Back to Journals » Clinical, Cosmetic and Investigational Dermatology » Volume 15
Satisfactory Wound Reconstruction with a Local Rotation Flap After Removal of Large Penile Divided Nevi: Original Technique, Early and Mid-Term Results
Authors Wang P ![]() , Fan Y, Lian W, Su Y, Xiao H, Jia C
, Fan Y, Lian W, Su Y, Xiao H, Jia C
Received 23 July 2022
Accepted for publication 5 October 2022
Published 18 October 2022 Volume 2022:15 Pages 2203—2210
DOI https://doi.org/10.2147/CCID.S383514
Checked for plagiarism Yes
Review by Single anonymous peer review
Peer reviewer comments 2
Editor who approved publication: Dr Jeffrey Weinberg
Peng Wang,1,2,* Yueying Fan,2,* Wenqin Lian,2,* Yingjun Su,3 Hou’an Xiao,1 Chiyu Jia2
1Department of Burns and Plastic and Cosmetic Surgery, Xi’an Ninth Hospital, Xi’an, People’s Republic of China; 2Department of Burns and Plastic and Wound Repair Surgery, Xiang’an Hospital of Xiamen University, School of Medicine, Xiamen University, Xiamen, People’s Republic of China; 3Department of Burns and Plastic Surgery, Plastic Surgery Hospital, Xi’an International Medical Center, Xi’an, People’s Republic of China
*These authors contributed equally to this work
Correspondence: Chiyu Jia, Department of Burns and Plastic and Wound Repair Surgery, Xiang’an Hospital of Xiamen University, School of Medicine, Xiamen University, Xiamen, People’s Republic of China, Email [email protected] Hou’an Xiao, Department of Burns and Plastic and Cosmetic Surgery, Xi’an Ninth Hospital, Xi’an, People’s Republic of China, Email [email protected]
Objective: To investigate the application of local rotation flaps for reconstruction of divided nevi of the penises in young male patients.
Methods: A group of 8 patients of divided nevi of the penises who underwent wound reconstruction with local rotation flaps after surgical lesion removal was enrolled in a retrospective clinical study. Postoperative complication, sexual function and psychological traits were evaluated during the follow-up.
Results: All patients, with ages ranged from 16 to 32 years (mean 23.25 years), were followed up for 6 to 48 months (mean 19.86 months). The patient’s average length of hospital stay was 7.85 day (7 to 15 days). The average dimension of the lesions was (2.31± 0.44) × (1.46± 0.48) cm2 on the glans and (1.38± 0.40) × (1.01± 0.46) cm2 on the inner prepuce plate. All patients had no postoperative infection and were satisfied with the postoperative outcome upon discharge. Five cases of benign intradermal nevi and 3 cases of compound nevi without malignant transformation were confirmed by pathological evaluation on the removed samples. The sexual function of all patients was unaffected postoperatively by male sexual function scale (BMSFI and IIEF-5) evaluation. The psychological status of depression, anxiety and stress was all improved after the surgical reconstruction confirmed by the psychological traits scale (DASS) evaluation.
Conclusion: Reconstruction with the local rotation flap is a simple, safe and appropriate surgical procedure, achieves satisfactory cosmetic outcome, and maintains intact male sexual function when used for the repair of defect after removal of divided nevi of the penises.
Keywords: divided nevi, local rotation flap, genital plastic surgery, postoperative, follow-up
Introduction
Divided nevus of the penis is a relatively rare genital skin disease. The kissing or divided nevus was initially referred to as nevus that separates by upper and lower eyelids during embryological development. In 1998, Desruelles et al first reported a case of divided nevus located in the penis.1 Divided nevus of the penis, which is highly visible due to hyperpigmentation and the obvious aesthetical impact of the lesions, can seriously affect the quality of social life and psychological well-being of patients, especially if they are very young. The clinical diagnosis and treatment methods of divided nevus of the penis mainly include laser treatment, cryotherapy, chemical exfoliation, and surgery.2,3 Surgical resection of divided nevus of the penis, which albeit more invasive than alternative non-surgical options, is able to remove the lesions completely.4 Despite this main advantage of the surgical approach, the clinical risk linked to complications, post-operative erectile dysfunction, reduced glans sensitivity, and unsatisfactory aesthetic results of wound healing, can be not negligible. We describe a novel surgical technique using a local rotation flap to reconstruct the postoperative wound of the penis and investigate the early and mid-term results of postoperative complications, sexual function, and psychological traits, which give excellent cosmetic and functional results.
