Back to Journals » Therapeutics and Clinical Risk Management » Volume 21
Risk Factors for Sigmoid Colonic Anastomosis: A Comparative and Cross-Sectional Analysis
Authors Talih T, Sonmez G ![]() , Sozuer EM, Tombul ST
, Sozuer EM, Tombul ST ![]() , Kulturoglu MO
, Kulturoglu MO ![]() , Islam DG, Akyıldız HY, Demirtas A, Karaagac M, Dal F
, Islam DG, Akyıldız HY, Demirtas A, Karaagac M, Dal F
Received 6 February 2025
Accepted for publication 20 July 2025
Published 4 August 2025 Volume 2025:21 Pages 1219—1226
DOI https://doi.org/10.2147/TCRM.S521002
Checked for plagiarism Yes
Review by Single anonymous peer review
Peer reviewer comments 2
Editor who approved publication: Professor De Yun Wang
Tutkun Talih,1 Gokhan Sonmez,2 Erdogan M Sozuer,1 Sevket Tolga Tombul,3 Mahmut O Kulturoglu,4 Dogan G Islam,1 Hızır Y Akyıldız,1 Abdullah Demirtas,2 Mustafa Karaagac,1 Fatih Dal1
1Department of General Surgery, Erciyes University, Kayseri, Turkey; 2Department of Urology, Erciyes University, Kayseri, Turkey; 3Department of Urology, Acibadem Hospital, Kayseri, Turkey; 4Department of General Surgery, Etlik City Hospital, Ankara, Turkey
Correspondence: Gokhan Sonmez, Email [email protected]
Objective: To evaluate the anastomotic leakage (AL) rates in cancerous and non-cancerous intestinal anastomoses and analyze the general risk factors for AL.
Methods: The primary endpoint of this study is to investigate whether there is a difference in terms of AL between patients who underwent sigmoid colon resection + colorectal anastomosis due to primary colon cancer (Group 1) and patients with a completely healthy colorectal region who underwent sigmoid colon resection + colorectal anastomosis for use in the orthotopic bladder during radical cystoprostatectomy (Group 2). The secondary endpoint, considering all the patients, is to evaluate and investigate the risk factors affecting the AL rates.
Results: A total of 178 patients, including 63 (35.4%) patients in Group 1 and 115 (64.6%) patients in Group 2, were included in the study. The mean age of all patients was 61.7 ± 9.9 years, and there was no statistical difference between the mean ages of the groups (62.8 ± 11.3 vs 60.7 ± 6.1, p = 0.106, respectively). Thirty-six (20.2%) of the patients were female, and 142 (79.8%) were male. There was no significant difference between the groups in terms of AL in the postoperative period. Postoperative AL was seen in three patients (4.8%) and six patients (5.2%) in Group 1 and Group 2, respectively (p = 0.642). According to univariate and multiple logistic regression analysis, the risk of AL increased in patients with comorbidities, in the presence of previous abdominal surgery, in patients with high neutrophil-to-lymphocyte ratio, and patients with postoperative ileus (p values are 0.042, 0.010, 0.029 and 0.048, respectively).
Conclusion: Our data suggest that anastomosis due to colon cancer resection does not increase the risk of AL compared with healthy bowel anastomoses. In addition, some clinical factors have been found to compromise anastomotic safety and are risk factors for AL. In addition, some clinical factors have been found to endanger anastomotic safety and are risk factors for AL.
Keywords: colorectal anastomosis, anastomotic leakage, bladder cancer, colon cancer, risk factors
Introduction
Colorectal cancer is one of the most common cancers experienced globally.1 The colorectal cancer epidemiology varies between different part of the world as well as between ages, genders and racial groups. There are multiple factors, which including risk factor exposure, demographic variations in addition to genetic susceptibility-genetic mutations and their effect on the prognosis and treatment response.2 Surgical treatment forms the basis of colorectal cancer treatment. The tumor-involved segment should be resected together with its lymphovascular pedicle. For the lesion in the sigmoid colon, resection should be performed up to the level of peritoneal reflection after the sigmoid branches of the inferior mesenteric artery are ligated and cut. Afterward, an anastomosis is performed between the descending colon and the upper rectum.3
Radical cystoprostatectomy is the standard treatment for localized but muscle-invasive bladder cancer. If the patient’s condition is suitable for this surgery, the primary preference is to replace the removed bladder with a new orthotopic bladder. One of the methods used for the orthotopic bladder is to make a bladder from the sigmoid colon. In making a sigmoid bladder, the pedicle of the sigmoid colon is preserved and transected. An anastomosis is performed between the descending colon and the upper rectum.4,5
Early complications in patients undergoing resection for use in the orthotopic bladder and colorectal cancer are generally associated with bowel anastomosis. Despite the advances in diagnosis, treatment, and surgical techniques in these patients, the problem of anastomotic leakage (AL) still maintains its importance. It continues to be one of the important causes of morbidity for patients.6
There are a limited number of studies in the literature on whether colon cancer increases the likelihood of anastomotic leakage, but the data are conflicting.7,8 In this study, patients who underwent sigmoid colon resection and colorectal anastomosis due to primary colon cancer and patients with a completely healthy colorectal region underwent sigmoid colon resection and colorectal anastomosis for use in the orthotopic bladder during radical cystoprostatectomy were compared in terms of early AL. This method aimed to investigate whether the malignancy factor in the intestinal tissue affects anastomosis safety and morbidity in this patient group.
