Back to Journals » Drug, Healthcare and Patient Safety » Volume 17
Risk of Antipsychotic Initiation Among Older Dementia Patients Initiating Cholinesterase Inhibitors
Authors Chikermane SG, Li J ![]() , Aparasu RR
, Aparasu RR ![]()
Received 20 November 2024
Accepted for publication 21 February 2025
Published 20 March 2025 Volume 2025:17 Pages 75—85
DOI https://doi.org/10.2147/DHPS.S506523
Checked for plagiarism Yes
Review by Single anonymous peer review
Peer reviewer comments 2
Editor who approved publication: Dr Hemalkumar B Mehta
Soumya G Chikermane, Jieni Li, Rajender R Aparasu
University of Houston, College of Pharmacy, Department of Pharmaceutical Health Outcomes and Policy, Houston, TX, USA
Correspondence: Rajender R Aparasu, Department of Pharmaceutical Health Outcomes and Policy College of Pharmacy, University of Houston, 4349 Martin Luther King Boulevard, Houston, 77204-5047, Texas, Tel +1 (832) 842-8374, Email [email protected]
Background: Cholinesterase inhibitors (ChEIs) are recognized as first-line therapies for patients with mild-to-moderate dementia. However, there is limited comparative evidence regarding antipsychotic initiation risk among individual ChEIs to manage behavioral symptoms of dementia.
Objective: This study aims to evaluate and compare the risk of antipsychotic initiation among dementia patients prescribed individual ChEIs.
Methods: This is a retrospective cohort study using the 2009– 2018 TriNetX electronic medical records data. Dementia patients aged over 60 years who were incident users of rivastigmine, donepezil, or galantamine with a 12-month washout period were included. Patients with a history of antipsychotic use during baseline and 30 days post-initiation of ChEIs were excluded. Patients were followed up to 12 months to identify the antipsychotic use. A generalized boosted model-based inverse probability treatment weights-adjusted Cox Proportional Hazard (CPH) model was applied to compare the risk of antipsychotic initiation across the different ChEIs.
Results: Among the 7,878 eligible dementia patients initiating ChEIs, 89.40% (n=7,043) were incident donepezil users, followed by 8.13% of (n=641) rivastigmine users, and 2.46% (n=194) galantamine users. During the 12-month follow-up, 807 patients (10.24%) initiated antipsychotics. The CPH model showed that rivastigmine users were at an increased risk of antipsychotic use compared to donepezil users (adjusted hazard ratio=1.45, 95% confidence interval: 1.11– 1.88). No significant difference was observed in the risk of antipsychotic initiation between galantamine and donepezil users.
Conclusion: This study found that rivastigmine users were more likely to initiate antipsychotics compared to donepezil users, while no significant difference between galantamine and donepezil users was observed. These findings emphasize the importance of careful medication monitoring and management to prevent prescribing cascades and reduce related adverse effects in dementia patients.
Keywords: dementia, cholinesterase inhibitor, antipsychotics, real-world evidence
Introduction
Dementia is a chronic progressive disease that represents a spectrum of persistent neurological disorders characterized by gradual impairment across multiple cognitive domains.1,2 Dementia often results in memory loss, behavioral disturbances, and decreased capacity for independent daily functioning.3 In the United States, over 6.9 million individuals aged 65 and older are estimated to live with dementia, and this number is projected to escalate rapidly.4 The economic impact is substantial, and direct medical costs associated with dementia are expected to increase from $290 billion in 2019 to approximately $1.1 trillion by 2050, largely driven by hospitalizations and prescription medication expenses.5 The societal burden of dementia is further magnified by increased informal caregiving demands and substantial out-of-pocket payments for long-term care services.6,7
Cholinesterase inhibitors (ChEIs), including donepezil, galantamine, and rivastigmine, are recommended as first-line therapies for patients with mild-to-moderate dementia.8–10 Since dementia is currently incurable, the primary goal of these medications is to slow down the process of cognitive decline. However, behavioral and psychological symptoms of dementia (BPSD) often manifest as agitation, aggression, and psychosis and affect over 90% of dementia patients.11–13 Without effective management, BPSD can accelerate the functional decline, substantially increase the caregiver burden, diminish the quality of life, that often result in the need for institutional care.14,15 The effect of individual ChEIs on BPSD is highly varied due to their underlying mechanism of action, and therefore, antipsychotics are commonly prescribed for dementia patients to address BPSD, with utilization rates ranging from 20% to 50%.16,17 However, antipsychotic use is associated with an increased risk of cerebrovascular events, extrapyramidal symptoms, accelerated cognitive decline, and mortality.18,19
Evidence consistently demonstrates that patients receiving ChEIs have a higher likelihood of initiating antipsychotic therapy to manage BPSD.16,20,21 While ChEIs have similar mechanisms of action and demonstrate comparable efficacy, they differ in their specificity for cholinesterase enzymes.22,23 Consequently, this variation results in differential effects on cognitive and behavioral symptoms among dementia patients.24,25 Only one study evaluated the differential risk of antipsychotic initiation among Medicare beneficiaries 65 years or older during 2013–2015 and found that although there was no difference in antipsychotic initiation for galantamine and donepezil, rivastigmine was associated with an increased risk of antipsychotic initiation.17 Given the limited comparative evidence regarding antipsychotic initiation risk among individual ChEIs, this study aims to evaluate and compare the risk of antipsychotic medication initiation among older adults with dementia who initiated donepezil, rivastigmine, or galantamine.
