Back to Journals » Patient Preference and Adherence » Volume 14
Role of Treatment Adherence, Doctor–Patient Trust, and Communication in Predicting Treatment Effects Among Tuberculosis Patients: Difference Between Urban and Rural Areas
Authors Du L ![]() , Wu R
, Wu R ![]() , Chen X, Xu J, Ji H
, Chen X, Xu J, Ji H ![]() , Zhou L
, Zhou L
Received 18 August 2020
Accepted for publication 2 November 2020
Published 24 November 2020 Volume 2020:14 Pages 2327—2336
DOI https://doi.org/10.2147/PPA.S277650
Checked for plagiarism Yes
Review by Single anonymous peer review
Peer reviewer comments 2
Editor who approved publication: Dr Naifeng Liu
Liang Du, Ruiheng Wu, Xu Chen, Jia Xu, Haoqiang Ji, Ling Zhou
School of Public Health, Dalian Medical University, Dalian, Liaoning 116044, People’s Republic of China
Correspondence: Ling Zhou
School of Public Health, Dalian Medical University, 9 Western Section, Lvshun South Street, Lvshunkou District, Dalian 116044, People’s Republic of China
Tel +86-411-8611-0368
Email [email protected].
Purpose: China is the second highest tuberculosis (TB) burden in the world, and TB patients in the rural areas are about twice as many as urban patients. The purpose of present study was to explore the roles of medication adherence, doctor–patient trust and communication on treatment effects, and its inequality between urban and rural areas.
Methods: There were 564 eligible TB patients, from four tuberculosis hospitals in China, participating in this cross-sectional study. They filled out questionnaires regarding socio-demographic characteristics, medication adherence, treatment effect, doctor–patient trust, and communication. The structural equation model (SEM) was applied to explore the hypotheses in this study. All statistical analysis was done by SPSS 25.0 and Mplus 7.0 statistical software.
Results: This study included 267 (47.34%) urban and 297 (52.66%) rural eligible TB patients. The data fitted the research model well, and the urban TB patients reported better treatment effect than the rural ones (P=0.027). Overall, treatment adherence positively predicted treatment effect (Est.=0.353, P< 0.001); doctor–patient communication positively influenced treatment adherence (Est.=0.214, P=0.002); and treatment adherence positively mediated the role of communication on treatment effect (Est.=0.076), 95% CI (0.026, 0.152). While in the grouping model, the urban patients’ treatment effect was only influenced by adherence (Est.=0.286, P=0.003); for the rural patients, treatment adherence (Est.=0.464, P< 0.001) and doctor–patient trust (Est.=0.382, P=0.019) directly predicted treatment effects, and treatment adherence positively mediated the role of doctor–patient communication on treatment effect (Est.=0.175, P=0.006).
Conclusion: The treatment effect of TB patients, from urban and rural China, was influenced by a different mechanism, among which rural TB patients need not only improve the treatment adherence but also establish good doctor–patient trust and communication to improve treatment effects. These findings provided a theoretical guide on treatment and control for rural TB patients.
Keywords: compliance, doctor–patient relationship, treatment effects, TB, inequality, China
Introduction
Tuberculosis (TB) is a widespread infectious disease which is caused by Mycobacterium tuberculosis. According to the World Health Organization (WHO) estimating, about 10.0 million people (range, 9.0–11.1 million) diagnosed with new TB cases worldwide in 2018.1 TB was also one of the top 10 causes of death around the world and it resulted in an estimated 1.2 million (range, 1.1–1.3 million) deaths in 2018.1 China now suffers from the second-highest TB burden in the world, accounting for about 9% of cases, following India (27%).1 Additionally, the population in urban area are densely populated more than the rural group, but it is estimated that TB patients in the rural area are about twice as many as urban patients.2 Because of poor socio-economic factors and unsatisfactory medical conditions, rural TB patients often do not receive good treatment outcomes, that is, treatment success or cure.3,4 Although the prevalence rate of urban and rural TB patients varies widely, there is still a lack of research on the gap of treatment and control between urban and rural residence.
