Back to Journals » Drug Design, Development and Therapy » Volume 18
Safety and Effectiveness of a Biosimilar Recombinant Growth Hormone in Adults with Growth Hormone Deficiency: Analysis of Final Data from PATRO Adults, an International Post-Marketing Surveillance Study
Authors Beck-Peccoz P, Höybye C, Simsek S ![]() , Stalla G, Murray RD, Esmael A, Urosevic D, Boldea A, Zabransky M
, Stalla G, Murray RD, Esmael A, Urosevic D, Boldea A, Zabransky M
Received 25 July 2024
Accepted for publication 9 November 2024
Published 5 December 2024 Volume 2024:18 Pages 5729—5741
DOI https://doi.org/10.2147/DDDT.S471967
Checked for plagiarism Yes
Review by Single anonymous peer review
Peer reviewer comments 2
Editor who approved publication: Prof. Dr. Georgios Panos
Paolo Beck-Peccoz,1 Charlotte Höybye,2 Suat Simsek,3 Günter Stalla,4 Robert D Murray,5 Altaher Esmael,6 Dragan Urosevic,7 Anca Boldea,6 Markus Zabransky6
1Fondazione Istituto di Ricovero e Cura a Carattere Scientifico Cà Granda Ospedale Maggiore Policlinico, Milan, Italy; 2Department of Endocrinology and Department of Molecular Medicine and Surgery, Karolinska University Hospital and Karolinska Institute, Stockholm, Sweden; 3Department of Internal Medicine/Endocrinology, Northwest Clinics, Alkmaar and Amsterdam University Medical Centers, Location VUmc, Amsterdam, The Netherlands; 4Medicover Neuroendocrinology and Medizinische Klinik und Poliklinik IV, Klinikum der Universität, Munich, Germany; 5Leeds Centre for Diabetes & Endocrinology, Leeds Teaching Hospitals NHS Trust, Leeds, UK; 6HEXAL AG (a Sandoz company), Holzkirchen, Germany; 7Novartis Sandoz Biopharmaceutical AG, c/o HEXAL AG, Basel, Switzerland
Correspondence: Paolo Beck-Peccoz, Fondazione Istituto di Ricovero e Cura a Carattere Scientifico Cà Granda Ospedale Maggiore Policlinico, Via Pietro Custodi 1, Milan, 20136, Italy, Tel +39 3357073239, Email [email protected]
Purpose: Long-term studies are needed to investigate the safety of recombinant human growth hormone (rhGH) for the treatment of growth hormone deficiency (GHD) in routine practice. The objective of this study was to evaluate the safety and effectiveness of biosimilar rhGH (somatropin; Omnitrope®) in adults with GHD.
Methods: PAtients TReated with Omnitrope (PATRO) Adults was a post-marketing surveillance study conducted across Europe. The primary objective was the safety of biosimilar rhGH in adults, particularly the occurrence of glucose intolerance or diabetes mellitus and malignancies. All adverse events (AEs) were recorded throughout treatment. Treatment effectiveness was a secondary objective.
Results: By December 2021, 1527 patients (50.3% male) were enrolled from 84 centers in 10 European countries. Most patients had adult-onset GHD (n = 1243; 81.4%) and 771 (50.5%) were rhGH-naïve at study entry. Median (interquartile range) treatment duration was 4.4 (1.90– 7.30) years. Overall, 1181 patients (77.3%) reported 6667 AEs. Treatment-related AEs were reported in 143 patients (9.4%; 216 AEs); arthralgia was most common (n = 24). There were 49 confirmed diabetes mellitus events; 44 in newly diagnosed patients. Overall, 84 malignancies were reported. There were 46 treatment-related serious AEs in 39 patients (2.6%). The most frequently reported treatment-related serious AE was “metabolism and nutrition disorders” (n = 12). In rhGH-naïve patients, an increase in mean insulin-like growth factor-1 (IGF-1) standard deviation score (SDS) was observed from – 2.03 at baseline to +0.28 at 5 years. An increase in IGF-1 SDS was also observed in previously treated patients from – 0.71 to +0.35. Body mass index remained stable while blood lipid levels improved from baseline to 5 years.
Conclusion: Final data from PATRO Adults confirm that biosimilar rhGH (Omnitrope) is not associated with any unexpected safety signals, with no evidence of increased diabetogenic or carcinogenic risk, and is effective in real-world clinical practice.
Plain Language Summary: Why was the study done?
– Growth hormone deficiency is a condition caused by insufficient amounts of growth hormone in the body, which can be treated with daily injections of a replacement growth hormone medicine.
– It is important to monitor the safety of long-term treatment with growth hormone, especially regarding the risk of cancer and diabetes.
What did the researchers do?
– The PATRO Adults study included adult patients with growth hormone deficiency who were treated with a growth hormone medicine called Omnitrope.
– The researchers main aim was to evaluate specific safety concerns, including any potential increased risk of cancer and diabetes.
What did the researchers find?
– A total of 1527 patients were enrolled in the study.
– Overall, 143 patients had an adverse reaction that was considered to be related to growth hormone treatment, the most common of which was arthralgia, a type of joint ache, which occurred in 1.6% of patients.
– Overall, 17 patients (1.1%) developed diabetes and four patients (0.3%) developed cancer that was suspected as being related to growth hormone treatment.
– The risk of developing diabetes and cancer was low and comparable to what has been seen in previous studies in patients treated with growth hormone.
What do the results mean?
– The safety findings from this study were consistent with the well characterized safety profile of growth hormone treatment in adults with growth hormone deficiency. This supports previous studies showing no evidence of increased risk of cancer or diabetes with growth hormone treatment in adults.
Keywords: somatropin, long-term, real-world, European, diabetes, malignancy
Introduction
Growth hormone (GH) deficiency (GHD) in adults is associated with abnormal substrate metabolism, body composition, and physical and psychosocial function. Consequently, adult patients with GHD have difficulty controlling their body weight and may have increased body fat and decreased muscle mass and exercise capacity, as well as poor psychosocial function, all of which have a negative impact on quality of life (QoL).1,2
Adults with GHD include individuals with acquired GHD secondary to structural lesions or treatment of them, prior childhood-onset GHD, head trauma, and idiopathic GHD.3
Adult patients diagnosed with severe GHD are eligible for GH replacement therapy, the main goals of which are to reverse the metabolic, functional, and psychological abnormalities associated with adult GHD. Treatment of GHD in adults with recombinant human GH (rhGH) has proved to be effective for improving body composition, exercise capacity, skeletal integrity, blood lipid profile, and overall QoL.1,2,4 Although the risks associated with rhGH therapy are low,2 long-term clinical studies are integral to assessing the safety of rhGH therapy in routine clinical practice, both during treatment and after treatment cessation, particularly regarding the potential diabetogenic and carcinogenic risk.
