Back to Journals » Open Access Journal of Contraception » Volume 16
Satisfaction with the Levonorgestrel 19.5-mg Intrauterine Device Treatment for Heavy Menstrual Bleeding: A Pilot Study
Authors Viscola M, Marcelino ACH, Pereira PDC, Espejo-Arce X, Bahamondes L ![]()
Received 27 June 2025
Accepted for publication 23 September 2025
Published 10 October 2025 Volume 2025:16 Pages 123—129
DOI https://doi.org/10.2147/OAJC.S550056
Checked for plagiarism Yes
Review by Single anonymous peer review
Peer reviewer comments 3
Editor who approved publication: Professor Igal Wolman
Marco Viscola, Ana Claudia H Marcelino, Paula da Cunha Pereira, Ximena Espejo-Arce, Luis Bahamondes
Department of Obstetrics and Gynaecology, University of Campinas (UNICAMP), Faculty of Medical Sciences, Campinas, SP, Brazil
Correspondence: Luis Bahamondes, Department of Obstetrics and Gynaecology, University of Campinas (UNICAMP), Faculty of Medical Sciences, Caixa Postal 6181, Campinas, SP, 13084-971, Brazil, Tel +55 19 3289 2856, Fax +55 19 3289 2440, Email [email protected]
Introduction: Heavy menstrual bleeding (HMB) is usually treated with the levonorgestrel 52-mg intrauterine device (IUD), but if a lower-dose IUD would have similar efficacy on bleeding control mainly in the first years of use, the benefits of its dimensions could be attractive to women with narrow cervical canal. The purpose of our study was to evaluate clinical outcomes and satisfaction over one year in women with subjective complaints of HMB treated with the levonorgestrel 19.5-mg IUD.
Methods: We conducted a pilot study at the Department of Obstetrics and Gynaecology, University of Campinas, Faculty of Medical Sciences, Campinas, SP, Brazil. We enrolled 73 women who consulted with complaints of HMB and accepted the use of the levonorgestrel 19.5-mg IUD. We assessed satisfaction with the IUD one year after device placement using a questionnaire that subjectively evaluated HMB through quantity, predictability, cramps, overall satisfaction, desire to continue using the IUD and the possibility of recommending it to others. Additionally, healthcare providers (HCPs) reported on the ease of insertion during device placement, and we obtained data on women’s opinions regarding pain during insertion.
Results: Most women were satisfied or very satisfied with the levonorgestrel 19.5-mg IUD as a treatment for HMB, regarding bleeding quantity (n=51; 96.2%), predictability (n=43; 81.1%), and cramps (n=42; 79.2%) one year after device placement. Overall satisfaction was 98.1%. Furthermore, HCPs reported that it was easy to place (n=66; 90.4%) with varied pain at insertion.
Conclusion: The levonorgestrel 19.5-mg IUD was easy to insert with varied pain at insertion, and the satisfaction of women with their bleeding pattern one year after the device placement was high or very high.
