Back to Journals » Open Access Journal of Contraception » Volume 11
Rural–Urban Differentials of Long-Acting Contraceptive Method Utilization Among Reproductive-Age Women in Amhara Region, Ethiopia: Further Analysis of the 2016 EDHS
Authors Wondie KY ![]() , Badi MB
, Badi MB ![]() , Tamiru AT
, Tamiru AT ![]()
Received 31 March 2020
Accepted for publication 25 June 2020
Published 5 August 2020 Volume 2020:11 Pages 77—89
DOI https://doi.org/10.2147/OAJC.S255551
Checked for plagiarism Yes
Review by Single anonymous peer review
Peer reviewer comments 3
Editor who approved publication: Professor Igal Wolman
Kindu Yinges Wondie,1 Marta Berta Badi,2 Animut Tagele Tamiru3
1Department of Clinical Midwifery, School of Midwifery, University of Gondar, Gondar, Amhara Regional State, Ethiopia; 2Department of Women’s and Family Health, School of Midwifery, University of Gondar, Gondar, Amhara Regional State, Ethiopia; 3Department of General Midwifery, School of Midwifery, University of Gondar, Gondar, Amhara Regional State, Ethiopia
Correspondence: Animut Tagele Tamiru Email [email protected]
Background: The sharp fertility drop-off in the Amhara region between 2000 and 2011 was due to an increase in modern contraceptive utilization of rural women. However, long-acting contraceptive method utilization was higher among urban than rural women. Therefore, this study aimed to assess rural–urban differentials of long-acting contraceptive method utilization and the contributing factors among reproductive-age women in the Amhara region: analysis of the 2016 EDHS.
Methods: The 2016 EDHS data were used. A weighted sample of 2188 (1675 rural and 513 urban) fecund reproductive-age women was used, and a mixed-effects logistic regression model was fitted. Multivariable logistic regression analysis at a P-value < 0.05 and adjusted odds ratio with a 95% confidence interval were used to declare significant associations.
Results: The overall long-acting contraceptive method use was 13.3% (95% CI=11.6– 15.8), and it was 14.8% (95% CI=12.4– 17.2) among rural and 8.3% (95% CI=4.5– 12.4) among urban women. Among urban women, the odds of long-acting contraceptive method use was higher for women living with a partner (AOR=6.83; 95% CI=1.23– 37.84), married women (AOR=5.21; 95% CI=1.95– 13.89), women living in a male-headed household (AOR=5.29; 95% CI=1.26– 22.38), and women whose partner wanted fewer children (AOR=11; 95% CI=3.46– 16.2). Among rural women, the odds of long-acting contraceptive use was higher for women in the richest wealth index (AOR=6.69; 95% CI=3.02– 14.83), married women (AOR=30.26; 95% CI=8.81– 42.9), women with good knowledge of LACMs (AOR=1.75; 95% CI=1.25– 2.46), and women who had no correct knowledge of their ovulatory cycle (AOR=1.93; 95% CI=1.16– 3.19).
Conclusion: Long-acting contraceptive method use was lower than the national target. LACM use was 8.3% (95% CI=4.5– 12.4) among urban and 14.8% (95% CI=12.4– 17.2) among rural women. Overall, marital status, educational level, the total number of children, knowledge of LACMs, and correct knowledge of the ovulatory cycle were significantly associated with LACM use.
Keywords: Amhara region, comparative cross-sectional study, long-acting contraceptive methods
Introduction
In the developing regions of the world, half of the sexually active women want to avoid pregnancy. But a 44% unintended pregnancy rate continues to be a major global problem, posing social, economic, and health challenges.1
Unintended pregnancy was recorded as 29% in Sub-Saharan African countries.2 The 2016 Ethiopian demographic and health survey (EDHS) reported that one in every four births was unintended.3 Births from unintended pregnancy are prone to many problems, and unintended pregnancy itself is a burden on public resources.4,5
Long-acting contraceptive methods (LACMs), which can prevent pregnancy from 3 years to life-long, are better options to avoid unintended pregnancy due to their high efficacy and better safety.6,7 Moreover, women who are using short-acting contraceptives are 21-times more likely to face an unintended pregnancy than those using LACMs.8
Around 56% of the global contraceptive method mix is covered by LACMs (Intrauterine device (IUD), implants, and sterilization). Yet most women in Africa, including Ethiopia, rely on short-acting methods.9,10 From a projection study in Sub-Saharan Africa, it will take only 5 years to prevent 1.8 million unintended pregnancies if 20% of oral contraceptive and injectable users switch to implants.11
The Ethiopian government planned to have a 33% implants and 15% IUCD (intrauterine contraceptive devices) share in the total method mix by 2020. However, 16% of urban and only 9.2% of rural women were using LACMs (long-acting contraceptive methods) in 2016.3,12
There is a 25% vs 11% rural–urban unmet need difference, and unmarried sexually active women also had a higher demand than married Ethiopian women (85% vs 58%). The unmet need in the Amhara region was 17% in 2016 and half of the women wanted to stop childbearing after they gave birth to their fourth child, which means a higher need for long-acting contraceptive methods.3
The change in modern contraception utilization of rural women was responsible for the observed drop-off in fertility in the Amhara region during 2000–2011. Contraception was the single most determinant factor for this change. However, its fertility constraining effect was higher for urban women than rural women.13 Yet, the LACM utilization of the rural women in the Amhara region was not determined.
Long-acting and permanent contraceptive method utilization among married reproductive-age women in Amhara regional state was 34.7% (Gondar town),14 12.9% (Janamora District),15 and 19.5% (Debre Markos town).16
From studies in Ethiopia, LACM utilization was 11.6% (EDHS 2016 data),17 12.3% (Mekelle town),18 20% (Nekemte town),19 16.3% (Bombe District),20 and 8.8% (Jijiga town).21 A comparative cross-sectional study from the Tigray region found that intrauterine devices and implant use were 37.8% in rural and 19.9% in urban married reproductive-age women, respectively.22
Evidence from western Kenya found that LACM use was 57% among contraceptive-user women.23 In order to determine the LACM adopted among women based on the place of their residence, this study was aimed to assess the rural–urban differentials of long-acting contraceptive method utilization and the associated factors among reproductive-age women in Amhara region, Northwest Ethiopia.
Methods
Data Source
The 2016 Ethiopian demographic and health survey (EDHS) data was a cross-sectional survey collected by the central statistics agency at the request of the Federal Ministry of Health.
The survey used a list of enumeration areas from the 2007 housing and population census and followed a two-stage stratified random sampling technique. First, each region was stratified into urban and rural. In the first stage, enumeration areas were selected independently in each stratum, and households were selected in the second stage. The EDHS collected information about contraceptive use from all non-pregnant, fecund, reproductive-age women using a structured and pretested questionnaire from January 18, 2016, to June 27, 2016.
From 15,683 interviewed reproductive-age women for the 2016 EDHS, 1719 were from the Amhara region. After 716 women were excluded because of being pregnant, being postpartum amenorrheic, or menopausal at the time of the survey, 1003 fecund reproductive-age women were included for analysis (Figure 1).