Omnitrope® (somatropin; Sandoz GmbH, Kundl, Austria; henceforth referred to as “biosimilar rhGH”) is a biosimilar rhGH approved by the European Medicines Agency in 2006 for the treatment of adult and pediatric patients with GHD, with approval granted based on similar quality, safety, and efficacy to the reference medicine (Genotropin®; Pfizer Limited, Sandwich, United Kingdom).5,6 Biosimilar rhGH is also approved in other pediatric populations, including patients with Turner syndrome, Prader-Willi syndrome, chronic renal insufficiency, and short children born small for gestational age.6 Sandoz undertook the development of biosimilar rhGH in 1996, which was the world’s first development program of a biosimilar. Biosimilar rhGH is currently approved in 80 countries, and in real-world practice has generated >886,092 patient treatment-years of experience worldwide in approved indications up to January 2022 (Unpublished data: Sandoz. Omnitrope Periodic Safety Update Report [PSUR]; March 2022), showing that biosimilar rhGH is as effective and well tolerated as other available rhGH products. This growing body of evidence highlights the importance of experience with biosimilars beyond clinical studies to reassure healthcare professionals and patients regarding their use.
The PAtients TReated with Omnitrope (PATRO) Adults study was a large, longitudinal, multicenter, post-marketing surveillance study of the long-term efficacy and safety of biosimilar rhGH for the treatment of adults with GHD, conducted in hospitals and specialized endocrinology clinics across Europe.
Previous interim analyses from the PATRO Adults study demonstrated that of biosimilar rhGH is not associated with any unexpected safety signals and is effective in adults with GHD treated in a real-world practice. The results did not indicate an increased risk of diabetes mellitus or carcinogenic effect of rhGH in adults with GHD, but an increased risk of second new malignancies in patients with previous cancer could not be excluded based on the interim data set.7–9 Here, we present the final global safety and effectiveness data from the PATRO Adults study.
Materials and Methods
The design of this study has been described previously in detail.10 Briefly, eligible patients were male or female adults who received biosimilar rhGH treatment as part of routine clinical practice and according to the Summary of Product Characteristics recommendations.11 Patients who received treatment with another rhGH therapy before starting biosimilar rhGH were also eligible for inclusion.10 The study was conducted at hospitals and specialized endocrinology practices in countries where biosimilar rhGH had received marketing authorization – Belgium, Czech Republic, France, Germany, Greece, Italy, the Netherlands, Spain, Sweden, and the UK.
The primary objective of PATRO Adults was to analyze the safety and efficacy of biosimilar rhGH in routine clinical practice, with particular emphasis on the diabetogenic and carcinogenic risk.10 Effectiveness was assessed as a secondary objective.
The PATRO Adults study protocol was approved by the ethics review committee of participating centers in accordance with national laws and regulations. All procedures were performed in accordance with the ethical standards of these committees and with the Declaration of Helsinki. Written informed consent was obtained from all participating patients.
All clinic visits and assessments were conducted as part of routine clinical practice according to the prescribing physician’s discretion, and data were collected at each routine visit during biosimilar rhGH treatment. Safety assessments comprised monitoring and recording all adverse events (AEs), including those considered serious according to the International Conference on Harmonisation Guideline for Good Clinical Practice definition.12 The relationship between AEs and biosimilar rhGH treatment was evaluated independently by investigator and sponsor assessment, and classified according to the worse case.
All AEs were recorded for the complete duration of biosimilar rhGH treatment. Particular emphasis was placed on long-term safety, the incidence of hyperglycemia, the development of glucose intolerance or diabetes, and the re-occurrence or de novo onset of malignancies.
Effectiveness assessments included evaluation of insulin-like growth factor-1 (IGF-1) and lipid levels, body composition, and QoL outcomes.
Data Collection and Study Populations
Patient data were entered into an electronic case report form (eCRF) at each routine visit. eCRFs were reviewed by data management and on-site monitoring was performed by a contract research organization.
Laboratory assessments and vital signs were requested to be documented at least annually, in accordance with routine clinical practice.
The study was conducted from September 2007 to December 2021. All enrolled patients who received ≥1 dose of biosimilar rhGH were included in the safety population, which consisted of all patients documented within the eCRF at the time of final database lock (December 2021; study close). Patients for whom neither a visit date nor a start date of biosimilar rhGH treatment had been documented were excluded.
The effectiveness population was a subset of the safety population and included all patients with a documented baseline visit (start of biosimilar rhGH treatment) and at least one further documented visit under biosimilar rhGH treatment. Missing data were not included in the analysis, and reasons for discontinuation for any reason, including lost to follow-up, were analyzed.
Results
Patient Characteristics and Diagnostic Details
By December 2021, 1527 patients had been enrolled from 84 centers in 10 European countries (Belgium, Czech Republic, France, Germany, Greece, Italy, the Netherlands, Spain, Sweden, and the UK). The majority of patients were enrolled in the UK (n = 446; 29.2%), Germany (n = 425; 27.8%), and Sweden (n = 311; 20.4%).
At the time of analysis (database lock), all 1527 patients (100%) stopped documentation following study closure. A total of 923 patients (60.4%) continued biosimilar rhGH treatment, 418 patients (27.4%) stopped treatment, and 78 patients (5.1%) had unknown further treatment at study closure. There were 108 patients (7.1%) lost to follow-up and without information on GH treatment.
All outcome data presented include patients with documented data as defined previously. Most patients had adult-onset GHD (n = 1243, 81.4%; childhood-onset, n = 267, 17.5%; missing, n = 17, 1.1%). In addition, 771 patients (50.5%) were rhGH-naïve at study entry, whereas 756 (49.5%) had been pretreated with another rhGH. Further baseline characteristics of enrolled patients are shown in Table 1. Overall, 1350 patients (88.4%) had multiple pituitary hormone deficiencies (one additional hormone deficiency, n = 278 [20.6%]; two additional deficiencies, n = 361 [26.7%]; three additional deficiencies, n = 709 [52.5%]) or isolated GHD (n = 169; 11.1%). Approximately half of the patients (756; 49.5%) had been pretreated with GH before study participation, for a mean (standard deviation [SD]) duration of 11.0 (7.9) years. Concomitant medication use included thyroid hormones (any; n = 1016), hydrocortisone/cortisone (any; n = 1185), sex hormones (any; n = 641), and desmopressin (any; n = 222). Brain tumor was the most frequent etiology for GHD in patients with isolated GHD (45.6%) and in patients with combined GHD (64.9%). Other etiologies included idiopathic, traumatic brain injury, autoimmune disease, malformation, genetic disorder, and infection (Table 2).