Patients and Method
General Information About the Study
Patients who underwent sigmoid colon resection and colorectal anastomosis surgery by E** University Medical Faculty-General Surgery and Urology Clinic between January 2015 and May 2024 were included in this retrospective study.
Interventions
Patients who underwent resection + colorectal anastomosis surgery due to primary sigmoid colon cancer (Group 1) and patients who underwent radical cystoprostatectomy + colorectal anastomosis during orthotopic bladder surgery due to bladder cancer (Group 2) were compared. In addition, risk factors for AL were investigated in all patients by combining Groups 1 and 2.
Inclusion and Exclusion Criteria
Inclusion criteria are as follows: patients with primary colon cancer who underwent simultaneous resection + anastomosis; and patients with primary bladder cancer who underwent simultaneous resection + anastomosis in radical cystoprostatectomy + orthotopic sigmoid bladder surgery. Exclusion criteria are as follows: patients who underwent palliative surgery for colon cancer, patients with Stage 4 colon cancer, patients under the age of 18, pregnant women, those with chronic inflammatory (tuberculosis, sarcoidosis, etc.) and autoimmune diseases, and hematological diseases, those with a disease that could change the values of the complete blood count, those who use medications that may affect tissue healing, presence of another known malignancy, patients using steroids, patients undergoing emergency surgery, and those whose records could not be reached. In addition, patients with metastatic bladder cancer and patients with bladder cancer and diagnosed colorectal cancer in preoperative rectosigmoidoscopy were also excluded from the study.
Data Collection
In addition to some demographic data such as age, gender, body mass index (BMI), comorbidities of the patients (diabetes mellitus, asthma, chronic obstructive pulmonary disease or coronary artery disease – patients who had at least one of these diseases were marked as “present”), preoperative complete blood count results, anastomosis technique applied (hand-stapler), and anastomosis complications were recorded. Demographic, clinical data and histopathology results of the patients were obtained from the local electronic data recording system.
Study Endpoints
The primary endpoint of this study is to investigate whether there is a difference in terms of early AL between patients who underwent sigmoid colon resection + colorectal anastomosis due to primary colon cancer and patients with a completely healthy colorectal region who underwent sigmoid colon resection + colorectal anastomosis for use in the orthotopic bladder during radical cystoprostatectomy. The study’s secondary endpoint, considering all the patients, is to evaluate the risk factors affecting the development of AL.
Rectosigmoidoscopy Procedures
Preoperative rectosigmoidoscopy was performed in all patients who were planned to have an orthotopic bladder due to bladder cancer. One day before the rectosigmoidoscopy, bowel cleansing was performed by having the patients drink Sennoside A+B Calcium 300 mg solution (X-M Solution) with plenty of water. In addition, two hours before the procedure, sodium dihydrogenphosphate 19 g + Disodiumhydrogenphosphate 7 g (B.T. Enema 210 mL, transanally) were administered. The procedure was started by placing the patients in the left side position. After standard premedication (1–3 mg midazolam and 1–1.5 mcg/kg fentanyl, intravenously), the examination was performed using video-endoscopy (Fujinon XL 4450, Japan). It was followed closely with pulse-oximetry. No pathological finding was observed in the colorectal region up to the splenic flexure.
The Procedure Used in Orthotopic Bladder Surgery
Bowel cleansing was applied to all patients as described in rectosigmoidoscopy. After radical cystoprostatectomy and pelvic lymphadenectomy by the urology team, the urethral border was confirmed to be intact through frozen examination. Afterward, the vascular pedicle of the sigmoid colon was preserved, the descending colon was transected from the junction of the sigmoid colon and approximately 10 cm proximal to the pelvic reflection, and the 20–25 cm sigmoid colon in-between was separated to make an orthotopic new bladder. The proximal and distal ends of the open colon were anastomosed as double-layer and end-to-end.