Every diagnosed patient has to take anti-TB drugs at least six months according to the treatment regimen recommended by WHO.1,5 However, there is a lack of assessment about the treatment effect in such a long-term medication process, which is associated with TB patients’ final treatment outcome.5 The treatment effect should be considered as a complex index that is affected by many factors.6 The curation of TB is mainly by taking anti-TB drugs on regimen and schedule, which means that medication adherence is directly associated with treatment outcome.7,8 Treatment adherence reflects the patients’ attitude and behavior towards the TB treatment, and higher adherence and regular medication can reduce the risk of treatment failure and relapse, which contributes to the good treatment effect of TB patients.6,9,10 Besides, doctors, playing the dominant role in treatment process, will also directly influence the treatment effect of TB patients.11 Patients’ trust in doctors is reflected in patients’ affirmation of doctors’ medical technology, prescription correctness and other treatment factors, and the more patients trust their doctors, the better their treatment effects will be.12 Additionally, previous studies showed that satisfactory doctor–patient communication during medical services, including an explanation of drug use and illness status, psychological counseling, and so on, was also one of means to improve the treatment effects of patients.13,14 To sum up, treatment adherence, doctor–patient trust, and communication may be directly associated with treatment effects.
Previous studies have shown that medication adherence of TB patients was not very ideal in China, while the treatment adherence of rural patients was generally low because of differences in economy, medical resources, TB control strategies.3,15 The determinants of treatment adherence are complex and the empirical relationship between medical staff and treatment adherence is still lacking.11,16 Doctor–patient trust is one of the important issues in the doctor–patient relationship.17 The higher the mutual trust, the more confident the patients will be about the treatment service offered by the doctors, and the more active he/she will be to participate in the treatment.18,19 Moreover, according to the medical agreement, TB patients have to go to the hospital every month for follow-up health examination and supplement drugs. If patients performed less trust in doctors, they may not take their medicine regularly, and even lose to follow-up or interrupt their treatment.20,21 In the treatment process, patients may have difficulty in adhering to treatment because of taking multiple treatment drugs and frequent occurrence of adverse reactions.5,7,22 At this point, it is necessary for doctors to communicate with patients to give reasonable explanations and provide solutions to these problems. Good doctor–patient communication can solve most problems in the treatment process, but deficient doctor–patient communication may provoke the occurrence of doctor–patient conflicts.23 Taken together, we considered that doctor–patient trust and communication could predict patient treatment adherence, and finally influence treatment effect.
In conclusion, we put forward the research model in this study (Figure 1), and we hypothesized that: (1) treatment adherence, doctor–patient trust, and communication directly predict treatment effect; (2) doctor–patient trust and communication directly predict treatment adherence; (3) treatment adherence mediated the role of doctor–patient trust or communication on treatment effect. Although the Chinese government has offered preferential treatment policies to TB patients, the burden of TB patients still remains severe, especially for the rural patients who are in lower economy, which would lead to poor TB treatment effect and hinder the end TB target.24–26 Therefore, in the above relationship, we assumed that there will be differences between urban and rural China.
 |
Figure 1 The research model based on the hypotheses. |
Methods
Study Design and Setting
This cross-sectional multi-center survey was done between June 20, 2019, and August 31, 2019. Four medical institutions in Dalian, northeast China were involved in this study. The four medical institutions, which served different types of patients, were chosen according to their institution level and location. The first was a tertiary hospital which serves patients across the whole city, especially critically ill and urban patients. The second was a county hospital and it serves both rural and urban TB patients. The other two medical institutions were tuberculosis dispensaries, which only serve local patients with milder disease.
Participants
Outpatients with pulmonary TB who had been on medication treatment for more than 2 months were eligible participants. We excluded TB patients aged <15 years and patients who were unable to complete the questionnaire due to mental or psychological illness. Prior to being interviewed by trained staff from the School of Public Health at Dalian Medical University, participants received verbal and written information about the purpose and instructions of the interview. All participants were told that their privacy would be protected and they were free to withdraw from the study at any time. The participants signed an informed consent form to participate in our study and for ones under the age of 18 years, we ask for permission of them and their parents (or legal guardian) before writing the informed consent.
Measurement
The questionnaire mainly consisted of participants’ socio-demographic characteristics, doctor–patient trust, doctor–patient communication, treatment adherence, and treatment effect. We collected the socio-demographic characteristics of the participants including gender, age, marriage status (married or unmarried/widowed), employment status, migration status, residence place (urban/rural), education level, their individual monthly income.
The self-report trust of the patient to doctor was measured by the sub-scale of Trust in Physician27 which consisted of 4 items: (1) you completely trust your doctor’s decisions about which treatment is the best for you; (2) your doctor only thinks about what is the best for you; (3) you have no worries about putting your life in your doctor’s hand; and (4) all in all, you have complete trust in your doctor. The 4-item scale could measure the patients’ global trust in doctors. Participants responded to the 4 items on a 5-point Likert-type scale (1=strongly disagree to 5= strongly agree). The scale reliability coefficient of Cronbach’s α was 0.85.
