Back to Journals » Clinical Ophthalmology » Volume 9
Scleral buckling for primary rhegmatogenous retinal detachment using noncontact wide-angle viewing system with a cannula-based 25 G chandelier endoilluminator
Authors Imai H, Tagami M, Azumi A
Received 28 June 2015
Accepted for publication 22 August 2015
Published 11 November 2015 Volume 2015:9 Pages 2103—2107
DOI https://doi.org/10.2147/OPTH.S91339
Checked for plagiarism Yes
Review by Single anonymous peer review
Peer reviewer comments 2
Editor who approved publication: Dr Scott Fraser
Hisanori Imai,1,2 Mizuki Tagami,1 Atsushi Azumi1,2
1Department of Ophthalmology, Kobe Kaisei Hospital, 2Division of Ophthalmology, Department of Organ Therapeutics, Kobe University Graduate School of Medicine, Kobe, Japan
Purpose: The aim of this study is to report the result of scleral buckling (SB) using a combination of a noncontact wide-angle viewing system and a cannula-based 25 G chandelier endoilluminator.
Methods: Retrospective analyses of the medical records of 79 eyes of 79 patients with primary uncomplicated rhegmatogenous retinal detachments who had underwent SB using a combination of a noncontact wide-angle viewing system and a chandelier endoilluminator were performed.
Results: There were 50 men and 29 women. The mean ± standard deviation age was 43.7±16.0 years. Their preoperative best-corrected visual acuity (BCVA) was 0.31±0.65 logMAR units. The final BCVA was 0.10±0.31 logMAR units, which was significantly better than the preoperative BCVA (P<0.01). The initial and final anatomical success rates were 92.4% and 100%, respectively. Backward logistic multiple regression analysis revealed no relationship between explanatory variables and the primary anatomic success (P=0.104).
Conclusion: SB using a combination of a noncontact wide-angle viewing system and a chandelier endoilluminator is a modified new technique and may be a valid option for the management of rhegmatogenous retinal detachments.
Keywords: scleral buckling, wide-angle viewing system, chandelier endoilluminator, retinal detachment
Introduction
Rhegmatogenous retinal detachment (RRD) is one of the sight-threatening diseases. Scleral buckling (SB) and pars plana vitrectomy (PPV) are the major surgical procedures for the treatment of RRD because of their high anatomical success rates,1,2 but still it is not fully elucidated which procedure is associated with a better functional and anatomical outcome.
Recently, there is a clear trend toward primary PPV as the first choice for the treatment of any type of RRD,3–5 despite the superiority of SB against PPV in uncomplicated retinal situations.6 In the traditional SB, the inverted small fundus image, the difficulty to identify tiny retinal breaks, and the inability to share the fundus information with medical staff are recognized as disadvantages.7–10 We speculate that these disadvantages may be one of the reasons that many surgeons prefer PPV over SB for the treatment of RRD.
In this study, we report the result of the modified SB using a combination of a noncontact wide-angle viewing system (Resight®; Carl Zeiss Meditec AG, Jena, Germany) and a cannula-based 25 G chandelier endoilluminator (Chandelier Lighting System; Alcon Laboratories, Inc., Fort Worth, TX, USA) as a fundus visualization system for the treatment of primary RRD.
Subjects and methods
We performed retrospective analyses of the medical records of 79 eyes of 79 patients with primary uncomplicated RRD who had underwent SB using a combination of a noncontact wide-angle viewing system and a cannula-based 25 G chandelier endoilluminator for fundus visualization during surgery. Our study was carried out based on the written informed consent from each patient, the approval of the institutional review board of Kobe Kaisei Hospital, and the tenets of the Declaration of Helsinki. Patients’ criteria included surgeries performed at Kobe Kaisei Hospital from April 2012 to May 2014. All surgeries were performed by two surgeons, HI and MT. Three ophthalmic residents in our hospital assisted all surgeries. HI is thought to be an experienced doctor who had experienced more than 1,000 vitreoretinal surgeries and more than 250 SB, and MT is thought to be an inexperienced doctor who had experienced less than 100 vitreoretinal surgeries and less than ten conventional SB. Patients were followed-up at least for 3 months after the surgery. The following variables were analyzed: sex, age, preoperative visual acuity, final visual acuity, follow-up period, primary surgeon, primary anatomical success rate, final anatomical success rate, lens status, number of retinal breaks, location of retinal breaks, number of quadrants involved, the presence or absence of the macular detachment, whether the external subretinal fluid drainage was performed or not, SB procedure, buckling material, and operative time.
Statistical methods
Univariate analysis was performed to establish the relationships between explanatory variables and the primary anatomic success rate, using Mann–Whitney U-test and chi-square test. The level of statistical significance was set at P<0.20. The variables found to be significant in univariate analysis were analyzed with backward logistic multiple regression analysis, using the MedCalc (MedCalc Version 12.7.5.0; MedCalc Software, Mariakerke, Belgium). Statistical significance was inferred for P<0.05.