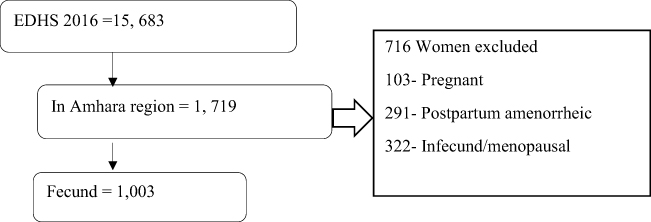 |
Figure 1 Schematic presentation of the selection of reproductive-age women to identify factors associated with LACM contraceptive methods utilization, Amhara region, Ethiopia, 2016. |
Measurement
Outcome Variable
The outcome variable for this study was the long-acting contraceptive method utilization.
Independent Variables
The independent variables were grouped into socio-demographic, reproductive health and fertility-related, and family planning program exposure variables.
Socio-Demographic Variables
Age, religion, marital status, educational level, husband’s educational level, occupation, husband’s occupation, working status, wealth index, sex of head of the household, and relationship to the head of the household.
Fertility and Reproductive Health-Related Variables
Age at first marriage, the ideal number of children, the total number of children ever born, history of abortion, number of living children, sex composition of living children, desire for more children, fertility preference, and husband’s desire for more children.
Family Planning Program Exposure Variables
Knowledge of long-acting contraceptive methods, media exposure to family planning programs, exposure to media, knowledge of fertility, and correct knowledge of the ovulatory cycle.
Good Knowledge to Family Planning
If the woman scored above the mean on the summative score of family planning question.
Good Media Exposure to Family Planning
If the woman answered she has heard of family planning via radio, television, newspaper, and or text messages at least once per week.
Analytical Methods
After getting permission, the data were downloaded from the DHS program’s official database. The data were weighted to consider disproportionate sampling and non-response. Cross-tabulations and summary statistics were done using STATA version 14 software.
The EDHS data structure is hierarchical. Women are nested in a cluster and we expect that women within the same cluster may be more similar to each other than women in the rest of the region. Similarly, women in the same enumeration area may be more similar to each other than women in the rest of the region, which violates the assumption of the traditional regression model which is independent of observations and equal variance across clusters and enumeration areas. It implies the need to take the between-cluster-variability into account by using an advanced model. Therefore, a mixed effect logistic regression model was fitted after checking the Intraclass Correlation Coefficient (ICC). Since the outcome variable was binary, Generalized Linear Mixed Models (GLMM) were fitted. Variables with a P-value <0.2 in the bi-variable analysis were selected for the multivariable mixed-effect logistic regression model. Adjusted Odds Ratio (AOR) with a 95% Confidence Interval (CI) and P-value <0.05 in the multivariable analysis were used to declare a significant association with long-acting contraceptive method use.
Result
Socio-Demographic Characteristics of Reproductive-Age Women
From all fecund reproductive-age women, 513 (23.5%) and 1675 (76.5%) were urban and rural residents, respectively. The mean age of urban and rural women was 27.13±9.03 and 28.02±9.48, respectively.
The majority (85%) and (83.6%) of urban and rural women, respectively were Orthodox Christians, and a high proportion (55.3%) of women were married, of whom 46.4% were wives for the head of the household. The majority of households in which women were living were headed by males (73%). The greater number (62.2%) of urban women were secondary and higher educated, with only 27.7% of rural women fitting this criteria.
By occupation, 45.8% of women were agricultural workers and 71.2% of all women were working at the time of the survey.
Regarding household wealth, 89.7% of urban and 25.5% of rural women were from households in the richest wealth index (Table 1).
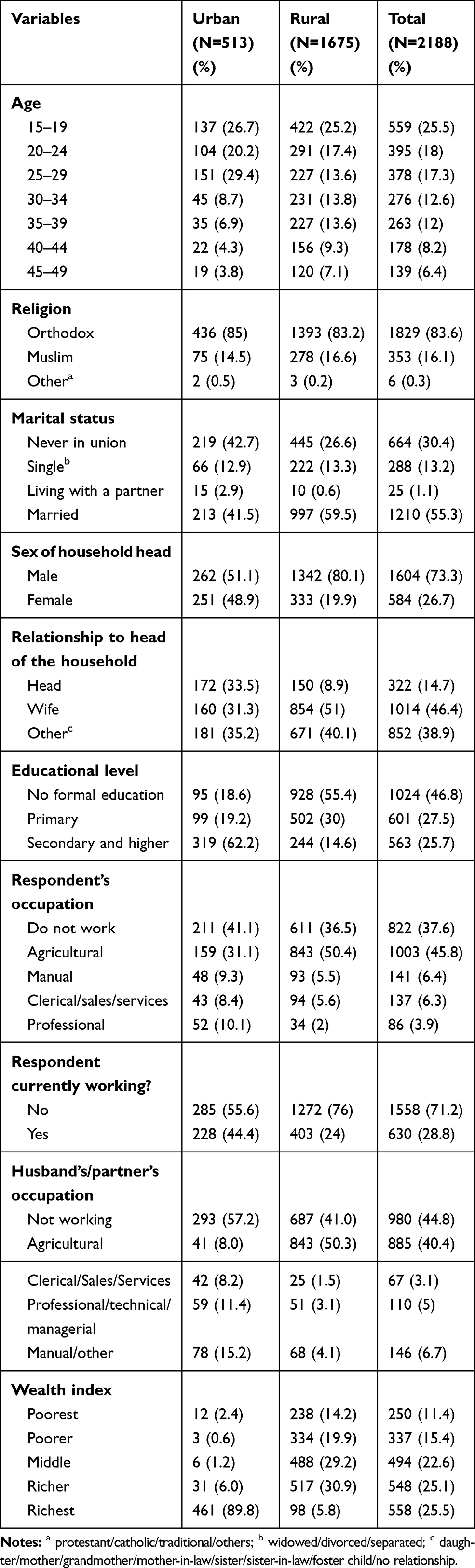 |
Table 1 Socio-Demographic Characteristics of Urban Reproductive-Age Women, Amhara Region, Ethiopia 2016 |
Fertility and Reproductive Health Characteristics
The mean age at first marriage for urban and rural women was 17.24±4.54 and 15.86±3.74, respectively. Marriage before the 19th birthday was 42.7% among urban and 26.6% among rural women. The majority of women (61.5%) mentioned having between one and three children as ideal, with 20% having given birth to more than four children.
Women having an equal number of sons and daughters or having no child at all accounted for 75.4% and 63.4% among urban and rural women, respectively.
More than half (53.3%) of women’s husbands or partners want more children than the wife wants.
When asked about the possibility of getting pregnant after birth and before the menstrual period resumed, 60.3% of all women answered yes (Table 2).