The communication between doctor and patients was measured by the 4-item scale, which was a component of the Consumer Assessment of Healthcare Providers and Systems (CAHPS) which involved doctor–patient communication, access to needed medical service, timely healthcare, and so on.28 Response options of each item ranged from 5=never to 1=always. Higher scores indicated high-level communication. The 4-item scale reliability coefficient of Cronbach’s α was 0.87.
Based on the literature review and expert consultation, we used two items to measure the participants’ treatment adherence. We asked them how often, during their treatment, they had the problems of medication behavior: 1) how often do you forget to take your medicine, and 2) how often do you stop taking medicine when you experience side effects or feel alleviated symptoms. Participants responded to these items on a 5-point Likert-type scale (1=always to 5=never). The 2-item scale reliability coefficient of Cronbach’s α was 0.88.
There was no validated TB-specific instrument that measures patients’ treatment effect,29 so based on the literature review and expert consultation, we compiled three items to measure the treatment effect of TB patients. The first item was that “What do you think of the severity of your illness now”, and the response option was from “very serious” to “not serious at all”, scored as 1–5, respectively. The second item asked the participants that “How do you feel about your health status and disease change after treatment” and the response option was from “more serious than before” to “almost cured”, scored as 1–5, respectively. The last item asked participants that “How do you feel about your overall health” and the response option was from “very bad” to “very good”, scored as 1–5, respectively. The 3-item scale reliability coefficient of Cronbach’s α was 0.68.
Statistical Analysis
A total of 593 TB patients containing the questionnaire data were collected, and we used EpiData software version 3.1 (The EpiData Association, Odense, Denmark) to set up a database to make the questionnaire records electronic. We deleted records containing >20% missing values, which led to 564 eligible participants in the final sample. We mainly used frequency and percentage to describe the study sample. Besides, the scores of the constructs exhibited normal distribution (Shapiro–Wilk normality test, P>0.05). We employed mean and standard deviation to describe the constructs in this study, and t-test of two independent-samples was used to test the differences between the rural and urban participants.
In consideration of mediating potential variable and complex relationships in the research model, we used structural equation model (SEM) to test research hypotheses. SEM can serve to find the potential but important associations that they produced a more complete picture of the potential effect mechanism, and it especially incorporates the measurement error in the research model.30 Additionally, the confirmatory factor analysis (CFA) was performed to examine the validity and reliability of scales and to combine with SEM to optimize the research model.30 The mediation models were done using the bootstrap method, which provided a nonparametric test that did not rely on assumptions of normal distribution.31 In this method, a significant indirect effect indicated by a 95% confidence interval (CI), which not including zero provided evidence for mediation.31 SPSS 25.0 statistical package (IBM Corporation, Armonk, State of New York, USA) was used to analyze data obtained from the survey preliminarily. According to the principle of SEM, our conceptual model was then tested using Mplus 7.0 statistical analysis software (Muthen & Muthen, Los Angeles, CA, USA). Two-side P<0.05 was considered as statistical significance.
Ethics Approval and Informed Consent
This study was conducted in accordance with the Declaration of Helsinki. The study protocol was reviewed and approved by the ethics committee of Dalian Medical University, Liaoning province, China (20,200,717–10). All participants signed an informed consent form to participate in our study, and parents or legal guardians provided informed consent for any patient under the age of 18.
Results
Socio-Demographic Characteristics of the Participants
Among the 564 participants, there were about twice as many male patients (66.31%) as female patients (33.69%). The mean age was 47.41 years and the median was 49 years. Most of the participants were married (71.10%), and only 93 (16.49%) were migrants. There were slightly more rural patients (52.66%) than urban patients (47.34%). Middle school education (34.22%) was the most common education level, and the percentages among the other education levels were almost the same as each other. The number of participants decreased with the increase of income monthly, and only 61 (10.82%) reported more than 5000 yuan per month (Table 1).
 |
Table 1 Demographic and Social Characteristics of the Sample |
Description of Study Constructs
In an overall view, the mean values of the constructs were not very high. Rural patients performed higher trust in their doctors than the urban ones (P=0.007). The urban patients showed higher doctor–patient communication scores than the rural ones (P=0.001). Besides, the urban patients reported better treatment effects than the rural patients (P=0.027). However, the treatment adherence exhibited no significance between urban and rural patients (Table 2).
 |
Table 2 Description of Constructs and Differences Between Urban and Rural Areas |
Validity and Reliability of the Measurement
All factor loadings of the items were >0.6, which exhibited that these items could measure the potential constructs well. The least value of the CR was 0.691, which implied that the constructs exhibited acceptable composite reliability. Besides, the values of 
 were more than the row or column Pearson correlation coefficient between constructs, which exhibited ideal discriminant validity. In brief, the research constructs exhibited good reliability and validity (Table 3).
