 and additional speculative risk factors are in italics. |
Evolution by natural selection requires diversity.128 This means that each of the factors in Figure 5 will be manifested in different individuals to varying degrees, sometimes not at all.106
An important consequence of an additive risk factor/resilience model is that researchers whose data support different causative factors for myopia do not have to compete for “the cause” of myopia. This model positions different causal factors as complimentary rather than competing.
Clinical Implications
Accommodation and Binocular Coordination are Neither Irrelevant nor Major Causative Factors in Myopia
One of the strongest indications for a causal role for accommodative/binocular factors in myopia aetiology is the finding by Mutti et al in the CLEERE study that the first optometric sign to precede the development of myopia is a higher AC/A ratio four years before the onset of myopia.45 This was interpreted as compromised accommodation. This does not prove causality as it is possible that this change could be secondary to some other factor that was not detected in the study.
From a clinical perspective, even if compromised accommodation is a predictor of myopia, there is no evidence that it can be treated in a way that will prevent myopia onset. Concerning myopia progression, attempts to reduce the demand for accommodation using bifocal/PAL spectacles have had disappointing treatment effects75 that are predominantly short-term.129 Two of the most effective interventions (atropine and lenslet spectacle lenses) are known to impair (atropine) and provide no support (lenslet spectacles)130–133 to accommodation. The fact that these interventions are among the most effective indicates that accommodation is unlikely to be a major cause of myopia progression.
The Need to Consider Idiosyncratic Effects
The multifactorial model in Figure 5 and natural variation in the population128 explains the considerable scatter that is seen in the results of most trials of myopia control interventions. This raises an important limitation of much research and reviews on this topic, which is the tendency to concentrate on mean or median results rather than exploring the diversity of results. Accommodative and binocular function may be of no relevance to myopia development for some individuals, of minor relevance to others, and an important feature for a few. This is why an individualised approach is likely to be more successful134,135 and combination treatments often will be required.2,136,137 A recent International Myopia Institute review recommends that comprehensive evaluations of myopic patients should include assessments of binocular co-ordination and accommodation.138
Convergence Excess Esophoria
Children who have a high AC/A ratio will sometimes have decompensated near esophoria (convergence excess).14 The prevalence of symptomatic convergence excess in two samples of university students in Spain was 1.5%139 and 2.3%.140 In rural schoolchildren in South Korea, the prevalence was 1.9%.141 The main treatment option for this condition is bifocal spectacles, with the near addition selected to neutralize eso-fixation disparity.14 The three studies of bifocal/PAL spectacles and contact lenses that obtained the greatest myopia control effect (~40–50%95,142 and ~70%96 respectively) adopted this approach. The COMET2 study targeted children with high accommodative lag and near esophoria, but did not select symptomatic participants.
Studies have demonstrated that with a lenslet spectacle lens design, the extra plus power of the lenslets cannot be used to focus near targets,131 and lenslet and cylindrical annular refractive element designs of spectacle lenses do not alter accommodative responses.130 In cases with symptomatic convergence excess esophoria and progressing myopia, the benefits from bifocal spectacles are two-fold. First, the symptoms from the near esophoria are likely to be alleviated. Second, bifocals are also likely to some extent to slow myopia progression. Aller et al96 reported a similar benefit from MFSCL. Lenslet designs may have a superior effect at slowing myopia progression but would not be expected to alleviate the symptoms from the decompensated near esophoria. The optimum treatment should be determined on an individual basis by balancing the need to treat symptoms (best addressed with bifocals) with the importance of slowing myopia progression (better treated with lenslet designs).
Recommendations for Research
Inter-individual variation is apparent in the response to myopia control interventions. For example, in Lam et al’s report of six years’ results with DIMS lenses, 22% of cases had no myopia progression over six years and in contrast 11% appeared to receive no benefit from the intervention (1.2 mm of axial elongation over the six years).8 A priority for research is to determine variables that would prospectively identify these high and low responders. A suitable study design would be to carry out a battery of optometric investigations before prescribing a myopia control intervention and then to monitor the cases to see which variables best predict treatment outcome.
The possibility raised in this review, that accommodation may be abnormal before the onset of myopia but may not be implicated in the progression of myopia, may be relevant to growing interest in treating myopia early, ideally preventing or delaying the onset of myopia.143 Research should investigate the possibility of using the early predictors of myopia highlighted in this review to detect cases for early intervention, and possibly for developing new interventions.
More generally, the multifactorial nature of myopia makes it particularly important that researchers report the range of findings, not just measures of central tendency (eg, mean and median). Measures of central tendency can mask heterogeneity within datasets. For example, widely different underlying datasets can produce similar bar charts,144 and therefore it is recommended that full data are presented graphically.145 Vision researchers have been shown to underperform146 in this movement towards transparent data reporting.144
Conclusions
A complete understanding of the reasons for the development and progression of myopia requires a multifactorial model. It is concluded from the literature that accommodative dysfunction seems to play some role in myopia onset, although accommodative and binocular factors are unlikely to be major causal factors in myopia progression.