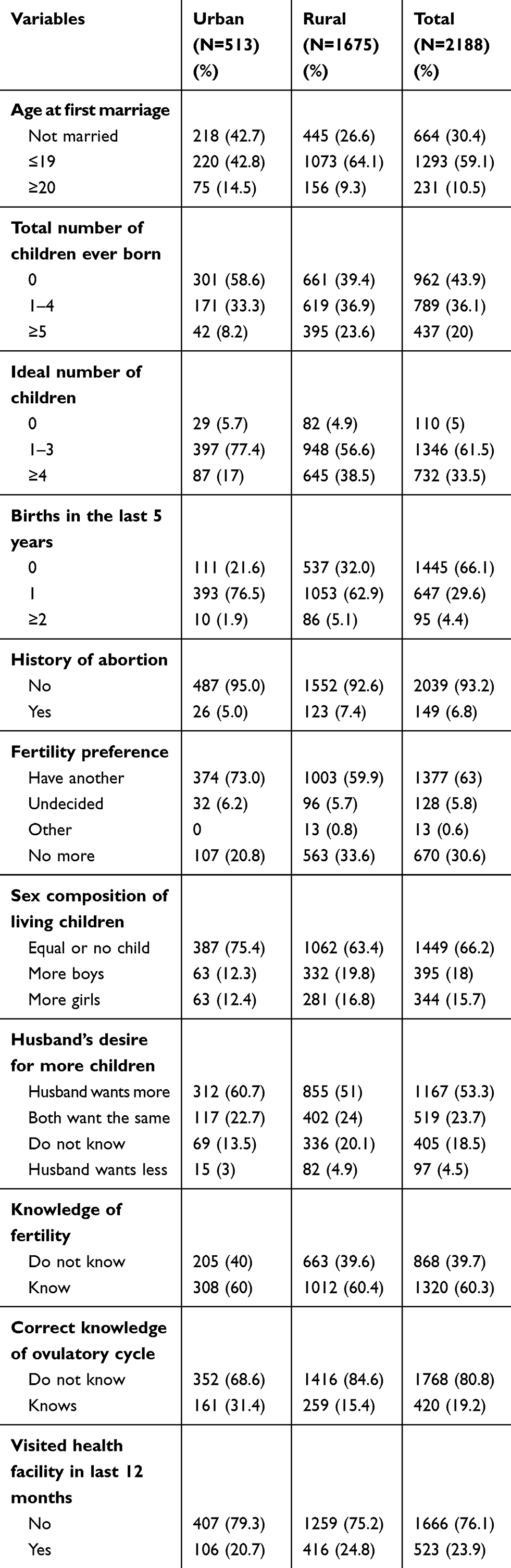 |
Table 2 Fertility and Reproductive Health Characteristics of Reproductive-Age Women, Amhara Region, Ethiopia, 2016 |
Exposure to Family Planning Program
Among urban women, 80.4% had good knowledge of long-acting contraceptive methods, with 58.3% of rural women doing so. Two-thirds (66.5%) of urban women had good media exposure, while 79.4% of rural women had poor media exposure to family planning programs.
A greater share (90.4%) of rural women had poor exposure to any type of media, with 56.6% of urban women having good exposure to media (Table 3).
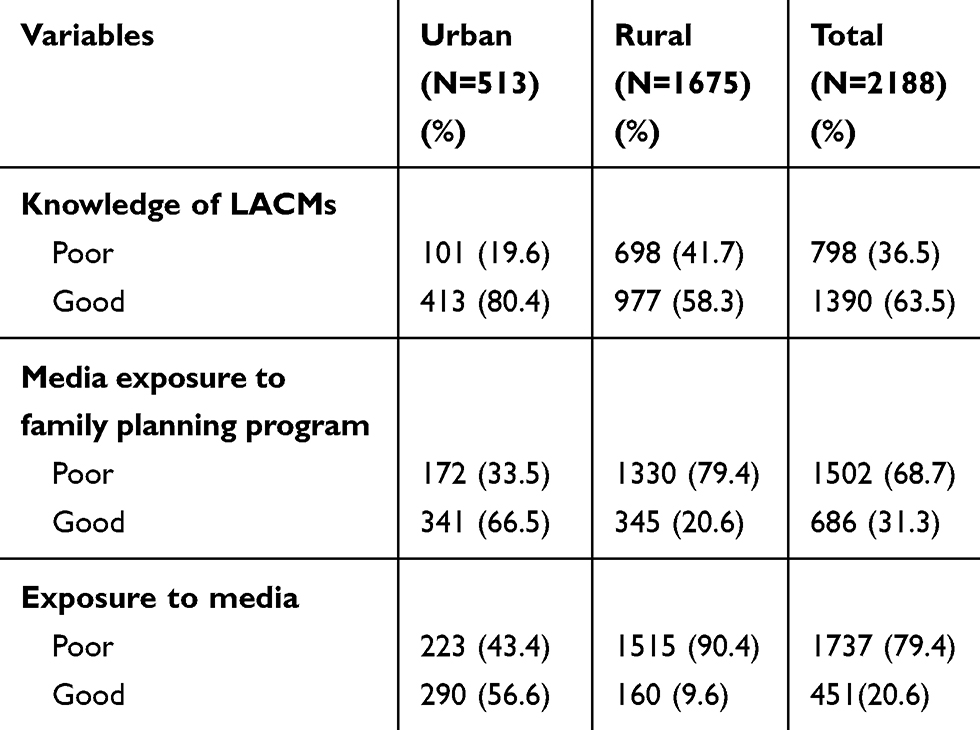 |
Table 3 Exposure to Family Planning Program Among Reproductive-Age Women, Amhara Region, Ethiopia, 2016 |
Prevalence of Long-Acting Contraceptive Method Utilization
The overall LACM use was 13.3% (95% CI=11.6–15.8). LACM use among rural and urban women was 14.8% (95% CI=12.4–17.2) and 8.3% (95% CI= 4.5–12.4), respectively (Figure 2).
 |
Figure 2 LACM use in urban and rural reproductive-age women, Amhara region, Ethiopia, 2016. |
Factors Associated with Long-Acting Contraceptive Method Utilization
Factors Associated with LACM Utilization Among Urban Women
Marital status, sex of the household head, educational level, and husband or partner’s desire for more children were significantly associated with long-acting contraceptive method utilization on multivariable logistic regression analysis (Table 4).