Materials and Methods
Patient Enrollment
In this retrospective study, 8 patients with divided nevi of the penis were operated on between January 2010 and July 2021. The mirror symmetrical pair of melanocytic nevi on the inner plate of prepuce and that on the glans were localized across the coronal sulcus. Exclusion criteria: (1): cases of malignant tumors at final pathology; (2): urinary infection, balanitis or impaired coagulation; (3): sexual dysfunction: (4): relevant medical co-morbidities.
Surgical Technique
After the skin was stretched to expose the lesions, a circular incision was made along the outer edge of the nevi on the glans and prepuce site, after local anesthesia with 2% lidocaine with epinephrine, 1:100,000 (Figures 1A and 2A). A local rotation flap was obtained beside the defect area of the prepuce inner plate and transferred to cover the secondary glans wounds. The wounds in the prepuce inner plates were closed by direct suturing (Figure 1B–D). When the divided nevus of the penis was located on ventral side, we preserved the skin of the inner plate below the glans to avoid excessive tension in the penile frenulum (Figure 2B–D). All cases were sutured intermittently with 5–0 no-absorbable polypropylene sutures with curved needles. Removal sutures on postoperative day 7 to 30 depending on postoperative recovery. All the operations were carried out by the same surgical team.
 |
Figure 1 Flap design and flowchart of Case 5. (A) Preoperative divided nevus position. (B) Lesion site excision extension. (C) Designed flap. (D) Immediate outcome after surgery. (E) The penis and glans position first day after surgery. (F) The penis and glans position about 6 months after surgery. (G) The penis and glans position about 27 months after surgery. (H and I), (H) Glans position, (I) Inner prepuce plate position. For the histopathology, HE staining indicated intradermal nevus under a magnification of 100×. |
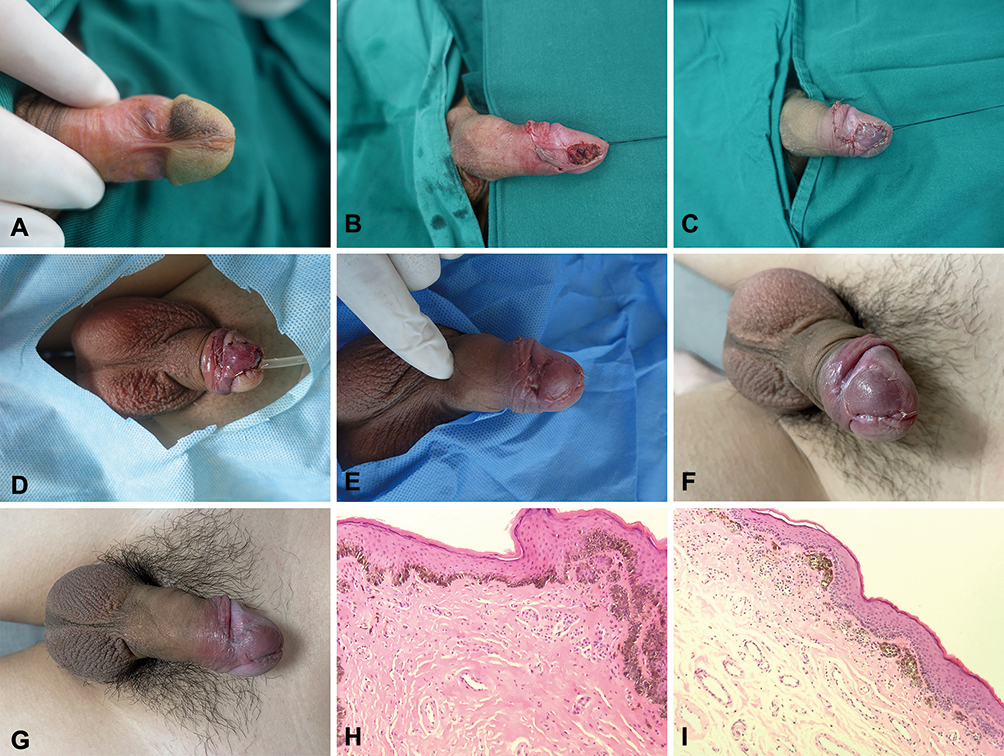 |
Figure 2 Flap design and flowchart of Case 8. (A) Preoperative divided nevus position. (B) Lesion site excision extension. (C) Immediate outcome after surgery. (D) The penis and glans position first day after surgery. (E) The penis and glans position 3rd day after surgery. (F) The penis and glans position about 1 month after surgery (Because of local tissue edema, the suture removal time was prolonged). (G) The penis and glans position about 6 months after surgery. (H and I), (H) Glans position, (I) Inner prepuce plate position. For the histopathology, HE staining indicated compound nevus under a magnification of 100×. Nevus cell nests at the dermo-epidermal junction and lower dermis. |
Postoperative Management and Follow-Up