Surgical procedures
All surgeries were performed under general anesthesia to eliminate patient’s pain during the surgery. After the induction of anesthesia, all procedures were performed using a surgical microscope (OPMI Lumera 700®; Carl Zeiss Meditec AG). After the sclera was exposed with a perilimbal conjunctival peritomy, extraocular rectus muscles were isolated. Traction sutures were placed with 3-0 Nurolon black underneath the isolated muscles. Mattress suture using 4-0 Mersilene was placed on the sclera. A 25 G trocar cannula with closure bulb (Chandelier lighting system; Alcon Laboratories, Inc.) was placed 4.0 mm behind the limbus. The position of the trocar cannula was chosen according to the localization of the break. When the break was at the inferior quadrant, the trocar cannula was positioned at 12 o’clock or vice versa.8 Subretinal fluid drainage through the external sclerotomy was performed under the surgical microscope. Resight® was activated. The chandelier endoilluminator was placed into the cannula and turned on. Observations and cryoretinopexies of original retinal breaks by dynamic scleral compression with a cryoprobe were performed. For buckling procedure, silicone band (#240; MIRA Inc, Waltham, MA, USA) with silicone sleeve (#270; MIRA Inc) combined with a silicone sponge (#506G; MIRA Inc) or a silicone tire (#287; MIRA Inc) was placed on the eye for 360° circumferential buckling, and silicone sponge (#506 or #503; MIRA Inc) or silicone tire (#287) was placed for the segmental buckling. The cannula with closure bulb did not make it difficult to rotate the eye during the buckling procedure. After the confirmation of the buckle position and whether or not unexpected complication is present on the fundus under Resight® with the endoilluminator, the cannula was removed and the vitreous herniation from the sclerotomy site was checked and cut if necessary. Surgery was completed by closing the conjunctiva.
Results
Table 1 summarizes the perioperative demographic data for the patients. There were 50 men and 29 women. The mean ± standard deviation (SD) age was 43.7±16.0 years. Their preoperative best-corrected visual acuity (BCVA) was 0.31±0.65 logMAR units. The final BCVA was 0.10±0.31 logMAR units, which was significantly better than the preoperative BCVA (P=0.0007, paired t-test). The mean ± SD follow-up period was 11.8±6.9 months. HI performed surgeries for 60 eyes and MT for 19 eyes. The initial and final anatomical success rates were 92.4% and 100%, respectively. Seventy-five eyes were phakic, three pseudophakic, and one aphakic. The mean ± SD number of retinal breaks was 1.5±0.8. Fifty eyes had original breaks at the superior quadrant and 27 had at the inferior quadrant. We could not find original breaks in two eyes. Twenty-eight eyes had RRD involving one or two quadrants. Fifty-one eyes had more extensive RRD with three or four quadrants of involvement. The macular was attached preoperatively in 43 (54.4%) eyes. Fifty-three eyes performed external subretinal fluid drainage and 26 did not. Twenty-one patients had undergone segmental buckling and 58 patients had 360° circumferential buckling. For SB, 56 eyes used silicone tire (#287), nine #506G, 13 #506, and one #503. For 360° circumferential buckling, silicone band (#240) with silicone sleeve (#270) was combined with a silicone sponge (#506G) or a silicone tire (#287). The mean ± SD operative time was 100.3±31.3 minutes.
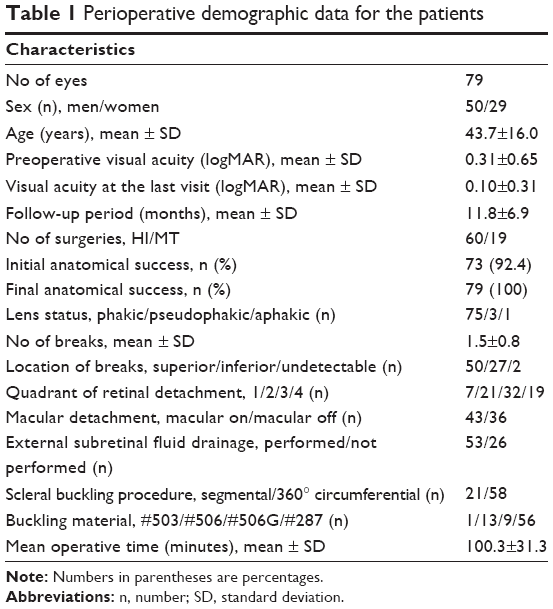 | Table 1 Perioperative demographic data for the patients |
We experienced intraoperative complications in seven eyes (Table 2). In five eyes, limited choroidal hemorrhage occurred during puncturing of the choroid for drainage of subretinal fluid through the external sclerotomy. We experienced two complications, which are thought to be related to the manipulation of the cannula-based chandelier endoilluminator. A new retinal break occurred at the diagonal part of the cannula just after the endoilluminator was removed from the cannula in one eye. Lens touch by the top of the chandelier endoilluminator happened during cryoretinopexy in another eye. Cataract progression had not been observed during the follow-up period. For limited choroidal hemorrhages and new retinal breaks, we performed additional cryoretinopexy and adjusted the buckling material to cover the lesion at the same session, if necessary. We experienced postoperative complications in seven eyes. Six eyes had retinal redetachments. We performed additional PPV with 20% sulfur hexafluoride gas tamponade for these eyes. Finally, all eyes had retinal attachment. One eye developed secondary glaucoma. Intraocular pressure decreased as a result of both trabeculectomy and the ablation of the #240 silicone band. Cataract progression was observed in one eye. We performed phacoemulsion and aspiration, and intraocular lens implantation for this eye.