Keywords: heavy menstrual bleeding, ease of placement, satisfaction, levonorgestrel intrauterine device, intrauterine device, Kyleena
Introduction
Although heavy menstrual bleeding (HMB) is well-defined for research purposes as the measurement of actual blood loss per menstrual period, and the gold standard is the measurement of alkaline hematin, the technique is expensive and not available in all settings. For this reason, the current recommendation values the routine clinical context based on the patient’s complaint to define it as excessive menstrual blood loss which the woman reports interfere with her physical, emotional, social, and material quality of life (QoL).1
The levonorgestrel 52-mg IUD is the best first-line treatment for reducing menstrual blood loss.2 Some benefits of a lower-dose IUD would be those related to its dimensions, which facilitate ease of insertion and cause less pain during the procedure.3 The levonorgestrel (LNG) 52-mg IUD is suitable for almost all medically eligible women, regardless of age or parity; however, the placement could be more difficult, and pain during the procedure seems to be greater in that group and in women with only previous caesarean deliveries.4–7 Furthermore, it is necessary to consider that differences in pain score at the time of placement of different IUDs could be statistically significant but not clinically relevant.8
A low dose and small size LNG 19.5-mg IUD was introduced in many markets with the advantage of better fitting women with thinner cervical canal.9,10 Considering that most of the strategies to reduce pain at device placement are not able to alleviate it,4 this new device with a thinner inserter tube would make insertion easier and less painful, especially among nulligravidas women.10,11 Moreover, this study is part of one of our groups that showed this IUD appears to be significantly useful in improving markers of anaemia, including haemoglobin, haematocrit, serum iron, and ferritin levels, compared to baseline evaluations among women with HMB during the first year of use.12 We conducted this pilot study with the objective of assessing satisfaction with this IUD among women with subjective HMB who accepted to use the LNG 19.5-mg IUD for one year and its ease of insertion and pain at placement.
Materials and Methods
We conducted a descriptive pilot study at the Department of Obstetrics and Gynaecology, University of Campinas, Faculty of Medical Sciences, Campinas, SP, Brazil, between July 2021 and April 2023. The university’s ethics committee approved the study protocol (CAAE # 45205721.1.0000.5404), our study complies with the Declaration of Helsinki, and all participants signed an informed consent form before enrolling in the study.
Women aged 18–48 years old who attended the clinic with complaints of HMB according to the self-perception of augmented bleeding by volume, which was interfering with their QoL and desiring the use of a low-dose levonorgestrel IUD rather than the LNG 52-mg IUD, which is commonly in use at our centre, were invited to participate. Exclusion criteria were pregnancy, congenital or acquired uterine abnormality, including fibroids if they distorted the uterine cavity or cervical canal and endometrial polyps, active pelvic inflammatory disease, recent deep vein thrombosis, and the use of illicit drugs.
After obtaining their demographic information, an HCP with extensive experience in IUD placement performed transvaginal ultrasonography to identify fibroids or polyps and the same professional placed the LNG 19.5-mg IUD (Kyleena®, Bayer Oy, Turku, Finland). The IUD was inserted after the HMB episode had ended. We did not use ultrasound to guide IUD placement or to confirm the correct IUD position at the end.
We evaluated the ease of placement in the opinion of the HCP who inserted the device, classifying the insertion as easy, difficult without dilators, difficult with dilators, or failed insertion. Furthermore, we assessed pain at insertion according to women’s opinions and scored from 0 to 10 on the visual analogue scale (VAS), reported as n (%), with scores ranging from 0–5 (mild to moderate) and 6–10 (moderate to intense). No pain killers were used before and during IUD placement. Women were instructed to return up to one year (±30 days) after device placement to answer a questionnaire of satisfaction with these questions:
- Since the beginning of the LNG IUD use, what is your satisfaction with the amount of monthly bleeding?
- Since the beginning of the LNG IUD use, what is your satisfaction with the predictability of monthly bleeding?
- Since the beginning of the LNG IUD use, what is your satisfaction with cramps during monthly bleeding?
- In general, what is your satisfaction with the LNG IUD?
- Do you want to continue using the LNG IUD?
- Would you recommend the LNG IUD to a friend or relative?
Participants’ satisfaction with bleeding patterns was assessed throughout the one-year observation period, including amenorrhea, spotting, and irregular bleeding. Satisfaction with predictability was defined as comfort with bleeding resembling a regular menstrual cycle. In cases of unpredictable but non-bothersome bleeding, participants were instructed to indicate satisfaction with monthly bleeding quantity but partial satisfaction with predictability. Independently of bleeding pattern, all participants were asked to evaluate the presence and intensity of cramps during the observation period. Possible answers to the first 4 questions were very dissatisfied, somewhat dissatisfied, neither satisfied nor dissatisfied, somewhat satisfied and very satisfied. Answers to the last 2 questions could be yes or no.