Postoperative blood perfusion was assessed 1 hour after the reconstruction. The dressing change was applied for each wound every 2 days and the stitches were removed on the postoperative day 7. The follow-up scale, outpatient controls, and telephone follow-up calls were designed to assess the post-operative parameters, like the length of hospital stay, the incidence of complications, the Brief Male Sexual Function Inventory (BMSFI) score, and the International Index of Erectile Function-5 (IIEF-5) score, which were carefully recorded and evaluated. BMSFI consists of 11 questions with 5 possible responses scored on a scale of 0 (worst) to 4 (best), including sexual drive, erectile function, ejaculatory function, problem assessment and overall sexual satisfaction.5 The value of each domain reflects the simple algebraic sum of the scores of the underlying question(s) with lower domain scores indicating more severely impaired sexual function. The IIEF-5 represents a short version of the 15-item version of International Index of Erectile Function used to measure erectile function.6 Each item of IIEF-5 has a rating of 1 (very low; never) to 5 (very high; always), with a lower score indicating more erectile difficulties. Patients’ mental health was evaluated after the operation using the Depression Anxiety and Stress Scales (DASS), respectively. The DASS is a validated questionnaire that evaluates the psychological traits of depression, anxiety, and stress.7 The questionnaire has its recommended cut-off score for each subscale, which is 9 points for depression, 7 points for anxiety, and 14 points for stress.
H&E Staining
Paraffin-embedded divided nevi tissues were sectioned, underwent the processes of preparation of tissue slides followed by being deparaffinized with absolute xylene and dehydrated in a sequentially diluted ethanol buffer. The slides were then rehydrated with deionized water and stained with Hematoxylin dye for 20 min at room temperature. The slides were again rinsed with deionized water and fast dipped in 1% acid-ethanol solution. After rinsing with deionized water, the slides were stained with Eosin dye for 30s at room temperature, washed, mounted with DPX (xylene based), and covered with a coverslip, and observed under the light microscope.
Statistical Analysis
Data are expressed in Mean ± SD; Data were analyzed using paired t-tests (normal distribution) or paired Mann–Whitney U-tests (non-normal distribution) to compare the preoperative and postoperative scale score of same patient. P<0.05 was considered statistically significant.
Results
General Information
Education Level
In this patient group, one high school student and the other one who just graduated from senior high school were the youngest patients. Three patients graduated from University, and the other three patients were still studying for graduate degrees.
Sexual Life
All the patients had sex life except the two younger patients who lived asexually during the follow-up period.