Methods
Data Source
This retrospective observational cohort study used the TriNetX® electronic medical record (EMR) data of patients diagnosed with dementia between January 2009 and December 2018. The TriNetX is a federated global health research network comprising electronic medical records for over 90 million patients in the US from 67 healthcare organizations.26 The TriNetX EMR data includes longitudinally linked de-identified data that captures patients’ demographic characteristics, inpatient and outpatient encounters, and prescription records. The EMR Data was obtained under a data use agreement with Trinetx. This study was exempt from review by the Institutional Review Board at the University of Houston.
Study Population and Operational Definitions
Patients with dementia who were newly prescribed ChEI, including donepezil, galantamine, and rivastigmine, between January 1, 2009, and December 31, 2017, were included in this study. The diagnosis of dementia was identified using the International Classification of Diseases, Ninth/Tenth Revision, Clinical Modification codes: 331.0, 290, 294, 797, G30.9, F03.90, F05, F015.1, F04, F02.80, F02.81, F03.90, F03.91, F06.0, F06.8, and R418.1.27 Patients with Parkinson’s disease, Lewy body dementia, schizophrenia, bipolar disorders, or using anti-parkinsonian medication at any time during the study period were excluded.28
The earliest ChEI prescription date was assigned as the index date during the identification period. Incident ChEI users were selected as patients with no ChEIs during the one-year washout period to mitigate the prevalent user bias. Furthermore, the following inclusion criteria were considered when selecting patients: (i) with ≥1 dementia diagnosis during the 6 months before or after the index date, and (ii) ≥ 60 years old at the index date. Additionally, the following exclusion criteria were applied: (i) patients prescribed more than one individual ChEI at the index date (ie, patients prescribed with donepezil and rivastigmine at the index date) concomitantly, (ii) patients with ≥1 memantine prescription during the baseline period, (iii) patients with ≥1 antipsychotic during the baseline period and within 30 days after the index date, and (iv) patients without any outpatient visits and prescription record at baseline.27 The schematic representation of the study design is illustrated in Figure 1.
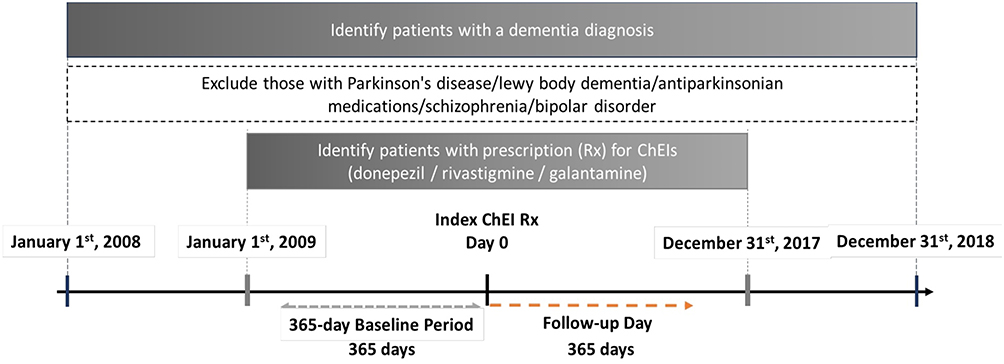 |
Figure 1 Study Design. Abbreviations: ChEI: Cholinesterase Inhibitors. |
Exposures and Outcome
Based on their index prescription, patients were categorized as incident users of donepezil, rivastigmine, or galantamine. Prescriptions of ChEIs were identified using RxNorm codes produced by the National Library of Medicine from prescription orders.
The outcome of this study was defined as the earliest prescription of antipsychotics and was identified starting on day 31 after the index date till day 365 after the index date. Antipsychotics were identified by RxNorm codes for both atypical and typical antipsychotics.17 Atypical antipsychotics included olanzapine, quetiapine, clozapine, risperidone, aripiprazole, ziprasidone, asenapine, paliperidone, iloperidone, lurasidone, and brexpiprazole. Typical antipsychotics included perphenazine, fluphenazine, thioridazine, thiothixene, perphenazine-amitriptyline, trifluoperazine, chlorpromazine, loxapine, and pimozide. Patients were followed until the earliest date of antipsychotics prescription, prescribed memantine, and switched between ChEIs (ie, from donepezil to rivastigmine on new ChEIs, death, or end of follow-up (day 365 after the index date).17