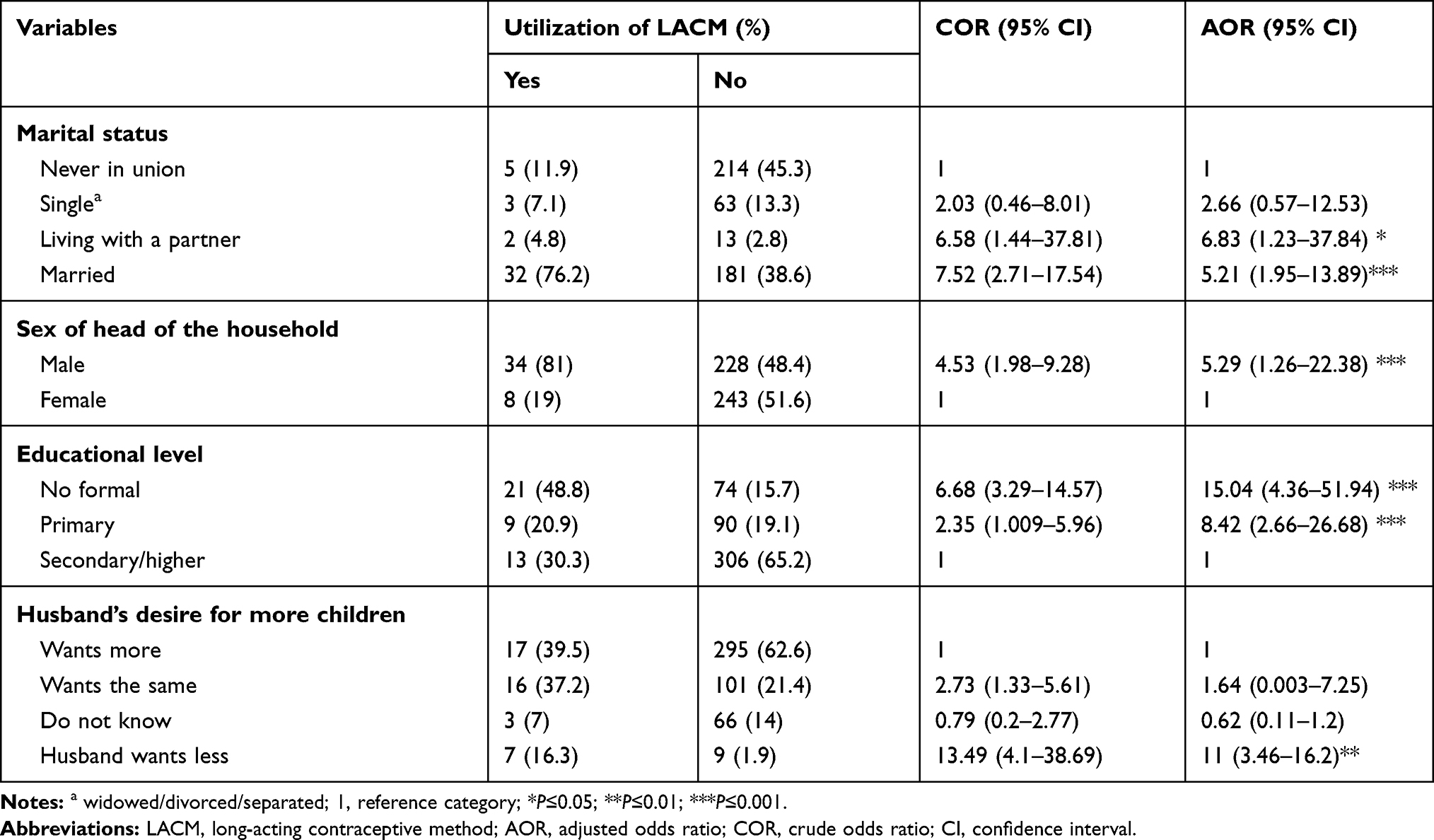 |
Table 4 Bivariable and Multivariable Logistic Regression Analysis of Factors Affecting LACM Utilization of Urban Reproductive-Age Women, Amhara Region, Ethiopia, 2016 (N=513) |
Regarding their marital status, women who were living with their partners and those who were legally married were 7- (AOR=6.83; 95% CI=1.23–37.84) and 5- (AOR=5.21; 95% CI=1.95–13.89) times more likely to use LACM than never in-union women.
Compared to women living in female-headed households, the odds of using long-acting contraceptive method use were 5-times (AOR=5.29; 95% CI=1.26–22.38) higher among women living in male-headed households.
Women who had no formal education were 15- (AOR=15.04; 95% CI=4.36–51.94) times more likely to use LACMs than women who had secondary and above education. Similarly, those women who had primary education were 8- (AOR=8.42; 95% CI=2.66–26.68) times more likely to use LACMs compared to women who had secondary and higher education.
The odds of LACM use was 11-times (AOR=11; 95% CI=3.46–16.2) higher among women whose husband or partner was wanting less children than women whose husband or partner was wanting more children (Table 4).
Factors Associated with LACM Utilization Among Rural Women
Marital status, wealth index, knowledge of long-acting contraceptive methods, correct knowledge of the ovulatory cycle, among those visited by a field worker in the last 12 months of the survey showed significant association with LACM utilization in the multivariable logistic regression analysis (Table 5).
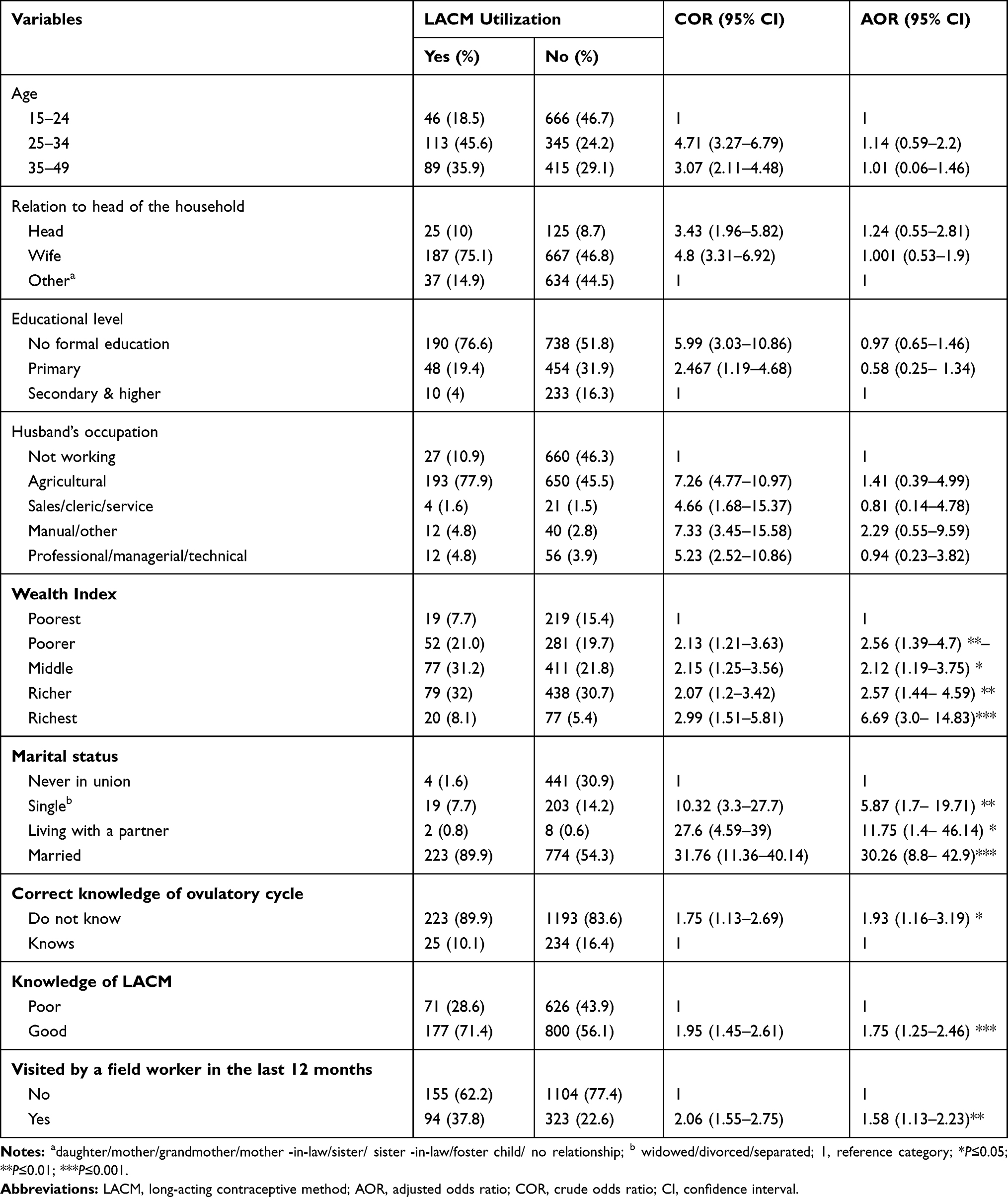 |
Table 5 Bivariable and Multivariable Logistic Regression Analysis of Factors Affecting LACM Utilization of Rural Reproductive-Age Women, Amhara Region, Ethiopia, 2016 (N=1675) |
Regarding marital status, the odds of LACM use among single women were 6-times higher (AOR=5.87; 95% CI=1.75–19.71) compared to never in-union women. LACM use was also 12-times (AOR=11.75; 95% CI=1.41–46.14) higher among women living with their partner. Married women were 30-times (AOR=30.26; 95% CI=8.81–42.9) more likely to use LACMs than women who were never in a union.