Main Causes of Operation
The cause of operation in these patients was the abnormal appearance of the affected area, which affected their psychological status. On the evaluation of the preoperative psychological status of the enrolled patients, the results of DASS (Table 1) showed that 62.5% (5/8) patients had depression, including 12.5% (1/8) moderate and 50% (4/8) of mild depression. All the enrolled patients (8/8) had mild anxiety and 25% (2/8) had mild stress.
 |
Table 1 Patient Distributions in Different Types and Severity Categories of Psychological Traits Before Operation |
Follow-Up
All the patients were followed up for 6 months to 48 months (mean 19.86 months), and no recurrence was reported this period of time. The average dimension of the lesions was (2.31±0.44) × (1.46±0.48) cm2 on the glans and (1.38±0.40) × (1.01±0.46) cm2 on the inner prepuce plate. None of the lesions involved prepuce frenulum. The appearance of the flaps was similar to that of the surrounding skin (Figure 1E–G), and all patients were satisfied except one patient claimed that there might be local bloated and abnormal feeling on the surface of glans skin (Figure 2E–G). We compared patients pre- and postoperative sex functions (Table 2), and the results showed that there were significant differences in postoperative overall satisfaction (P=0.025) compared with pre-operation. Based on statistical analyses, there were no significant differences in the scores of sexual drive, erection, ejaculation, problem assessment, and IIEF-5 scores among these patients between pre- and post-operation (all P>0.05). Based on the results of DASS evaluation, except for one patient who had mild postoperative anxiety and stress, other patients had no signs of psychological issues of depression, anxiety and stress (Table 3).
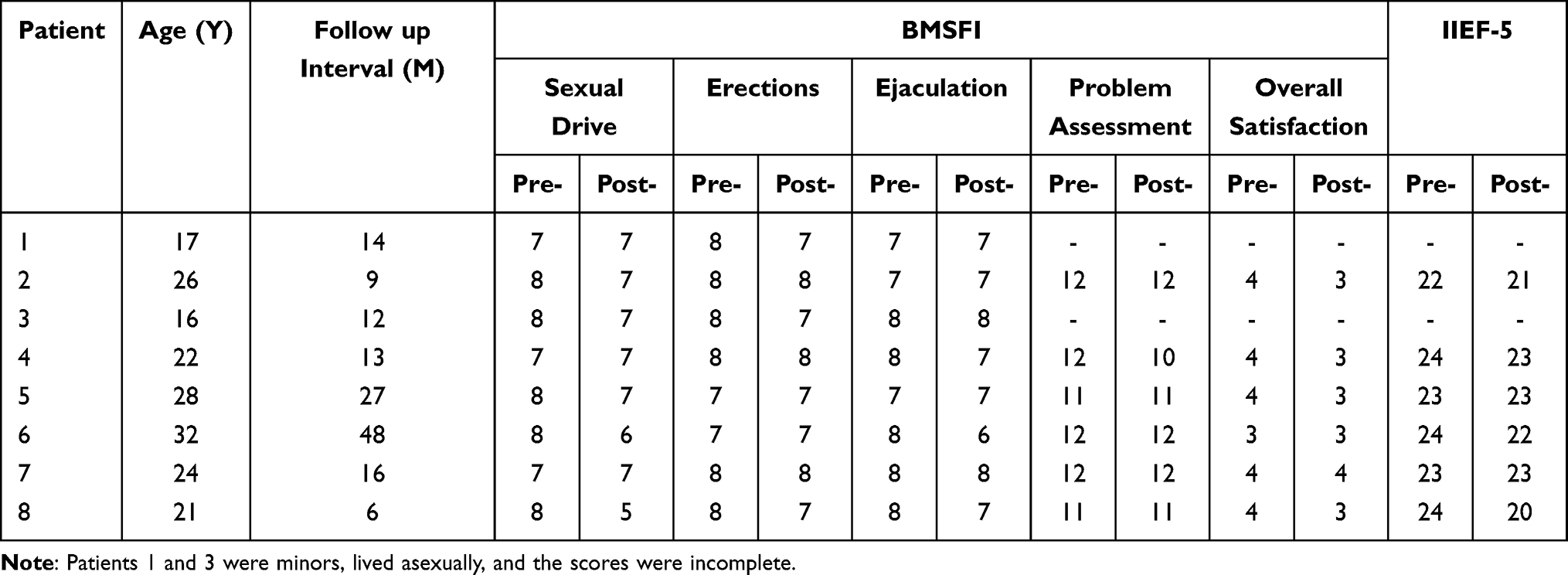 |
Table 2 The Sexual Function Scale (BMSFI and IIEF-5) Pre-Operation (Pre-) and Post-Operation (Post-) of 8 Patients |
 |
Table 3 Patient Distributions in Different Types and Severity Categories of Psychological Traits After Operation |
Patient Characteristics and Prognosis
The patient’s age ranged from 16 to 32 years (mean 23.25 years). The patient’s average length of hospital stay was 7.85 days (7 to 15 days). To avoid wound infection, all patients’ wounds were kept dry and clean with routine dressing change every 2–3 days. The patients were instructed to take oral estrogen (Estradiol Valerate Tablets, 1 mg/per day) to inhibit morning erection. The suture was removed at postoperative days 10~14, followed by evaluation of the penis function recovery. All wounds healed uneventfully except for one patient who had venous stagnation of the flap on the second postoperative day, which was relieved after the local puncture, drainage, and soaking the local skin with magnesium sulfate solution. For the diagnoses of the lesions, 5 cases of intradermal nevi (Figure 1H and I) and 3 cases of compound nevi (Figure 2H and I) were confirmed pathologically.
Discussion