were more than the row or column Pearson correlation coefficient between constructs, which exhibited ideal discriminant validity. In brief, the research constructs exhibited good reliability and validity (Table 3).
 |
Table 3 Results of the Reliability and Validity Test |
Testing the Goodness Fit of the Research Model
With the maximum likelihood method used, the research model exhibited ideal goodness fit comparing to the threshold values (Chi-square/DF<3; CFI>0.90; TLI>0.90; RMSEA<0.08; SRMR<0.08), which indicated that the data fit the two conceptual research model very well (Table 4).
 |
Table 4 Fitting Index of the Research Model |
Determinants and Mechanism of Treatment Effect
With no separation of the urban and rural patients, the SEM results showed that treatment adherence could positively and directly predict treatment effect (Est.=0.353, P<0.001). Besides, doctor–patient communication exhibited positively and directly impact on treatment adherence (Est.=0.214, P=0.002). Furthermore, treatment adherence positively mediated the role of doctor–patient communication and treatment effect (Est.=0.076), 95% CI (0.026, 0.152). However, the other relationships in the SEM exhibited no statistical significance (Table 5).
 |
Table 5 Determinants and Mechanism of Treatment Effect Among TB Patients in China |
Differences in Treatment Between Urban and Rural Patients
As the SEM results showed, treatment adherence significantly and positively predicted treatment effect for the urban patients (Est.=0.286, P=0.003), but other factors showed no statistical significance. For rural TB patients, doctor–patient trust (Est.=0.382, P=0.019) positively predicted patients’ treatment effect, which was significantly higher than urban patients (Est.=0.391, P=0.032); treatment adherence (Est.=0.464, P<0.001) positively predicted patients’ treatment effect; doctor–patient communication positively predicted treatment adherence (Est.=0.376, P<0.001), which was significantly higher than the urban patients (Est.=0.287, P=0.027); and, treatment adherence positively mediated the role of doctor–patient communication and treatment effect (Est.=0.175, P=0.006), which was also significantly higher than the urban patients (Est.=0.149, P=0.028). Though it showed no significance among urban or rural areas patients, the difference also exhibited in the effect of doctor–patient trust on treatment adherence, and the mediation of treatment adherence in doctor–patient trust and treatment effect (Table 6).
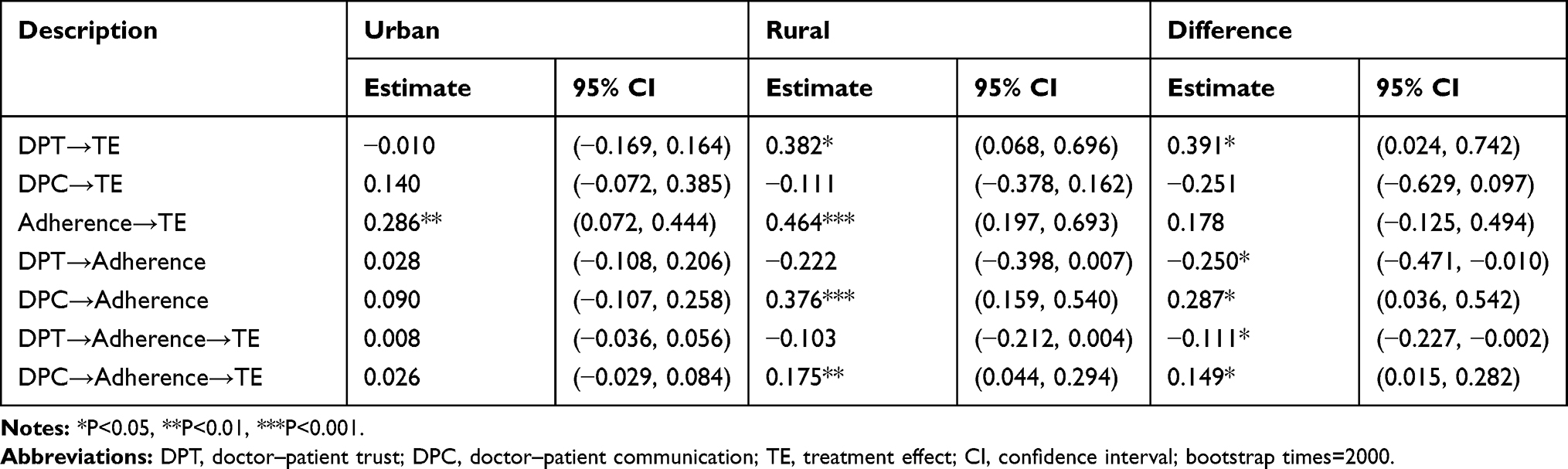 |
Table 6 Difference in Treatment Between Urban and Rural Patients |
Discussions
With a high prevalence of TB in China, researchers have carried out various studies on the treatment outcome of TB, while few studies have focused on the treatment effect in the medication process even though each TB patient has to take anti-TB medicine chronically. This was the first study on treatment effects among the TB patients in China. Additionally, this study innovatively explored the role of medication adherence, doctor–patient trust and communication on the treatment effect in medication process, and the difference between urban and rural TB patients. The results showed that the urban TB patients reported better treatment effects than the rural ones. Using the SEM method, we found that doctor–patient trust and communication, and treatment adherence significantly predicted treatment effect for TB patients, in direct and indirect paths, and these relationships exhibited significant inequity between urban and rural China.