Women with partial or complete expulsion (partially in the cervical canal; or the IUD completely in the canal or vagina or IUD not found; identified at clinical visits) were offered removal of the IUD and its replacement by the LNG 52-mg IUD (which is the gold standard treatment for HMB in Brazil); however, they were discontinued from the study. The demographic and clinical characteristics of the women are presented as medians and interquartile ranges, as the data were not normally distributed. Ease of device placement was reported as n (%). Satisfaction of women was illustrated in a diverging stacked bar chart.
Results
We screened 740 women, and we enrolled 73. Table 1 shows their demographic characteristics. The mean age was 30.0 (range: 24–38) years, more than half were white and the median body mass index (BMI; kg/m2) was 27.0 (range 22.4–30.3). Of the enrolled women, 20 (27.4%) participants left the study due to being lost to follow-up (n = 12; 16.4%), expulsion (n = 7; 9.6%), or uterine perforation (n = 1; 1.4%) (Figure 1). One year after IUD placement, amenorrhoea (absence of any menstrual bleeding for at least 90 days) was reported by 10 (13.7%) women.
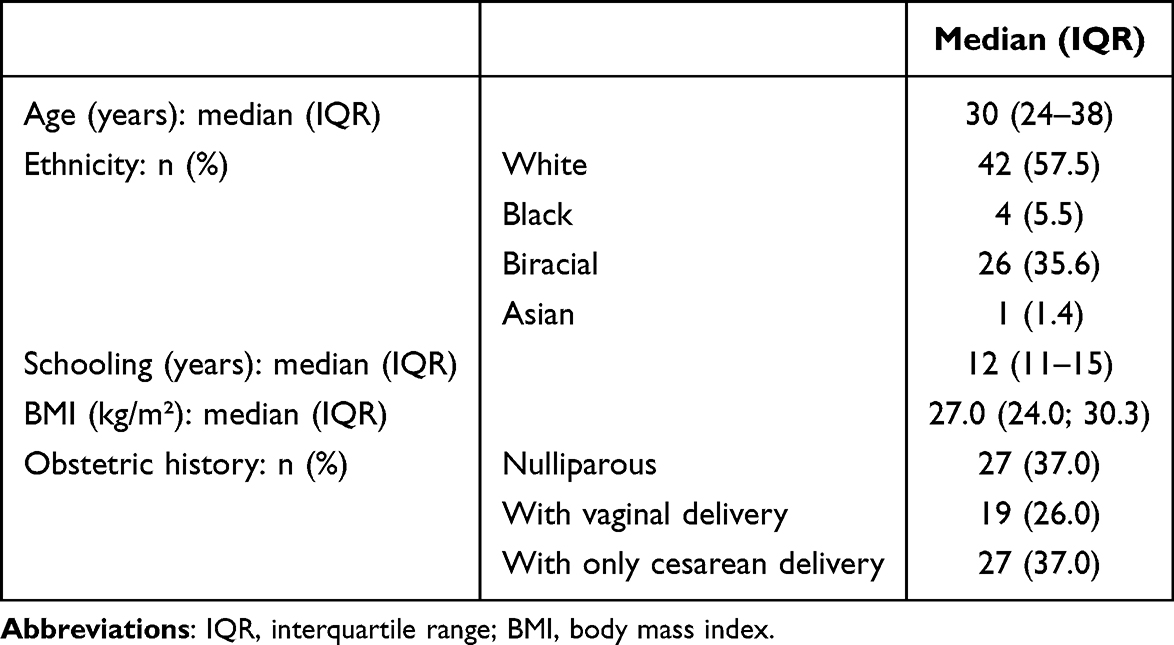 |
Table 1 Main Characteristics of Participants with Heavy Menstrual Bleeding, Users of the Levonorgestrel 19.5-mg Intrauterine Device at the University of Campinas, Brazil (n=73) |
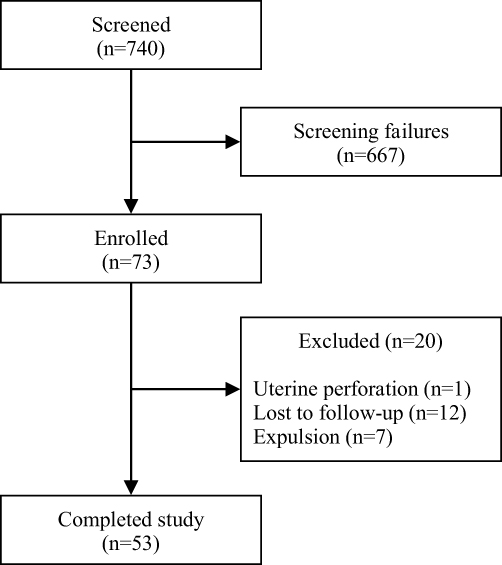 |