The Procedure Used in Colorectal Cancer Surgery
Bowel cleansing was applied to all patients as described in rectosigmoidoscopy. The sigmoid colon was transected from the antimesenteric part and was detubularized. The detubularized segment was sutured as circular shape. The ureters were anastomosed to the newly formed sigmoid bladder with an antireflux mechanism over a double J stent. The urethral catheter was removed two weeks later. The double J catheter was removed by cystoscopy after 30 days.
Statistical Analysis
The Statistical Package for the Social Sciences-SPSS 23.0 (Armonk, NY: IBM Corp.) program was used for statistical analysis. The Kolmogorov–Smirnov test and Histogram Charts were used to determine the distribution characteristics of the data. Categorical measurements were expressed as numbers and percentages, numerical measurements showing normal distribution were expressed as mean ± standard deviation (SD), and numerical data not showing normal distribution were expressed as median (1–3 quartile). Pearson chi-square and Fisher exact tests were used to compare categorical data. In comparing continuous measurements between groups, the independent samples t-test was used for parameters with normal distribution. The Mann–Whitney U-test was used for parameters that did not show normal distribution. Logistic regression analyzes were used to evaluate the relationship between variables (univariate and multiple).
In the post-hoc power analyses for χ²-tests, the power of the study sample size was calculated as 0.87 when the effect size was 0.3 (since moderate-AL is a rare pathology), the alpha error rate was 0.05, and the total sample size was 168 patients. The p-value of 0.05 was accepted as statistically significant.
Results
A total of 178 patients, including 63 (35.4%) patients in Group 1 and 115 (64.6%) patients in Group 2, were included in the study. Thirty-six (20.2%) of the patients were female, and 142 (79.8%) were male. The mean age of all patients was 61.7 ± 9.9 years, and there was no statistical difference between the mean ages of the groups (62.8 ± 11.3 vs 60.7 ± 6.1, p = 0.106, respectively). Although, the rate of additional disease was higher in patients who were operated on with the diagnosis of colon cancer than in patients with bladder cancer (p < 0.001). Some demographic and clinical data of all patients and groups are given in Table 1.
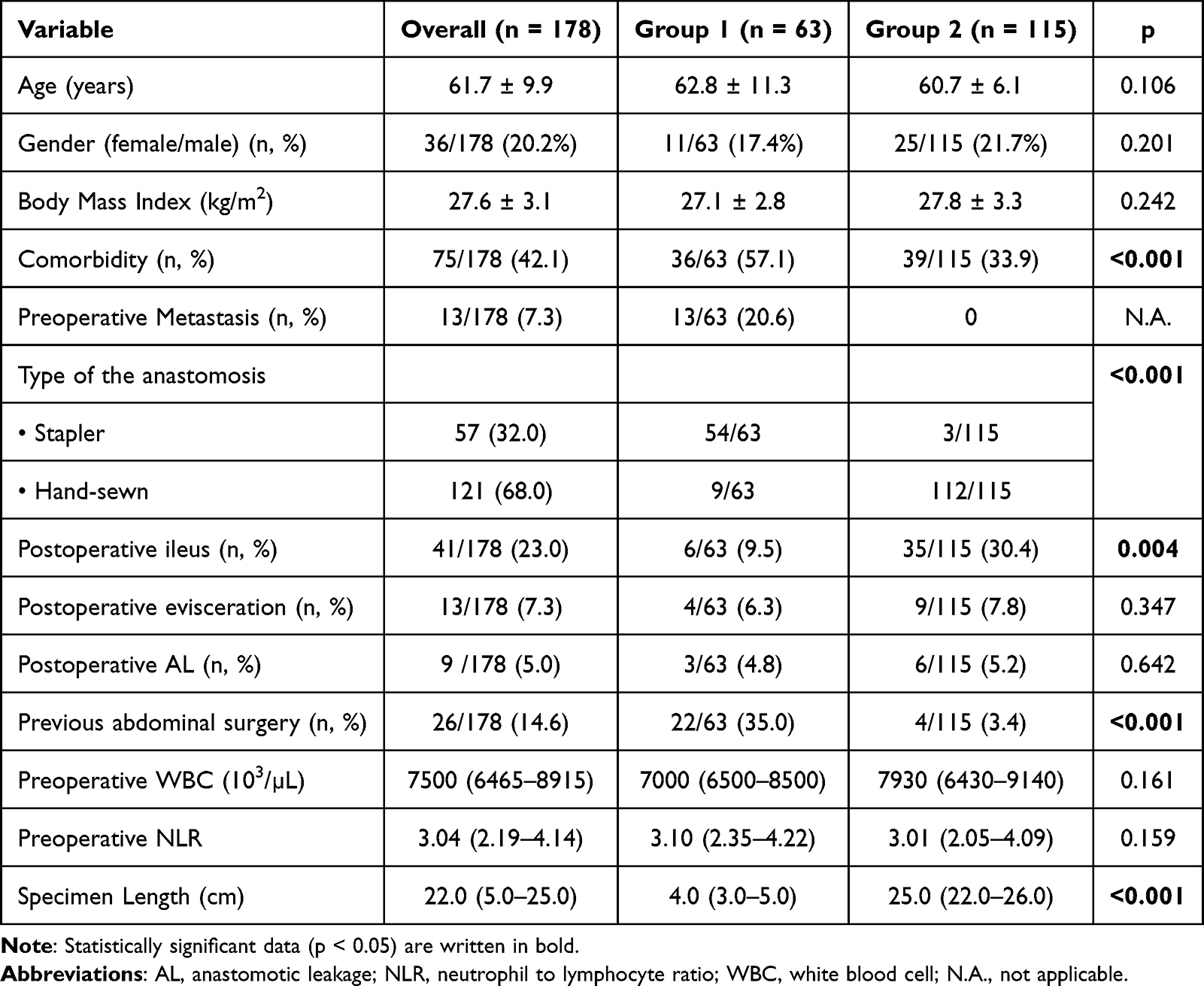 |
Table 1 Demographics and Some Clinical Data of the Groups |
It was observed that colorectal anastomosis was performed manually in 55 patients (87.6%) in Group 1 and all but three of the patients in Group 2. While postoperative anastomotic leakage was observed in three (4.8%) patients in Group 1, postoperative anastomotic leakage was observed in six (5.2%) patients in Group 2. There was no statistically significant difference between the two groups regarding postoperative AL (p = 0.642). When the white blood cell and Neutrophil to Lymphocyte Ratio (NLR) obtained from the preoperative complete blood count were analyzed, it was observed that the groups were similar (p = 0.461, p = 0.159, respectively) (see Table 1).
