Back to Journals » Clinical Ophthalmology » Volume 16
Risk Factors for Severe Bleeding Complications in Glaucoma Surgery and the Role of Antiplatelet or Anticoagulant Agents
Authors Lauermann P ![]() , Klingelhöfer A, Mielke D, Bahlmann D, Hoerauf H, Koscielny J, Sucker C, Feltgen N
, Klingelhöfer A, Mielke D, Bahlmann D, Hoerauf H, Koscielny J, Sucker C, Feltgen N ![]() , van Oterendorp C
, van Oterendorp C
Received 22 February 2022
Accepted for publication 6 April 2022
Published 22 April 2022 Volume 2022:16 Pages 1245—1254
DOI https://doi.org/10.2147/OPTH.S361867
Checked for plagiarism Yes
Review by Single anonymous peer review
Peer reviewer comments 2
Editor who approved publication: Dr Scott Fraser
Peer Lauermann,1 Anthea Klingelhöfer,1 Dorothee Mielke,2 Dirk Bahlmann,1 Hans Hoerauf,1 Juergen Koscielny,3 Christoph Sucker,4 Nicolas Feltgen,1 Christian van Oterendorp1
1Department of Ophthalmology, University Medical Center Goettingen, Goettingen, Germany; 2Department of Neurosurgery, University Medical Center Goettingen, Goettingen, Germany; 3Gerinnungsambulanz mit Hämophiliezentrum im Ambulanten Gesundheitszentrum (AGZ), Charité Universitätsmedizin Berlin, Berlin, Germany; 4COAGUMED Coagulation Center, Berlin, Germany
Correspondence: Peer Lauermann, Department of Ophthalmology, University Medical Center Goettingen, Robert-Koch Str. 40, Goettingen, 37075, Germany, Email [email protected]
Purpose: To evaluate the influences and risk factors for severe bleeding complications during glaucoma surgery, and to investigate the role of antiplatelet (AP) and anticoagulant (AC) agents.
Methods: This prospective study enrolled patients undergoing trabeculectomy, trabeculotomy (with Trabectome® or Kahook Dual Blade®), viscocanaloplasty and Ahmed or Baerveldt implants. Bleeding severity was graded on an ordinal scale ranging from 0 to 5. Immediately after surgery and one day later, the incidence and severity of bleeding events was documented on a standardized form. A grade ≥ 3 was defined as severe bleeding. The influence of known systemic disorders, the type of anesthesia, surgical procedure, intraoperative blood pressure, and the use of or change in AP or AC agents on intraoperative bleeding were analyzed.
Results: Data from 89 eyes undergoing glaucoma procedures were included (age 71.3y ± 10.5). We observed severe intraoperative bleeding in 8 eyes (9%) and found that concomitant diseases such as the history of a deep vein thrombosis or peripheral arterial occlusive disease, and the type of surgical procedure (trabeculectomy and viscocanaloplasty) were significantly associated with severe bleeding events. By contrast, the use of AP/ AC agents had no significant influence on severe intraoperative bleeding events.
Conclusion: According to the results of our study cohort, glaucoma procedures entailing scleral manipulations (trabeculectomy and viscocanaloplasty) and concomitant diseases such as the history of a deep vein thrombosis or peripheral arterial occlusive disease influence the risk of severe intraoperative bleeding events, we detected no increased risk related to concomitant antiplatelet and/ or anticoagulant medication use.
Keywords: glaucoma surgery, severe bleeding complications, antiplatelet agents, anticoagulant agents
Introduction
Intraoperative bleeding can negatively influence the ophthalmic surgical result. This is particularly true for glaucoma surgery, where bleeding can lead to procedural failure or irreversible optic-nerve damage caused by postoperatively elevated/excessive intraocular pressure.1 Patients requiring glaucoma surgery are often taking various systemic medications including antiplatelet (AP) and anticoagulant (AC) agents, and the percentage of patients taking these has been rising for years.2 The question glaucoma surgeons face is whether these medications should be discontinued for surgery to possibly reduce the risk of bleeding, or whether a potentially higher risk of thromboembolic events is acceptable.3–5 Despite its being an everyday topic for glaucoma surgeons, there is, as well as for retinal surgeons,6,7 still no standardized guideline on how to proceed with the various AP and AC agents prior to different glaucoma procedures.8 Efforts have been made to assess the effect of platelet inhibitors or anticoagulants on bleeding frequency and severity during different ophthalmic procedures. In retinal surgery, there is growing evidence that the use of anticoagulant medications is unlikely to have a significant impact on the incidence of severe bleeding complications.9–11 A prospective study of 374 retinal patients performed concurrently with this study also came to this conclusion.7 However, in glaucoma surgery, uncertainty prevails regarding the extent to which anticoagulant medications raise the intraoperative bleeding risk. Studies demonstrating an increased risk of bleeding in patients using vitamin k antagonists appeared over a decade ago.12,13 More recent reviews recommend taking an individualized approach to each patient’s preoperative management,14 but there still seems to be too little known about the influence of direct oral anticoagulants (DOACs).1,15,16 The purpose of this prospective study was thus to identify risk factors for intraoperative severe bleeding events, and to evaluate the influence of AP and AC agents on their incidence and severity in glaucoma surgical procedures. Another aim was to validate a consensus scale of bleeding complications serving as a possible guide for upcoming glaucoma studies.