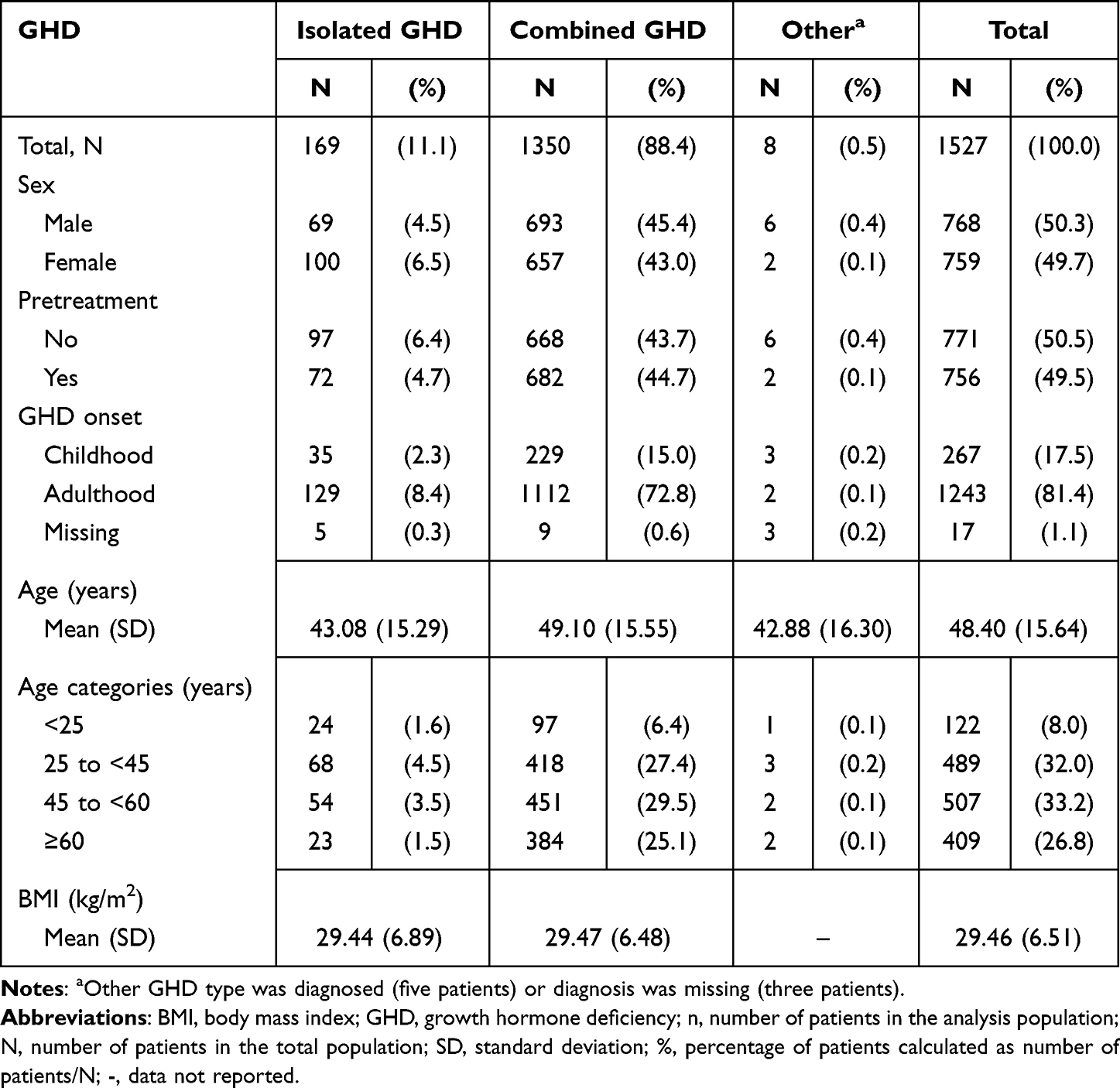 |
Table 1 Patient Characteristics at Enrollment (Safety Analysis Set) |
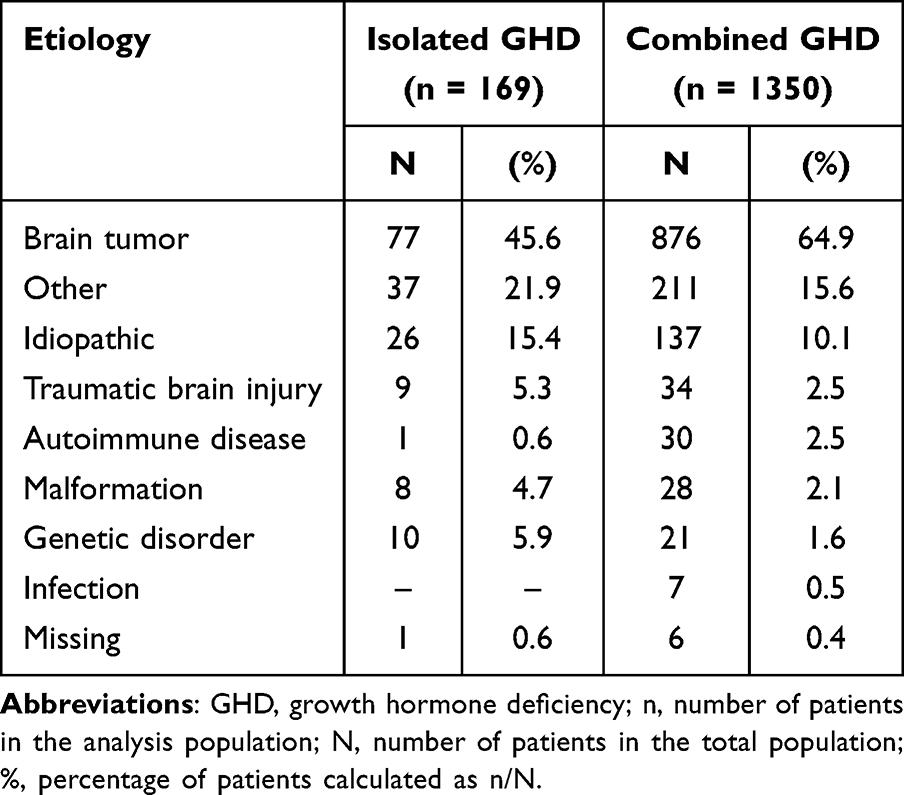 |
Table 2 Diagnostic Details (Safety Population, N = 1527) |
Overall, 1527 patients were included in the safety analysis and 1386 were included in the efficacy analysis.
rhGH Treatment
The overall mean (SD) baseline biosimilar rhGH dose was 0.288 (0.230) mg/day. Among patients with isolated GHD, the mean (SD) baseline dose was 0.344 (0.263) mg/day, whereas in patients with combined GHD it was 0.309 (0.221) mg/day. In patients who were pretreated with GH, baseline biosimilar rhGH dose was 0.375 (0.271) mg/day, whereas naïve patients received a baseline dose of 0.201 (0.132) mg/day. Most patients were dosed within the recommended dose range of 0.2–0.5 mg/day. The European Summary of Product Characteristics considers doses >1.0 mg/day rare.11 However,33 patients (2.2%) received doses >1.0 mg/day.