When the relationship between age, gender, BMI, presence of additional disease, history of previous abdominal surgery, presence of colon ca, the anastomosis method applied (hand-stapler), presence of preoperative metastasis, preoperative NLR, postoperative early ileus-evisceration, specimen length, and postoperative anastomotic leakage is evaluated in univariate and multiple logistic regression analyses, it was observed that the risk of AL increased in patients with comorbidities, in the presence of previous abdominal surgery, in patients with high NLR, and patients with postoperative ileus (see Table 2).
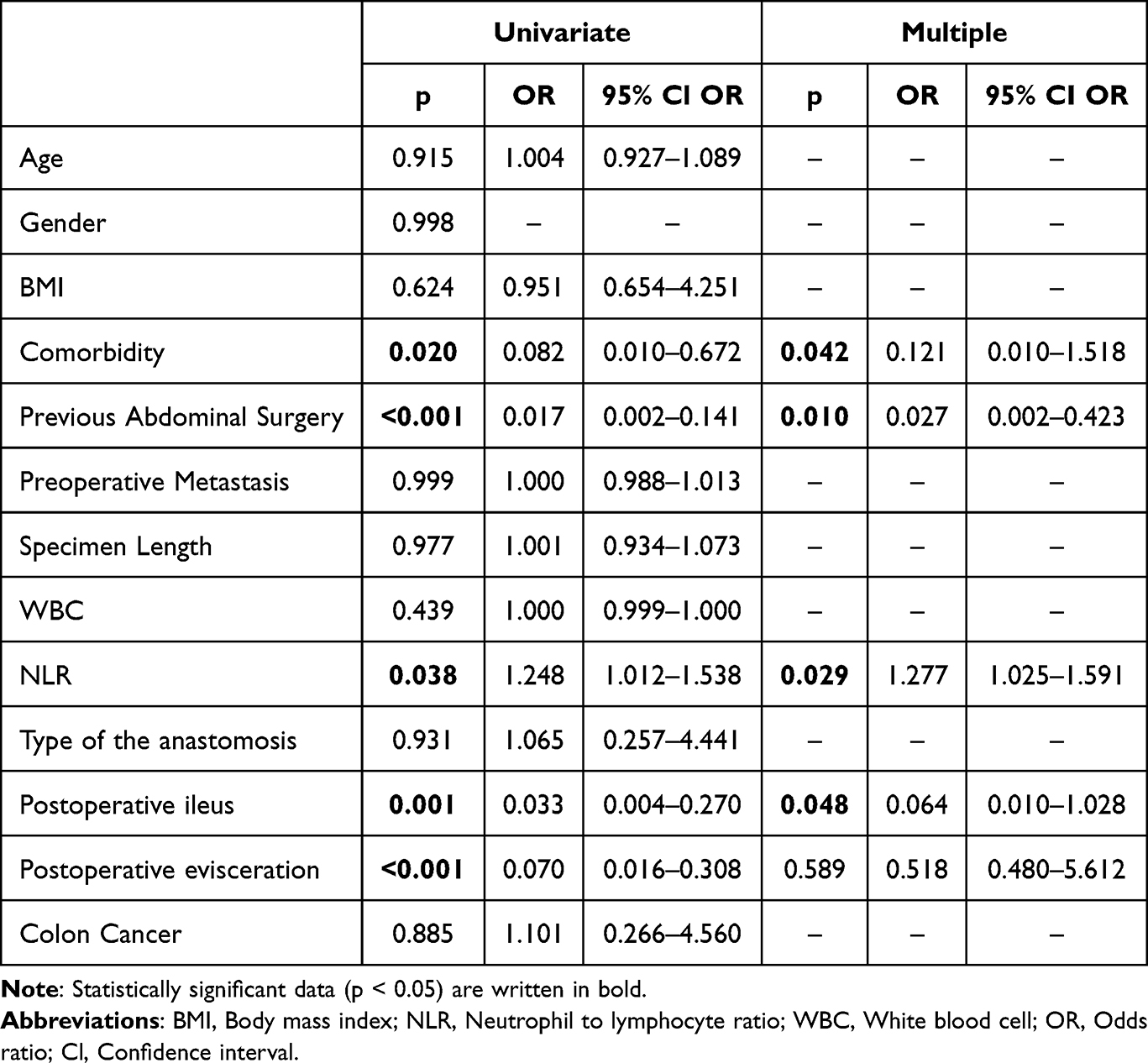 |
Table 2 Evaluation of Factors Affecting Anastomotic Leakage in Univariate and Multiple Logistic Regression Analyses |
Discussion
Colorectal cancer has the 3rd highest incidence out of all cancers and 2nd highest mortality globally.9 Surgery is a curative treatment method applied to approximately three-quarters of patients diagnosed with colorectal cancer. However, complications can be seen in approximately 30% of patients due to surgery.10 One of the most important of these complications is postoperative AL, and its overall incidence is reported to be between 1.5–16%.11 AL after colorectal surgeries becomes vital as it may sometimes be mortal, and it is essential to predict this complication.12
Our study investigated whether many clinical factors are risk factors for the development of anastomotic leakage. According to our findings, comorbidities, previous abdominal surgery, high NLR, and postoperative ileus development were significant risk factors for anastomotic leakage. Sakr et al published a study of 224 patients in 2017 and reported male gender, multiple comorbidities, emergency surgery status, preoperative leukocyte count, and blood transfusion as risk factors for anastomotic leakage.11 Some different results (such as gender, emergency surgery, blood transfusion) were obtained in that study compared to our study; this may be because only elective cases were included in our study. According to a recent study in which 141 patients were included, a high American Society of Anesthesiologists (ASA) score was determined as a risk factor for anastomotic leakage.13 Similarly, Kryzauskas et al reported that a high ASA score is a risk factor for anastomotic leakage.14 Although the ASA scores of the patients could not be evaluated due to the retrospective nature of our study, it can be said that we obtained similar results with these studies since the presence of comorbidities, which is a factor that may be associated with a high ASA score, poses a risk for anastomosis safety. Similar to our results, Lipska et al reported that a history of previous abdominal surgery increases the risk of anastomotic leakage.15