Figure 1 Study flow for participants in a study evaluating a levonorgestrel 19.5-mg intrauterine device among women who subjectively reported heavy menstrual bleeding (HMB) treatment. (n=73). |
Table 2 shows the obstetric history, ease of placement and pain at insertion of the LNG IUD. According to the HCPs, most of the women (n = 66; 90.4%) had an easy placement, but according to the VAS score, pain at insertion varied; 32 (43.8%) experienced mild to moderate pain and 41 (56.2%) reported moderate to intense pain.
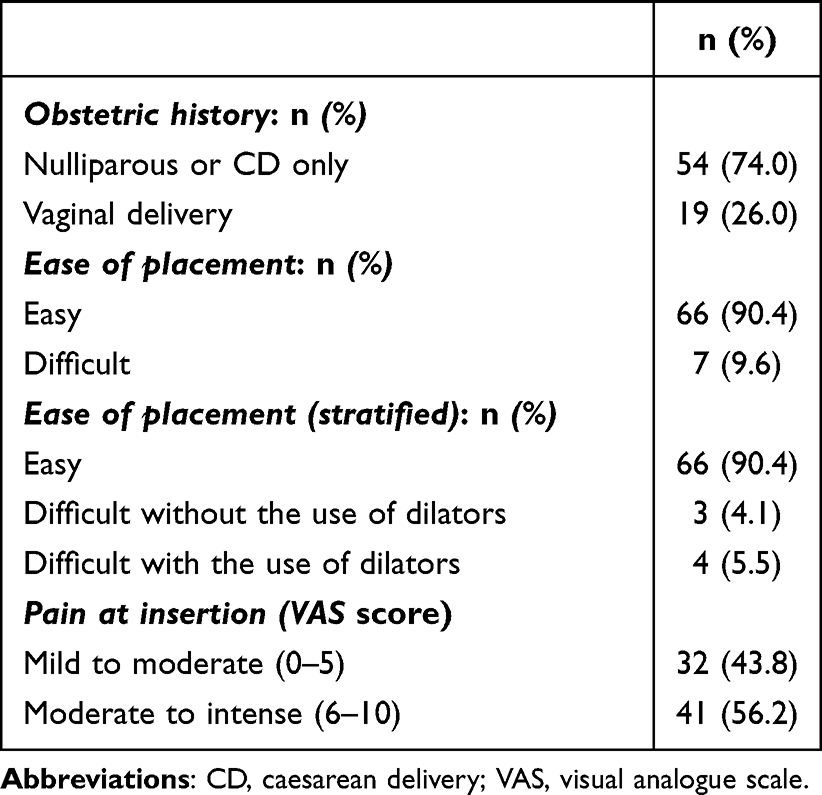 |
Table 2 Obstetric History, Ease of Placement and Pain at Insertion of Participants with Heavy Menstrual Bleeding Treated with the Levonorgestrel 19.5-mg Intrauterine Device, Campinas, Brazil. (n=73) |
In Figure 2 we showed participants´ satisfaction with the LNG IUD one year (±30/90 days) after device placement regarding uterine bleeding as quantity, predictability, cramps, and overall impression. Most women were satisfied or very satisfied with the method, and few were dissatisfied regarding predictability (n = 1; 0.02%) or cramps (n = 4; 0.07%). Others were somewhat dissatisfied regarding predictability (n = 4; 0.07%) or cramps (n = 3; 0.06%). Four women did not wish to continue the IUD use, two of them because of desire to become pregnant, and the other two did not provide any reason; however, all participants would recommend it to a friend or relative.
