Back to Journals » Clinical Ophthalmology » Volume 20
Satisfaction and Visual Outcomes with a Non-Diffractive EDOF IOL in Post-Myopic LASIK and PRK Patients with High Corneal Spherical Aberration
Authors Micheletti JM ![]() , Hall B
, Hall B ![]()
Received 11 September 2025
Accepted for publication 16 December 2025
Published 8 January 2026 Volume 2026:20 566800
DOI https://doi.org/10.2147/OPTH.S566800
Checked for plagiarism Yes
Review by Single anonymous peer review
Peer reviewer comments 3
Editor who approved publication: Dr Bharat Gurnani
J Morgan Micheletti,1 Brad Hall2
1Berkeley Eye Center, Houston, TX, USA; 2Sengi, Penniac, NB, Canada
Correspondence: J Morgan Micheletti, Berkeley Eye Center, 3100 Weslayan, Suite 400, Houston, TX, USA, Tel +1-713-526-1600, Email [email protected]
Purpose: To evaluate patient satisfaction and visual outcomes with extended depth of focus (EDOF) intraocular lens (IOL) implantation in post myopic refractive surgery patients with high corneal spherical aberrations.
Methods: This was a non-interventional, observational, ambispective, bilateral, single center multi-surgeon study. Patients had history of myopic LASIK or PRK, and relatively high corneal spherical aberrations, and were bilaterally implanted with Vivity or Vivity toric EDOF IOLs targeting emmetropia. Endpoints included monocular and binocular uncorrected and distance corrected visual acuities at distance (UDVA, CDVA), intermediate (UIVA, DCIVA; 66cm), and near (UNVA, DCNVA; 40cm), binocular defocus curve, and patient satisfaction (IOLSAT) and visual disturbance (QUVID) questionnaires.
Results: A total of 20 subjects (40 eyes) completed the study. Mean binocular UDVA, UIVA, and UNVA were 0.02 ± 0.16 logMAR, 0.14 ± 0.13 logMAR, and 0.24 ± 0.14 logMAR, respectively. The percentages of eyes with mean residual spherical equivalent and residual astigmatism ≤ 0.50 D were 95% (38/40) and 98% (39/40), respectively. On the QUVID questionnaire, 0% (0/20), 5% (1/20), and 0% (0/20) of patients reported being “Bothered quite a bit” or “Bothered very much” by halo, starbursts, or glare, respectively. On the IOLSAT, patient reported spectacle use was “Never” or “Rarely” in 90% (18/20), 75% (15/20), and 30% (6/20) of patients at distance, intermediate, and near, respectively.
Conclusion: Results suggest good visual outcomes at distance, intermediate and functional near vision and high patient satisfaction with Vivity and Vivity toric IOL implantation in post myopic refractive surgery patients with high corneal spherical aberrations.
Keywords: Vivity, EDOF, cataract surgery, post-refractive
Introduction
One of the most common elective procedures performed in ophthalmology is laser vision correction (LVC). The three general types are photorefractive keratectomy (PRK), laser in situ keratomileusis (LASIK), and, relatively recently, keratorefractive lenticule extraction (KLEx). As LVC was introduced more than 30 years ago, many of these patients have since developed cataracts and require surgery and intraocular lens (IOL) implantation. Patients who have undergone LVC, which provides spectacle independence prior to the onset of presbyopia, may wish to retain or return to spectacle independence following cataract surgery. Therefore, careful consideration of the IOL to implant is needed.
One option would be to implant a trifocal IOL, which can provide clear vision at distance, intermediate, and near by splitting incoming light into 3 distinct foci. However, multifocal IOLs, including trifocal IOLs, use diffractive technology, which may cause unwanted photic phenomena such as halos and glare.1,2 In addition, LVC alters the curvature of the cornea as well as corneal anterior/posterior curvature ratio, making lens power calculation less accurate. Current IOL power calculation formulas may only achieve less than 70% of post-LVC eyes within ± 0.50 D of the target refraction.3,4 Missing the refractive target may impact trifocal IOL recipients more than monofocal patients, although it is worth noting that a few studies have reported successful outcomes implanting trifocal IOLs in post-myopic LASIK and PRK eyes,5–8 and that this author (JMM) routinely uses trifocal IOLs in appropriate post-myopic LVC patients. Furthermore, post-LVC eyes may have high corneal aberrations prior to cataract surgery, which can make it even more challenging to achieve good visual outcomes.9
Another IOL option to implant would be an extended depth of focus (EDOF) IOL. Rather than creating distinct foci, EDOF IOLs aim to create one continuous focal point, enabling clear vision at distance, intermediate and functional vision at near.10,11 Compared to diffractive multifocal or diffractive EDOF IOLs, non-diffractive EDOF IOLs have less photic phenomena.12,13 In addition, missing the refractive target may be less impactful on final visual outcomes compared to a multifocal IOL.14 Indeed, there are reports of successful outcomes with EDOF IOLs in post-LVC eyes.15–17
The AcrySof® IQ and Clareon Vivity IOLs (Alcon Vision, LLC, Fort Worth, Texas, USA) create an EDOF effect using wavefront shaping technology.18 The shaping is done using two surface transition elements on the anterior surface that stretches and shifts, but does not split nor bend, the emerging wavefront to provide an extended depth of focus.19 Visual outcomes including extended range of vision and low visual disturbances have been reported with the Vivity IOL in normal cataract patients.13,20,21 However, studies of outcomes with the Vivity in post-LVC eyes are lacking. In addition, many surgeons consider high spherical aberration as an exclusion to implanting presbyopia correcting IOLs, such as diffractive trifocal and EDOF lenses. The purpose of this study was to evaluate patient satisfaction and visual outcomes with bilateral AcrySof® IQ or Clareon Vivity implantation in post myopic refractive surgery patients with high corneal spherical aberrations.