Compared to women in the lowest wealth quintile, the odds of LACM use among women in the lower wealth quintile were 3-times (AOR=2.56; 95% CI=1.39–4.7). Women in the middle wealth quintile were 2-times (AOR=2.12; 95% CI=1.19–3.75) more likely to use LACMs compared with those in the lowest wealth quintile. In contrast to women in the lowest quintile, women in the higher wealth quintile were 6-times (AOR=2.57; 95% CI=1.44–4.59) more likely to use LACMs. Similarly, the odds of LACM use was 7-times (AOR=6.69; 95% CI=3.02–14.83) higher among women in the highest wealth index than women in the lowest wealth index.
The odds of LACM use among women having good knowledge of LACMs was 2-times more likely (AOR=1.75; 95% CI=1.25–2.46) compared to those who had poor knowledge.
Women who did not correctly know the time of their ovulatory cycle were 2-times (AOR=1.93; 95% CI=1.16–3.19) more likely to use LACMs than women who correctly knew the time of their ovulatory cycle.
The odds of LACM use were 2-times (AOR=1.58; 95% CI=1.13–2.23) higher among women who were visited by a field worker in the last 12 months than women who were not visited by a field worker in the last 12 months (Table 5).
Factors Associated with LACM Utilization Among the Women Overall
Marital status, educational level, the total number of children ever born, knowledge of LACMs, and correct knowledge of the ovulatory cycle were significantly associated with LACMs on a multivariable logistic regression analysis of women overall.
Compared to women who were never in a union, the odds of LACM use were 3-times (AOR=3.25; 95% CI=1.27–8.36), 40-times (AOR=39.78; 95% CI=4.96–53.3), and more than 20-times (AOR=22.09; 95% CI=4.64–41.1) higher in those who were single, living with a partner, and married, respectively.
The odds of using LACM among women who had no formal education were 3- (AOR=2.85; 95% CI=1.37–5.88) times higher than women who had secondary and higher education.
Women who gave birth to at least one and at most four children were 2- (AOR=1.97; 95% CI=1.03–3.77) times more likely to use LACMs than women who had never given birth.
The odds of LACM use were 2-times (AOR=1.99; 95% CI=1.38–2.87) higher in women who had good knowledge of long-acting contraceptive methods than those who had poor knowledge.
Compared to women who correctly knew the time of their ovulatory cycle, the odds of using LACM were 2 (AOR=2.27; 95% CI=1.38–3.73) times higher among women who did not correctly know the time of their ovulatory cycle (Table 6).
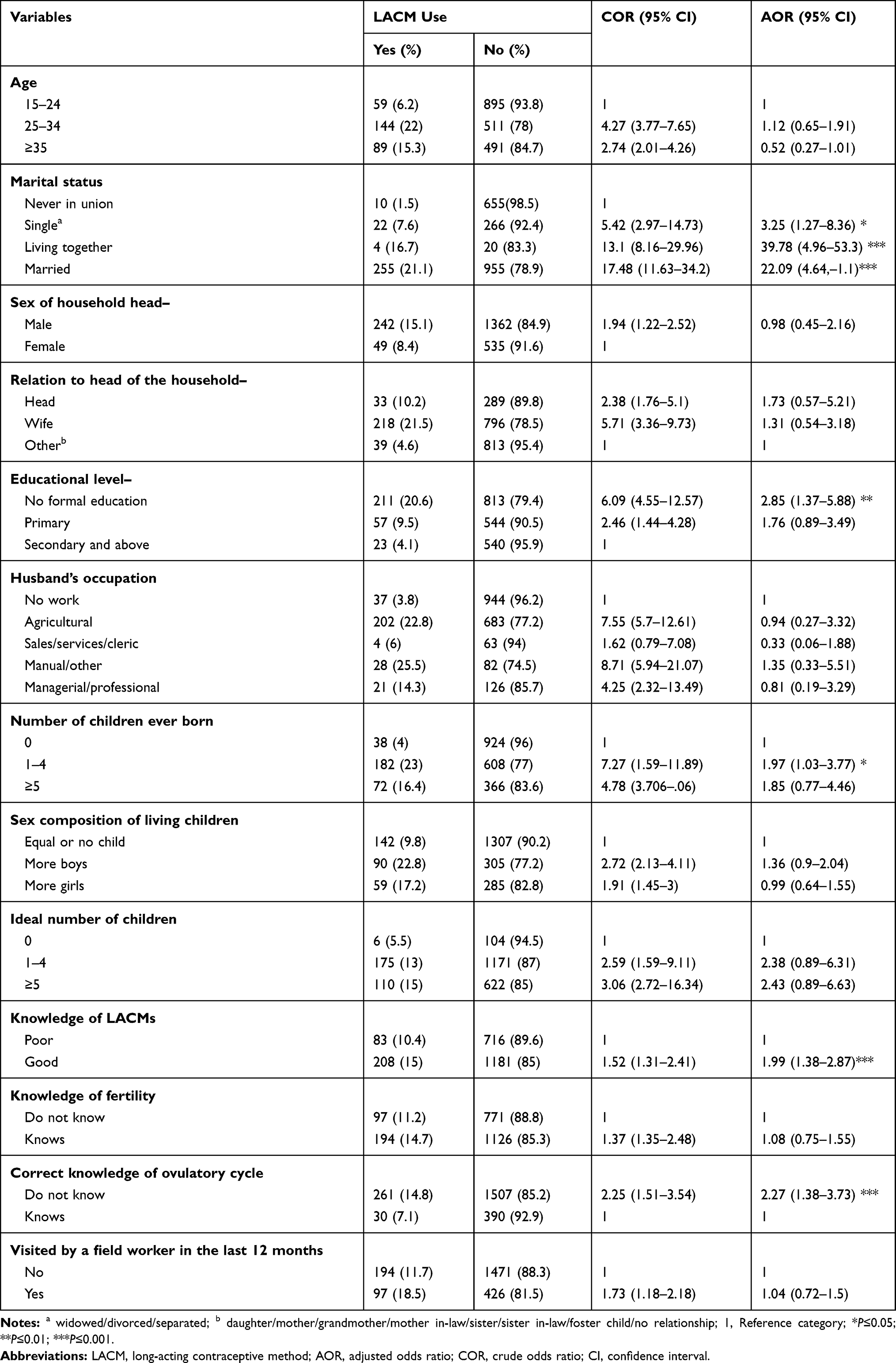 |
Table 6 Bivariable and Multivariable Mixed-Effects Logistic Regression Analysis of Factors Affecting LACM Utilization of Reproductive-Age Women, Amhara Region, Ethiopia, 2016 (N=2188) |
Discussion
The overall prevalence of LACM use was 13.3% (95% CI=11.6–15.8). LACM use was 8.3% (95% CI=4.5–12.4) among urban and 14.8% (95% CI=12.4–17.2) among rural women.