The overall median (interquartile range) biosimilar rhGH treatment duration in the study was 4.4 (1.90–7.30) years. In the current study, pretreated patients had a longer treatment duration compared with naïve patients (5.40 [2.30–7.65] versus 3.90 [1.60–6.60] years, respectively). Overall, patients were observed for 7293.1 patient-years.
Treatment Discontinuation
Following study closure, over half of patients (n = 837; 54.8%) discontinued the study since the sponsor requested that documentation stop. Other reasons included administrative center/site closure (n = 117; 7.7%), patients lost to follow-up (n = 108; 7.1%), or stopping after referral to another endocrinologist (n = 30; 2.0%). In addition to the sponsor-requested documentation stop, 418 of the 1527 (27.4%) patients stopped treatment for other reasons, most commonly due to an AE (n = 159/418; 38.0%) or because they did not wish to continue injections (n = 157/418; 37.6%).
The most common AEs that resulted in discontinuation were (Medical Dictionary for Regulatory Activities [MedDRA] preferred term [PT]) prostate cancer (n = 10), headache (n = 8), breast cancer (n = 7), neoplasm progression (n = 6), peripheral edema (n = 6), arthralgia (n = 5), colorectal cancer (n = 4), and pain in extremity (n = 4).
AEs of special interest that led to discontinuation (MedDRA system organ class [SOC]) comprised “Neoplasms benign, malignant, and unspecified”, n = 48 (3.1%) (including new malignancies [n = 38; 2.5%]) and “Metabolism and nutrition disorders”, n = 4 (0.3%) (including confirmed diabetes mellitus [n = 3; 0.2%]).
Adverse Events
Reported AEs are summarized in Table 3 (safety population, N = 1527). Overall, 1181 patients (77.3%) reported AEs (n = 6667 events). Most AEs were considered mild or moderate in intensity (Table 3); 373 AEs in 218 patients (14.3%) were severe. In total, 143 patients (9.4%) reported 216 AEs considered to be related to treatment. The most frequently reported treatment-related AEs (MedDRA PTs) were arthralgia (n = 24/1527; 1.6%), newly diagnosed type 2 diabetes mellitus (n = 17; 1.1%), myalgia (n = 16; 1.0%), headache (n = 15; 1.0%), and peripheral edema (n = 10; 0.7%).
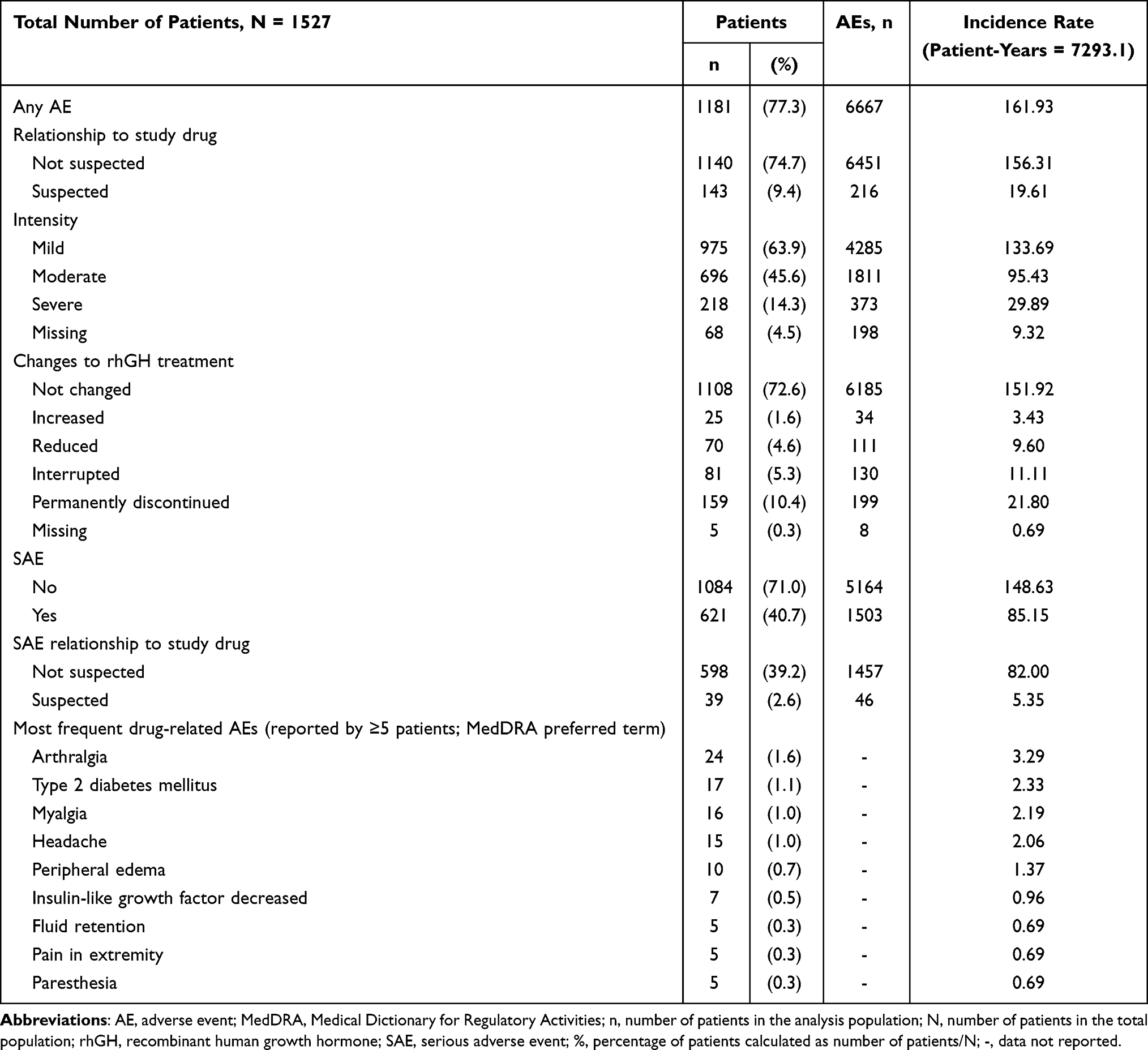 |
Table 3 Summary of AEs (Safety Population, N = 1527) |
Serious AEs (SAEs) were reported in 621 patients (40.7%) (n = 1503 events); of these, 39 patients (2.6%) had SAEs that were considered to be related to treatment (n = 46 events). The most frequently reported treatment-related SAEs (MedDRA SOCs) were “metabolism and nutrition disorders” (n = 22 [1.4%] patients, including newly diagnosed type 2 diabetes [n = 17 (1.1%) patients] and worsening or inadequately controlled diabetes mellitus [n = 4 (0.3%) patients]) and “neoplasms benign, malignant, and unspecified (including cysts and polyps)” (n = 8 [0.5%] patients).