Rare conditions of male genitalia, and other rare urological genital conditions, are currently being evaluated and approached by international multidisciplinary teams of experts, as a modern strategy to encourage optimal care and continuous recording of new techniques.8 Divided nevus of the penis is a kind of rare skin pigmented nevus.9 Because it is located on the skin surface of the male external genitalia, the divided nevus of the penis may have a negative impact on the psychology of patients themselves and sexual partners.10 In addition, with the gradual development of male sexual maturity and sexual behavior, the divided nevus of the penis has a certain risk of malignant transformation. Currently, the divided nevus of the penis is treated in many ways with varied efficacy. Yun et al and Bernardo et al treated the divided nevi of the penis with Nd: YAG laser or CO2 laser, but only for cases with small lesions.11,12 In cases with large foci, traditional surgical excision (resected the focus and sutured directly) may cause scarring and local abnormalities of the glans penises. Li et al reported a case in which circumcision and free inner prepuce grafting were utilized, but did not follow up the sexual function and satisfaction of the patient postoperatively.4
Completely remove the lesion, reduce the formation of scars and maintain the erection of the penis are the three key purposes for the surgical treatment. Congenital nevi cells exist in both the epidermis and dermis, and some infiltrate to deeper layer of dermis.13 It should be noted that the risk of malignant transformation of divided nevi of the penis is low, but not zero.14 Along with the sexual behavior after adulthood, the incidence of malignant transformation of divided nevi of the penis will increase under frequent stimulation. The pathological results of our present study showed that there were 3 cases of compound nevi, indicating the possibility of potential malignant transformation of divided nevi of the penis. Local rotation flap has achieved better results in the treatment of nasal reconstruction15 and hypospadias repair.16 Therefore, we treated divided nevi of the penis with extended lesion resection and local rotation flap, and followed these cases for a relatively long time after the operation. The results showed that all patients had no postoperative infection and were satisfied with the postoperative effects before discharge. It has been reported that skin grafts and local rotation flaps both have achieved good therapeutic effects in the treatment of eyelid-divided nevi.17 However, there is still the possibility of scar contracture in the treatment of divided nevi by skin transplantation.14 The skin of the inner prepuce is redundant, provides more elasticity, analogous texture, thickness, and color than skin grafts from other regions. The postoperative follow-up results showed that all patients were satisfied with the postoperative appearance except for one patient who has local mild edema (possibly because of the short follow-up period) and arose psychological state of mild anxiety and stress. Although the degree of “sexual pleasure” of inner plate of prepuce is lower than that of glans,18 the prepuce has rich sensory nerve endings19 and is easy to obtain, making it an ideal donor area of flap. The results of the functional evaluation in this study showed that the male sexual function was normal and unaffected postoperatively. With regard to the aspect of dissatisfaction, one patient complained that the local bloated shape, though mildly, of the glans might affect the self-confidence during sexual intercourse after the surgery.