Methods
This was a non-interventional, observational, ambispective, bilateral, single center multi-surgeon study of patient reported satisfaction and visual outcomes following bilateral implantation of the Vivity IOL in post-refractive patients. An independent institutional review board reviewed and approved the study (WCG, approval number 1337766). All subjects gave written informed consent. The study was registered in a clinical trials database (NCT06064916) and was conducted in compliance with international harmonization guidelines, good clinical practice, and the tenets of the Declaration of Helsinki. Data are not available for sharing.
Uncomplicated phacoemulsification and implantation with the Vivity IOL were performed by four surgeons at a single private practice. Subjects selected their desired IOL after discussion with the surgeon prior to surgery. All eyes were targeted for emmetropia and the Barrett II Universal or Kane formulas were used for IOL calculation with physician optimized A-constants. Cataract surgery and IOL implantation were performed in the second eye within two weeks following surgery in the first eye.
Subjects enrolled were adults (40 years of age or older) having already undergone uncomplicated cataract removal by phacoemulsification with a clear corneal incision in both eyes and implantation of bilateral Vivity IOLs, with prior uncomplicated bilateral myopic LASIK or PRK surgery achieving optimal distance vision in both eyes, corneal spherical aberration (SA) between 0.30 µ and 1.20 µ inclusive in at least one eye prior to cataract surgery (measured with the Atlas 9000, Carl Zeiss Meditec AG), corrected distance visual acuity (CDVA) of 0.10 logMAR or better, minimum of two weeks post neodymium-doped yttrium aluminum garnet (Nd:YAG) laser capsulotomy for posterior capsule opacification (PCO) treatment, residual refractive astigmatism ≤0.50 D following cataract surgery (in at least one eye), and post-cataract surgery refractive spherical equivalent of 0.00 ± 0.50 D (in at least one eye). The strict inclusion criteria were designed to limit confounders and maximally explore the impact of high SA on outcomes with the Vivity IOL. Subjects were excluded who had any corneal abnormality (other than LASIK surgery or regular corneal astigmatism, any complication during cataract surgery, retinal conditions or predisposition to retinal conditions or anterior or posterior segment inflammation of any etiology, amblyopia or strabismus in either eye, any neovascularization on or within the eye, glaucoma or other optic nerve atrophy, diagnosed degenerative eye disorders, or systemic illness likely to confound the study results.
Subjects meeting the inclusion/exclusion criteria above were identified by retrospective review of consecutive charts between July 2023 and December 2024. Subjects attended 1 visit, at least 3 months after their second eye surgery. Assessments included monocular and binocular uncorrected and distance corrected visual acuities at distance (UDVA, CDVA), intermediate (UIVA, DCIVA; 66 cm), and near (UNVA, DCNVA; 40) using Early Treatment Diabetic Retinopathy Study (ETDRS) charts, subjective refraction, binocular distance corrected defocus curve, and administration of two proprietary (Alcon Vision, LLC) and validated questionnaires. The first was the questionnaire for visual disturbances (QUVID), which asks subjects to rate the frequency, severity, and bothersomeness of different dysphotopsias. The second was the intraocular lens satisfaction questionnaire (IOLSAT), which asks subjects to rate their satisfaction, spectacle independence, and visual performance at distance, intermediate, and near under different lighting conditions. Exploratory endpoints included SA correlation to responses on the QUVID and SA correlation to visual outcomes, and p-values were adjusted using Benjamini–Hochberg. A p-value ≤0.05 after adjustment was considered significant. All statistical analyses were performed using R (version 4.4.2; The R Foundation for Statistical Computing, Vienna, Austria). The trapezoidal numerical integration method was used to calculate areas under the curve for the binocular defocus curve, normalizing the 0.5 defocus steps and using a functional vision cutoff of 0.2 logMAR. The total defocus range was +1.00 D to −3.00 D, including +0.50 D to −0.50 D for far, −0.50 D to −2.00 D for intermediate, and −2.00 D to −3.00 D for near.
Results
Table 1 summarizes the baseline (prior to cataract surgery) and demographic data. A total of 20 subjects completed the study, including 45% (9/20) female subjects and 40% (16/40) non-toric IOLs.