There were 49 events of confirmed diabetes mellitus (MedDRA high-level term: diabetes mellitus [including subgroups]) in 49 patients (3.2%); 44 events (in 44 [2.9%] patients) were newly diagnosed and five events (in five [0.3%] patients) were worsening or inadequately controlled diabetes mellitus in patients with pre-existing diabetes mellitus (Table 4). Among these 49 patients with diabetes mellitus, the event was assessed as serious in 47 patients (3.1%), 38 patients (2.5%) required medical treatment, and three patients (0.2%) permanently discontinued rhGH treatment as a result. Diabetes mellitus cases were suspected as being related to rhGH treatment in 21 patients (1.4%): 17 patients (1.1%) with newly diagnosed type 2 diabetes mellitus and four patients (0.3%) with worsening or inadequately controlled diabetes mellitus (type 2 diabetes mellitus in three patients and diabetes type unknown in one patient). In addition, there were 19 patients (1.2%) with impaired glucose metabolism; the MedDRA PTs were: “Glucose tolerance impaired” in 11 patients (0.7%), “Impaired fasting glucose” in two (0.1%), “Insulin resistance” in three (0.2%), and “Hyperglycemia” in three (0.2%), respectively. All except one were classified as nonserious.
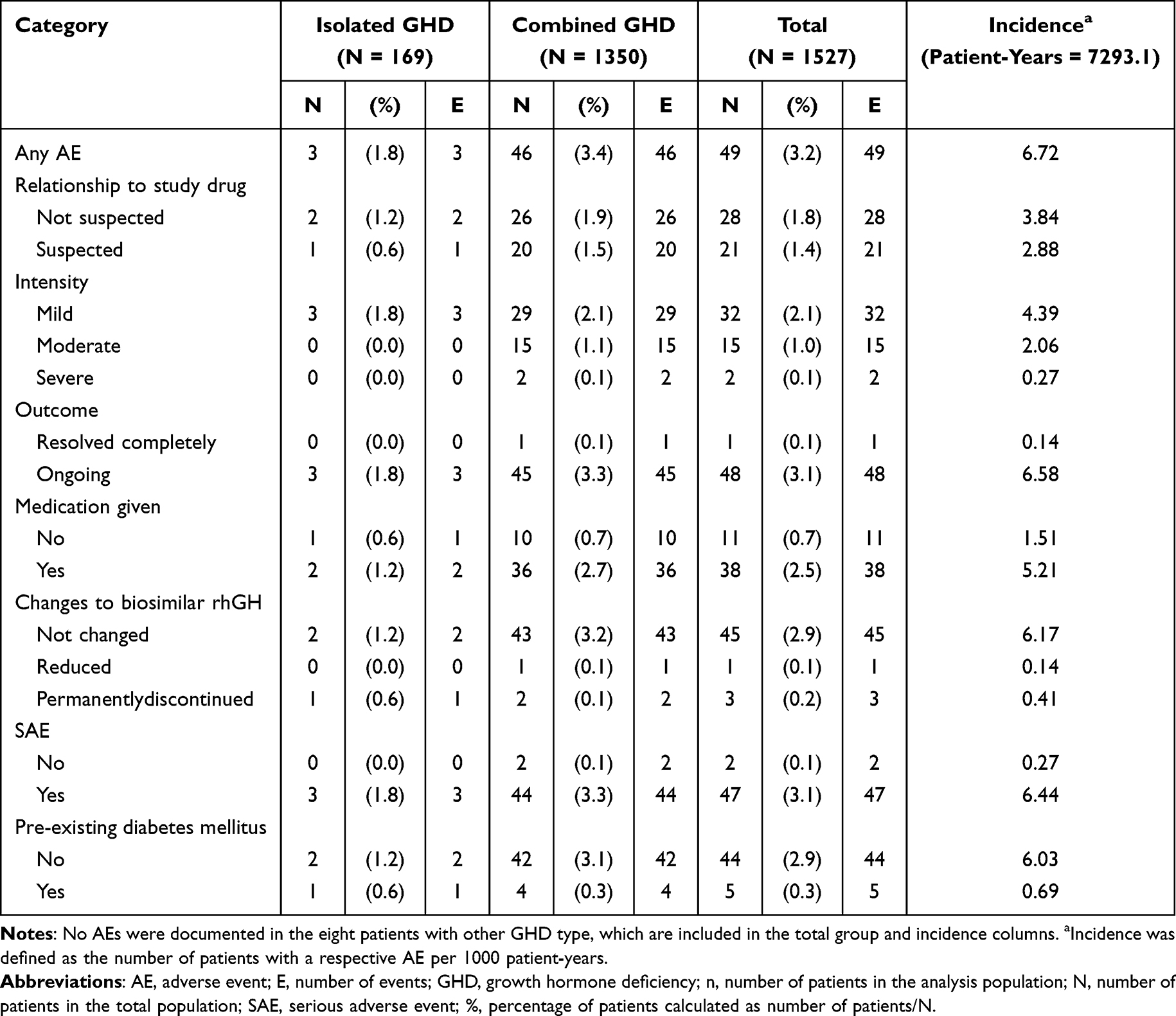 |
Table 4 Patients with Confirmed Diabetes Mellitus by GHD Type (Safety Population, N = 1527) |
Malignancies were documented as MedDRA SOC “Neoplasms benign, malignant, and unspecified” and were classified as malignant. A total of 84 malignancies (80 primary and four secondary) were reported in 75 patients (4.9%); 71 events in 63 patients (4.1%) were newly diagnosed (Table 5), 13 events in 13 patients (0.9%) were recurring pre-existing malignancies, and one event (0.1%) in one patient was a newly diagnosed and recurrence of malignancy. Four patients (0.3%) had malignancies (all newly diagnosed) suspected to be related to treatment: one patient with adult-onset combined GHD diagnosed with malignant melanoma at 72 years of age, 0.9 years after biosimilar rhGH initiation (GHD aetiology: brain tumor [benign pituitary macroadenoma]); one patient with adult-onset isolated GHD diagnosed with breast cancer at 60 years of age, 2.6 years after biosimilar rhGH initiation (GHD aetiology: malformation); one patient with childhood-onset isolated GHD diagnosed with ovarian cancer at 60 years of age, 1.9 years after biosimilar rhGH initiation (GHD aetiology: idiopathic); one patient with adult-onset combined GHD diagnosed with prostate cancer at 74 years of age, 4.3 years after biosimilar rhGH initiation (GHD aetiology: brain tumor [benign pituitary macroadenoma]). Among the 63 patients (4.1%) with newly diagnosed malignancies, 38 patients (2.5%) permanently discontinued treatment due to the malignancy and four patients (0.3%) died due to the malignancy. The most frequently reported newly diagnosed malignancies were basal cell carcinoma (15 events in 13 patients [0.9%]), prostate cancer (12 events in 12 patients [0.8%]), and breast cancer and malignant melanoma (both with five events in five patients [0.3%]).