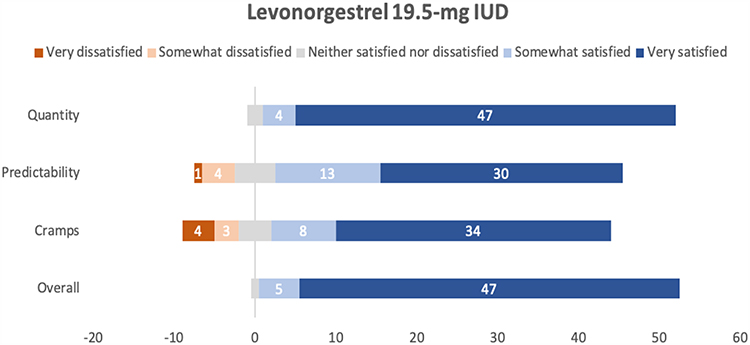 |
Figure 2 Satisfaction of levonorgestrel 19.5-mg IUD users one year after device placement according to bleeding patterns (n=53). |
Discussion
The LNG 19.5-mg IUD is currently approved for contraceptive use and has not been indicated for the management of HMB. To date, no comparative studies have been published evaluating the LNG 52-mg and LNG 19.5-mg IUDs in this context. Our pilot investigation assessed satisfaction among women with HMB using the LNG 19.5-mg IUD at one year following device placement.
Our study showed that most of the participants were satisfied or very satisfied with this IUD, and non-satisfied women reported they disliked the unpredictability of bleeding and cramps. Furthermore, the LNG 19.5-mg IUD was considered by HCPs as easy to place in women with HMB. There was considerable variability in pain perception even with the small width of the insertion tube (3.8 mm) as found with the LNG 52-mg IUD insertion tube (4.4 mm), highlighting that pain includes several sources like inserting the speculum, the tenaculum grasping of the cervix, the uterine sounding, eventual use of dilators, and the placement of the IUD more than the size of the insertion tube.
Although there is no contraindication for the use of any IUDs by nulligravidas or adolescents, those women, generally experienced more pain and eventually difficult insertion and since they usually have a tighter cervical canal, nulliparous could benefit from the LNG 19.5-mg IUD given it is smaller, and has an insertor 0.6 mm smaller compared with the LNG 52-mg IUD.6,13,14 Likewise, regarding parity, no difference in pain at IUD insertion was seen by others, though a recent study had shown intense pain at insertion more related to nulligravidas than parous women and higher pain with the LNG 52-mg IUD than with the copper-IUD (TCu380A).4,15,16
It is also worth noting that, although there is controversial evidence to support the routine use of topical lidocaine injected into the cervix, pre-insertion oral misoprostol or nonsteroidal anti-inflammatory drugs for reducing pain during insertion of an IUD, the use of topical lidocaine spray should be further evaluated.4,17,18 A recent review showed that more important than pharmacological actions is to consider the characteristics of the women and the guidance, anticipated pain and support provided by the HCP involved in the procedure.19
The unexpectedly high rate of expulsion was an issue in this study. In a previous report of our group, in which the IUD was placed during the acute bleeding episode, the possibility of expulsion was high, and the high incidence of expulsion in women with HMB was also seen by others.20–22 However, in a recent report, we found a similar expulsion rate among women who received the LNG 52-mg IUD due to contraception or as treatment of HMB.23 The high expulsion rate could have affected the number of women dissatisfied with the IUD, but some of them required replacement of the IUD, which denotes satisfaction, and even some who did not want to continue the IUD use would recommend it to a friend or relative. That agrees with the high continuation rate, an indicator of user satisfaction, observed with the LNG 19.5-mg IUD.24
Our study found high rates of satisfaction with the LNG 19.5-mg IUD among women with HMB; however, apparently, bleeding control requires higher levels of levonorgestrel and maybe, in the last years of this IUD life span, the amount of steroid released could not ensure adequate bleeding control, diminishing satisfaction over time, and other studies could evaluate this issue.