LACM method utilization had no statistically significant difference between urban and rural women (COR=1.85; 95% CI=0.79–4.29).
This non-difference may be due to the free cost of LACMs in Ethiopia and even though LACM use among urban women is expected to be higher than rural women, since the majority of rural women are without formal education, they might be earlier to reach the desired fertility and were using LACMs.
This result is higher than the 2016 EDHS data (11.6%),17 Janamora District (12.9%),15 Jinka town (7.3%),32 and Jijiga town (8.8%).21 The result was also higher than a study in Uganda (7.7%) in urban and (10.9%) in rural women.40
But this is lower than studies from Gondar town (34.7%),14 Debre Markos town (19.5%),16 Mekelle town (19.9%) in urban and (37.8%) in a rural setting,22 Nekemte town (20%),19 and Bombe District, Southern Ethiopia (16.3%).20
One possible reason for this discrepancy may be the difference in LACM utilization due to socio-cultural, socio-demographic, and socio-economic differences. For instance, religious, marital status, and residence differences may affect LACM utilization. Lower LACM prevalence by studies from Jinka and Jijiga town21,32 might be due to these socio-cultural differences.
Otherwise, the higher report might be due to the study population difference, for instance, the study from Gondar (34.7%) was on women who want no more children. The other reason might be the difference in the study area. Most of the studies were done in towns and the majority of them were facility-based and among married women,14,16,22 while this study was on both married and unmarried, rural, and urban women of reproductive age.
The sex of the head of the household was found to be associated with LACM use among urban women. Women who were living in male-headed households were 5- (AOR=5.29; 95% CI=1.26–22.38) times more likely to use LACM than women living in female-headed households.
This finding is in line with the 2016 EDHS data17 and a study from Lesotho.41 This may be attributed to women in female-headed households having less frequent sexual intercourse in that most of them might be unmarried, widowed, divorced, separated, or their husband was living away so that they will not use contraceptives or prefer short-acting methods.
Among the overall women, the odds of LACM use were 3- (AOR=2.85; 95% CI=1.37–5.88) times higher in those with no formal education compared to women of secondary and higher education. Similarly, among urban women, those who had no formal education were 15-times (AOR=15.04; 95% CI=4.3–51.94) more likely to use LACMs than secondary and higher educated women, and the odds of LACM were also 8-times (AOR=8.42; 95% CI=2.66–26.68) higher among women with primary education.
This finding is supported by findings from Rural Nepal,42 Uzbekistan,43 and western Kenya.23 In contrast, the 2011 EDHS data44 and other studies conducted in our country19,45,46 contradict this finding.
Possibly less educated women might attain the desired fertility earlier than higher educated women who will still be pursuing their fertility goals. Educated women may also have better compliant with natural and short-acting methods due to their better reproductive health knowledge, including the time of ovulation.
In urban women, the odds of LACM use were 7- (AOR=6.83; 95% CI=1.23–37.84) and 5- (AOR=5.21; 95% CI=1.95–13.89) times higher for women living with their partner and married women, respectively. Similarly, among rural women, those who were single, women living with their partner, and married women were 6-, 12-, and 30-times (AOR=5.87; 95% CI=1.75–19.71; AOR=11.75; 95% CI=1.41–46.14; AOR=30.26; 95% CI= 8.81–42.91), respectively, more likely to use LACM than women never in a union.
The odds of LACM use were 3- (AOR=3.25; 95% CI=1.27–8.36), 40- (AOR=39.78; 95% CI=4.96–53.3), and more than 20- (AOR=22.09; 95% CI= 4.64–41.1) times for single women, women living with their partner, and married women, respectively, compared to those never in a union among overall women.
This finding is in agreement with the 2011 EDHS data.44 Possibly, to conform to the social norm, women never in a union may avoid sexual intercourse so that they may not use LACMs or they may also prefer short-acting methods just in case they need it.
The other significant factor in urban women is the husband’s desire for more children. That is, women whose husband or partner wanted fewer children were 12-times (AOR=11.; 95% CI=3.46–16.2) more likely to use LACMs than those whose husband or partner was wanting more children than she wants.
This may be because of the husband’s dominance over reproductive health issues due to gender inequality, and their important role in reproductive decision-making including contraceptive use.
Regarding wealth status and among rural women, in contrast to women in the poorest wealth index, those women in the poorer and richer wealth index were 3- (AOR=2.56; 95% CI=1.39–4.7) and (AOR=2.57; 95% CI=1.44–4.59) times higher to use LACMs. Similarly, the odds of LACMs use among women in the middle and the richest wealth index were 2- and 7-times, respectively, higher than women in the poorest wealth quintile.
The 2016 EDHS data and a multi-country study on developing countries support this evidence.17,47
The possible explanation is that wealthy women have a better lifestyle and self-reliance to decision-making on their reproductive health so that they may prefer LACMs.
In the final model, the odds of LACM use for women who gave birth at least once and up to four times were 2- (AOR=1.97; 95% CI=1.03–3.77) times more likely compared with women who have never given birth.
This may be explained by the increasing need for limiting pregnancy after having three children in that between one and three children was ideal for the majority of the study participants.
Women who had good knowledge of LACMs were found to use them 1.8- (AOR=1.75; 95% CI=1.25–2.46) and 2- (AOR=1.99; 95% CI=1.38–2.87) times, respectively, than women who had poor knowledge among rural women and the overall women.
This finding is in line with a study from Janamora district15 and other studies conducted in Ethiopia.18,20,32,48
This could be due to a better understanding of the advantages of LACMs among women with better knowledge about LACMs.
The odds of LACM use in rural women in the final model were 2- (AOR=1.93; 95% CI=1.16–3.19) and (AOR=2.27; 95% CI=1.38–3.73) times higher for women who do not correctly know the time of their ovulatory cycle.
The possible explanation is that women who correctly know the time of their ovulatory cycle might have been using natural methods or those women who do not correctly know the time of the ovulatory cycle might be less educated and less compliant to natural and short-acting methods.
Women who were visited by a field worker in the last 12 months before the survey were 2-times (AOR=1.58; 95% CI=1.13–2.23) more likely to use LACMs than women who were not visited by a fieldworker.
This finding is in line with the 2016 EDHS data.17 This could be due to better reproductive health knowledge including LACMs in women who have been visited by fieldworkers and they will, as a result, choose LACMs.
Limitation of the Study
We assessed only individual-level factors and attitudes, and behavioral factors, especially those related to the husbands or partners, were not addressed due to the nature of the EDHS data.
Conclusion
The overall long-acting contraceptive method use was lower than the national target set in the Ethiopian costed implementation plan. LACM use was 8.3% (95% CI=4.5–12.4) among urban and 14.8% (95% CI=12.4–17.2) among rural women.
In urban women, the odds of LACM use were higher among women who were living with a partner, among married women, among women who were living in a male-headed household, among women with no formal education, among primary educated women, and among women whose husband or partner wanted fewer children.