Abbreviations
AC/A, accommodative convergence to accommodation ratio; CA/C, convergence-accommodation to convergence ratio; CLEERE, Collaborative Longitudinal Evaluation of Ethnicity and Refractive Error; COMET, Correction of Myopia Evaluation Trial; CONT, control; DIMS, Defocus Incorporated Multiple Segment; e, edition; eso, eso-deviation (esophoria or esotropia); exo, exo-deviation (exophoria or exotropia); HAT, habitual accommodative tone; HDA, high dose atropine; IMI, International Myopia Institute; IOP, intraocular pressure; LDA, low dose atropine; L-M, long- to medium- wavelength cone photoreceptor contrast; LOM, late onset myope; MDA, medium dose atropine; MFSCL, multifocal soft contact lenses; MFSL, multifocal spectacle lenses; N, number of participants; NAS, National Academy of Sciences; NITM, near work-induced transient myopia; NRA, negative relative accommodation; ORTHOK, orthokeratology; ORTHOKA, orthokeratology combined with atropine; p, probability; PAL, progressive addition lens spectacles; PD, prism dioptre; PPSL, peripheral plus spectacle lenses; PRA, positive relative accommodation; r, correlation coefficient; RGP, rigid gas permeable contact lenses; RLRL, repeated low-level red light; RPHD, relative peripheral hyperopic defocus; SER, spherical equivalent refraction; STAMP, Study of Theories about Myopia Progression Trial; SVL, single vision lenses; UCSL, under-corrected spectacle lenses; WEPrOM, Wenzhou Medical University Essilor Progression and Onset of Myopia.
Author Contributions
All authors made a significant contribution to the work reported, whether that is in the conception, study design, execution, acquisition of data, analysis and interpretation, or in all these areas; took part in drafting, revising or critically reviewing the article; gave final approval of the version to be published; have agreed on the journal to which the article has been submitted; and agree to be accountable for all aspects of the work.
Funding
This work was funded by HOYA Vision Care.
Disclosure
This work was funded by HOYA Vision Care. NV is an employee of HOYA Vision Care. RS was an employee of HOYA Vision Care when the review was conducted. BE has received from HOYA Vision Care funding for research, consultancy, and conference attendance.
References
1. Wolffsohn JS, Jong M, Smith EL. et al. IMI 2021 reports and digest - reflections on the implications for clinical practice. Invest Ophthalmol Vis Sci. 2021;62(5):1. doi:10.1167/iovs.62.5.1
2. Shah R, Vlasak N, Evans BJW. High myopia: reviews of myopia control strategies and myopia complications. Ophthalmic Physiol Opt. 2024;44(6):1248–1260. doi:10.1111/opo.13366
3. Sankaridurg P, Berntsen DA, Bullimore MA, et al. IMI 2023 Digest. Invest Ophthalmol Vis Sci. 2023;64(6):7. doi:10.1167/iovs.64.6.7
4. Zhang H, Lam CSY, Tang WC, et al. Myopia control effect is influenced by baseline relative peripheral refraction in children wearing Defocus Incorporated Multiple Segments (DIMS) spectacle lenses. J Clin Med. 2022;11(9):2294. doi:10.3390/jcm11092294
5. Radhakrishnan H, Lam CSY, Charman WN. Multiple segment spectacle lenses for myopia control. Part 2: impact on myopia progression. Ophthalmic Physiol Opt. 2023;43(5):1137–1144. doi:10.1111/opo.13194
6. Wolffsohn JS, Gifford KL. Optical strategy utilizing contrast modulation to slow myopia. Ophthalmol Sci. 2025;5(4):100672. doi:10.1016/j.xops.2024.100672
7. Atchison DA, Charman WN. Optics of spectacle lenses intended to treat myopia progression. Optom Vis Sci. 2024;101(5):238–249. doi:10.1097/OPX.0000000000002140
8. Lam CSY, Tang WC, Zhang HY, et al. Long-term myopia control effect and safety in children wearing DIMS spectacle lenses for 6 years. Sci Rep. 2023;13(1):5475. doi:10.1038/s41598-023-32700-7
9. Wong YL, Li X, Huang Y, et al. Eye growth pattern of myopic children wearing spectacle lenses with aspherical lenslets compared with non-myopic children. Ophthalmic Physiol Opt. 2024;44(1):206–213. doi:10.1111/opo.13232
10. Chamberlain P, Bradley A, Arumugam B, et al. Long-term effect of dual-focus contact lenses on myopia progression in children: a 6-year multicenter clinical trial. Optom Vis Sci. 2022;99(3):204–212. doi:10.1097/OPX.0000000000001873
11. Stansbury FC. Pathogenesis of myopia; a new classification. Arch Ophthal. 1948;39(3):273–299. doi:10.1001/archopht.1948.00900020280003
12. Kinney JA, Luria SM, McKay CL, Ryan AP. Vision of submariners. Undersea Biomed Res. 1979;6 Suppl:S163–73.
13. Burns DH, Evans BJW, Allen PM. Clinical measurement of amplitude of accommodation: a review. Optom Pract. 2014;15(3):75–86.