 | Table 2 Details on patients with surgical complications |
As a result of univariate analysis (Table 3), the following variables were selected to perform backward logistic multiple regression analysis: sex, primary surgeon, number of quadrants involved, and operative time. The logistic multiple regression analysis revealed that all variables were not associated with the primary anatomic success (P=0.104; Table 3).
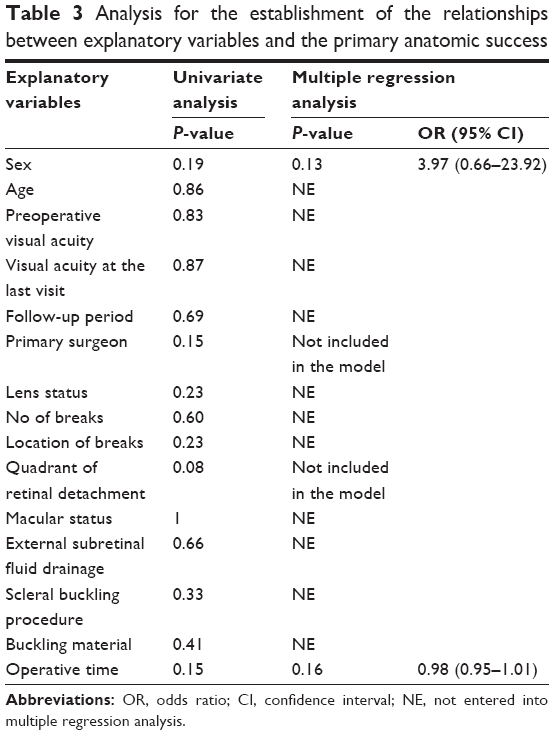 | Table 3 Analysis for the establishment of the relationships between explanatory variables and the primary anatomic success |
Discussion
Recently, several reports suggested the usefulness of SB using the wide-angle viewing system.7–10 Mutual advantages of wide-angle viewing system for SB are as follows: First, surgeons can easily visualize the fundus up to peripheral retina. Second, it is relatively easy to find small breaks that may be difficult to identify with an indirect ophthalmoscope. Finally, it is possible to share the fundus information with medical staff. Although both contact and noncontact types are available as the wide-angle viewing system and both slit lump and chandelier endoilluminator are available for the fundus illumination, a combination of noncontact wide-angle viewing system and cannula-based chandelier endoilluminator may be the best choice to visualize the fundus more stably and wider and to avoid the development of unneeded vitreous traction at the sclerotomy site for now.7–10
The primary anatomic success rate was 92.4% in this study. This rate was comparable with the previous reports, in which SB was performed both in the traditional manner3,11 and with a wide-angle viewing system.7,8 This result may support the positive use of this modified SB procedure in conjunction with the usefulness of this procedure listed earlier.
We performed logistic multiple regression analysis to establish the relationships between explanatory variables and the primary anatomic success. Although we could not find any association between these variables, the result that the primary anatomic success rate was not different between experienced and inexperienced surgeons is interesting. Many evidences about the correlation of the surgeon’s experience and better result for a variety of surgical procedures have been published. Regarding vitreoretinal surgery, Mazinani et al suggested that experience is a factor influencing the outcome of retinal detachment surgery in the beginning of the training period.12 Moreover, Kita et al, suggested the usefulness of SB with a wide-angle viewing system in surgical education.10 We consider that better fundus visualization and the ease of manipulation made it easier to identify retinal breaks and to determine the adequacy of the height and position of the buckling material and that these positive effects resulted in the better outcome.