Overall, the analysis of the whole sample showed that effective doctor–patient communication contributed to the improvement of treatment adherence. In doctor–patient communication, doctors expound knowledge about the prevention and treatment of TB to patients, and patients comprehend the importance of treating TB, which will help to improve their treatment adherence.14,32 Moreover, as the SEM results indicated, the improvement of treatment adherence generated a better treatment effect, and treatment adherence positively mediated the role of communication and treatment effect. This relationship, which has not been evidenced previously, provides a possible mechanism by which enhanced doctor–patient communication can not only prompt treatment adherence but also further improve treatment effects for TB patients. However, when we explored the treatment of urban and rural TB patients separately, we found that the treatment effects of the two had different mechanisms of association.
The findings exhibited that treatment adherence showed a significantly positive role in the treatment effect among both urban and rural patients. Complete adherence means that patients can overcome various obstacles in the treatment process and take their anti-TB drugs on time according to the treatment regimen.26,33 Taking drugs regularly is conducive to eliminate Mycobacterium tuberculosis in the body and mitigate the TB-related clinic symptoms, and the treatment effect is significantly improved.10,34 Hence, in practice, more attention should be paid to monitoring TB patients’ treatment adherence, and feasible strategies should be formulated to improve patients’ treatment adherence.35,36 The doctor–patient trust played a significantly positive role in the treatment effects for rural patients, but no significant effect was observed in urban patients. This may be the reason that the rural patients performed higher trust in doctors than the urban ones, and higher trust contributed to better treatment effects. Since improvement of the doctor–patient trust is conducive to improve the treatment effect for the rural TB patients, we should pay attention to building up doctor–patient trust in TB treatment. The rural doctors working in the Tuberculosis Dispensary and Control Unit often performed lower medical technology and skills in China,37,38 which would weaken doctor–patient trust. Therefore, it is imperative to implement strategies to enhance doctors’ professional skills and social reputation, and further encourage the rural doctor–patient trust in practice.
Moreover, in rural China, doctor–patient communication had a significant positive effect on treatment adherence, while no significance for the urban patients. This explained why rural patients’ treatment adherence was suboptimal and also provided a possibility to improve their treatment adherence. Of course, this relationship should not all impute to the rural patients, but to the health-care resources they live in.37,39 Previous studies have shown that the medical staff in rural medical institutions received less medical education and limited knowledge in medical service delivery,38 so doctors were not able to provide satisfactory health education and counseling services to patients,40 which could lead to patients’ low communication willingness, non-ideal enthusiasm and less initiative to participate in anti-TB treatment.19,41 Further SEM results revealed that the treatment adherence of rural patients played a mediating role in the doctor–patient communication predicting the treatment effect. This finding provided a reasonable explanation for why rural TB patients were in suboptimal treatment, but meanwhile, it implied a solution to improve their treatment effect. Therefore, we believe that restoring the service capacity of rural medical staff and the depth of doctor–patient communication can promote the medication adherence and treatment effects of patients, which may be a key issue in rural TB prevention and control.42,43
Nevertheless, several limitations need to be addressed in the future study. First, the sample in this study was limited to come from Dalian only. This limits our ability to generalize findings to other regional groups. Further study should be extend to more regions to test the adaptability of our research model. Second, the data were collected only through self-report measures, and it might affect the results of this study. It seems likely that patients with preferential treatment from the doctor may be more inclined to perform positive feedback, which may account for report bias. Future studies should combine participants’ self-reported measures, objective information (eg, medical records) and content analyses by interviewing their opinion and feedback from others. Finally, our findings were based on cross-sectional data, which limits our ability to draw practical causal relations. Although the tested model provides one possible combination of the relationships, its power of persuasion still seems inadequate. Therefore, longitudinal designs are needed to examine causal relationships between these variables.