The main strength of our study is that this is the first to assess the satisfaction of users with HMB regarding the levonorgestrel 19.5-mg IUD since the usual treatment of that condition is the levonorgestrel 52-mg IUD. Limitations include the small sample size, the relatively high rate of losses (follow-up and expulsion), the inability to correlate HMB reduction with the use of the LNG 19.5-mg IUD by one year because we did not use a quantitative method such as alkaline haematin to determine the actual blood loss and the lack of a comparison group of women. Nevertheless, the satisfaction of users was considered in the recent definition of HMB, which assumed the woman’s perception of physical, emotional, social, and material interference in her QoL.
Since satisfaction does not necessarily equate to clinical efficacy in controlling bleeding without objective measures, future research directions could better compare the LNG 19.5-mg with the LNG 52-mg IUDs in the treatment of HMB and address the limitations of our study with adequate sample size and an objective method of bleeding measurement: quantitative (alkaline hematin) or semiquantitative (PBAC).
Conclusion
The use of the LNG 19.5-mg IUD among women with subjectively HMB was easy to place with varied pain, and it was associated with high satisfaction by one year after device placement. More studies should evaluate how the LNG 52-mg IUD and the LNG 19.5-mg IUD are comparable on bleeding control and show for how long the latter could be used to treat HMB.
Abbreviations
HCP, healthcare provider; HMB, heavy menstrual bleeding; IUD, intrauterine device; QoL, quality of life; VAS, visual analogue scale.
Data Sharing Statement
The datasets used or analyzed in the current study are available from the corresponding author upon reasonable request.
Ethics Approval and Informed Consent
The university’s ethics committee approved the study protocol (CAAE # 45205721.1.0000.5404), our study complies with the Declaration of Helsinki, and all participants signed an informed consent form before enrolling in the study.
Acknowledgments
To Sara Xavier Lima Castro for her work on data collection, Andréia Ribeiro da Silva Gonçalves for contacting participants and Helymar da Costa Machado for his work on statistical analysis. All of them work at the University of Campinas (UNICAMP), Faculty of Medical Sciences and do not have any conflict of interest.
Author Contributions
All authors made a significant contribution to the work reported, whether that is in the conception, study design, execution, acquisition of data, analysis and interpretation, or in all these areas; took part in drafting, revising or critically reviewing the article; gave final approval of the version to be published; have agreed on the journal to which the article has been submitted; and agree to be accountable for all aspects of the work.
Funding
This study received partial financial support from Fundação de Apoio à Pesquisa do Estado de São Paulo (FAPESP) award No. 2015/20504-9 and from the Brazilian National Research Council (CNPq) grant No. 573747/2008-3. The funders had no role in the study design, data collection, data analysis, data interpretation, manuscript writing or the decision to submit the manuscript for publication.
Disclosure
LB received an honorarium as a speaker from Bayer, Merck and Organon. The other authors declare no conflicts of interest.