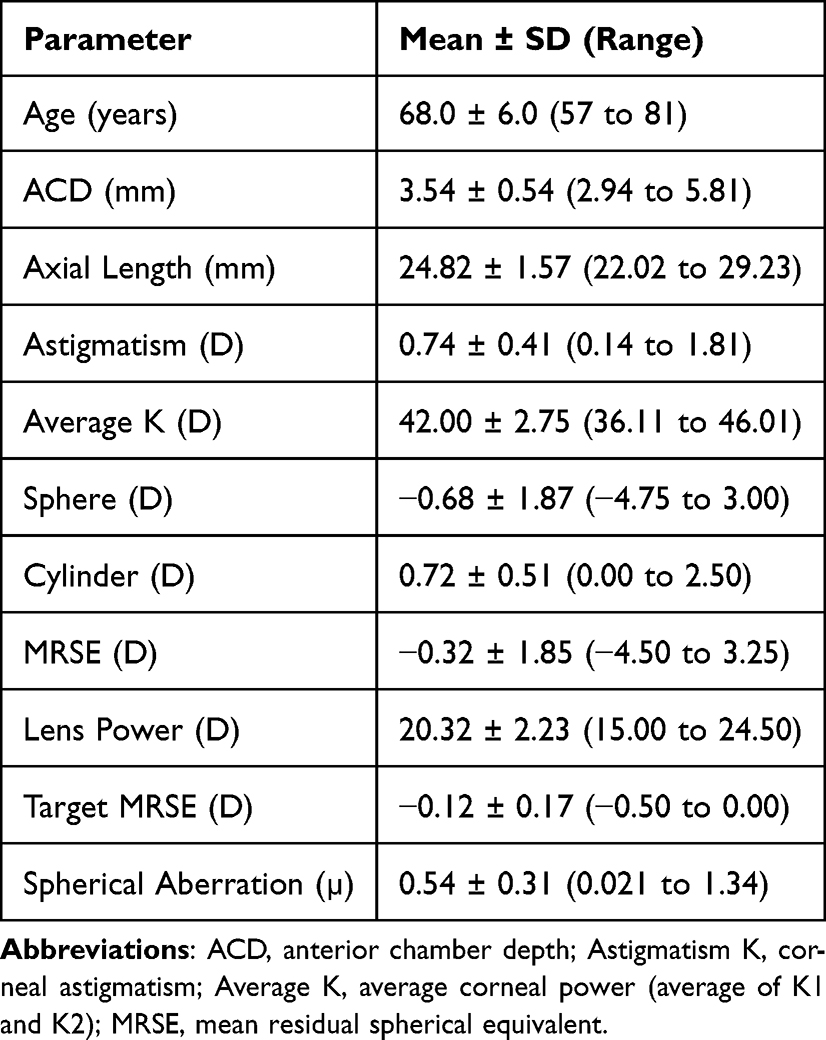 |
Table 1 Patient Demographic and Baseline Data |
Monocular and binocular uncorrected and distance corrected visual acuities at 3 months postoperative are summarized in Table 2 and Figure 1. Binocular uncorrected visual acuities at distance were good, with 85% of subjects (17/20) 20/25 or better. Binocular uncorrected visual acuities at intermediate and near were functional with 90% of subjects (18/20) 20/32 or better at intermediate and 75% of subjects (15/20) 20/40 or better at near. Figure 1 also summarizes the refractive outcomes at 3 months postoperatively. The percentages of eyes with manifest refraction spherical equivalent and residual astigmatism ± 0.5 D were 95% (38/40) and 98% (39/40), respectively. The 3 months postoperative binocular defocus curve is shown in Figure 1. The defocus curve suggests excellent vision at distance and intermediate and, as expected, there was a gradual decline after −1.50 D.
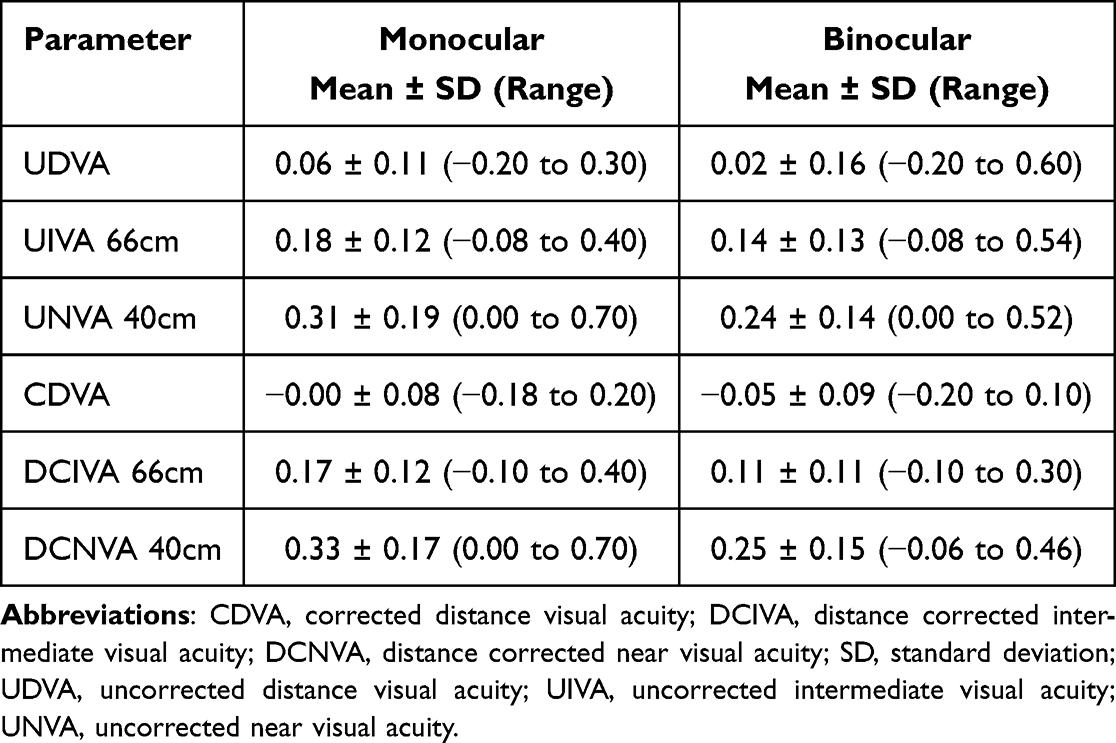 |
Table 2 Postoperative Visual Acuities |
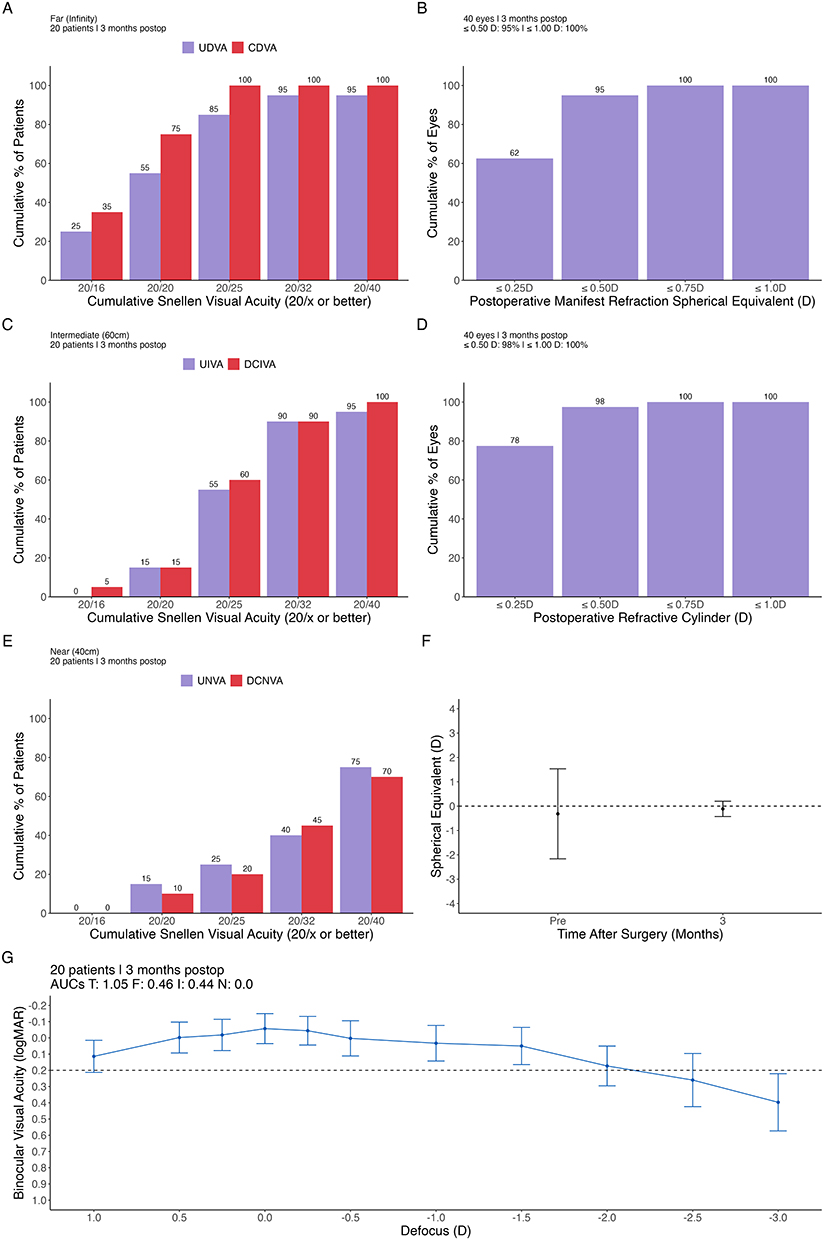 |
Figure 1 Standard graphs for presbyopia correcting intraocular lenses, including cumulative percentage of patients achieving binocular uncorrected and distance corrected visual acuity at (A) cumulative percentage of patients achieving binocular uncorrected and distance corrected visual acuity at far, (B) postoperative manifest refraction spherical equivalent distribution, (C) cumulative percentage of patients achieving binocular uncorrected and distance corrected visual acuity at intermediate, (D) postoperative refractive cylinder distribution, (E) cumulative percentage of patients achieving binocular uncorrected and distance corrected visual acuity at near, (F) postoperative manifest refraction spherical equivalent distribution over time, and (G) binocular defocus curve. Abbreviations: AUC, area under the curve; D, diopters; F, far; I, intermediate; logMAR, log of minimum angle of resolution; N, near; T, total. |
Patient responses on the QUVID questionnaire are summarized in Table 3. The three dysphotopsias that had the highest percentages of patients reporting as “moderate” or “severe” were glare, starbursts, and halos at 35% (7/20), 25% (5/20), and 20% (4/20), respectively. However, only 0% (0/20), 5% (1/20), and 0% (0/20) of subjects indicated that they were bothered “quite a bit” or “very much” by glare, starbursts, and halos, respectively.