In addition, we aimed to investigate whether the presence of colon cancer is an anastomotic leakage risk factor by itself by adding bladder cancer + orthotopic bladder patients without colon cancer and completely healthy colonic mucosa to the study cohort. The reasons for choosing patients who have orthotopic bladders from the sigmoid colon are that these patients have completely healthy colon that have been confirmed with colonoscopy. In addition, these patients are generally patients who do not have serious comorbidities but are similar to patients with colon cancer in terms of age. There is no previous study that includes such a control group, and we believe that it will reflect the results of anastomosis performed on a healthy colon quite well compared to anastomoses performed due to ileus or other acute pathologies. However, our results showed that cancerous intestinal mucosa is not a risk factor for anastomotic leakage. According to the results of a study that included 64 patients who underwent elective surgery, it was reported that anastomotic leakage was observed at a higher rate in patients with a primary diagnosis of cancer.7 However, unlike our study, not only sigmoid colon anastomoses but all intestinal anastomoses were included in that study, which may be the reason for the difference in our results. Another study argued that as the tumor grade increases, the risk of anastomotic leakage might increase.8 However, only cancer patients were included in that study, and no comparison was made with anastomoses performed on non-cancerous patients. According to the results of a study published in 2022, delayed oral intake and more advanced histologic stages of the tumor were significantly correlated with AL.16 In that study, factors such as stapler use, tumor volume, age, and gender were found to be insignificant in the occurrence of AL, similar to our study. In addition, there are interesting studies investigating the effects of anastomosis type (side to end-end to end) and preoperative mechanical bowel cleaning on AL.17,18
Ileus is one of the most common complications after colon surgery. While postoperative ileus can be seen in 4–75% of patients after colorectal surgery, in Millan et al, postoperative ileus was found in 13.8% of patients operated on for colon cancer.19,20 In our study, postoperative ileus was observed in 23% of colon surgery patients. In addition, the reason why ileus was detected more frequently in patients undergoing bladder cancer surgery compared to patients undergoing colon cancer surgery alone in our cohort (9.5% vs 30.4%, p = 0.004) may be due to the significant prolonging of the operation time due to radical cystoprostatectomy compared to pure colon resection. Randomized controlled studies have previously shown that ileus endangers anastomosis’s safety and increases the risk of anastomotic leakage.21 Our study observed that postoperative ileus increased the risk of anastomotic leakage, consistent with the current literature.
The relationship of some inflammation markers with anastomotic leakage has been shown previously.22–24 A recent retrospective cohort study of 116 patients reported that high NLR and C-reactive protein (CRP) levels after colorectal surgeries pose a significant risk for anastomotic leakage. Still, it has been argued that the diagnostic value of CRP is superior to NLR.23 Similarly, in another study, it was argued that high NLR and CRP values increase the possibility of anastomotic leakage.24 Our study found that high NLR values were associated with anastomotic leakage, similar to these studies.