14. Evans BJW. Pickwell’s Binocular Vision Anomalies.
15. Corpus G, Molina-Martin A, Pinero DP. Efficacy of soft contact lenses for myopia control: a systematic review. Semin Ophthalmol. 2024;39(3):185–192. doi:10.1080/08820538.2023.2271063
16. Berntsen DA, Sinnott LT, Mutti DO, Zadnik K, Group CS. Accommodative lag and juvenile-onset myopia progression in children wearing refractive correction. Vis Res. 2011;51(9):1039–1046. doi:10.1016/j.visres.2011.02.016
17. Cheng X, Xu J, Brennan NA. Accommodation and its role in myopia progression and control with soft contact lenses. Ophthalmic Physiol Opt. 2019;39(3):162–171. doi:10.1111/opo.12614
18. Read SA, Collins MJ, Woodman EC, Cheong SH. Axial length changes during accommodation in myopes and emmetropes. Optom Vis Sci. 2010;87(9):656–662. doi:10.1097/OPX.0b013e3181e87dd3
19. Woodman EC, Read SA, Collins MJ. Axial length and choroidal thickness changes accompanying prolonged accommodation in myopes and emmetropes. Vis Res. 2012;72:34–41. doi:10.1016/j.visres.2012.09.009
20. Schmid KL, Strang NC. Differences in the accommodation stimulus response curves of adult myopes and emmetropes: a summary and update. Ophthalmic Physiol Opt. 2015;35(6):613–621. doi:10.1111/opo.12255
21. Yan L, Huibin L, Xuemin L. Accommodation-induced intraocular pressure changes in progressing myopes and emmetropes. Eye. 2014;28(11):1334–1340. doi:10.1038/eye.2014.208
22. Deng B, Zhou M, Kong X, et al. The lack of causal link between myopia and intraocular pressure: insights from cross-sectional analysis and Mendelian randomization study. Photodiagnosis Photodyn Ther. 2024;49:104334. doi:10.1016/j.pdpdt.2024.104334
23. Marcos S. Optical and visual diet in myopia. Invest Ophthalmol Vis Sci. 2025;66(7):3. doi:10.1167/iovs.66.7.3
24. Hargrave BK. Accommodation: the role of the external muscles of the eye: a consideration of refractive errors in relation to extraocular malfunction. Med Hypotheses. 2014;83(5):607–613. doi:10.1016/j.mehy.2014.08.006
25. Bayramlar H, Karadag R, Uslu H, Cakici O. Which one is more causative for myopia progression: accommodation or convergence? Med Hypotheses. 2015;85(1):112. doi:10.1016/j.mehy.2015.04.003
26. Walline JJ, Lindsley KB, Vedula SS, et al. Interventions to slow progression of myopia in children. Cochrane Database Syst Rev. 2020;(1). doi:10.1002/14651858.CD004916.pub4
27. Shahsuvaryan ML. Atropine: updates on myopia pharmacotherapy. Taiwan J Ophthalmol. 2024;14(2):225–229. doi:10.4103/tjo.TJO-D-22-00060
28. Hughes RPJ, Woodman-Pieterse EC, Read SA, Vincent SJ, Collins MJ. Effect of 0.025% atropine on ocular biometry changes during accommodation. Ophthalmic Physiol Opt. 2025;45(3):865–876. doi:10.1111/opo.13485
29. Horn D, Salzano AD, Jenewein EC, et al. Topical review: potential mechanisms of atropine for myopia control. Optom Vis Sci. 2025;102(5):260–270. doi:10.1097/OPX.0000000000002249
30. Dahlmann-Noor AH, Bokre D, Khazova M, Price LLA. Measuring the visual environment of children and young people at risk of myopia: a scoping review. Graefes Arch Clin Exp Ophthalmol. 2025;263:1213–1228. doi:10.1007/s00417-024-06719-z
31. Queiros A, Cervino A, Gonzalez-Meijome JM. Peripheral refraction of myopic eyes with spectacle lenses correction and lens free emmetropes during accommodation. Eye Vis. 2021;8(1):45. doi:10.1186/s40662-021-00267-x
32. Song D, Yang Q, Ge J, Chen K, Tong J, Shen Y. Color vision-associated environmental and biological factors in the development of myopia. Exp Eye Res. 2025;254:110324. doi:10.1016/j.exer.2025.110324
33. Morgan IG, Wu PC, Ostrin LA, et al. IMI risk factors for myopia. Invest Ophthalmol Vis Sci. 2021;62(5):3. doi:10.1167/iovs.62.5.3
34. Munn Z, Peters MDJ, Stern C, Tufanaru C, McArthur A, Aromataris E. Systematic review or scoping review? Guidance for authors when choosing between a systematic or scoping review approach. BMC Med Res Methodol. 2018;18(1):143. doi:10.1186/s12874-018-0611-x
35. Khalil H, Peters MD, Tricco AC, et al. Conducting high quality scoping reviews-challenges and solutions. J Clin Epidemiol. 2021;130:156–160. doi:10.1016/j.jclinepi.2020.10.009
36. Chakraborty R, Ostrin LA, Benavente-Perez A, Verkicharla PK. Optical mechanisms regulating emmetropisation and refractive errors: evidence from animal models. Clin Exp Optom. 2020;103(1):55–67. doi:10.1111/cxo.12991
37. Bullimore MA, Lee SS, Schmid KL, et al. IMI-onset and progression of myopia in young adults. Invest Ophthalmol Vis Sci. 2023;64(6):2. doi:10.1167/iovs.64.6.2