Among rural women, the odds of LACM use was higher for women in the richer wealth index, for single women, for women who were living with a partner, for married women, for women who did not correctly know the time of their ovulatory cycle, for women with good knowledge of LACMs, and for women who were visited by a field worker in the last 12 months.
In the final model, women who were living with a partner, women who were married, women who had no formal education, women who gave birth to at least one and at most four children, women who had good knowledge of LACMs, and women who did not correctly know the time of their ovulatory cycle have higher LACM utilization.
Therefore, efforts shall be towards enhancing women’s wealth, knowledge of long-acting contraceptive methods, and visits to women by field workers to increase their adoption of these methods.
Abbreviations
AOR, adjusted odds ratio; CI, confidence interval; COR, crude odds ratio; CPR, contraceptive prevalence rate; DHS, demographic and health survey; EDHS, Ethiopian demographic and health survey; IUCD, intrauterine contraceptive device; LACM, long-acting contraceptive method.
Ethics Approval and Consent to Participate
Ethical clearance was obtained from the Ethical review committee of the University of Gondar Department of midwifery and an authorization letter for data access was obtained from the DHS program.
The 2016 EDHS protocol was reviewed and approved by the national ethics review committee of the Federal Democratic Republic of Ethiopia, Ministry of Science and Technology, and the institutional review board of ICF International. Written informed consent was obtained from all women who participated in the EDHS.
Acknowledgments
We would like to thank the University of Gondar for the ethical letter and financial support. Our gratitude also goes to the DHS for allowing data set access.
Author Contributions
All authors contributed to data analysis, drafting or revising the article, gave final approval of the manuscript to be published, and agree to be accountable for all aspects of the work.
Disclosure
The authors declare that they have no competing interests.
References
1. Guttmacher Institute, BMGF. Adding it up: investing in contraception and maternal and newborn health. Guttmacher Inst. 2017;June:1–4.
2. Ameyaw EK, Budu E, Sambah F, et al. Prevalence and determinants of unintended pregnancy in sub-Saharan Africa. PLoS One. 2019;14(8):1–16. doi:10.1371/journal.pone.0220970
3. CSA, Ethiopia. Ethiopia Demographic and Health Survey 2016. Addis Ababa, Ethiopia: CSA and ICF; 2017.
4. Gipson JD, Koenig MA, Hindin MJ. The effects of unintended pregnancy on infant, child, and parental health: a review of the literature. Stud Fam Plann. 2008;39(1):18–38. doi:10.1111/j.1728-4465.2008.00148.x
5. Blumenthal PD, Voedisch A, Gemzell-Danielsson K. Strategies to prevent unintended pregnancy: increasing use of long-acting reversible contraception. Hum Reprod Update. 2011;17(1):121–137. doi:10.1093/humupd/dmq026
6. Winner B, Peipert JF, Zhao Q, et al. Effectiveness of long-acting reversible contraception. N Engl J Med. 2012;67(9):10.
7. Stoddard A, McNicholas C, Peipert JF. Efficacy and safety of long-acting reversible contraception. Drugs. 2011;71(8):969–980. doi:10.2165/11591290-000000000-00000
8. Lotke PS. Increasing use of long-acting reversible contraception to decrease unplanned pregnancy. Obstet Gynecol Clin North Am. 2019;42:557–567. doi:10.1016/j.ogc.2015.07.008
9. United Nation, Department of Economic and Social Affairs PD. Trends in Contraceptive Use Worldwide 2015. Contraception; 2015:1–70.
10. Tsui AO, Brown W, Li Q. Contraceptive practice in Sub-Saharan Africa. Popul Dev Rev. 2017;43(Suppl Suppl 1):166–191. doi:10.1111/padr.12051
11. Hubacher D, Mavranezouli I, McGinn E. Unintended pregnancy in sub-Saharan Africa: magnitude of the problem and potential role of contraceptive implants to alleviate it. Contraception. 2008;78(1):73–78. doi:10.1016/j.contraception.2008.03.002
12. FDRE Ministry of health. Costed Implementation Plan for Family Planning in Ethiopia 2015–2020. 2016:110.
13. Alazbih NM, Tewabe GN, Demissie TD. Contraception and fertility transition in Amhara National Regional State of Ethiopia: an application of BONGAARTS’ model. Fertil Res Pract. 2017;3(1):12. doi:10.1186/s40738-017-0039-8
14. Zenebe CB, Adefris M, Yenit MK, Gelaw YA. Factors associated with utilization of long-acting and permanent contraceptive methods among women who have decided not to have more children in Gondar city. BMC Womens Health. 2017;17(1):75. doi:10.1186/s12905-017-0432-9
15. Shitu Getahun D, Fekadu Wolde H, Fentahun Muchie K, et al. Utilization and determinants of long term and permanent contraceptive methods among married reproductive age women at Janamora district, northwest Ethiopia. BMC Res Notes. 2018;11(1):1–6. doi:10.1186/s13104-017-3088-5
16. Bulto GA, Zewdie TA, Beyen TK. Demand for long-acting and permanent contraceptive methods and associated factors among married women of the reproductive age group in Debre Markos Town, North West Ethiopia. BMC Womens Health. 2014;14(1):46. doi:10.1186/1472-6874-14-46
17. Fekadu GA, Omigbodun AO, Roberts OA, Yalew AW. Factors associated with long-acting and permanent contraceptive methods use in Ethiopia. Contracept Reprod Med. 2019;4(1):1–11. doi:10.1186/s40834-019-0091-3
18. Alemayehu M, Belachew T, Tilahun T. Factors associated with the utilization of long-acting and permanent contraceptive methods among married women of reproductive age in Mekelle town, Tigray region, north Ethiopia. BMC Pregnancy Childbirth. 2012;12(1). doi:10.1186/1471-2393-12-6
19. Melka AS, Tekelab T, Wirth D. Determinants of long-acting and permanent contraceptive methods utilization among married women of reproductive age groups in western Ethiopia: a cross-sectional study. Pan Afr Med J. 2015;21:1–10. doi:10.11604/pamj.2015.21.246.5835
20. Geta W, Asseffa NA, Mekonnen N. Utilization of long-acting and permanent contraceptive methods and associated factors among married childbearing age women in Bombe District, Southern Ethiopia. Reprod Syst Sex Disord. 2018;07(01):1–9. doi:10.4172/2161-038X.1000223
21. Abdisa B, Mideksa L. Factors associated with utilization of long-acting and permanent contraceptive methods among women of reproductive age group in Jigjiga Town. Anat Physiol. 2017;07(02). doi:10.4172/2161-0940.1000254
22. Alemayehu M, Kalayu A, Desta A, Gebremichael H, Hagos T, Yebyo H. Rural women are more likely to use long acting contraceptive in Tigray region, Northern Ethiopia: a comparative community-based cross sectional study. BMC Womens Health. 2015;15(1):71. doi:10.1186/s12905-015-0229-7
23. Amo-Adjei J, Mutua M, Mukiira C, et al. Fertility intentions and the adoption of long-acting and permanent contraception (LAPM) among women: evidence from Western Kenya. BMC Womens Health. 2019;19(1):1–8. doi:10.1186/s12905-019-0716-3
24. Islam AZ. Factors affecting modern contraceptive use among fecund young women in Bangladesh: does couples’ joint participation in household decision making matter? Reprod Health. 2018;15(1):1–9. doi:10.1186/s12978-018-0558-8
25. Mandiwa C, Namondwe B, Makwinja A, Zamawe C. Factors associated with contraceptive use among young women in Malawi: analysis of the 2015–16 Malawi demographic and health survey data. Contracept Reprod Med. 2018;3(1). doi:10.1186/s40834-018-0065-x
26. Yaya S, Uthman OA, Amouzou A, Ekholuenetale M, Bishwajit G. Inequalities in maternal health care utilization in Benin: a population based cross-sectional study. BMC Pregnancy Childbirth. 2018. doi:10.1186/s12884-018-1846-6
27. Abeje G, Id F, Omigbodun AO, et al; Determinants of change in long-acting or permanent contraceptives use in Ethiopia. A multivariate decomposition analysis of data from the Ethiopian demographic and health survey. PLoS One. 2020;15(1):e0227218. doi:10.1371/journal.pone.0227218
28. Lakew Y, Reda AA, Tamene H, Benedict S, Deribe K. Geographical variation and factors influencing modern contraceptive use among married women in Ethiopia: evidence from a national population based survey. Reprod Health. 2013;10(1):1–10. doi:10.1186/1742-4755-10-52
29. Abate MG, Abera Tareke A, Tareke AA, Abera Tareke A. Individual and community level associates of contraceptive use in Ethiopia: a multilevel mixed effects analysis. Arch Public Heal. 2019;77(1):1–12.