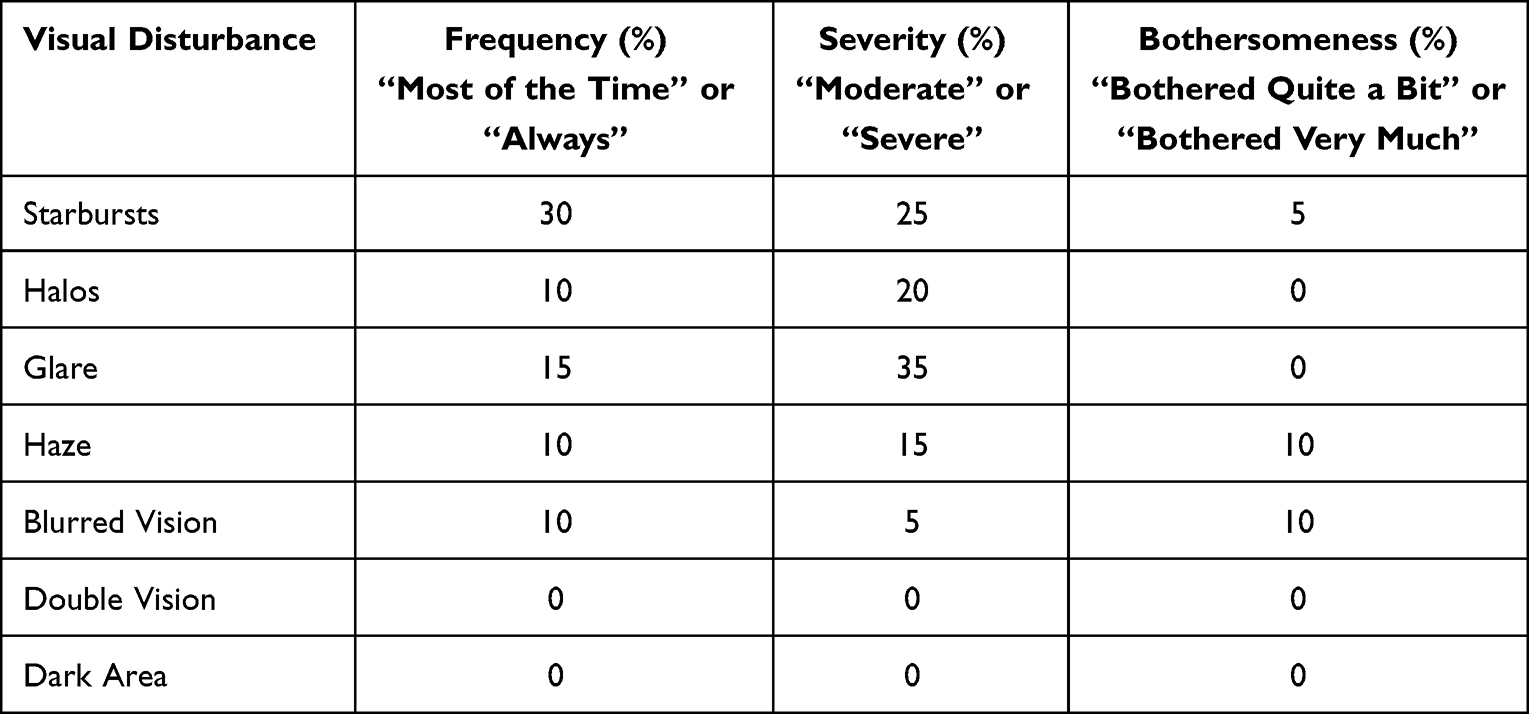 |
Table 3 Summary of QUVID Questionnaire Responses at 3 Months Postoperatively (n=20) |
Patient responses on the IOLSAT questionnaire are summarized in Table 4. Spectacle independence was defined as answering “Never” or “Rarely” on the questionnaire. Good visual performance was defined as answering “Very good” or “Good” on the questionnaire. Spectacle independence overall at distance, intermediate, and near were 90% (18/20), 75% (15/20), and 30% (6/20), respectively. In addition, 80% (16/20) of subjects reported being “satisfied” or “very satisfied” with their vision, 65% (13/20) would have the same lenses implanted again, and 70% (14/20) would recommend the implanted lens to friends and family. It is important to note that many of these patients initially desired a trifocal IOL, but opted for Vivity due to concerns about dysphotopsias given their history of refractive surgery.
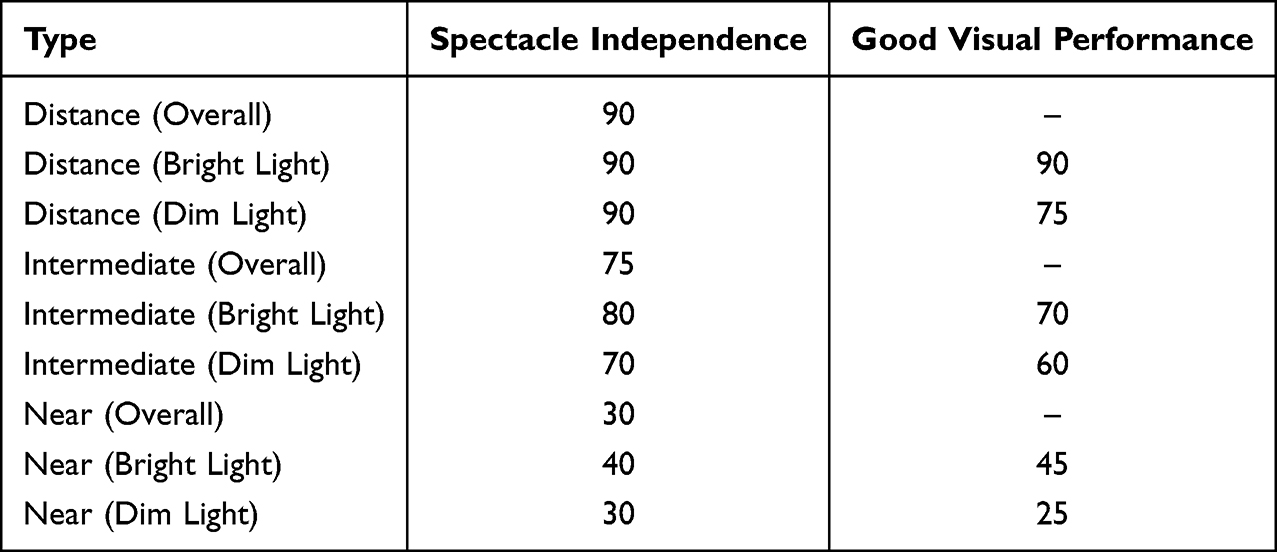 |
Table 4 Summary of IOLSAT Questionnaire Responses at 3 Months Postoperatively (n=20) |
Spearman correlations between preoperative SA and postoperative responses about severity or bothersomeness of dysphotopsias were weak (rho = 0.03 and rho = −0.01, respectively). Pearson correlations between preoperative SA and postoperative visual outcomes are summarized in Table 5. We observed moderate negative correlations between SA and monocular UDVA (r = −0.28) and monocular DCNVA (r = −0.32). The association with DCNVA reached significance (p = 0.05) prior to adjustment, but not after (p = 0.27).