38. Tarrant J, Severson H, Wildsoet CF. Accommodation in emmetropic and myopic young adults wearing bifocal soft contact lenses. Ophthalmic Physiol Opt. 2008;28(1):62–72. doi:10.1111/j.1475-1313.2007.00529.x
39. Ghoushchi VP, Mompean J, Prieto PM, Artal P. Binocular dynamics of accommodation, convergence, and pupil size in myopes. Biomed Opt Express. 2021;12(6):3282–3295. doi:10.1364/BOE.420334
40. Rosenfield M, Desai R, Portello JK. Do progressing myopes show reduced accommodative responses? Optom Vis Sci. 2002;79(4):268–273. doi:10.1097/00006324-200204000-00014
41. Goss DA. Clinical accommodation and heterophoria findings preceding juvenile onset of myopia. Optom Vis Sci. 1991;68(2):110–116. doi:10.1097/00006324-199102000-00005
42. Goss DA, Jackson TW. Clinical findings before the onset of myopia in youth: 2. Zone of clear single binocular vision. Optom Vis Sci. 1996;73(4):263–268. doi:10.1097/00006324-199604000-00008
43. Mutti DO, Mitchell GL, Hayes JR, et al. Accommodative lag before and after the onset of myopia. Invest Ophthalmol Vis Sci. 2006;47(3):837–846. doi:10.1167/iovs.05-0888
44. Zadnik K, Sinnott LT, Cotter SA, et al. Prediction of juvenile-onset myopia. JAMA Ophthalmol. 2015;133(6):683–689. doi:10.1001/jamaophthalmol.2015.0471
45. Mutti DO, Mitchell GL, Jones-Jordan LA, et al. The response AC/A ratio before and after the onset of myopia. Invest Ophthalmol Vis Sci. 2017;58(3):1594–1602. doi:10.1167/iovs.16-19093
46. Wong YL, Yuan Y, Su B, et al. Prediction of myopia onset with refractive error measured using non-cycloplegic subjective refraction: the WEPrOM Study. BMJ Open Ophthalmol. 2021;6(1):e000628. doi:10.1136/bmjophth-2020-000628
47. Luo F, Hao J, Li L, et al. Baseline refractive error, habitual accommodative tone, and its association with myopia in children: the Lhasa Childhood Eye Study. Invest Ophthalmol Vis Sci. 2023;64(11):4. doi:10.1167/iovs.64.11.4
48. Sun W, Yu M, Wu J, et al. Pseudomyopia as an independent risk factor for myopia onset: a prospective cohort study among school-aged children. Br J Ophthalmol. 2024;108(6):873–878. doi:10.1136/bjo-2022-322330
49. Goss DA, Jackson TW. Clinical findings before the onset of myopia in youth: 3. Heterophoria. Optom Vis Sci. 1996;73(4):269–278. doi:10.1097/00006324-199604000-00009
50. Gwiazda J, Thorn F, Bauer J, Held R. Myopic children show insufficient accommodative response to blur. Invest Ophthalmol Vis Sci. 1993;34(3):690–694.
51. Jensen H. Myopia in teenagers. An eight-year follow-up study on myopia progression and risk factors. Acta Ophthalmol Scand. 1995;73(5):389–393. doi:10.1111/j.1600-0420.1995.tb00294.x
52. Abbott ML, Schmid KL, Strang NC. Differences in the accommodation stimulus response curves of adult myopes and emmetropes. Ophthalmic Physiol Opt. 1998;18(1):13–20.
53. Gwiazda JE, Hyman L, Norton TT, et al. Accommodation and related risk factors associated with myopia progression and their interaction with treatment in COMET children. Invest Ophthalmol Vis Sci. 2004;45(7):2143–2151. doi:10.1167/iovs.03-1306
54. Lu F, Xu D, Qu J. A study on difference of ocular motor parameters in myopia. Zhonghua Yan Ke Za Zhi. 2004;40(9):583–586.
55. Seidel D, Gray LS, Heron G. The effect of monocular and binocular viewing on the accommodation response to real targets in emmetropia and myopia. Optom Vis Sci. 2005;82(4):279–285. doi:10.1097/01.opx.0000159369.85285.21
56. Wang Q, Wang QM. [The roles of AC/A ratio and other ocular motor parameters in the induction of late-onset myopia]. Zhonghua Yan Ke Za Zhi. 2006;42(9):792–795. Hausa
57. Allen PM, O’Leary DJ. Accommodation functions: co-dependency and relationship to refractive error. Vis Res. 2006;46(4):491–505. doi:10.1016/j.visres.2005.05.007
58. Pandian A, Sankaridurg PR, Naduvilath T, et al. Accommodative facility in eyes with and without myopia. Invest Ophthalmol Vis Sci. 2006;47(11):4725–4731. doi:10.1167/iovs.05-1078
59. Lundstrom L, Mira-Agudelo A, Artal P. Peripheral optical errors and their change with accommodation differ between emmetropic and myopic eyes. J Vis. 2009;9(6):17.1–11. doi:10.1167/9.6.17
60. Berntsen DA, Sinnott LT, Mutti DO, Zadnik K. A randomized trial using progressive addition lenses to evaluate theories of myopia progression in children with a high lag of accommodation. Invest Ophthalmol Vis Sci. 2012;53(2):640–649. doi:10.1167/iovs.11-7769
61. Sreenivasan V, Aslakson E, Kornaus A, Thibos LN. Retinal image quality during accommodation in adult myopic eyes. Optom Vis Sci. 2013;90(11):1292–1303. doi:10.1097/OPX.0000000000000068
62. Koomson NY, Amedo AO, Opoku-Baah C, Ampeh PB, Ankamah E, Bonsu K. Relationship between reduced accommodative lag and myopia progression. Optom Vis Sci. 2016;93(7):683–691. doi:10.1097/OPX.0000000000000867