References
1. Fraser IS, Critchley HO, Broder M, Munro MG. The FIGO recommendations on terminologies and definitions for normal and abnormal uterine bleeding. Semin Reprod Med. 2011;29(5):383–390. doi:10.1055/s-0031-1287662
2. Bofill Rodriguez M, Dias S, Jordan V, et al. Interventions for heavy menstrual bleeding; overview of Cochrane reviews and network meta-analysis. Cochrane Database Syst Rev. 2022;5(5):Cd013180. doi:10.1002/14651858.CD013180.pub2
3. Goldstuck ND. Clarification of the role of the Jaydess(Skyla) LNG- IUS 13.5mg and Kyleena LNG-IUS 19.5mg as intrauterine contraceptive systems. Expert Rev Med Devices. 2017;14(8):593–599. doi:10.1080/17434440.2017.1350169
4. Lopes-Garcia EA, Carmona EV, Monteiro I, Bahamondes L. Assessment of pain and ease of intrauterine device placement according to type of device, parity, and mode of delivery. Eur J Contracept Reprod Health Care. 2023;28(3):163–167. doi:10.1080/13625187.2023.2189500
5. Bahamondes MV, Hidalgo MM, Bahamondes L, Monteiro I. Ease of insertion and clinical performance of the levonorgestrel-releasing intrauterine system in nulligravidas. Contraception. 2011;84(5):e11–6. doi:10.1016/j.contraception.2011.05.012
6. Mansour D. The benefits and risks of using a levonorgestrel-releasing intrauterine system for contraception. Contraception. 2012;85(3):224–234. doi:10.1016/j.contraception.2011.08.003
7. Chaves IA, Baêta T, Dolabella GB, et al. Pain scores at the insertion of the 52 MG levonorgestrel-releasing intrauterine system among nulligravidas and parous women. Eur J Contracept Reprod Health Care. 2021;26(5):399–403. doi:10.1080/13625187.2021.1925882
8. Anjos F, Marcelino AC, Espejo-Arce X, et al. Pain and ease of insertion of three different intrauterine devices in Brazilian adolescents: a participant-blinded randomized trial. Contraception. 2023;122:109997. doi:10.1016/j.contraception.2023.109997
9. Gemzell-Danielsson K, Apter D, Hauck B, et al. The effect of age, parity and body mass index on the efficacy, safety, placement and user satisfaction associated with two low-dose levonorgestrel intrauterine contraceptive systems: subgroup analyses of data from a phase III trial. PLoS One. 2015;10(9):e0135309. doi:10.1371/journal.pone.0135309
10. Gemzell-Danielsson K, Apter D, Dermout S, et al. Evaluation of a new, low-dose levonorgestrel intrauterine contraceptive system over 5 years of use. Eur J Obstet Gynecol Reprod Biol. 2017;210:22–28. doi:10.1016/j.ejogrb.2016.11.022
11. Marions L, Lövkvist L, Taube A, Johansson M, Dalvik H, Øverlie I. Use of the levonorgestrel releasing-intrauterine system in nulliparous women--a non-interventional study in Sweden. Eur J Contracept Reprod Health Care. 2011;16(2):126–134. doi:10.3109/13625187.2011.558222
12. Viscola M, Marcelino AC, da CPP, Monteiro I, Espejo-Arce X, Bahamondes L. Improvement of laboratory markers of anaemia in the treatment of heavy menstrual bleeding with a 19.5-mg intrauterine device: a pilot study. Eur J Contracept Reprod Health Care. 2024;29:1–5. doi:10.1080/13625187.2023.2284085
13. Adeyemi-Fowode OA, Bercaw-Pratt JL. Intrauterine devices: effective contraception with noncontraceptive benefits for adolescents. J Pediatr Adolesc Gynecol. 2019;32(5s):S2–S6. doi:10.1016/j.jpag.2019.07.001
14. Gemzell-Danielsson K, Schellschmidt I, Apter D. A randomized, Phase II study describing the efficacy, bleeding profile, and safety of two low-dose levonorgestrel-releasing intrauterine contraceptive systems and Mirena. Fertil Steril. 2012;97(3):
15. Kaislasuo J, Heikinheimo O, Lähteenmäki P, Suhonen S. Predicting painful or difficult intrauterine device insertion in nulligravid women. Obstet Gynecol. 2014;124(2 Pt 1):345–353. doi:10.1097/AOG.0000000000000362
16. Santos AR, Bahamondes MV, Hidalgo MM, Atti A, Bahamondes L, Monteiro I. Pain at insertion of the levonorgestrel-releasing intrauterine system in nulligravida and parous women with and without cesarean section. Contraception. 2013;88(1):164–168. doi:10.1016/j.contraception.2012.10.015
17. Marcelino AC, da Cunha Pereira P, Charles CM, Espejo-Arce X, Bahamondes L. Pain relief during intrauterine device placement in nulligravid women with both oral ketorolac and an analgesic: a double-blinded randomised trial. Eur J Contracept Reprod Health Care. 2024;29(6):276–281. doi:10.1080/13625187.2024.2398440
18. Curtis KM, Nguyen AT, Tepper NK, et al. U.S. Selected practice recommendations for contraceptive use, 2024. MMWR Recomm Rep. 2024;73(3):1–77.