Conclusion
Overall, the reconstruction by local rotation flap for wound defect after the removal of divided nevi of the penis in young male patients was satisfactory. Thus, this surgical technique could be suggested as a treatment method with an effective outcome for divided nevi of the penis. This article describes an original novel technique for tissue reconstruction after the removal of large penile divided nevi, which could be potentially applied also in the case of tissue reconstruction in the penis for other reasons. This represents a major advancement in the andrology, repair, and reconstruction surgery field.
Data Availability Statement
Data sharing not applicable to this article as no datasets were generated or analyzed during the current study.
Ethics Statement
The Ethics Committee of the Xi’an Ninth Hospital approved this study. Informed consent was collected from each enrolled patient whose pathological tissue paraffin specimens were used in this study.
Informed Consent for Photographs
All patients had signed an informed consent form and agreed to the use of the photographs for this study. All reported studies/experiments complied with all applicable ethical standards (including the Helsinki declaration and its amendments, institutional/national research committee standards, and international/national/institutional guidelines).
Acknowledgments
We would like to thank the staff of the Department of Burns and Plastic and Cosmetic Surgery, Xi’an Ninth Hospital, Department of Burns and Plastic and Wound Repair Surgery, Xiang’an Hospital of Xiamen University, for their help in this study. We would like to thank Ms. Haijing Lai for her help in this study.
Funding
The project was supported by the Open Project of Provincial Key Laboratory of Union Hospital Affiliated to Fujian Medical University (No. XHZDSYS202004 and No.XHZDSYS202103); Key Research and Development Plan of Shaanxi Province (No. S2021-YF-YBSF-0936); China Red Cross Foundation Xu Rongxiang Regenerative Life Public Welfare Fund Research Project (No. RXRL2021-05); Young Investigator Research Program of Xiang’an Hospital of Xiamen University (No. XM01120001).
Disclosure
The authors have no conflict of interest to disclose.
References
1. Desruelles F, Lacour JP, Mantoux F, Ortonne JP. Divided nevus of the penis: an unusual location. Arch Dermatol. 1998;134(7):879–880. doi:10.1001/archderm.134.7.879
2. Savas S, Balı YY, Erdemir AV, Simsek H. Divided nevus of the penis. Int J Dermatol. 2018;57(6):724–726. doi:10.1111/ijd.13899
3. Hardin CA, Tieu KD. Divided or kissing nevus of the penis. Dermatol Online J. 2013;19(10):20027. doi:10.5070/D31910020027
4. Li ZB, Liu T, Zhang QG, Hu JT. Treatment of divided nevus of the penis with circumcision and free inner prepuce grafting. Plast Reconstr Surg Glob Open. 2015;3(5):e389. doi:10.1097/GOX.0000000000000362
5. O’Leary MP, Fowler FJ, Lenderking WR, et al. A brief male sexual function inventory for urology. Urology. 1995;46(5):697–706. doi:10.1016/S0090-4295(99)80304-5
6. Rosen RC, Cappelleri JC, Smith MD, Lipsky J, Peña BM. Development and evaluation of an abridged, 5-item version of the International Index of Erectile Function (IIEF-5) as a diagnostic tool for erectile dysfunction. Int J Impot Res. 1999;11(6):319–326. doi:10.1038/sj.ijir.3900472
7. Henry JD, Crawford JR. The short-form version of the Depression Anxiety Stress Scales (DASS-21): construct validity and normative data in a large non-clinical sample. Br J Clin Psychol. 2005;44(Pt 2):227–239. doi:10.1348/014466505X29657