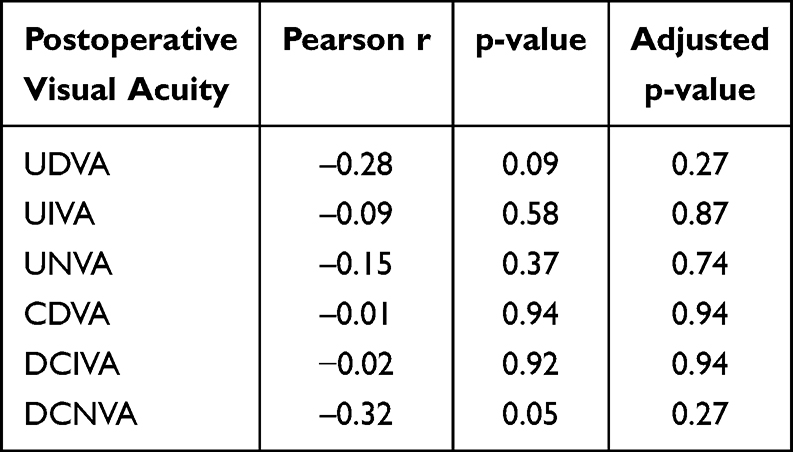 |
Table 5 Correlation of Preoperative Spherical Aberration to Postoperative Visual Outcomes |
Discussion
It can be challenging to achieve good refractive and visual outcomes in post-LVC eyes after cataract surgery and IOL implantation. In addition, there are concerns that high spherical aberration can cause too much blur, which is then worsened by implanting a trifocal or EDOF IOL, leading to poor visual outcomes and patient satisfaction. In this study, we investigated the visual outcomes and patient reported satisfaction, spectacle independence, and quality of vision in post-myopic LASIK and PRK eyes, with high corneal spherical aberration, after bilateral Vivity implantation. To the best of our knowledge, this is the first study that specifically targeted post-myopic LASIK and PRK patients with high corneal spherical aberration. We are aware of one other report of the Vivity IOL in post-LVC eyes from patients in Spain.17 Carreras et al17 reported mean binocular UDVA, UIVA, and UNVA of 0.02, −0.02, and 0.14 logMAR, respectively, at 3 months postoperatively, compared to 0.02, 0.14, and 0.24 logMAR, respectively, in our study. Differences may be due to the higher number of toric IOLs in our study (40%) compared to their study (10%) or patient populations. Our results are also comparable to studies of the Vivity IOL in eyes without prior corneal refractive surgery. Mean binocular UDVA, UIVA, and UNVA were reported in the US Food and Drug Administration (FDA) clinical trial of the Vivity IOL as 0.04, 0.06, and 0.21, respectively.20 In addition, a randomized trial of the Vivity IOL from multiple countries reported mean binocular UDVA, UIVA, and UNVA of 0.01, 0.06, and 0.23, respectively.19 The results from our study and others suggest binocular uncorrected visual outcomes in post-LVC eyes may be similar to eyes without LVC.
Post-LVC patients may have higher expectations of spectacle independence compared to patients with no prior LVC. In our study, 90%, 75%, and 30% of patients overall were spectacle independent at distance, intermediate, and near, respectively. Carreras et al17 reported spectacle independence of 91%, 73%, and 50%, respectively, overall at distance, intermediate and near on the IOLSAT questionnaire (in post-LVC patients). Differences between their study and ours may be due to differences in sample size, as 11 subjects answered the IOLSAT questionnaire in their study compared to 20 in our study. Other studies of patients without prior LVC also suggest high spectacle independence with the Vivity IOL. Kandavel et al22 reported spectacle independence of 90%, 94%, and 58%, respectively, overall at distance, intermediate and near on the IOLSAT questionnaire. In the US FDA clinical trial of the Vivity IOL, spectacle independence was reported in 94% and 87% of subjects at distance and intermediate, respectively. Studies using different questionnaires, in patients without prior LVC, have also reported high spectacle independence with the Vivity IOL.11,23
Of particular concern when implanting presbyopia-correcting IOLs in post-LVC patients are dysphotopsias. Even mild dysphotopsias can lower patient satisfaction, and in some cases, lead to secondary surgical intervention. In our study, 25%, 20%, and 35%, of subjects reported the severity of starbursts, halo, and glare as “Severe” or “Moderate”, respectively, on the QUVID. In contrast, Carreras et al17 reported that 16%, 12%, and 12% of subjects (with prior LVC) reported the severity of starbursts, halo, and glare as “Severe” or “Moderate”, respectively, on the QUVID. Other studies of patients without prior LVC also suggest low severity of dysphotopsias with the Vivity IOL. In the US FDA clinical trial of the Vivity IOL,1 17%, 9%, and 9% of subjects reported the severity of starbursts, halo, and glare as “Severe” or “Moderate”, respectively, on the QUVID. Scheepers and Hall20 observed that 9%, 0%, and 3% of subjects reported the severity of starbursts, halo, and glare as “Severe” or “Moderate”, respectively, on the QUVID. Differences between our study and others may be due to differences in patient population, especially considering the post-LVC eyes and high corneal spherical aberration in our study.