 |
Table 5 Newly Occurring Malignancies Overall and by GHD Type (Safety Population, N = 1527) |
AEs of special interest occurred in seven patients, none of which were considered related to treatment (MedDRA PT) and included cerebral hemorrhage (each as one event in two patients), intracranial hemorrhage, intracranial aneurysm, pituitary apoplexy, subarachnoid hemorrhage, and traumatic intracranial hemorrhage (each as one event in one patient).
In total, 34 deaths were recorded, none of which were suspected by the physician to be related to biosimilar rhGH treatment.
Safety Subgroup Analysis
Safety outcomes were compared across rhGH pre-treatment and GHD type subgroups (Table 6). Rates of AEs and SAEs were generally comparable between patients with isolated GHD and combined GHD in the GH-naïve and rhGH-pretreated groups. The incidence of suspected treatment-related AEs and SAEs were also generally comparable across the groups.
 |
Table 6 Summary of AEs by Pretreatment and GHD-Type Subgroups (Safety Population, N = 1527) |
Effectiveness
The effectiveness population included 1386 patients: 696 were rhGH-naïve at study entry and 690 were rhGH-pretreated; 155 patients had isolated GHD and 1226 had combined GHD (5 patients had “other” GHD type). Data for each outcome are shown for patients in this population with available data. In patients who were rhGH-naïve, a marked increase in mean (SD) IGF-1 SD score (SDS) was observed from –2.03 (1.67) at baseline to +0.28 (1.48) at 5 years (Figure 1A). An increase in IGF-1 SDS was also observed in previously treated patients from –0.71 (2.09) to +0.35 (1.38) (Figure 1B). The increase in IGF-1 SDS remained relatively stable in both sets of patients over time.
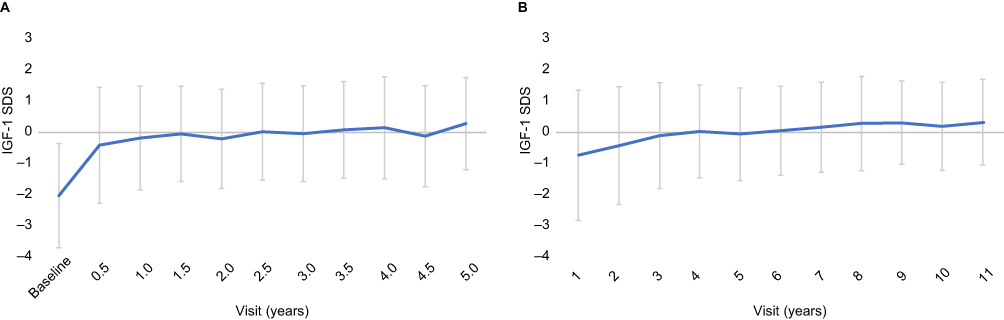 |
Figure 1 IGF-1 SDS over time in (A) rhGH-naïve patients and (B) pretreated patients (full effectiveness population, N = 1386). Data shown are mean ± SD. Abbreviations: IGF-1, insulin-like growth factor-1; rhGH, recombinant human growth hormone; SD, standard deviation; SDS, standard deviation score. |
Lean body mass increased by approximately 5% compared with baseline after 1 year (n = 131); after 5 years, the increase was approximately 3% (n = 68). Total fat mass decreased by approximately 1% at 1 year (n = 231) compared with baseline; by 5 years, this decrease remained at approximately 1% (n = 108). Mean body mass index (BMI) and mean change from baseline remained stable up to approximately 8 years. Both naïve and pretreated patients with isolated and combined GHD had similar BMI values.
For patients who were rhGH-naïve on study entry, lipid profile improved over time with rhGH treatment; in part as a consequence of a decrease in mean (SD) total cholesterol/high-density lipoprotein cholesterol (TC/HDL) ratio over the study observation period, from 4.21 (1.31) at baseline to 4.11 (1.45) after 5 years (isolated GHD), and from 4.51 (1.54) at baseline to 3.95 (1.26) after 5 years (combined GHD). For pretreated patients, lipid profile was generally constant over time, with mean (SD) TC/HDL ratio reported as 3.74 (0.94) at baseline and 4.17 (1.11) after 5 years (isolated GHD), and from 3.94 (1.30) at baseline to 3.74 (1.19) after 5 years (combined GHD).
Quality of Life Subgroup Analysis
QoL data are reported for the UK, where the QoL tool recommended in National Institute for Health and Care Excellence (NICE) guidance is typically used in routine clinical practice. Changes in QoL from the previous assessment are shown in Figure 2. Within the first year of treatment, 38.1% of the 189 evaluable rhGH-naïve patients had a documented improvement in QoL and 3.7% had no improvement. This trend continued for the duration of the study, with more patients reporting an improvement than a worsening of QoL at most time points.