30. Adedini SA, Omisakin OA, Somefun OD. Trends, patterns and determinants of long-acting reversible methods of contraception among women in sub-Saharan Africa. PLoS One. 2019;14(6):1–16. doi:10.1371/journal.pone.0217574
31. Bulto GA, Demmissie DB. Practice and intention to use long acting and permanent contraceptive methods among married women of reproductive age in North West Ethiopia. Gynecol Obstet. 2018;8(459):2161–0932.1000459.
32. Mekonnen G, Enquselassie F, Tesfaye G, Semahegn A. Prevalence and factors affecting use of long acting and permanent contraceptive methods in Jinka town, Southern Ethiopia: a cross sectional study. Pan Afr Med J. 2014;18:1–8. doi:10.11604/pamj.2014.18.98.3421
33. Desta SA, Worku A. Usage of long acting reversible contraceptive methods among women who want no more children, in-depth analysis of the Ethiopian demographic and health survey. Science. 2017;5(6):428–439.
34. Dasa TT, Kassie TW, Roba AA, Wakwoya EB, Kelel HU. Factors associated with long-acting family planning service utilization in Ethiopia: a systematic review and meta-analysis. Contracept Reprod Med. 2019;4(1):1–14. doi:10.1186/s40834-019-0095-z
35. Rahman MM, Islam AZ, Islam MR. Rural-urban differentials of knowledge and practice of contraception in Bangladesh. J Popul Soc Stud. 2010;18(2):87–110.
36. Aregay W, Azale T, Sisay M, Gonete KA. Utilization of long acting reversible contraceptive methods and associated factors among female college students in Gondar town, northwest Ethiopia, 2018: institutional based cross-sectional study. BMC Res Notes. 2018;11(1):862. doi:10.1186/s13104-018-3971-8
37. Mesfin YM, Kibret KT. Practice and intention to use long acting and permanent contraceptive methods among married women in Ethiopia: systematic meta-analysis. Reprod Health. 2016;13(1):78. doi:10.1186/s12978-016-0194-0
38. Taye A, Woldie M, Sinaga M. Predictors of long acting reversible contraceptive use among married women visiting health facilities in Jimma Town | OMICS international. J Womens Health Care. 2014;4:1.
39. District K. Barriers to the use of long acting contraceptive methods among married women of reproductive age in Kicukiro District, Rwanda. Int J Sci Res Publ. 2015;5(12):513–521.
40. Paul B, Ayo AS, Ayiga N. Rural-urban contraceptive use in Uganda: evidence from UDHS 2011. J Hum Ecol. 2015;52(3):168–182. doi:10.1080/09709274.2015.11906941
41. Makatjane T. Bioline international union for African Population Studies African Population Studies/Etude de la Population Contraceptive Prevalence in Lesotho: does the sex of the household head matter? Afr Popul Stud. 1997;12:1–11.
42. Hossain MB, Khan M, Ababneh F, Shaw J. Identifying factors influencing contraceptive use in Bangladesh: evidence from BDHS 2014 data. BMC Public Health. 2018;18(1):1–14. doi:10.1186/s12889-018-5098-1
43. Janevic T, Sarah PW, Leyla I, Elizabeth BH. Individual and community level socioeconomic inequalities in contraceptive use in 10 newly independent States: a multilevel cross-sectional analysis. Int J Equity Health. 2012;11(1). doi:10.1186/1475-9276-11-69
44. Shimeka Teferra A, Wondifraw AA, Teferra AS, Wondifraw AA. Determinants of long acting contraceptive use among reproductive age women in Ethiopia: evidence from EDHS 2011. Sci J Public Health. 2015;3(1):143. doi:10.11648/j.sjph.20150301.33
45. Habtamu A, Tesfa M, Kassahun M, Animen S. Determinants of long-acting contraceptive utilization among married women of reproductive age in Aneded district, Ethiopia: a case-control study. BMC Res Notes. 2019;12(1):433. doi:10.1186/s13104-019-4445-3
46. Bewket Zeleke L, Gella MM, Almaw Derseh H, Alemu AA, Abebe Kassahun E, Gelaw KA. Utilization of long-acting contraceptive methods and associated factors among female health care providers in East Gojjam Zone, Northwest Ethiopia, in 2018. Biomed Res Int. 2019;2019.
47. Ugaz JI, Chatterji M, Gribble JN, Banke K. Is household wealth associated with use of long-acting reversible and permanent methods of contraception? A multi-country analysis. Glob Health Sci Pract. 2016;4(1):43–540. doi:10.9745/GHSP-D-15-00234
48. Abebaw Gebeyehu AE, Mangham-Jefferies L, Mathewos B; The Federal Democratic Republic of Ethiopia Ministry of Health, et al. Determinants of long acting and permanent contraceptive methods utilization among married women in Hossana Town, Southern Ethiopia: a case - control study. Räisänen SH, editor. J Pregnancy Child Health. 2015;2(03):37–48.
 © 2020 The Author(s). This work is published and licensed by Dove Medical Press Limited. The
full terms of this license are available at https://www.dovepress.com/terms
and incorporate the Creative Commons Attribution
- Non Commercial (unported, 3.0) License.
By accessing the work you hereby accept the Terms. Non-commercial uses of the work are permitted
without any further permission from Dove Medical Press Limited, provided the work is properly
attributed. For permission for commercial use of this work, please see paragraphs 4.2 and 5 of our Terms.
© 2020 The Author(s). This work is published and licensed by Dove Medical Press Limited. The
full terms of this license are available at https://www.dovepress.com/terms
and incorporate the Creative Commons Attribution
- Non Commercial (unported, 3.0) License.
By accessing the work you hereby accept the Terms. Non-commercial uses of the work are permitted
without any further permission from Dove Medical Press Limited, provided the work is properly
attributed. For permission for commercial use of this work, please see paragraphs 4.2 and 5 of our Terms.