Conclusions
This study explored the predicting role of treatment adherence, doctor–patient trust and communication in treatment effects, and the difference between urban and rural TB patients. The urban TB patients reported better treatment effects than the rural ones. With the SEM method used, we found that the urban patients’ treatment effect was only influenced by treatment adherence; for the rural patients, treatment adherence and doctor–patient trust directly and positively predicted treatment effects, and treatment adherence positively mediated the role of doctor–patient communication on treatment effect. The treatment effect of TB patients, from urban and rural China, was influenced by a different mechanism, among which rural TB patients required not only to improve treatment adherence but also establish good doctor–patient trust and communication. These research results provided theoretical guides on improving the treatment effect for rural patients, which was helpful to alleviate the TB burden in Chinese rural areas.
Abbreviations
TB, tuberculosis; SEM, structural equation model; WHO, World Health Organization; CFA, confirmatory factor analysis; F.L., factor loading; CR, composite reliability; AVE, average of variance extracted; DPT, doctor–patient trust; DPC, doctor–patient communication; TE, treatment effect; DF, degree of the freedom; CFI, comparative fit index; TLI, Tucker-Lewis index; RMSEA, root mean squared error of approximation; SRMR, standardized root mean square residual; CI, confidence interval; S.E., standard error; Est, estimate.
Acknowledgments
We thank all 15 interviewers, who came from the School of Public Health at Dalian Medical University, for their efforts in collecting the data. In addition, we are grateful to all the medical personnel from the four investigative districts who contributed to our study. Finally, we express gratitude to the TB patients who made our study possible.
Author Contributions
All authors made a significant contribution to the work reported, whether that is in the conception, study design, execution, acquisition of data, analysis and interpretation, or in all these areas; took part in drafting, revising or critically reviewing the article; gave final approval of the version to be published; have agreed on the journal to which the article has been submitted; and agree to be accountable for all aspects of the work.
Funding
This research received no external funding.
Disclosure
The authors report no conflicts of interest in this work.
References
1. World Health Organization. Global Tuberculosis Report 2019. WHO/CDS/TB/2019.15. Geneva, Switzerland: World Health Organization;2019.
2. Wang L, Zhang H, Ruan Y, et al. Tuberculosis prevalence in China, 1990–2010; a longitudinal analysis of national survey data. Lancet. 2014;383(9934):2057–2064. doi:10.1016/S0140-6736(13)62639-2
3. Xu CH, Jeyashree K, Shewade HD, et al. Inequity in catastrophic costs among tuberculosis-affected households in China. Infect Dis Poverty. 2019;8(1):46. doi:10.1186/s40249-019-0564-2
4. Wang Y, Li Y, Qin S, et al. The disequilibrium in the distribution of the primary health workforce among eight economic regions and between rural and urban areas in China. Int J Equity Health. 2020;19(1):28. doi:10.1186/s12939-020-1139-3
5. Zha BS, Nahid P. Treatment of drug-susceptible tuberculosis. Clin Chest Med. 2019;40(4):763–774. doi:10.1016/j.ccm.2019.07.006
6. Munro SA, Lewin SA, Smith HJ, Engel ME, Fretheim A, Volmink J. Patient adherence to tuberculosis treatment: a systematic review of qualitative research. PLoS Med. 2007;4(7):1230–1245. doi:10.1371/journal.pmed.0040238
7. Tweed CD, Dawson R, Burger DA, et al. Bedaquiline, moxifloxacin, pretomanid, and pyrazinamide during the first 8 weeks of treatment of patients with drug-susceptible or drug-resistant pulmonary tuberculosis: a multicentre, open-label, partially randomised, phase 2b trial. Lancet Respir Med. 2019;7(12):1048–1058. doi:10.1016/S2213-2600(19)30366-2
8. Keutzer L, Wicha SG, Simonsson US. Mobile health apps for improvement of tuberculosis treatment: descriptive review. JMIR Mhealth Uhealth. 2020;8(4):e17246. doi:10.2196/17246
9. Haynes RB, Ackloo E, Sahota N, McDonald HP, Yao X. Interventions for enhancing medication adherence. Cochrane Database Systematic Rev. 2008;(2):129.