Conceptual Framework for Covariates
The Andersen Behavioral Model framework was used to conceptualize covariates in this study.29 This framework includes predisposing, enabling, and need factors. Predisposing factors like age at index date, gender, race, and ethnicity were included because these factors explain an individual’s predisposition to use medications. Enabling factors explain an individual’s ability to access healthcare; however, this study did not include enabling factors due to data limitations. Proxy measures were included at baseline to ensure the patient’s outpatient visits and medication prescriptions were recorded in the data. In addition, need factors were included as these indicate an individual’s perceived health status. Need factors like sleep disorders, osteoporosis, osteoarthritis, falls, frailty syndrome, Elixhauser comorbidities, and comedications were included.30,31 Frailty syndrome included fractures, pressure ulcers and weight loss, mobility problems, incontinence, dependence and care, and anxiety and depression.32 In addition to comorbidities, comedications like lipid modifying agents, medications for obstructive airway disease, anti-diabetic medications, sedative/ hypnotics, anxiolytics, diuretics, antihypertensives, vasodilators, antidepressants, antiarrhythmic medications, and anticonvulsants were identified and captured during the baseline period.17,27
Statistical Analyses
Propensity score (PS) methods are frequently employed in observational studies to mitigate measured confounding and estimate treatment effects with reduced observable bias.33 When dealing with a dependent variable that includes more than two treatment groups, the Generalized Boosted Model (GBM) is preferred over traditional logistic regression for calculating PS.34 The GBM (using the TWANG macro program in SAS) leverages a machine learning algorithm through an iterative process of building a series of regression trees. This process captures the complex and nonlinear relationships between treatment groups and covariates without overfitting the data.34,35 Research has indicated that GBM generates more stable weights and more effectively optimizes the balance between treatment groups compared to other PS approaches.34,36 Among various PS methods, inverse probability treatment weighting (IPTW) is recognized for providing marginal treatment effect estimates that exhibit lower bias and greater generalizability to the entire treatment population, in contrast to other approaches.37,38 This characteristic makes IPTW particularly valuable for analyzing observational study data, ensuring that the findings are more representative of the broader patient group under investigation. The cutoff for standardized differences was established at 0.2 to ensure the equivalence of covariates across the different ChEI cohorts.38