 |
Figure 2 Quality-of-life change from previous assessment within the first year for rhGH-naïve patients in the UK (effectiveness population subgroup, N = 189). Abbreviations: GHD, growth hormone deficiency; rhGH, recombinant human growth hormone. |
Discussion
The PATRO Adults post-marketing surveillance study provides data on the long-term safety and effectiveness of biosimilar rhGH treatment in adult patients with GHD treated in routine clinical practice. Based on the analysis of final data from this study, there were no unexpected safety signals, and treatment with biosimilar rhGH was effective in both rhGH-naïve and pretreated patients. These findings align with those from the concurrent PATRO Children study, which was conducted in pediatric patients treated with biosimilar rhGH.13
In the analysis of final data, there were 44 cases of new-onset diabetes mellitus and five cases of worsening or inadequately controlled pre-existing diabetes mellitus. Previous analyses of data from PATRO Adults (data cutoff July 2018) found no evidence of an increased risk of diabetes mellitus and glucose metabolism disorders with biosimilar rhGH, with newly diagnosed diabetes mellitus observed in 15 patients (incidence rate of 3.61 per 1000 patient-years).7 In the analysis reported here, newly diagnosed diabetes mellitus was observed in 44 patients (incidence rate of 6.03 per 1000 patient-years). The observed increase over time in the number of new cases of diabetes mellitus in PATRO Adults aligns with the increase in non–insulin-dependent diabetes mellitus observed with increasing age.14 These findings are consistent with findings for other rhGH treatments, showing no evidence of an increased risk of diabetes mellitus with rhGH in adult patients. In the Global HypoCCS surveillance study including adult patients with GHD treated with rhGH Humatrope® (Eli Lilly and Co., Indianapolis, Indiana, USA), the incidence of diabetes mellitus was 7.0 per 1000 patient-years in Europe.15 In an analysis of the non-interventional NordiNet® study in non-diabetic patients with adulthood-onset GHD, treatment with rhGH Norditropin® (Novo Nordisk, Plainsboro, New Jersey, USA) did not have an adverse impact on glucose homeostasis in most patients.16 Reported cases of diabetes mellitus in the PATRO Adults study were similar to, or possibly lower than, what would be expected in the enrolled population based on their demographic characteristics (60% of patients were aged ≥45 years) and presence of other risk factors (eg, BMI >30 kg/m2, GH pretreatment). Analysis of data from large-scale registry studies of patients receiving GH replacement therapy concluded that the incidence of diabetes mellitus may be slightly increased only in patients with pre-existing risk factors for diabetes mellitus, rather than due to changes resulting from rhGH therapy.17
A total of 84 malignancies were reported during the study, of which 71 events in 63 patients were newly diagnosed (incidence rate 8.64 per 1000 patient-years), with the most frequently reported newly diagnosed malignancies basal cell carcinoma, prostate cancer, breast cancer, and malignant melanoma. This aligns with previously reported data on the occurrence of on-study malignancies in PATRO Adults (data from July 2018); in this analysis, there were 41 malignancies reported in 33 patients (incidence rate 7.94 per 1000 patient-years).8 Overall, data from PATRO Adults suggest that biosimilar rhGH does not increase the risk of malignancies in adults with GHD, although there may be an increased risk of second malignancies in patients with a history of cancer. These findings are consistent with those in previously published data on the risk of malignancies in adult GHD patients receiving GH replacement therapy.17,18
The current analysis of the efficacy of biosimilar rhGH suggests improvements in body composition (lean body mass), blood lipid profile (TC/HDL ratio), and QoL in patients who were rhGH-naïve at study entry, consistent with the interim analysis from PATRO Adults9 and previously reported benefits of rhGH therapy in adult patients.2,19 This was supported by results of the subgroup analysis. However, information on concomitant medication with cholesterol-lowering medication was not available. In addition, the heterogeneity of the underlying pituitary disease and treatments of other pituitary deficiencies may have affected the results.
The PATRO Adults study has several limitations that are common to all observational or registry studies. These include the potential for selection bias through inclusion of selected clinics (and enrollment of patients from these clinics), and information bias from incorrect recording when study data were collected during routine clinical practice (ie, no regular visit schedule), and perhaps using different techniques to measure the same parameter. Also, AEs may have been under-reported because of the extended time periods (6–12 months) between patient visits and restricted consultation time during visits. In addition, the relatively small sample size for rare events such as neoplasms is also a potential limitation, hindering the interpretation of certain data, while useful information may have been missed because of how the eCRF was set up.
Conclusions
This analysis of the final global data from PATRO Adults indicates that biosimilar rhGH (Omnitrope) is not associated with any unexpected safety signals and is effective in adults with GHD treated in real-world clinical practice, in line with previous interim analyses, and extends the global safety of biosimilar rhGH across a large diverse patient population. This adds to the growing clinical experience with biosimilar rhGH and other approved biosimilars in other indications, offering reassurance that these agents are as effective as, and have safety profiles in line with, other medications in the therapeutic class. Ultimately, these findings provide the opportunity to transform healthcare by expanding access to new and innovative treatments.
Abbreviations
AE, adverse event; BMI, body mass index; eCRF, electronic case report form; GH, growth hormone; GHD, growth hormone deficiency; HDL, high-density lipoprotein; IGF-1, insulin-like growth factor-1; MedDRA, Medical Dictionary for Regulatory Activities; NICE, National Institute for Health and Care Excellence; PR, preferred term; QoL, quality of life; rhGH, recombinant human growth hormone; SAE, serious adverse event; SD, standard deviation; SDS, standard deviation score; SOC, system organ class; TC, total cholesterol.
Ethics Approval and Informed Consent
The PATRO Adults study protocol was approved by the ethics review committee of participating centers in accordance with national laws and regulations. The full details of all ethics review committees can be found in Supplementary Table 1. The study was conducted according to the ethical principles of the Declaration of Helsinki (1964) and its later amendments.
Consent to Participate
All patients provided written informed consent. Patients were permitted to withdraw their informed consent at any time or discontinue biosimilar rhGH treatment for any reason. Consent for publication was not applicable.
Acknowledgments
The authors thank all patients and investigators who participated in the PATRO Adults study.
Medical writing support was provided by Eve Blumson and Caroline McGown of Apollo, OPEN Health Communications, and was funded by Sandoz/Hexal AG, in accordance with Good Publication Practice (GPP) guidelines (www.ismpp.org/gpp-2022). All authors have authorized the submission of their manuscript via a third party and approved all statements and declarations. Statistical input was provided by Masiur Rahman of Novartis Pharmaceuticals, Wallingford, CT, USA.
Funding
The PATRO Adults study was funded by HEXAL AG (a Sandoz Company). HEXAL AG (a Sandoz company) were involved in all stages of the study, from design to submission of the paper for publication.
Disclosure
Paolo Beck-Peccoz and Suat Simsek are members of the global steering committee for the PATRO Adults study. Charlotte Höybye has acted as an investigator for Novo Nordisk, Pfizer, and Sandoz; has received lecture fees from Novo Nordisk, Pfizer, and Sandoz; and is a member of the global steering committee for the PATRO Adults study. Günter Stalla has received honoraria for scientific advisory work and/or reimbursement of delegate fees for congresses/seminars and/or travel costs and/or research grants from the HRA, Ipsen, Lilly, Novartis, Novo Nordisk, Pfizer, Sandoz, and Shire; and is a member of the global steering committee for the PATRO Adults study. Robert D Murray has received research funding from Ipsen, Pfizer, and Sandoz; has received lecture fees from Pfizer; and is a member of the global steering committee for the PATRO Adults study. Altaher Esmael and Markus Zabransky are employees of HEXAL AG (a Sandoz Company), Holzkirchen, Germany. Dragan Urosevic is an employee of Novartis Sandoz Biopharmaceutical AG, c/o HEXAL AG, Basel, Switzerland. Anca Boldea was an employee of HEXAL AG (a Sandoz Company), Holzkirchen, Germany, when the study and manuscript development were undertaken. The authors report no other conflicts of interest in this work.