However, we experienced two complications related to the manipulation of the cannula-based chandelier endoilluminator. Previous reports concerned about complications such as endophthalmitis due to possible vitreous wick from sclerotomy sites and lens damage by the endoilluminator.8–10 We actually experienced the development of a retinal break probably due to the vitreoretinal traction by the herniated vitreous from the sclerotomy site and lens touch by the endoilluminator. As mentioned in the previous reports, we should take caution to the manipulation of the chandelier endoilluminator and make it certain to remove the vitreous herniation from the sclerotomy site.
The major limitation of our study is that it is not prospective and does not have any control group. Therefore, it is difficult to address the advantage of this modified SB procedure compared to the traditional procedure. A large randomized comparative study will need to be undertaken to definitively determine whether this new SB procedure is superior to the traditional SB.
Conclusion
In conclusion, SB using a combination of a noncontact wide-angle viewing system combined and a cannula-based chandelier endoilluminator is a modified new technique and is promising for the management of RRDs. This procedure may be acceptable to both experienced and inexperienced surgeons who are in the beginning of the training period, but we should perform this procedure with the greatest care because there is a possibility of complication that we have never experienced in the traditional procedure.
Disclosure
The authors report no conflicts of interest in this work.
References
Miki D, Hida T, Hotta K, Shinoda K, Hirakata A. Comparison of scleral buckling and vitrectomy for retinal detachment resulting from flap tears in superior quadrants. Jpn J Ophthalmol. 2001;45:187–191. | ||
Kobashi H, Takano M, Yanagita T, et al. Scleral buckling and pars plana vitrectomy for rhegmatogenous retinal detachment: an analysis of 542 eyes. Curr Eye Res. 2014;39:204–211. | ||
Falkner-Radler CI, Myung JS, Moussa S, et al. Trends in primary retinal detachment surgery: results of a Bicenter study. Retina. 2011;31:928–936. | ||
Ho JD, Liou SW, Tsai CY, Tsai RJ, Lin HC. Trends and outcomes of treatment for primary rhegmatogenous retinal detachment: a 9-year nationwide population-based study. Eye (Lond). 2009;23:669–675. | ||
Wong CW, Wong WL, Yeo IY, et al. Trends and factors related to outcomes for primary rhegmatogenous retinal detachment surgery in a large Asian tertiary eye center. Retina. 2014;34:684–692. | ||
Adelman RA, Parnes AJ, Ducournau D. European Vitreo-Retinal Society (EVRS) Retinal Detachment Study Group: strategy for the management of uncomplicated retinal detachments: the European vitreo-retinal society retinal detachment study report 1. Ophthalmology. 2013;120:1804–1808. | ||
Ohji M, Tano Y. Vitreoretinal surgery with slit-lamp illumination combined with a wide-angle-viewing contact lens. Am J Ophthalmol. 2004;137:955–956. | ||
Aras C, Ucar D, Koytak A, Yetik H. Scleral buckling with a non-contact wide-angle viewing system. Ophthalmologica. 2012;227:107–110. | ||
Nam KY, Kim WJ, Jo YJ, Kim JY. Scleral buckling technique using a 25-gauge chandelier endoilluminator. Retina. 2013;33:880–882. | ||
Kita M, Fujii Y, Kawagoe N, Hama S. Scleral buckling with a noncontact wide-angle viewing system in the management of retinal detachment with undetected retinal break: a case report. Clin Ophthalmol. 2013;7:587–589. | ||
Heussen N, Feltgen N, Walter P, Hoerauf H, Hilgers RD, Heimann H. SPR Study Group: scleral buckling versus primary vitrectomy in rhegmatogenous retinal detachment study (SPR Study): predictive factors for functional outcome. Study report no 6. Graefes Arch Clin Exp Ophthalmol. 2011;249:1129–1136. | ||
Mazinani BA, Rajendram A, Walter P, Roessler GF. Does surgical experience have an effect on the success of retinal detachment surgery? Retina. 2012;32:32–37. |
 © 2015 The Author(s). This work is published and licensed by Dove Medical Press Limited. The
full terms of this license are available at https://www.dovepress.com/terms
and incorporate the Creative Commons Attribution
- Non Commercial (unported, 3.0) License.
By accessing the work you hereby accept the Terms. Non-commercial uses of the work are permitted
without any further permission from Dove Medical Press Limited, provided the work is properly
attributed. For permission for commercial use of this work, please see paragraphs 4.2 and 5 of our Terms.
© 2015 The Author(s). This work is published and licensed by Dove Medical Press Limited. The
full terms of this license are available at https://www.dovepress.com/terms
and incorporate the Creative Commons Attribution
- Non Commercial (unported, 3.0) License.
By accessing the work you hereby accept the Terms. Non-commercial uses of the work are permitted
without any further permission from Dove Medical Press Limited, provided the work is properly
attributed. For permission for commercial use of this work, please see paragraphs 4.2 and 5 of our Terms.