Descriptive statistics were performed to assess differences in baseline characteristics between the donepezil, rivastigmine, and galantamine cohorts. Mean and standard deviation (SD) were calculated for continuous variables, and frequency and proportion were calculated for binary or categorical variables. T-tests and chi-square tests were performed to assess the significance of differences in baseline characteristics between the cohorts. Kaplan-Meier survival curves were plotted to evaluate the crude relationship between the use of three ChEIs and the time to antipsychotic initiation. Further, the Schoenfeld test was performed to assess if the proportional hazards assumption was satisfied. A Cox proportional hazard (CPH) regression model adjusted for IPTW was used to examine the time to antipsychotic prescription between individual cohorts. Donepezil was used as the reference category as it is the most commonly used ChEI.
In the sensitivity analysis, the GBM-calculated PS was included as a covariate in the CPH model to examine the robustness of findings. Furthermore, the E-value was the measure of the minimum strength of association that an unmeasured confounder would require with both the treatment groups (eg, ChEI cohorts) and the outcome (eg, risk of antipsychotic use) to nullify the observed association. A higher E-value indicates that considerable unmeasured confounding would be necessary to weaken the observed effect, suggesting that the findings are robust and more reliable, even in the presence of potential unmeasured confounders.39 All statistical analyses were conducted at a priori 5% alpha level and were performed using SAS version 9.4 (SAS Institute, Inc., Cary, NC, USA).
Results
Cohort Characteristics
The study cohort included 47,996 dementia patients. After applying inclusion and exclusion criteria, there were 7,878 patients in the final cohort, of which 89.40% (n=7,043) were incident donepezil users, followed by 8.13% of (n=641) incident rivastigmine users, and 2.46% (n=194) incident galantamine users. Table 1 shows the detailed attrition table for the study flow. Most of the patients were aged greater than 80 years old (45.68%), males (64.78%), Whites (80.58%), and non-Hispanic (77.99%, Table 2). The average age of rivastigmine users was 78.23 years (SD: 5.83), 77.86 (SD: 6.20) years for donepezil users, and 76.75 (SD: 6.08) years for galantamine users. Table 2 shows significant differences in the distribution of various factors between ChEI cohorts. These factors include predisposing characteristics (such as age and ethnicity) and need-related factors (such as Elixhauser comorbidities, frailty syndrome, and comedications).
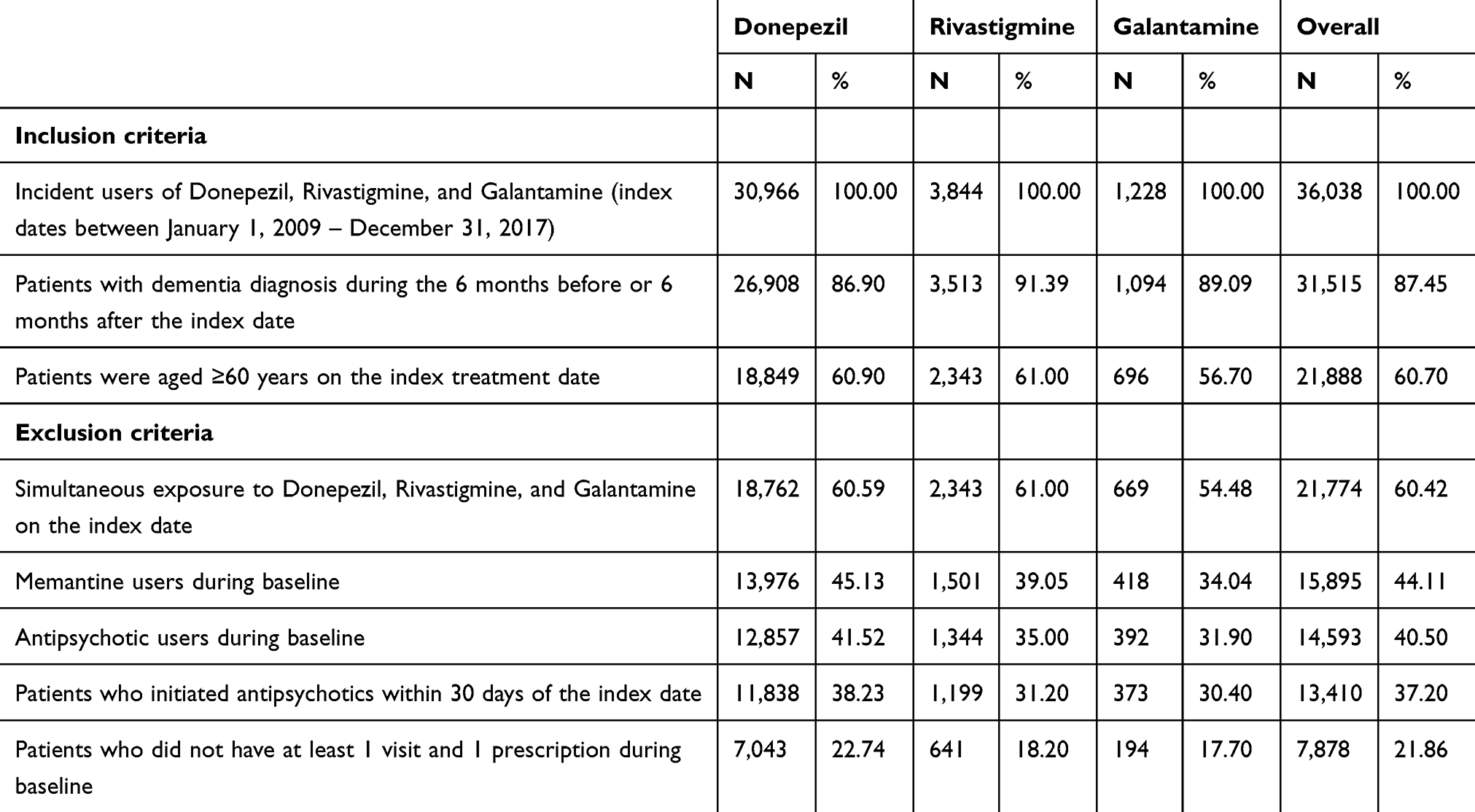 |
Table 1 Attrition Flow Chart of the Study Cohort |
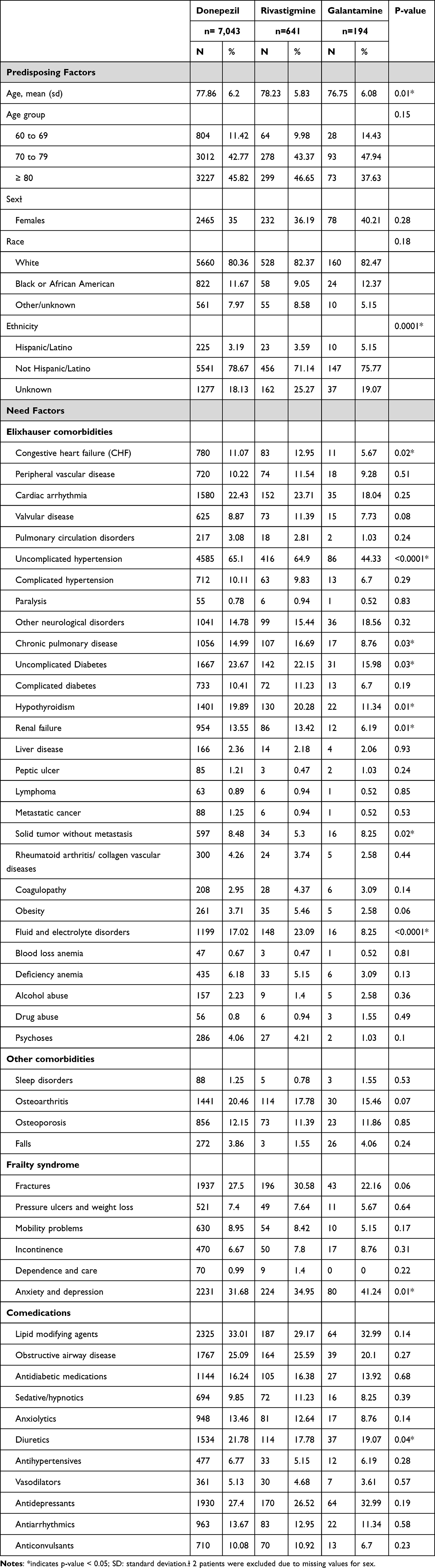 |
Table 2 Characteristics of Patients With Dementia Initiated With Cholinesterase Inhibitors in 2009–2017 TriNetx Data |
Risk of Antipsychotic Initiation Between ChEI
In the study cohort, 10.24% (n=807) initiated antipsychotics during the 12-month follow-up period, and the median time to antipsychotic initiation was 164 days. The mean time to antipsychotic initiation in donepezil users was 178 days (SD: 99.70), 175 days (SD: 96.28) in the rivastigmine users, and 162 days (SD: 94.86) in the galantamine users. Of the donepezil users who initiated antipsychotics during the study period (n=690), 61% (n=426) initiated atypical antipsychotics. Of the galantamine users who initiated antipsychotics during the study period (n=23), 86.96% (n=20) of them initiated atypical antipsychotics. Similarly, of the rivastigmine users who initiated antipsychotics during the study period (n=94), 75.53% (n=71) initiated atypical antipsychotics.