It is worthwhile to touch on the result that 65% of patients would have the same lens implanted again. Notably, these patients originally preferred a trifocal IOL, and this level of satisfaction could be a reflection of their desire and expectations for spectacle independence from a trifocal IOL, rather than dissatisfaction with the EDOF IOL, given the good and functional visual outcomes in our study. For a future study, it may be interesting to ask if patients had a choice between the EDOF and a monofocal, would they choose the same lens again.
We observed a moderate negative correlation between preoperative SA and postoperative UDVA and DCNVA, although we note that these were exploratory endpoints. The Vivity IOL has been shown to have net negative SA,24 which can partially correct the positive SA of the cornea. It is possible that patients with higher SA (mean 0.54 ± 0.31 µ in our study) may have higher remaining positive SA that increases the depth of focus. Savini et al25 reported a positive correlation between preoperative corneal SA and DCNVA, opposite to our study, although the mean SA (0.10 ± 0.21 µ) in their study was lower than in our study. Our sample size was also relatively low, therefore further studies are warranted.
The primary limitation of this study was the relatively low sample size. Presbyopia-correcting IOLs are not routinely implanted in post-refractive eyes, therefore it was challenging to get a larger sample. Despite this, there is a sufficient sample to be able to describe the performance of the Vivity IOL in post-refractive eyes. Another limitation was the single-arm nature of the study. A comparator group of patients without prior refractive surgery and who were implanted with the Vivity, or a group of post-LVC eyes implanted with a different IOL, would allow for more robust conclusions to be drawn. Finally, long-term stability was not addressed.
Conclusions
The results of this study are encouraging and suggest good visual outcomes with high patient satisfaction with Vivity and Vivity toric IOL implantation in post myopic refractive surgery patients.
Acknowledgment
This paper was presented at the 2024 and 2025 American Society of Cataract and Refractive Surgery (ASCRS) Annual Meeting as a conference talk.
Funding
This study was supported with an investigator-initiated study grant (69865263) from Alcon Vision, LLC, Fort Worth, TX, USA.
Disclosure
J. Morgan Micheletti, MD, is a consultant for Alcon, and reports the following outside the submitted work: Alcon – Consultant, Speaker, Research Grant; Bausch & Lomb – Consultant; BVI – Consultant; Johnson & Johnson Vision – Research Grant; Lenstec – Speaker; RxSight – Consultant, Speaker; Zeiss – Consultant. Brad Hall reports independent contractor fees from Topcon Healthcare Inc. The authors report no other conflicts of interest for this work.
References
1. Schallhorn JM. Multifocal and extended depth of focus intraocular lenses: a comparison of data from the United States food and drug administration premarket approval trials. J Refract Surg. 2021;37:98–9. doi:10.3928/1081597X-20201111-02
2. Hovanesian JA, Jones M, Allen Q. The PanOptix trifocal IOL vs the ReSTOR 2.5 active focus and ReSTOR 3.0-add multifocal lenses: a study of patient satisfaction, visual disturbances, and uncorrected visual performance. Clin Ophthalmol. 2021;15:983–990. doi:10.2147/OPTH.S285628
3. Ianchulev T, Hoffer KJ, Yoo SH, et al. Intraoperative refractive biometry for predicting intraocular lens power calculation after prior myopic refractive surgery. Ophthalmology. 2014;121:56–60. doi:10.1016/j.ophtha.2013.08.041
4. McCarthy M, Gavanski GM, Paton KE, Holland SP. Intraocular lens power calculations after myopic laser refractive surgery: a comparison of methods in 173 eyes. Ophthalmology. 2011;118:940–944. doi:10.1016/j.ophtha.2010.08.048
5. Chow SSW, Chan TCY, Ng ALK, Kwok AKH. Outcomes of presbyopia-correcting intraocular lenses after laser in situ keratomileusis. Int Ophthalmol. 2019;39:1199–1204. doi:10.1007/s10792-018-0908-0
6. Li QM, Wang F, Wu ZM, et al. Trifocal diffractive intraocular lens implantation in patients after previous corneal refractive laser surgery for myopia. BMC Ophthalmol. 2020;20:293. doi:10.1186/s12886-020-01556-0
7. Cobo-Soriano R, Ortega-Usobiaga J, Rodriguez-Gutierrez B, et al. Trifocal intraocular lens implantation in eyes with previous corneal refractive surgery for myopia and hyperopia. J Cataract Refract Surg. 2021;47:1265–1272. doi:10.1097/j.jcrs.0000000000000637
8. Blaylock JF, Hall BJ. Refractive outcomes following trifocal intraocular lens implantation in post-myopic LASIK and PRK eyes. Clin Ophthalmol. 2022;16:2129–2136. doi:10.2147/OPTH.S370061
9. Khor WB, Afshari NA. The role of presbyopia-correcting intraocular lenses after laser in situ keratomileusis. Curr Opin Ophthalmol. 2013;24:35–40. doi:10.1097/ICU.0b013e32835ab457