19. Bayer LL, Ahuja S, Allen RH, et al. Best practices for reducing pain associated with intrauterine device placement. Am J Obstet Gynecol. 2025;232:409–421. doi:10.1016/j.ajog.2025.01.039
20. Diaz J, Bahamondes L, Monteiro I, Petta C, Hildalgo MM, Arce XE. Acceptability and performance of the levonorgestrel-releasing intrauterine system (Mirena) in Campinas, Brazil. Contraception. 2000;62(2):59–61. doi:10.1016/S0010-7824(00)00140-2
21. Hidalgo M, Bahamondes L, Perrotti M, Diaz J, Dantas-Monteiro C, Petta C. Bleeding patterns and clinical performance of the levonorgestrel-releasing intrauterine system (Mirena) up to two years. Contraception. 2002;65(2):129–132. doi:10.1016/S0010-7824(01)00302-X
22. Youm J, Lee HJ, Kim SK, Kim H, Jee BC. Factors affecting the spontaneous expulsion of the levonorgestrel-releasing intrauterine system. Int J Gynaecol Obstet. 2014;126(2):165–169. doi:10.1016/j.ijgo.2014.02.017
23. Furlani RM, Garcia E, Castro S, Machado HC, Bahamondes L, Monteiro I. Expulsion rates of the levonorgestrel 52 mg intrauterine system are similar among women with heavy menstrual bleeding and users for contraception. Contraception. 2022;105:75–79. doi:10.1016/j.contraception.2021.09.001
24. Stovall DW, Aqua K, Römer T, et al. Satisfaction and continuation with LNG-IUS 12: findings from the real-world kyleena(®) satisfaction study. Eur J Contracept Reprod Health Care. 2021;26(6):462–472. doi:10.1080/13625187.2021.1975268
 © 2025 The Author(s). This work is published and licensed by Dove Medical Press Limited. The
full terms of this license are available at https://www.dovepress.com/terms
and incorporate the Creative Commons Attribution
- Non Commercial (unported, 4.0) License.
By accessing the work you hereby accept the Terms. Non-commercial uses of the work are permitted
without any further permission from Dove Medical Press Limited, provided the work is properly
attributed. For permission for commercial use of this work, please see paragraphs 4.2 and 5 of our Terms.
© 2025 The Author(s). This work is published and licensed by Dove Medical Press Limited. The
full terms of this license are available at https://www.dovepress.com/terms
and incorporate the Creative Commons Attribution
- Non Commercial (unported, 4.0) License.
By accessing the work you hereby accept the Terms. Non-commercial uses of the work are permitted
without any further permission from Dove Medical Press Limited, provided the work is properly
attributed. For permission for commercial use of this work, please see paragraphs 4.2 and 5 of our Terms.