Findings from the Log rank test and Schoenfeld test both illustrated that the proportional hazards assumption was satisfied in this study. (Supplementary Figure 1) The IPTW-adjusted CPH found that rivastigmine users were at an increased risk of antipsychotic use (adjusted hazard ratio [aHR]=1.45, 95% confidence interval [CI]: 1.11–1.88, p<0.01, Table 3). Meanwhile, there was no difference in the risk of antipsychotic initiation between galantamine and donepezil users. Similar findings were obtained in the sensitivity analysis involving the GBM-calculated PS approach. In this study, the estimated E-value for the observed associations was 2.26. This means any unmeasured confounders would have to be associated with a 2.26-fold risk of antipsychotic initiation and use of ChEIs to nullify the observed findings.
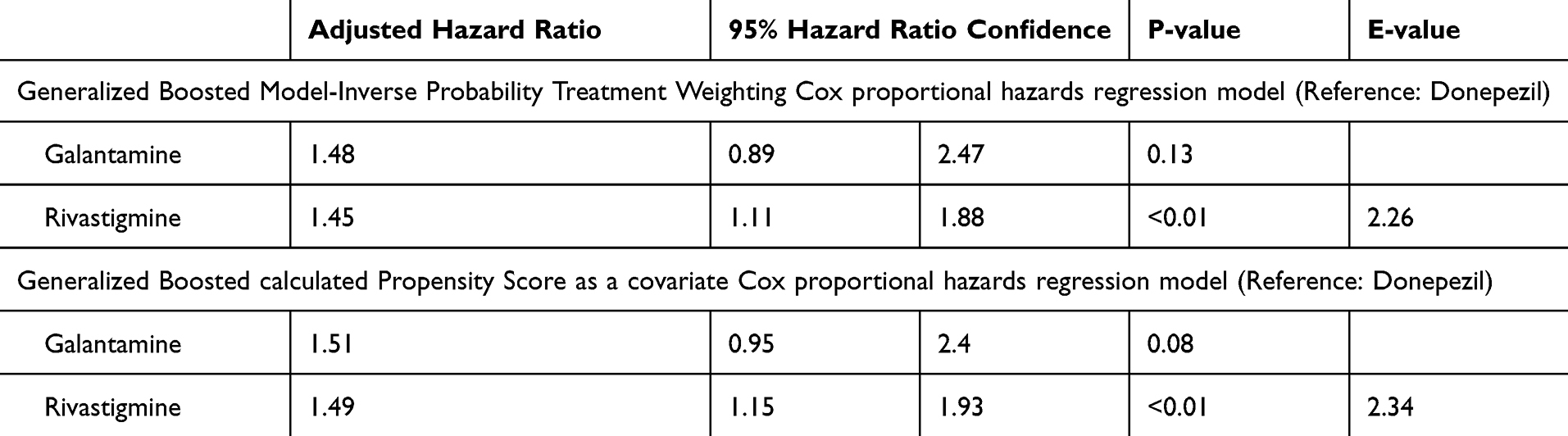 |
Table 3 Risk of Initiation of Antipsychotics for Dementia Patients Using Cholinesterase Inhibitors: Findings From Inverse Probability Treatment Weighting Based Cox Proportional Hazards Regression Model |
Discussion
Using ten years of EMR data, this study evaluated the risk of antipsychotic initiation associated with individual ChEIs among dementia patients. Notably, approximately 10% of dementia patients initiated with ChEI prescription also initiated antipsychotics within a 12-month follow-up period, which was similar to previous studies.17,23 Current therapeutic approaches for dementia predominantly focus on symptomatic management, utilizing strategies that inhibit the acetylcholinesterase enzyme to enhance both the concentration and duration of action of acetylcholine.40 However, there is very limited comparative evidence regarding antipsychotic initiation risk among individual ChEIs to manage BPSD.
The key finding of this study is that the risk of initiating antipsychotic medication among dementia patients varied by individual ChEI. Rivastigmine users were associated with a 45% higher risk of initiating antipsychotics compared to donepezil users, while no significant difference was observed in the risk of antipsychotic initiation between galantamine and donepezil users. Findings were aligned with a previous study using Medicare data, which reported an increased risk of antipsychotic initiation among rivastigmine users compared to those treated with donepezil (aHR 1.32; 95% CI 1.20–1.46) among community-dwelling older adults.17 However, Scharre et al found that rivastigmine users were associated with a reduced risk of antipsychotic use compared with donepezil using commercial insurance claims and Medicare Supplemental claims data.23 The discrepancies in findings may be attributed to the different formulations of rivastigmine used in the studies, as the transdermal patch, which was prevalent in this study cohort, received approval in 2007, after the study period of Scharre et al’s work. Rivastigmine in patches has been shown to offer more compliance and potentially decrease the risk of side effects compared to oral formulations, which might explain the variation in risk profiles observed across studies.24,41
While all ChEIs share a common mechanism of action through the inhibition of acetylcholinesterase, the primary enzyme responsible for the degradation of acetylcholine (ACh), distinctions exist among the individual drugs within this class, particularly regarding their specificity for the cholinesterase enzymes they inhibit.42 Donepezil is piperidine-based selective for acetylcholinesterase.22 Differently, rivastigmine acts as a dual inhibitor, targeting both acetylcholinesterase and butyrylcholinesterase, while galantamine not only inhibits acetylcholinesterase but also modulates nicotinic cholinergic receptors, enhancing the release of ACh.43–46 Despite comparable effectiveness profiles for cognitive function, rivastigmine was found to be associated with an increased risk of adverse events, including hospitalization and death, compared to donepezil, which needs to be carefully considered and monitored when selecting the ChEI for dementia patients.27,47
Overall, the findings of this study have significant implications regarding the differential effects of individual ChEIs and the need for antipsychotic treatment for managing BPSD. Donepezil and galantamine seem comparable concerning antipsychotic use; however, rivastigmine is associated with a higher risk of antipsychotic use. The increased likelihood of prescribing antipsychotics among dementia patients raises important clinical concerns related to polypharmacy and associated drug-related morbidity. Understanding the risk of BPSD and antipsychotic use will help clinicians make more informed decision-making regarding the use of individual ChEIs. Additionally, the results highlight the need for careful monitoring of dementia patients for BPSD to optimize antipsychotic use and enhance the overall quality of care for dementia patients.