10. Sotgiu G, Centis R, D’Ambrosio L, Migliori GB. Tuberculosis treatment and drug regimens. Cold Spring Harb Perspect Med. 2015;5(5):a017822. doi:10.1101/cshperspect.a017822
11. Zhang J, Yang Y, Qiao X, et al. Factors influencing medication nonadherence to pulmonary tuberculosis treatment in tibet, china: a qualitative study from the patient perspective. Patient Prefer Adherence. 2020;14:1149–1158. doi:10.2147/PPA.S252448
12. Petrocchi S, Iannello P, Lecciso F, Levante A, Antonietti A, Schulz PJ. Interpersonal trust in doctor-patient relation: evidence from dyadic analysis and association with quality of dyadic communication. Soc Sci Med. 2019;235:8. doi:10.1016/j.socscimed.2019.112391
13. Bredart A, Bouleuc C, Dolbeault S. Doctor-patient communication and satisfaction with care in oncology. Curr Opin Oncol. 2005;17(4):351–354. doi:10.1097/01.cco.0000167734.26454.30
14. Shan W, Wang Y, Luan J, Tang P. The Influence of physician information on patients’ choice of physician in mHealth services using China’s chunyu doctor app: eye-tracking and questionnaire study. JMIR Mhealth Uhealth. 2019;7(10):e15544. doi:10.2196/15544
15. Xu ML, Markstrom U, Lyu JC, Xu LZ. Detection of low adherence in rural tuberculosis patients in china: application of morisky medication adherence scale. Int J Environ Res Public Health. 2017;14(3):10.
16. Du L, Chen X, Zhu X, et al. Determinants of medication adherence for pulmonary tuberculosis patients during continuation phase in dalian, Northeast China. Patient Prefer Adherence. 2020;14:1119–1128. doi:10.2147/PPA.S243734
17. Kao AC, Green DC, Zaslavsky AM, Koplan JP, Cleary PD. The relationship between method of physician payment and patient trust. JAMA. 1998;280(19):1708–1714. doi:10.1001/jama.280.19.1708
18. Friedman DS, Hahn SR, Gelb L, et al. Doctor-patient communication, health-related beliefs, and adherence in glaucoma. Ophthalmology. 2008;115(8):1320–1327. doi:10.1016/j.ophtha.2007.11.023
19. Ren J, Li Q, Zhang T, et al. Perceptions of engagement in health care among patients with tuberculosis: a qualitative study. Patient Prefer Adherence. 2019;13:107–117. doi:10.2147/PPA.S191800
20. Tupasi T, Garfin A, Mangan JM, et al. Multidrug-resistant tuberculosis patients’ views of interventions to reduce treatment loss to follow-up. Int J Tuberculosis Lung Disease. 2017;21(1):23–31. doi:10.5588/ijtld.16.0433
21. Adams LV, Basu D, Grande SW, et al. Barriers to tuberculosis care delivery among miners and their families in South Africa: an ethnographic study. Int J Tuberculosis Lung Disease. 2017;21(5):571–578. doi:10.5588/ijtld.16.0669
22. Ayele AA, Asrade Atnafie S, Balcha DD, et al. Self-reported adherence and associated factors to isoniazid preventive therapy for latent tuberculosis among people living with HIV/AIDS at health centers in Gondar town, North West Ethiopia. Patient Prefer Adherence. 2017;11:743–749. doi:10.2147/PPA.S131314
23. Steihaug S, Gulbrandsen P, Werner A. Recognition can leave room for disagreement in the doctor-patient consultation. Patient Educ Couns. 2012;86(3):316–321. doi:10.1016/j.pec.2011.06.011
24. Long Q, Qu Y, Lucas H. Drug-resistant tuberculosis control in China: progress and challenges. Infect Dis Poverty. 2016;5:9.
25. Ai X, Men K, Guo L, et al. Factors associated with low cure rate of tuberculosis in remote poor areas of Shaanxi Province, China: a case control study. BMC Public Health. 2010;10:112. doi:10.1186/1471-2458-10-112
26. Chen S, Zhang H, Pan Y, et al. Are free anti-tuberculosis drugs enough? An empirical study from three cities in China. Infect Dis Poverty. 2015;4:47. doi:10.1186/s40249-015-0080-y
27. Hall MA, Zheng B, Dugan E, et al. Measuring patients’ trust in their primary care providers. Medical Care Research Review. 2002;59(3):293–318. doi:10.1177/1077558702059003004
28. Hays RD, Chawla N, Kent EE, Arora NK. Measurement equivalence of the Consumer Assessment of Healthcare Providers and Systems (CAHPS((R))) Medicare survey items between Whites and Asians. Quality Life Res. 2017;26(2):311–318. doi:10.1007/s11136-016-1383-6
29. Brown J, Capocci S, Smith C, Morris S, Abubakar I, Lipman M. Health status and quality of life in tuberculosis. Int J Infect Dis. 2015;32:68–75. doi:10.1016/j.ijid.2014.12.045
30. Hayes AF. Introduction to Mediation, Moderation, and Conditional Process Analysis: A Regression-Based Approach. The Guilford Press; 2018.