In our study, the rate of anastomotic leakage was 5%. Walker et al reported the rate of anastomotic leakage in the sigmoid colon as 8.5%.24 Voron et al reported the rate of anastomotic leakage after colon resection as 3.5% in their study in which they included 1940 patients.25 In another study that included 541 patients, this rate was reported as 6.5%.13 According to these results, it can be said that our anastomotic leakage rates are within the limits of the literature.
If a future evaluation is made regarding the approach to anastomotic leaks, some researchers have defined nomograms and indices to predict anastomotic leakage.26,27 Ma et al argued that anastomotic leakage could be predicted by pelvic anatomical measurements based on preoperative magnetic resonance images.26 In a meta-analysis in which many controlled studies were included, the PROCOLE (prognostic colorectal leakage) index was defined, and it was reported that anastomotic leakage could be predicted with the calculations made according to this index.27
There are some critical limitations in this study. The study’s retrospective nature and the small sample size are the most important. Due to the study’s retrospective nature, the inability to obtain data on patients’ ASA scores, CRP values, additional medications, and the severity of other diseases such as diabetes is one of the crucial limitations. In addition, the small sample size may have caused some data with borderline insignificant p values (such as WBC or NLR) to be found to be false negative. Although the relationship between NLR and anastomotic leakage was demonstrated, a significant NLR cutoff value could not be determined due to the small number of patients included. This may cause the study’s results not to be transferred to the daily clinical approach, and thus it is another significant limitation of our study. Finally, differences in quality of surgery between the groups might effect the results. The fact that this standardization has not been achieved is also an important imitation.
Conclusions
Our data show that colon cancer does not increase the risk of anastomotic leakage as long as resection is performed correctly. In addition, some clinical factors such as previous abdominal surgery, high NLR rate, postoperative ileus, and presence of other disease have been found to endanger anastomotic safety and are risk factors for anastomotic leakage. Further cohort studies on the subject may contribute to more clearly revealing the risk factors of anastomotic leakage and predicting it. In the future, prospective, multicenter studies with larger sample sizes are needed to investigate the etiology and risk factors of AL, which is an important clinical problem for colorectal surgery.
Data Sharing Statement
The original contributions presented in the study are included in the article further inquiries can be directed to the corresponding author.
Ethics Statement
Study approval statement: This study protocol was reviewed and approved by Erciyes University Clinical Research Ethics Committee, approval number 2020/370.