10. Ozulken K, Kiziltoprak H, Yuksel E, Mumcuoglu T. A comparative evaluation of diffractive trifocal and new refractive/extended depth of focus intraocular lenses for refractive lens exchange. Curr Eye Res. 2021;46:811–817. doi:10.1080/02713683.2020.1833347
11. Hovanesian JA, Jones M, Allen Q. The Vivity extended range of vision IOL vs the PanOptix trifocal, ReSTOR 2.5 active focus and ReSTOR 3.0 multifocal lenses: a comparison of patient satisfaction, visual disturbances, and spectacle Independence. Clin Ophthalmol. 2022;16:145–152. doi:10.2147/OPTH.S347382
12. Teshigawara T, Meguro A, Mizuki N. The effect of age, postoperative refraction, and pre- and postoperative pupil size on halo size and intensity in eyes implanted with a trifocal or extended depth-of-focus lens. Clin Ophthalmol. 2021;15:4141–4152. doi:10.2147/OPTH.S327660
13. Scheepers MA, Hall B. Randomized and double-blind comparison of clinical visual outcomes of 2 EDOF intraocular lenses. J Cataract Refract Surg. 2023;49:354–359. doi:10.1097/j.jcrs.0000000000001113
14. Kanclerz P, Toto F, Grzybowski A, Alio JL. Extended depth-of-field intraocular lenses: an update. Asia Pac J Ophthalmol. 2020;9:194–202. doi:10.1097/APO.0000000000000296
15. Alvarez-Garcia MT, Fuente-Garcia C, Munoz-Puyol C, Pinero DP. Clinical outcomes with extended depth of focus intraocular lenses in cases in which multifocal lenses are not primarily recommended. J Ophthalmol. 2023;2023:8814627. doi:10.1155/2023/8814627
16. Ferreira TB, Pinheiro J, Zabala L, Ribeiro FJ. Comparative analysis of clinical outcomes of a monofocal and an extended-range-of-vision intraocular lens in eyes with previous myopic laser in situ keratomileusis. J Cataract Refract Surg. 2018;44:149–155. doi:10.1016/j.jcrs.2017.11.007
17. Carreras H, Renones J, Carreras MDR, Canto C, Pinero DP. Clinical performance of an extended range of vision intraocular lens after LASIK. J Refract Surg. 2024;40:e742–e753. doi:10.3928/1081597X-20240903-01
18. Kohnen T. Nondiffractive wavefront-shaping extended range-of-vision intraocular lens. J Cataract Refract Surg. 2020;46:1312–1313. doi:10.1097/j.jcrs.0000000000000247
19. Bala C, Poyales F, Guarro M, et al. Multicountry clinical outcomes of a new nondiffractive presbyopia-correcting IOL. J Cataract Refract Surg. 2022;48:136–143. doi:10.1097/j.jcrs.0000000000000712
20. McCabe C, Berdahl J, Reiser H, et al. Clinical outcomes in a U.S. registration study of a new EDOF intraocular lens with a nondiffractive design. J Cataract Refract Surg. 2022;48:1297–1304. doi:10.1097/j.jcrs.0000000000000978
21. Kohnen T, Petermann K, Bohm M, et al. Nondiffractive wavefront-shaping extended depth-of-focus intraocular lens: visual performance and patient-reported outcomes. J Cataract Refract Surg. 2022;48:144–150. doi:10.1097/j.jcrs.0000000000000826
22. Kandavel R, Colvard M, Dredge J, et al. Comparative study between non-diffractive extended depth of focus and monofocal intraocular lenses. Clin Ophthalmol. 2023;17:1161–1168. doi:10.2147/OPTH.S402069
23. Shafer BM, McCabe C, Reiser H, Newsom TH, Berdahl J. The REVIVE study: long term outcomes of a novel non-diffractive extended vision IOL versus monofocal control IOL. Clin Ophthalmol. 2022;16:3945–3950. doi:10.2147/OPTH.S390380
24. Bang SP, Jung H, Li KY, Yoon G. Comparison of modal and zonal wavefront measurements of refractive extended depth of focus intraocular lenses. Biomed Opt Express. 2024;15:1618–1629. doi:10.1364/BOE.513529
25. Savini G, Galzignato A, Coutinho CP, et al. Influence of preoperative variables on the 3-month functional outcomes of the Vivity extended depth-of-focus intraocular lens: a prospective case series. Eye Vis. 2025;12:8. doi:10.1186/s40662-024-00424-y
 © 2026 The Author(s). This work is published and licensed by Dove Medical Press Limited. The
full terms of this license are available at https://www.dovepress.com/terms
and incorporate the Creative Commons Attribution
- Non Commercial (unported, 4.0) License.
By accessing the work you hereby accept the Terms. Non-commercial uses of the work are permitted
without any further permission from Dove Medical Press Limited, provided the work is properly
attributed. For permission for commercial use of this work, please see paragraphs 4.2 and 5 of our Terms.
© 2026 The Author(s). This work is published and licensed by Dove Medical Press Limited. The
full terms of this license are available at https://www.dovepress.com/terms
and incorporate the Creative Commons Attribution
- Non Commercial (unported, 4.0) License.
By accessing the work you hereby accept the Terms. Non-commercial uses of the work are permitted
without any further permission from Dove Medical Press Limited, provided the work is properly
attributed. For permission for commercial use of this work, please see paragraphs 4.2 and 5 of our Terms.