Strengths and Limitations
This study offers important real-world evidence that examines and compares the risk of antipsychotic use among individual ChEIs. Leveraging a substantial cohort of ten years of EMR, the research is generalizable to dementia patient populations, providing a broadened perspective on the real-world implications of safety evaluation of dementia treatments. To address potential selection bias among treatment cohorts, this study applied both IPTW and PS techniques, which balanced patients’ demographic factors and various clinically relevant factors. Meanwhile, the robustness of the findings is further examined through E-value calculations, which assess the impact of unmeasured confounders, thereby reinforcing the robustness of the conclusions drawn from the observed associations.
However, when interpreting the findings, several limitations must be carefully considered. Firstly, because TriNetX EMR data is reported by various academic health centers (including specialty hospitals, integrated delivery networks, and large specialty physician practices), the results need to be interpreted with care and generalized within the bounds of the study population. Secondly, the TriNetX EMR data brings several inherent limitations. Although this study considered an incident patient cohort, there was a lack of information about the duration of dementia and severity of dementia when ChEIs were initiated. The baseline factors considered in calculating the IPTW were limited to those available in the TriNetX. Lastly, although the study included relevant exclusion/inclusion criteria, the specific indication for antipsychotic use was not evaluated, which might warrant future research.
Conclusions
This ten-year retrospective real-world study showed that 10% of dementia patients who initiated ChEI would use antipsychotics during the 12-month follow-up period. Furthermore, patients who initiated rivastigmine are at a 45% higher risk of antipsychotic initiation compared to donepezil users. Conversely, there was no significant difference in the risk of antipsychotic initiation between galantamine users and donepezil users. These findings highlight the importance of managing dementia symptoms using ChEI, especially BPSD and optimizing antipsychotic use and associated consequences in dementia patients. More research is needed to understand better the role of ChEI on variation in antipsychotic initiation across ChEI use in older adults to improve dementia care.
Ethics Approval
The study was approved by the University of Houston institutional review board with a waiver of informed consent.
Funding
The authors declare that no funds, grants, or other support were received for the research described in this manuscript.
Disclosure
Dr. Aparasu has received research funding from Astellas Inc., Incyte Corp., Gilead, and Novartis Inc. for projects unrelated to the current work. The other authors declare no conflicts of interest for this article.
References
1. Atri A. The alzheimer’s disease clinical spectrum: diagnosis and management. Med Clin North Am. 2019;103(2):263–293. doi:10.1016/j.mcna.2018.10.009
2. Duong S, Patel T, Chang F. Dementia: what pharmacists need to know. Can Pharm J. 2017;150(2):118–129. doi:10.1177/1715163517690745
3. Cipriani G, Danti S, Picchi L, Nuti A, Fiorino MD. Daily functioning and dementia. Dement Neuropsychol. 2020;14(2):93–102. doi:10.1590/1980-57642020dn14-020001
4. Alzheimer’s Association. 2024 alzheimer’s disease facts and figures. Alzheimers Dement. 2024;20(5):3708–3821. doi:10.1002/alz.13809
5. Stefanacci RG. The costs of Alzheimer’s disease and the value of effective therapies. Am J Manag Care. 2011;17(Suppl 13):S356–62.
6. Jutkowitz E, Kane RL, Gaugler JE, MacLehose RF, Dowd B, Kuntz KM. Societal and family lifetime cost of dementia: implications for policy. J Am Geriatr Soc. 2017;65(10):2169–2175. doi:10.1111/jgs.15043
7. Kelley AS, McGarry K, Bollens-Lund E, et al. Residential setting and the cumulative financial burden of dementia in the 7 years before death. J Am Geriatr Soc. 2020;68(6):1319–1324. doi:10.1111/jgs.16414
8. Rabins PV, Blacker D, Rovner BW, et al. American Psychiatric Association practice guideline for the treatment of patients with Alzheimer’s disease and other dementias. Am J Psychiatry. 2007;164(12 Suppl):5–56.
9. Farlow MR, Cummings JL. Effective pharmacologic management of Alzheimer’s disease. Am J Med. 2007;120(5):388–397. doi:10.1016/j.amjmed.2006.08.036
10. Small G, Bullock R. Defining optimal treatment with cholinesterase inhibitors in alzheimer’s disease. Alzheimers Dement. 2011;7(2):177–184. doi:10.1016/j.jalz.2010.03.016
11. Benoit M, Arbus C, Blanchard F, et al. Professional consensus on the treatment of agitation, aggressive behaviour, oppositional behaviour and psychotic disturbances in dementia. J Nutr Health Aging. 2006;10(5):410–415.