63. Labhishetty V, Bobier WR. Are high lags of accommodation in myopic children due to motor deficits? Vis Res. 2017;130:9–21. doi:10.1016/j.visres.2016.11.001
64. Chen Y, Drobe B, Zhang C, et al. Accommodation is unrelated to myopia progression in Chinese myopic children. Sci Rep. 2020;10(1):12056. doi:10.1038/s41598-020-68859-6
65. Meyer D, Gantes-Nuñez J, Rickert M, et al. Accommodative behaviour and retinal defocus in highly myopic eyes fitted with a dual focus myopia control contact lens. Ophthalmic Physiol Opt. 2025;45(1):189–199. doi:10.1111/opo.13420
66. Singh NK, Kollbaum P. Accommodative behaviour and retinal defocus of children during prolonged viewing of electronic devices while wearing dual-focus myopia control soft contact lenses. Ophthalmic Physiol Opt. 2025;45(6):1456–1467. doi:10.1111/opo.13533
67. Rosenfield M, Li RT, Kirsch NT. A double-blind test of blue-blocking filters on symptoms of digital eye strain. Work. 2020;65(2):343–348. doi:10.3233/WOR-203086
68. Labhishetty V, Cholewiak SA, Roorda A, Banks MS. Lags and leads of accommodation in humans: fact or fiction? J Vis. 2021;21(3):21. doi:10.1167/jov.21.3.21
69. Tarrant J, Roorda A, Wildsoet CF. Determining the accommodative response from wavefront aberrations. J Vis. 2010;10(5):4. doi:10.1167/10.5.4
70. Kochgaway L, Chandra A, Basu I, Chaudhury D, Jethani J, Bhaumik A. Practice patterns in pediatric myopia management: insights from a 2023 survey among Indian ophthalmologists. Indian J Ophthalmol. 2025;73(2):280–286. doi:10.4103/IJO.IJO_3110_23
71. Lin Z, Vasudevan B, Liang YB, Zhou HJ, Ciuffreda KJ. The association between nearwork-induced transient myopia and progression of refractive error: a 3-year cohort report from Beijing Myopia Progression Study. J Optom. 2021;14(1):44–49. doi:10.1016/j.optom.2020.05.004
72. Vasudevan B, Ciuffreda KJ, Gilmartin B. Sympathetic inhibition of accommodation after sustained nearwork in subjects with myopia and emmetropia. Invest Ophthalmol Vis Sci. 2009;50(1):114–120. doi:10.1167/iovs.08-1762
73. Vera-Diaz FA, Strang NC, Winn B. Nearwork induced transient myopia during myopia progression. Curr Eye Res. 2002;24(4):289–295.
74. Liu ESF, Cudia M, Wong GKY, Ko CN, Lam DSC. The concept of cone opponency may extend beyond accommodation, to myopiagenesis and emmetropization, for a better peripheral defocus lens. Asia Pac J Ophthalmol. 2024;13(6):100125. doi:10.1016/j.apjo.2024.100125
75. Lawrenson JG, Huntjens B, Virgili G, et al. Interventions for myopia control in children: a living systematic review and network meta‐analysis. Cochrane Database Syst Rev. 2025;2(2):CD014758. doi:10.1002/14651858.CD014758.pub3
76. Bullimore MA. Myopia control: the time is now. Ophthalmic Physiol Opt. 2014;34(3):263–266.
77. Sankaridurg PR, Holden BA. Practical applications to modify and control the development of ametropia. Eye. 2014;28(2):134–141.
78. Correction of Myopia Evaluation Trial 2 Study Group for the Pediatric Eye Disease Investigator Group. Progressive-addition lenses versus single-vision lenses for slowing progression of myopia in children with high accommodative lag and near esophoria. Invest Ophthalmol Vis Sci. 2011;52(5):2749–2757. doi:10.1167/iovs.10-6631
79. National Academy of Sciences (NAS). Myopia: Causes, Prevention, and Treatment of an Increasingly Common Disease. The National Academies Press; 2024:374.
80. Walline JJ, Walker MK, Mutti DO, et al. Effect of high add power, medium add power, or single-vision contact lenses on myopia progression in children: the BLINK Randomized Clinical Trial. JAMA. 2020;324(6):571–580. doi:10.1001/jama.2020.10834
81. Berntsen DA, Ticak A, Sinnott LT, et al. Peripheral defocus, pupil size, and axial eye growth in children wearing soft multifocal contact lenses in the BLINK Study. Invest Ophthalmol Vis Sci. 2023;64(14):3. doi:10.1167/iovs.64.14.3
82. Chandler MA, Robich ML, Jordan LA, et al. Accommodation in children after 4.7 years of multifocal contact lens wear in the BLINK study randomized clinical trial. Optom Vis Sci. 2023;100(7):425–431. doi:10.1097/OPX.0000000000002040
83. Allen PM, Radhakrishnan H, Price H, et al. A randomised clinical trial to assess the effect of a dual treatment on myopia progression: the Cambridge Anti-Myopia Study. Ophthalmic Physiol Opt. 2013;33(3):267–276. doi:10.1111/opo.12035
84. Zhu M, Feng H, Zhu J, Qu X. The impact of amplitude of accommodation on controlling the development of myopia in orthokeratology. Zhonghua Yan Ke Za Zhi. 2014;50(1):14–19.