Consent to Participate Statement
Written informed consent was obtained from all the patients before the procedures. This research was conducted ethically in accordance with the World Medical Association Declaration of Helsinki.
Author Contributions
All authors made a significant contribution to the work reported, whether that is in the conception, study design, execution, acquisition of data, analysis and interpretation, or in all these areas; took part in drafting, revising or critically reviewing the article; gave final approval of the version to be published; have agreed on the journal to which the article has been submitted; and agree to be accountable for all aspects of the work.
Funding
This research did not receive any specific grant from funding agencies in the public, commercial, or not-for-profit sectors.
Disclosure
None of the authors have any disclosures or conflicts of interest to report for this work.
References
1. Benedix F, Kube R, Meyer F, Schmidt U, Gastinger I, Lippert H. Comparison of 17,641 patients with right- and left-sided colon cancer: differences in epidemiology, perioperative course, histology, and survival. Dis Colon Rectum. 2010;53(1):57–64. doi:10.1007/DCR.0b013e3181c703a4
2. Dekker E, Tanis PJ, Vleugels JLA, Kasi PM, Wallace MB. Colorectal cancer. Lancet. 2019;394(10207):1467–1480. doi:10.1016/S0140-6736(19)32319-0
3. Brunicardi FC. Schwartz Principles of Surgery Tenth Edition. McGraw-Hill Education; 2014:1187–1188.
4. Morrison CD, Kielb SJ. Use of bowel in reconstructive urology: what a colorectal surgeon should know. Clin Colon Rectal Surg. 2017;30:207–214. doi:10.1055/s-0037-1598162
5. Farnham SB, Cookson MS. Surgical complications of urinary diversion. World J Urol. 2004;22:157–167. doi:10.1007/s00345-004-0429-5
6. Kube R, Mroczkowski P, Granowski D, et al. Anastomotic leakage after colon cancer surgery: a predictor of significant morbidity and hospital mortality, and diminished tumour-free survival. Eur J Surg Oncol. 2010;36(2):120–124. doi:10.1016/j.ejso.2009.08.011
7. Bolívar-Rodríguez MA, Magaña-Olivas F, Cázarez-Aguilar MA, Pamanes-Lozano A, Osuna-Wong BA, Peraza-Garay FJ. Risk factors associated to intestinal anastomotic leakage in elective surgery. Cir Cir. 2022;90(1):84–89. doi:10.24875/CIRU.20001324
8. Řezáč T, Špička P, Zbořil P, Stašek M, Vrba R, Klos D. Effect of reinforcement suture on anastomotic healing in rectal and sigmoid tumor resections, single-center experience: a retrospective case-controlled study. Ann Coloproctol. 2022;39:139–146. doi:10.3393/ac.2021.00948.0135
9. Bray F, Laversanne M, Sung H, et al. Global cancer statistics 2022: GLOBOCAN estimates of incidence and mortality worldwide for 36 cancers in 185 countries. CA Cancer J Clin. 2024;74(3):229–263. doi:10.3322/caac.21834
10. Brown SR, Mathew R, Keding A, Marshall HC, Brown JM, Jayne DG. The impact of postoperative complications on long-term quality of life after curative colorectal cancer surgery. Ann Surg. 2014;259(5):916–923. doi:10.1097/SLA.0000000000000407
11. Sakr A, Emile SH, Abdallah E, Thabet W, Khafagy W. Predictive factors for small intestinal and colonic anastomotic leak: a multivariate analysis. Indian J Surg. 2017;79(6):555–562. doi:10.1007/s12262-016-1556-0
12. Tabatabai A, Hashemi M, Mohajeri G, Ahmadinejad M, Khan IA, Haghdani S. Incidence and risk factors predisposing anastomotic leak after transhiatal esophagectomy. Ann Thorac Med. 2009;4(4):197–200. doi:10.4103/1817-1737.56012
13. Kostov GG, Dimov RS, Almeida DD. Risk factors for anastomotic leakage after low anterior resection. Folia Med. 2020;62(2):290–294. doi:10.3897/folmed.62.e47727
14. Kryzauskas M, Bausys A, Degutyte AE, et al. Risk factors for anastomotic leakage and its impact on long-term survival in left-sided colorectal cancer surgery. World J Surg Oncol. 2020;18(1):205. doi:10.1186/s12957-020-01968-8
15. Lipska MA, Bissett IP, Parry BR, Merrie AE. Anastomotic leakage after lower gastrointestinal anastomosis: men are at a higher risk. ANZ J Surg. 2006;76(7):579–585. doi:10.1111/j.1445-2197.2006.03780.x