12. Chan DC, Kasper JD, Black BS, Rabins PV. Prevalence and correlates of behavioral and psychiatric symptoms in community-dwelling elders with dementia or mild cognitive impairment: the memory and medical care study. Int J Geriatr Psychiatry. 2003;18(2):174–182. doi:10.1002/gps.781
13. Lyketsos CG, Lopez O, Jones B, Fitzpatrick AL, Breitner J, DeKosky S. Prevalence of neuropsychiatric symptoms in dementia and mild cognitive impairment: results from the cardiovascular health study. JAMA. 2002;288(12):1475–1483. doi:10.1001/jama.288.12.1475
14. Chen CT, Chang CC, Chang WN, et al. Neuropsychiatric symptoms in Alzheimer’s disease: associations with caregiver burden and treatment outcomes. QJM. 2017;110(9):565–570. doi:10.1093/qjmed/hcx077
15. Pless A, Ware D, Saggu S, Rehman H, Morgan J, Wang Q. Understanding neuropsychiatric symptoms in alzheimer’s disease: challenges and advances in diagnosis and treatment. Front Neurosci. 2023;17:1263771. doi:10.3389/fnins.2023.1263771
16. Ohno Y, Kunisawa N, Shimizu S. Antipsychotic treatment of Behavioral and Psychological Symptoms of Dementia (BPSD): management of extrapyramidal side effects. Front Pharmacol. 2019;10:1045. doi:10.3389/fphar.2019.01045
17. Rege S, Carnahan RM, Johnson ML, Chen H, Holmes HM, Aparasu RR. Antipsychotic initiation among older dementia patients using cholinesterase inhibitors: a national retrospective cohort study. Drugs Aging. 2021;38(6):493–502. doi:10.1007/s40266-021-00851-9
18. DeMercy HM, Brenner CA. The relationship between antipsychotics, cognitive enhancers, and Major Adverse Cardiovascular/Cerebrovascular Events (MACCE) in older adults with behavioral and psychological symptoms of dementia. Drugs Aging. 2024;41(10):847–858. doi:10.1007/s40266-024-01134-9
19. Martinez C, Jones RW, Rietbrock S. Trends in the prevalence of antipsychotic drug use among patients with Alzheimer’s disease and other dementias including those treated with antidementia drugs in the community in the UK: a cohort study. BMJ Open. 2013;3(1). doi:10.1136/bmjopen-2012-002080
20. Blaszczyk AT, Mang BH, Garza H, Mathys M. The impact of cholinesterase inhibitors with or without memantine on antipsychotic prescribing. Consult Pharm. 2018;33(5):273–282. doi:10.4140/TCP.n.2018.273
21. Robinson M, Rowett D, Leverton A, Mabbott V. Changes in utilisation of anticholinergic drugs after initiation of cholinesterase inhibitors. Pharmacoepidemiol Drug Saf. 2009;18(8):659–664. doi:10.1002/pds.1739
22. Grossberg GT. Cholinesterase inhibitors for the treatment of alzheimer’s disease:: getting on and staying on. Curr Ther Res Clin Exp Apr. 2003;64(4):216–235. doi:10.1016/S0011-393X(03)00059-6
23. Scharre DW, Vekeman F, Lefebvre P, Mody-Patel N, Kahler KH, Duh MS. Use of antipsychotic drugs in patients with Alzheimer’s disease treated with rivastigmine versus donepezil: a retrospective, parallel-cohort, hypothesis-generating study. Drugs Aging. 2010;27(11):903–913. doi:10.2165/11584290-000000000-00000
24. Birks J. Cholinesterase inhibitors for Alzheimer’s disease. Cochrane Database Syst Rev. 2006;2006(1):CD005593. doi:10.1002/14651858.CD005593
25. Matsunaga S, Fujishiro H, Takechi H. Efficacy and safety of cholinesterase inhibitors for mild cognitive impairment: a systematic review and meta-analysis. J Alzheimers Dis. 2019;71(2):513–523. doi:10.3233/JAD-190546
26. Stapff M, Hilderbrand S. First-line treatment of essential hypertension: a real-world analysis across four antihypertensive treatment classes. J Clin Hypertens. 2019;21(5):627–634. doi:10.1111/jch.13531
27. Masurkar PP, Chatterjee S, Sherer JT, Chen H, Johnson ML, Aparasu RR. Risk of serious adverse events associated with individual cholinesterase inhibitors use in older adults with dementia: a population-based cohort study. Drugs Aging. 2022;39(6):453–465. doi:10.1007/s40266-022-00944-z
28. Kachru N, Holmes HM, Johnson ML, Chen H, Aparasu RR. Antimuscarinic use among older adults with dementia and overactive bladder: a Medicare beneficiaries study. Curr Med Res Opin. 2021;37(8):1303–1313. doi:10.1080/03007995.2021.1920899
29. Andersen RM. Revisiting the behavioral model and access to medical care: does it matter? J Health Soc Behav. 1995;36(1):1–10. doi:10.2307/2137284
30. Elixhauser A, Steiner C, Harris DR, Coffey RM. Comorbidity measures for use with administrative data. Med Care. 1998;36(1):8–27. doi:10.1097/00005650-199801000-00004
31. Moore BJ, White S, Washington R, Coenen N, Elixhauser A. identifying increased risk of readmission and in-hospital mortality using hospital administrative data: the AHRQ elixhauser comorbidity index. Med Care. 2017;55(7):698–705. doi:10.1097/MLR.0000000000000735
32. Chrischilles E, Schneider K, Wilwert J, et al. Beyond comorbidity: expanding the definition and measurement of complexity among older adults using administrative claims data. Med Care. 2014;52(Suppl 3):S75–84. doi:10.1097/MLR.0000000000000026
33. Rosenbaum PR, Rubin DB. The central role of the propensity score in observational studies for causal effects. Biometrika. 1983;70(1):41–55. doi:10.1093/biomet/70.1.41
34. McCaffrey DF, Griffin BA, Almirall D, Slaughter ME, Ramchand R, Burgette LF. A tutorial on propensity score estimation for multiple treatments using generalized boosted models. Stat Med. 2013;32(19):3388–3414. doi:10.1002/sim.5753
35. Griffin B, McCaffrey D. TWANG short course/educational videos: three videos — introduction, propensity score weighted analyses with 2 groups, and propensity score weighted analyses with more than 2 groups. RAND Corporation. 2020. https://www.rand.org/pubs/presentations/PT147.html#introduction.