85. Lv Z, Tao Z, Chu H, et al. Efficacy of naked-eye 3D technology in mitigating myopia progression among children. Transl Pediatr. 2025;14(4):628–638. doi:10.21037/tp-2024-523
86. Tripepi G, Chesnaye NC, Dekker FW, Zoccali C, Jager KJ. Intention to treat and per protocol analysis in clinical trials. Nephrology. 2020;25(7):513–517. doi:10.1111/nep.13709
87. Rosenfield M, Gilmartin B. Effect of a near-vision task on the response AC/A of a myopic population. Ophthalmic Physiol Opt. 1987;7(3):225–233.
88. Ma J, Yang X, Liu Z, et al. The impact of vergence dysfunction on myopia control in children wearing defocus spectacle lenses. Clin Ophthalmol. 2024;18:799–807. doi:10.2147/OPTH.S453731
89. Leone JF, Cornell E, Morgan IG, et al. Prevalence of heterophoria and associations with refractive error, heterotropia and ethnicity in Australian school children. Br J Ophthalmol. 2010;94(5):542–546. doi:10.1136/bjo.2009.163709
90. Jang JU, Park IJ, Jang JY. The distribution of near point of convergence, near horizontal heterophoria, and near vergence among myopic children in South Korea. Taiwan J Ophthalmol. 2016;6(4):187–192. doi:10.1016/j.tjo.2016.07.001
91. Hong J, Fu J, Wang YD, Zhao BW, Li L. Prevalence of heterophoria in a population of school children in central China: the Anyang Childhood Eye Study. Int J Ophthalmol. 2020;13(5):801–805. doi:10.18240/ijo.2020.05.16
92. Su H, Fu J, Chen W, et al. Prevalence of heterophoria in tibetan grade-one students: the Lhasa Childhood Eye Study. J Ophthalmol. 2020;2020:9570908. doi:10.1155/2020/9570908
93. Chen X, Jiang Y, Fan Q, Li L, Lu W, Wang Y. Association of axial length and refraction with near horizontal heterophoria in Chinese children: an observational cross-sectional study. J Ophthalmol. 2022;2022(1):7549851. doi:10.1155/2022/7549851
94. Alrasheed SH. Relationship between myopia severity, near exophoria, vergence, and accommodation amplitude in children. Saudi J Ophthalmol. 2025. doi:10.4103/sjopt.sjopt_352_24
95. Goss DA, Grosvenor T. Rates of childhood myopia progression with bifocals as a function of nearpoint phoria: consistency of three studies. Optom Vis Sci. 1990;67(8):637–640.
96. Aller TA, Liu M, Wildsoet CF. Myopia control with bifocal contact lenses: a randomized clinical trial. Optom Vis Sci. 2016;93(4):344–352. doi:10.1097/OPX.0000000000000808
97. Fulk GW, Cyert LA, Parker DE. A randomized trial of the effect of single vision vs. bifocal lenses on myopia progression in children with esophoria. Optom Vis Sci. 2000;77(8):395–401.
98. Zhu X, Wang D, Li N, Zhao F. Effects of customized progressive addition lenses vs. single vision lenses on myopia progression in children with esophoria: a randomized clinical trial. J Ophthalmol. 2022;2022:9972761. doi:10.1155/2022/9972761
99. Cheng D, Woo GC, Drobe B, Schmid KL. Effect of bifocal and prismatic bifocal spectacles on myopia progression in children: three-year results of a randomized clinical trial. JAMA Ophthalmol. 2014;132(3):258–264. doi:10.1001/jamaophthalmol.2013.7623
100. Aller T, Wildsoet C. Optical control of myopia has come of age: or has it? Optom Vis Sci. 2013;90(5):e135–e137. doi:10.1097/OPX.0b013e31828b47cf
101. Evans BJW. Monovision: a review. Ophthal Physiol Opt. 2007;27:417–439.
102. Tang STW, Evans BJW. The Near Mallett Unit Foveal Suppression Test: a cross-sectional study to establish test norms and relationship with other optometric tests. Ophthal Physiol Opt. 2007;27(1):31–43.
103. Goris KG, Swarbrick H, Evans BJW Orthokeratology, binocular co-ordination and myopia control [Doctoral]. London South Bank University; 2017.
104. Kang P, watt K, Chau T, Zhu J, Evans BJW, Swarbrick H. The impact of orthokeratology lens wear on binocular vision and accommodation: a short-term prospective study. Cont Lens Anterior Eye. 2018;41(6):501–506. doi:10.1016/j.clae.2018.08.002
105. Prousali E, Haidich AB, Tzamalis A, Ziakas N, Mataftsi A. ‘The role of accommodative function in myopic development: a review.’. Semin Ophthalmol. 2022;37(4):455–461. doi:10.1080/08820538.2021.2006724
106. Kneepkens SCM, Vught LV, Polling JR, Klaver CCW, Tideman JWL, Beenakker JWM. A novel MRI-based approach to peripheral refraction and prediction of myopia progression. Am J Ophthalmol. 2025;278:239–249. doi:10.1016/j.ajo.2025.06.013
107. Scheiman M, Wick B. Clinical Management of Binocular Vision. Heterophoric, Accommodative, and Eye Movement Disorders.