8. Oomen L, Leijte E, Shilhan DE, Battye M, Feitz WFJ. Rare and complex urology: clinical overview of ERN eUROGEN. Eur Urol. 2022;81(2):204–212. doi:10.1016/j.eururo.2021.02.043
9. Uehara M, Sato S, Kato A, et al. A rare case of pigmented epithelioid melanocytoma on the penis as a divided nevus. Eur J Dermatol. 2014;24(2):248–249. doi:10.1684/ejd.2014.2272
10. Godinho N, Nai GA, Schaefer ALF, Schaefer LV. Kissing nevus of the penis: a case report and dermatoscopic findings. An Bras Dermatol. 2017;92(5 Suppl 1):95–97. doi:10.1590/abd1806-4841.20175574
11. Yun SJ, Wi HS, Lee JB, Kim SJ, Won YH, Lee SC. Kissing nevus of the penis. Ann Dermatol. 2011;23(4):512–514. doi:10.5021/ad.2011.23.4.512
12. Correia B, Duarte AF, Haneke E, Correia O. CO(2) laser treatment of a kissing nevus of the penis: an alternative solution for a rare condition. J Dermatolog Treat. 2021;32(1):120–123. doi:10.1080/09546634.2019.1629384
13. Gu C, Wang XX, Luo X, et al. An alternative strategy treated giant congenital melanocytic nevi with epidermis and superficial dermis of the lesions. Medicine. 2018;97(4):e9725. doi:10.1097/MD.0000000000009725
14. Jia R, Zhu H, Lin M, et al. Clinicopathological characteristics and surgical outcomes of divided nevus of the eyelids: a decade’s experience on 73 cases. Ann Plast Surg. 2012;68(2):166–170. doi:10.1097/SAP.0b013e3182119155
15. Benoit A, Hollmig ST, Leach BC. The nasal tip rotation flap for reconstruction of the lateral nasal tip, anterior ala, and soft triangle: the authors’ experience with 55 patients. Dermatol Surg. 2017;43(10):1221–1232. doi:10.1097/DSS.0000000000001184
16. Patel RP, Shukla AR, Leone NT, Carr MC, Canning DA. Split onlay skin flap for the salvage hypospadias repair. J Urol. 2005;173(5):1718–1720. doi:10.1097/01.ju.0000154609.14084.5c
17. Schober JM, Meyer-Bahlburg HF, Dolezal C. Self-ratings of genital anatomy, sexual sensitivity and function in men using the ‘self-assessment of genital anatomy and sexual function, male’ questionnaire. BJU Int. 2009;103(8):1096–1103. doi:10.1111/j.1464-410X.2008.08166.x
18. Li X, Wang T, Li W, et al. 李秀琪, 王太玲, 李无言, 等. 眼睑分裂痣的手术方法选择. 中华整形外科杂志 [Surgical treatment of eyelid divided nevus]. Zhonghua Zheng Xing Wai Ke Za Zhi. 2015;31(2):96–99. Chinese. doi:10.3760/cma.j.issn.1009-4598.2015.02.005
19. Martín-Alguacil N, Cooper RS, Aardsma N, Mayoglou L, Pfaff D, Schober J. Terminal innervation of the male genitalia, cutaneous sensory receptors of the male foreskin. Clin Anat. 2015;28(3):385–391. doi:10.1002/ca.22501
 © 2022 The Author(s). This work is published and licensed by Dove Medical Press Limited. The
full terms of this license are available at https://www.dovepress.com/terms
and incorporate the Creative Commons Attribution
- Non Commercial (unported, 3.0) License.
By accessing the work you hereby accept the Terms. Non-commercial uses of the work are permitted
without any further permission from Dove Medical Press Limited, provided the work is properly
attributed. For permission for commercial use of this work, please see paragraphs 4.2 and 5 of our Terms.
© 2022 The Author(s). This work is published and licensed by Dove Medical Press Limited. The
full terms of this license are available at https://www.dovepress.com/terms
and incorporate the Creative Commons Attribution
- Non Commercial (unported, 3.0) License.
By accessing the work you hereby accept the Terms. Non-commercial uses of the work are permitted
without any further permission from Dove Medical Press Limited, provided the work is properly
attributed. For permission for commercial use of this work, please see paragraphs 4.2 and 5 of our Terms.