36. Lee BK, Lessler J, Stuart EA. Improving propensity score weighting using machine learning. Stat Med. 2010;29(3):337–346. doi:10.1002/sim.3782
37. Austin PC, Yu AYX, Vyas MV, Kapral MK. Applying propensity score methods in clinical research in neurology. Neurology. 2021;97(18):856–863. doi:10.1212/WNL.0000000000012777
38. Austin PC, Stuart EA. Moving towards best practice when using inverse probability of treatment weighting (IPTW) using the propensity score to estimate causal treatment effects in observational studies. Stat Med. 2015;34(28):3661–3679. doi:10.1002/sim.6607
39. VanderWeele TJ, Ding P. Sensitivity analysis in observational research: introducing the E-Value. Ann Intern Med. 2017;167(4):268–274. doi:10.7326/M16-2607
40. Colovic MB, Krstic DZ, Lazarevic-Pasti TD, Bondzic AM, Vasic VM. Acetylcholinesterase inhibitors: pharmacology and toxicology. Curr Neuropharmacol. 2013;11(3):315–335. doi:10.2174/1570159X11311030006
41. Raina P, Santaguida P, Ismaila A, et al. Effectiveness of cholinesterase inhibitors and memantine for treating dementia: evidence review for a clinical practice guideline. Ann Intern Med. 2008;148(5):379–397. doi:10.7326/0003-4819-148-5-200803040-00009
42. Lombardo S, Maskos U. Role of the nicotinic acetylcholine receptor in alzheimer’s disease pathology and treatment. Neuropharmacology. 2015;96(Pt B):255–262. doi:10.1016/j.neuropharm.2014.11.018
43. Giacobini E, Spiegel R, Enz A, Veroff AE, Cutler NR. Inhibition of acetyl- and butyryl-cholinesterase in the cerebrospinal fluid of patients with alzheimer’s disease by rivastigmine: correlation with cognitive benefit. J Neural Transm. 2002;109(7–8):1053–1065. doi:10.1007/s007020200089
44. Lanctot KL, Rajaram RD, Herrmann N. Therapy for alzheimer’s disease: how effective are current treatments? Ther Adv Neurol Disord. 2009;2(3):163–180. doi:10.1177/1756285609102724
45. Lilienfeld S. Galantamine--a novel cholinergic drug with a unique dual mode of action for the treatment of patients with alzheimer’s disease. CNS Drug Rev. 2002;8(2):159–176. doi:10.1111/j.1527-3458.2002.tb00221.x
46. Qaseem A, Snow V, Cross JT Jr, et al. Current pharmacologic treatment of dementia: a clinical practice guideline from the American College of Physicians and the American Academy of Family Physicians. Ann Intern Med. 2008;148(5):370–378. doi:10.7326/0003-4819-148-5-200803040-00008
47. Dou KX, Tan MS, Tan CC, et al. Comparative safety and effectiveness of cholinesterase inhibitors and memantine for alzheimer’s disease: a network meta-analysis of 41 randomized controlled trials. Alzheimers Res Ther. 2018;10(1):126. doi:10.1186/s13195-018-0457-9
 © 2025 The Author(s). This work is published and licensed by Dove Medical Press Limited. The
full terms of this license are available at https://www.dovepress.com/terms
and incorporate the Creative Commons Attribution
- Non Commercial (unported, 3.0) License.
By accessing the work you hereby accept the Terms. Non-commercial uses of the work are permitted
without any further permission from Dove Medical Press Limited, provided the work is properly
attributed. For permission for commercial use of this work, please see paragraphs 4.2 and 5 of our Terms.
© 2025 The Author(s). This work is published and licensed by Dove Medical Press Limited. The
full terms of this license are available at https://www.dovepress.com/terms
and incorporate the Creative Commons Attribution
- Non Commercial (unported, 3.0) License.
By accessing the work you hereby accept the Terms. Non-commercial uses of the work are permitted
without any further permission from Dove Medical Press Limited, provided the work is properly
attributed. For permission for commercial use of this work, please see paragraphs 4.2 and 5 of our Terms.