16. Kronberg U, Kiran RP, Soliman MS, et al. A characterization of factors determining postoperative ileus after laparoscopic colectomy enables the generation of a novel predictive score. Ann Surg. 2011;253:78–81. doi:10.1097/SLA.0b013e3181fcb83e
17. Jašarović D, Stojanović D, Mitrović N, Stevanović D, Lazić A. Difference in predictors of anastomotic leakage depending on the level of anastomosis after colorectal cancer surgery. Acta Clin Croat. 2022;60(3):341–346. doi:10.20471/acc.2021.60.03.01
18. Danihel L, Cerny M, Dropco I, et al. Pre-operative mechanical bowel preparation does not affect the impact of anastomosis leakage in left-side colorectal surgery-a single center observational study. Life. 2024;14(9):1092. doi:10.3390/life14091092
19. Habeeb TAAM, Mohammad H, Wasefy T, Mansour MI. Outcomes of side-to-end versus end-to-end colorectal anastomosis in nonemergent sigmoid and rectal cancers: a randomized controlled clinical trial. Ann Coloproctol. 2023;39(3):231–241. doi:10.3393/ac.2021.00906.0129
20. Millan M, Biondo S, Fraccalvieri D, Frago R, Golda T, Kreisler E. Risk factors for prolonged postoperative ileus after colorectal cancer surgery. World J Surg. 2012;36:179–185. doi:10.1007/s00268-011-1339-5
21. Peters EG, Dekkers M, van Leeuwen-Hilbers FW, et al. Relation between postoperative ileus and anastomotic leakage after colorectal resection: a post hoc analysis of a prospective randomized controlled trial. Colorectal Dis. 2017;19(7):667–674. doi:10.1111/codi.13582
22. Mik M, Dziki L, Berut M, Trzcinski R, Dziki A. Neutrophil to lymphocyte ratio and C-reactive protein as two predictive tools of anastomotic leak in colorectal cancer open surgery. Dig Surg. 2018;35(1):77–84. doi:10.1159/000456081
23. Pantoja Pachajoa DA, Gielis M, Palacios Huatuco RM, et al. Neutrophil-to-lymphocyte ratio vs C-reactive protein as early predictors of anastomotic leakage after colorectal surgery: a retrospective cohort study. Ann Med Surg. 2021;64:102201. doi:10.1016/j.amsu.2021.102201
24. Walker PA, Kunjuraman B, Bartolo DCC. Neutrophil-to-lymphocyte ratio predicts anastomotic dehiscence. ANZ J Surg. 2018. doi:10.1111/ans.14369
25. Voron T, Bruzzi M, Ragot E, et al. Anastomotic location predicts anastomotic leakage after elective colonic resection for cancer. J Gastrointest Surg. 2019;23(2):339–347. doi:10.1007/s11605-018-3891-x
26. Ma T, Zhong Q, Cao W, et al. Clinical anastomotic leakage after rectal cancer resection can be predicted by pelvic anatomic features on preoperative MRI scans: a secondary analysis of a randomized controlled trial. Dis Colon Rectum. 2019;62(11):1326–1335. doi:10.1097/DCR.0000000000001481
27. Rojas-Machado SA, Romero-Simó M, Arroyo A, Rojas-Machado A, López J, Calpena R. Prediction of anastomotic leak in colorectal cancer surgery based on a new prognostic index PROCOLE (prognostic colorectal leakage) developed from the meta-analysis of observational studies of risk factors. Int J Colorectal Dis. 2016;31(2):197–210. doi:10.1007/s00384-015-2422-4
 © 2025 The Author(s). This work is published and licensed by Dove Medical Press Limited. The
full terms of this license are available at https://www.dovepress.com/terms
and incorporate the Creative Commons Attribution
- Non Commercial (unported, 4.0) License.
By accessing the work you hereby accept the Terms. Non-commercial uses of the work are permitted
without any further permission from Dove Medical Press Limited, provided the work is properly
attributed. For permission for commercial use of this work, please see paragraphs 4.2 and 5 of our Terms.
© 2025 The Author(s). This work is published and licensed by Dove Medical Press Limited. The
full terms of this license are available at https://www.dovepress.com/terms
and incorporate the Creative Commons Attribution
- Non Commercial (unported, 4.0) License.
By accessing the work you hereby accept the Terms. Non-commercial uses of the work are permitted
without any further permission from Dove Medical Press Limited, provided the work is properly
attributed. For permission for commercial use of this work, please see paragraphs 4.2 and 5 of our Terms.