108. Goss DA. Ocular Accommodation, Convergence, and Fixation Disparity.
109. Berntsen DA, Mutti DO, Zadnik K. The effect of bifocal add on accommodative lag in myopic children with high accommodative lag. Invest Ophthalmol Vis Sci. 2010;51(12):6104–6110. doi:10.1167/iovs.09-4417
110. Brennan NA, Cheng X, Jong M, Bullimore MA. Commonly held beliefs about myopia that lack a robust evidence base: 2025 update. Eye Contact Lens. 2025;51(8):319–335. doi:10.1097/ICL.0000000000001191
111. Dhakal R, Huntjens B, Shah R, Lawrenson JG, Verkicharla PK. Influence of location, season and time of day on the spectral composition of ambient light: investigation for application in myopia. Ophthalmic Physiol Opt. 2023;43(2):220–230. doi:10.1111/opo.13085
112. Kido A, Miyake M, Watanabe N. Interventions to increase time spent outdoors for preventing incidence and progression of myopia in children. Cochrane Database Syst Rev. 2024;6(6):CD013549. doi:10.1002/14651858.CD013549.pub2
113. Medina A. The cause of myopia development and progression: theory, evidence, and treatment. Surv Ophthalmol. 2022;67(2):488–509. doi:10.1016/j.survophthal.2021.06.005
114. Adler D, Millodot M. The possible effect of undercorrection on myopic progression in children. Clin Exp Optom. 2006;89(5):315–321. doi:10.1111/j.1444-0938.2006.00055.x
115. Brennan NA, Cheng X. Commonly held beliefs about myopia that lack a robust evidence base. Eye Contact Lens. 2019;45(4):215–225. doi:10.1097/icl.0000000000000566
116. Chung K, Mohidin N, O’Leary DJ. Undercorrection of myopia enhances rather than inhibits myopia progression. Vis Res. 2002;42:2555–2559.
117. Li SY, Li SM, Zhou YH, et al. Effect of undercorrection on myopia progression in 12-year-old children. Graefes Arch Clin Exp Ophthalmol. 2015;253(8):1363–1368. doi:10.1007/s00417-015-3053-8
118. Sun YY, Li SM, Li SY, et al. Effect of uncorrection versus full correction on myopia progression in 12-year-old children. Graefes Arch Clin Exp Ophthalmol. 2017;255(1):189–195. doi:10.1007/s00417-016-3529-1
119. Phillips JR. Monovision slows juvenile myopia progression unilaterally. Br J Ophthalmol. 2005;89(9):1196–1200.
120. Koh LH, Charman WN. Accommodative responses to anisoaccommodative targets. Ophthal Physiol Opt. 1998;18(3):254–262.
121. Goss DA, Zhai H. Clinical and laboratory investigations of the relationship of accommodation and convergence function with refractive error. A literature review. Doc Ophthalmol. 1994;86(4):349–380. doi:10.1007/BF01204595
122. Logan N, Radhakrishnan H, Cruickshank F, et al. IMI accommodation and binocular vision in myopia development and progression. Invest Ophthalmol Visual Sci. 2021;62:4. doi:10.1167/iovs.62.5.4
123. Haarman AEG, Tedja MS, Verhoeven VJM, Klaver CCW; The Erasmus MC Myopia Research Group, Consortium of Refractive Error, Myopia (CREAM). Genetics of myopia: gene finding and beyond. Acta Ophthalmol. 2022;100(S275). doi:10.1111/j.1755-3768.2022.15383
124. Vincent SJ, Collins MJ, Read SA, Carney LG. Myopic anisometropia: ocular characteristics and aetiological considerations. Clin Exp Optom. 2014;97(4):291–307. doi:10.1111/cxo.12171
125. Li L, Wen L, Lan W, Zhu H, Yang Z. A novel approach to quantify environmental risk factors of myopia: combination of wearable devices and big data science. Transl Vis Sci Technol. 2020;9(13):17. doi:10.1167/tvst.9.13.17
126. Martinez-Albert N, Bueno-Gimeno I, Gene-Sampedro A. Risk factors for myopia: a review. J Clin Med. 2023;12(18):6062. doi:10.3390/jcm12186062
127. Ying Z-Q, Li D-L, Zheng X-Y, Zhang X-F, Pan C-W. Risk factors for myopia among children and adolescents: an umbrella review of published meta-analyses and systematic reviews. Br J Ophthalmol. 2023;108(2):167–174. doi:10.1136/bjo-2022-322773
128. Darwin C. On the Origin of Species by Means of Natural Selection, or Preservation of Favoured Races in the Struggle for Life. John Murray; 1859.