31. Hayes AF, Baron B, Kenny. Statistical mediation analysis in the new millennium. Commun Monogr. 2009;4:408–420. doi:10.1080/03637750903310360
32. Wu S, Roychowdhury I, Khan M. Evaluating the impact of healthcare provider training to improve tuberculosis management: a systematic review of methods and outcome indicators used. Int J Infect Dis. 2017;56:105–110. doi:10.1016/j.ijid.2016.11.421
33. Valencia S, León M, Losada I, Sequera VG, Fernández QM, García-Basteiro AL. How do we measure adherence to anti-tuberculosis treatment? Expert Rev Anti Infect Ther. 2017;15(2):157–165. doi:10.1080/14787210.2017.1264270
34. Sariem CN, Odumosu P, Dapar MP, Musa J, Ibrahim L, Aguiyi J. Tuberculosis treatment outcomes: a fifteen-year retrospective study in Jos-North and Mangu, Plateau State, North - Central Nigeria. BMC Public Health. 2020;20(1):1224. doi:10.1186/s12889-020-09289-x
35. Alipanah N, Jarlsberg L, Miller C, et al. Adherence interventions and outcomes of tuberculosis treatment: A systematic review and meta-analysis of trials and observational studies. PLoS Med. 2018;15(7):e1002595.
36. Lutge EE, Wiysonge CS, Knight SE, Sinclair D, Volmink J. Incentives and enablers to improve adherence in tuberculosis. Cochrane Database Syst Rev. 2015;2015(9):Cd007952.
37. Wang X, Wu Z. Factors associated with adherence to antiretroviral therapy among HIV/AIDS patients in rural China. Aids. 2007;21(Suppl 8):S149–155. doi:10.1097/01.aids.0000304711.87164.99
38. Li Y, Ehiri J, Tang S, et al. Factors associated with patient, and diagnostic delays in Chinese TB patients: a systematic review and meta-analysis. BMC Med. 2013;11:156. doi:10.1186/1741-7015-11-156
39. Yuan L, Zhang H, Zhou C, Jiang W, Zhao Q, Biao X. Better care provided to patients with tuberculosis at county designated TB hospitals (CTD) compared to non-CTDs in rural China. BMC Infect Dis. 2017;17(1):71. doi:10.1186/s12879-016-2108-8
40. Wang Q, Kong YJ, Sun JY, Zhang Y, Yuan LL, Wang J. What are the challenges faced by village doctors in provision of basic public health services in shandong, china? A qualitative study. Int J Environ Res Public Health. 2019;16(14):18.
41. Roettl J, Bidmon S, Terlutter R. What predicts patients’ willingness to undergo online treatment and pay for online treatment? Results from a web-based survey to investigate the changing patient-physician relationship. J Med Internet Res. 2016;18(2):15. doi:10.2196/jmir.5244
42. Maatouk-Burmann B, Ringel N, Spang J, et al. Improving patient-centered communication: results of a randomized controlled trial. Patient Educ Couns. 2016;99(1):117–124. doi:10.1016/j.pec.2015.08.012
43. Dang BN, Westbrook RA, Njue SM, Giordano TP. Building trust and rapport early in the new doctor-patient relationship: a longitudinal qualitative study. BMC Med Educ. 2017;17:10. doi:10.1186/s12909-017-0868-5
 © 2020 The Author(s). This work is published and licensed by Dove Medical Press Limited. The
full terms of this license are available at https://www.dovepress.com/terms
and incorporate the Creative Commons Attribution
- Non Commercial (unported, 3.0) License.
By accessing the work you hereby accept the Terms. Non-commercial uses of the work are permitted
without any further permission from Dove Medical Press Limited, provided the work is properly
attributed. For permission for commercial use of this work, please see paragraphs 4.2 and 5 of our Terms.
© 2020 The Author(s). This work is published and licensed by Dove Medical Press Limited. The
full terms of this license are available at https://www.dovepress.com/terms
and incorporate the Creative Commons Attribution
- Non Commercial (unported, 3.0) License.
By accessing the work you hereby accept the Terms. Non-commercial uses of the work are permitted
without any further permission from Dove Medical Press Limited, provided the work is properly
attributed. For permission for commercial use of this work, please see paragraphs 4.2 and 5 of our Terms.