References
1. Ho KK. GH Deficiency Consensus Workshop Participants. Consensus guidelines for the diagnosis and treatment of adults with GH deficiency II: a statement of the GH Research Society in association with the European Society for Pediatric Endocrinology, Lawson Wilkins Society, European Society of Endocrinology, Japan Endocrine Society, and Endocrine Society of Australia. Eur J Endocrinol. 2007;157(6):695–700. doi:10.1530/EJE-07-0631
2. Molitch ME, Clemmons DR, Malozowski S, Merriam GR, Vance ML. Endocrine Society. Evaluation and treatment of adult growth hormone deficiency: an Endocrine Society clinical practice guideline. J Clin Endocrinol Metab. 2011;96(6):1587–1609. doi:10.1210/jc.2011-0179
3. Bianchi A, Giampietro A, Pontecorvi A, De Marinis L. Isolated growth hormone deficiency: clinical entity? J Endocrinol Invest. 2008;31(9 Suppl):12–15.
4. Höybye C, Beck-Peccoz P, Simsek S, et al. Safety of current recombinant human growth hormone treatments for adults with growth hormone deficiency and unmet needs. Expert Opin Drug Saf. 2020;19(12):1539–1548. doi:10.1080/14740338.2020.1839410
5. Romer T, Zabransky M, Walczak M, Szalecki M, Balser S. Effect of switching recombinant human growth hormone: comparative analysis of phase 3 clinical data. Biol Ther. 2011;1(1):5. doi:10.1007/s13554-011-0004-8
6. López-Siguero JP, Pfäffle R, Chanson P, Szalecki M, Höbel N, Zabransky M. Ten years’ clinical experience with biosimilar human growth hormone: a review of efficacy data. Drug Des Devel Ther. 2017;11:1489–1495. doi:10.2147/DDDT.S130320
7. Beck-Peccoz P, Höybye C, Murray RD, et al. No increased risk of glucose metabolism disorders in adults with growth hormone deficiency undergoing long-term treatment with biosimilar somatropin (Omnitrope®): data from an observational, longitudinal study. BMC Endocr Disord. 2019;19(1):138. doi:10.1186/s12902-019-0464-2
8. Beck-Peccoz P, Höybye C, Murray RD, et al. Malignancy risk in adults with growth hormone deficiency undergoing long-term treatment with biosimilar somatropin (Omnitrope®): data from the PATRO Adults study. Ther Adv Endocrinol Metab. 2020;11:2042018820943377. doi:10.1177/2042018820943377
9. Höybye C, Beck-Peccoz P, Murray RD, et al. Safety and effectiveness of replacement with biosimilar growth hormone in adults with growth hormone deficiency: results from an international, post-marketing surveillance study (PATRO Adults). Pituitary. 2021;24(4):622–629. doi:10.1007/s11102-021-01139-2
10. Beck-Peccoz P, Minuto F, Leal-Cerro A, Zabransky M, Stalla G. Rationale and design of PATRO Adults, a multicentre, noninterventional study of the long-term efficacy and safety of Omnitrope® for the treatment of adult patients with growth hormone deficiency. Ther Adv Endocrinol Metab. 2012;3(3):85–91. doi:10.1177/2042018812444152
11. European Medicines Agency. Summary of Product Characteristics: omnitrope 1.3 mg/mL powder and solvent for solution for injection. Available from: https://www.ema.europa.eu/en/documents/product-information/omnitrope-epar-product-information_en.pdf. Published 2023.
12. European Medicines Agency. ICH Topic E 6 (R1): Guideline for Good Clinical Practice. Available from: https://www.ema.europa.eu/en/documents/scientific-guideline/ich-e6-r1-guideline-good-clinical-practice_en.pdf.
13. Loche S, Kanumakala S, Backeljauw P, et al. Safety and effectiveness of a biosimilar recombinant human growth hormone in children requiring growth hormone treatment: analysis of final data from PATRO Children, an international, post-marketing surveillance study. Drug Des Devel Ther. 2024;18:667–684. doi:10.2147/DDDT.S440009
14. Liu J, Ren ZH, Qiang H, et al. Trends in the incidence of diabetes mellitus: results from the Global Burden of Disease Study 2017 and implications for diabetes mellitus prevention. BMC Public Health. 2020;20(1):1415. doi:10.1186/s12889-020-09502-x
15. Attanasio AF, Jung H, Mo D, et al. Prevalence and incidence of diabetes mellitus in adult patients on growth hormone replacement for growth hormone deficiency: a surveillance database analysis. J Clin Endocrinol Metab. 2011;96(7):2255–2261. doi:10.1210/jc.2011-0448
16. Weber MM, Biller BM, Pedersen BT, Pournara E, Christiansen JS, Höybye C. The effect of growth hormone (GH) replacement on blood glucose homeostasis in adult nondiabetic patients with GH deficiency: real-life data from the NordiNet® International Outcome Study. Clin Endocrinol (Oxf). 2017;86(2):192–198. doi:10.1111/cen.13256
17. Stochholm K, Kiess W. Long-term safety of growth hormone–a combined registry analysis. Clin Endocrinol (Oxf). 2018;88(4):515–528. doi:10.1111/cen.13502
18. Krzyzanowska-Mittermayer K, Mattsson AF, Maiter D, et al. New neoplasm during GH replacement in adults with pituitary deficiency following malignancy: a KIMS analysis. J Clin Endocrinol Metab. 2018;103(2):523–531. doi:10.1210/jc.2017-01899
19. Höybye C, Burman P, Feldt-Rasmussen U, et al. Change in baseline characteristics over 20 years of adults with growth hormone (GH) deficiency on GH replacement therapy. Eur J Endocrinol. 2019;181(6):629–638. doi:10.1530/EJE-19-0576
 © 2024 The Author(s). This work is published and licensed by Dove Medical Press Limited. The
full terms of this license are available at https://www.dovepress.com/terms
and incorporate the Creative Commons Attribution
- Non Commercial (unported, 3.0) License.
By accessing the work you hereby accept the Terms. Non-commercial uses of the work are permitted
without any further permission from Dove Medical Press Limited, provided the work is properly
attributed. For permission for commercial use of this work, please see paragraphs 4.2 and 5 of our Terms.
© 2024 The Author(s). This work is published and licensed by Dove Medical Press Limited. The
full terms of this license are available at https://www.dovepress.com/terms
and incorporate the Creative Commons Attribution
- Non Commercial (unported, 3.0) License.
By accessing the work you hereby accept the Terms. Non-commercial uses of the work are permitted
without any further permission from Dove Medical Press Limited, provided the work is properly
attributed. For permission for commercial use of this work, please see paragraphs 4.2 and 5 of our Terms.