129. Kaphle D, Atchison DA, Schmid KL. Multifocal spectacles in childhood myopia: are treatment effects maintained? A systematic review and meta-analysis. Surv Ophthalmol. 2019;65(2):239–249. doi:10.1016/j.survophthal.2019.10.001
130. Lin Z, Christaras D, Duarte-Toledo R, et al. Dynamic accommodation responses in subjects wearing myopia control spectacles modifying peripheral refraction. Invest Ophthalmol Vis Sci. 2025;66(1):55. doi:10.1167/iovs.66.1.55
131. Jaskulski M, Singh NK, Bradley A, Kollbaum PS. Optical and imaging properties of a novel multi-segment spectacle lens designed to slow myopia progression. Ophthalmic Physiol Opt. 2020;40(5):549–556. doi:10.1111/opo.12725
132. Lam CSY, Tang WC, Qi H, et al. Effect of defocus incorporated multiple segments spectacle lens wear on visual function in myopic Chinese children. Transl Vis Sci Technol. 2020;9(9):11. doi:10.1167/tvst.9.9.11
133. Huang Y, Li X, Wang C, et al. Visual acuity, near phoria and accommodation in myopic children using spectacle lenses with aspherical lenslets: results from a randomized clinical trial. Eye Vis. 2022;9(1):33. doi:10.1186/s40662-022-00304-3
134. Chen Y, Mueller A, Morgan I, et al. Best practice in myopia control: insights and innovations for myopia prevention and control – a round table discussion. Br J Ophthalmol. 2024;108(7):913–914. doi:10.1136/bjo-2023-325112
135. Tapaszto B, Flitcroft DI, Aclimandos WA, et al. Myopia management algorithm. Annexe to the article titled Update and guidance on management of myopia. European Society of Ophthalmology in cooperation with International Myopia Institute. Eur J Ophthalmol. 2023;34:11206721231219532. doi:10.1177/11206721231219532
136. Dahlmann-Noor AH, Ghorbani-Mojarrad N, Williams KM, et al. 2024 UK and Ireland modified Delphi consensus on myopia management in children and young people. Ophthalmic Physiol Opt. 2024;44(7):1368–1391. doi:10.1111/opo.13381
137. Nucci P, Lembo A, Schiavetti I, Shah R, Edgar DF, Evans BJW. A comparison of myopia control in European children and adolescents with defocus incorporated multiple segments (DIMS) spectacles, atropine, and combined DIMS/atropine. PLoS One. 2023;18(2):e0281816. doi:10.1371/journal.pone.0281816
138. Jones D, Chow A, Fadel D, et al. IMI-Instrumentation for Myopia Management. Invest Ophthalmol Vis Sci. 2025;66(9):7. doi:10.1167/iovs.66.9.7
139. Porcar E, Martinez-Palomera A. Prevalence of general binocular dysfunctions in a population of university students. Optom Vis Sci. 1997;74(2):111–113. doi:10.1097/00006324-199702000-00023
140. Garcia-Munoz A, Carbonell-Bonete S, Canto-Cerdan M, Cacho-Martinez P. Accommodative and binocular dysfunctions: prevalence in a randomised sample of university students. Clin Exp Optom. 2016;99(4):313–321. doi:10.1111/cxo.12376
141. Jang JU, Park IJ. Prevalence of general binocular dysfunctions among rural schoolchildren in South Korea. Taiwan J Ophthalmol. 2015;5(4):177–181. doi:10.1016/j.tjo.2015.07.005
142. Cheng D, Schmid KL, Woo GC, Drobe B. Randomized trial of effect of bifocal and prismatic bifocal spectacles on myopic progression: two-year results. Arch Ophthalmol. 2010;128(1):12–19. doi:10.1001/archophthalmol.2009.332
143. Bullimore MA, Brennan NA. Myopia: an ounce of prevention is worth a pound of cure. Ophthalmic Physiol Opt. 2023;43(1):116–121. doi:10.1111/opo.13058
144. Bandholm T, Thorborg K, Ardern CL, Christensen R, Henriksen M. Writing up your clinical trial report for a scientific journal: the REPORT trial guide for effective and transparent research reporting without spin. Br J Sports Med. 2022;56(12):683–691. doi:10.1136/bjsports-2021-105058
145. Weissgerber TL, Milic NM, Winham SJ, Garovic VD. Beyond bar and line graphs: time for a new data presentation paradigm. PLoS Biol. 2015;13(4):e1002128. doi:10.1371/journal.pbio.1002128
146. Riedel N, Schulz R, Kazezian V, Weissgerber T. Replacing bar graphs of continuous data with more informative graphics: are we making progress? Clin Sci. 2022;136(15):1139–1156. doi:10.1042/cs20220287
 © 2025 The Author(s). This work is published and licensed by Dove Medical Press Limited. The
full terms of this license are available at https://www.dovepress.com/terms
and incorporate the Creative Commons Attribution
- Non Commercial (unported, 4.0) License.
By accessing the work you hereby accept the Terms. Non-commercial uses of the work are permitted
without any further permission from Dove Medical Press Limited, provided the work is properly
attributed. For permission for commercial use of this work, please see paragraphs 4.2 and 5 of our Terms.
© 2025 The Author(s). This work is published and licensed by Dove Medical Press Limited. The
full terms of this license are available at https://www.dovepress.com/terms
and incorporate the Creative Commons Attribution
- Non Commercial (unported, 4.0) License.
By accessing the work you hereby accept the Terms. Non-commercial uses of the work are permitted
without any further permission from Dove Medical Press Limited, provided the work is properly
attributed. For permission for commercial use of this work, please see paragraphs 4.2 and 5 of our Terms.
Recommended articles
Baseline Accommodation and Binocular Vision Measures in Malay Schoolchildren Enrolled in the Myopia Control Study Using Spectacle Lenses in Kuala Lumpur
Norazman FNN, Mohd-Ali B, Syed Mohd Dardin SF, Mohamad Shahimin M, Mohamad Fadzil N, Mohd Saman MN, Mohidin N
Clinical Optometry 2024, 16:45-52
Published Date: 20 February 2024
Normative Data for Non-Strabismic Binocular Vision Parameters in a Nepalese Young Adults
Chhetri S, Poudel R, Thapa Magar S, Suwal R, Belbase U, Mahat B, Subedi A, Cantó-Cerdán M
Clinical Ophthalmology 2026, 20:584486
Published Date: 10 March 2026