Methods
Study Population and Procedure
This single-center prospective trial enrolled patients undergoing glaucoma surgery. Informed consent was obtained from all patients participating in the study. The study protocol was implemented in accordance with the Helsinki Declaration after approval by our local ethics committee (application number 16/6/18, Institutional Ethics Board, University Medical Center Goettingen, Germany). In addition to the data presented here on glaucoma patients, we had collected retinal-surgery data for a similar study on patients undergoing vitreoretinal procedures. Those data have been published.7 Inclusion criteria were age ≥ 18 years, written informed consent and a planned surgical procedure for glaucoma, which was either filtration surgery (trabeculectomy with mitomycin C; Ahmed® - or Baerveldt® glaucoma drainage device implantation), non-penetrating glaucoma surgery (viscocanaloplasty) or microincisional glaucoma surgery (goniotomy with Trabectome® or Kahook Dual Blade®). Exclusion criteria were age < 18 years, inability to give consent and neovascularization glaucoma. Interventions were carried out by two different surgeons (CvO, DB).
Study Procedure
On the day of hospital admission, patients were asked about their medications affecting coagulation, and about any concomitant cardiovascular diseases. In addition, patients completed a standardized questionnaire on known intraoperative bleeding events in the past evaluated in conjunction with different surgical interventions. According to the 12 answers given in the questionnaire, a score was calculated.17
We developed a classification system for a standardized assessment of the severity of bleeding events, which were graded on an ordinal scale ranging from 0 to 5 with 0 indicating no bleeding event and 5 indicating severe bleeding necessitating cessation of the surgical procedure (Table 1).
 |
Table 1 Bleeding Severity Grades; Scale Level 3 or Higher is Defined as Severe Bleeding (Gray) |
Immediately after surgery and again the day thereafter, the bleeding incidence was documented in a standardized form and the bleeding severity graded. Severe bleeding was classified by a bleeding grade of 3 or higher (Table 1). We analyzed the influence of several factors on the incidence of severe bleeding: the type of intervention, anesthetic procedure, first or repeated intervention, surgery duration, presence of diabetes mellitus, blood pressure at specific time points during the surgical procedure (start/end/min/max/postop) and influence of AP and/or AC agents (including supplementals known for influences on hemostasis: gingko biloba and garlic extract). The use of AP and/or AC agents was documented for all patients, but their treatment was not modified perioperatively. Depending on the instruction of the referring general practitioner or ophthalmologist, patients discontinued, adjusted, or continued their medication unchanged prior to surgery. The International Normalized Ratio (INR) was not routinely measured in patients taking the vitamin K antagonists (VKA) phenprocoumon or warfarin. In patients anticoagulated with VKA who suffered intraoperative bleeding complications, we measured the INR value immediately after surgery.
Surgical Procedures
Trabeculectomy with Mitomycin C
Corneal traction suture. Fornix-based peritomy supero-nasal or -temporal. Placement of a mitomycin-C 0.2 mg/mL-soaked sponge for three minutes followed by 20 mL BSS rinse. Three-millimeter-wide scleral flap after careful diathermy to close episcleral vessels in the area of flap preparation. Trabeculectomy with 15° blade, iridectomy with vannas scissors. Placement of 10–0 nylon sutures at the scleral flap until the desired amount of filtration was reached. Re-adaptation of tenon’s capsule and conjunctiva at the limbus with 7–0 or 8–0 polyglactin and placement of a limbal conjunctival running suture 10–0 nylon or polyglactin.
Glaucoma Drainage Device Implantation
Corneal traction suture. Fornix-based peritomy over 2–3 clock hours in the temporal, nasal superior or nasal inferior quadrant enlarged by radial incisions at both ends. Priming or ligation of tube, depending on the type of implant (Ahmed FP7 (New World Medical, Rancho Cucamonga, CA, USA) or Baerveldt 350 (Johnson & Johnson Surgical Vision, Inc. 2019)). Scleral fixation of the endplate with 8–0 polypropylene sutures at 8–10 mm limbus distance. Transscleral anterior chamber entry with a 22-gauge needle. Scleral fixation of the tube after insertion using two 10–0 nylon sutures. Coverage of the tube with bovine pericardium (Tutopatch, Tutogen Medical GmbH) scleral fixated with 8–0 polyglactin sutures. Re-adaptation of tenon’s capsule and conjunctiva at the limbus with 7–0 polyglactin plus 8–0 polyglactin for the radial conjunctival incisions.
Viscocanaloplasty
Corneal traction suture. Fornix-based peritomy in a superior quadrant. Preparation of 2 scleral flaps without prior diathermy. Catheterization of Schlemm’s canal with a canaloplasty catheter (RUCK Ophthalmologische Systeme GmbH, Germany). Attachment of a 10–0 polypropylene suture at the tip and catheter retraction while injecting 10mg/mL hyaluronic acid gel (Healon, Johnson & Johnson Surgical Vision, Inc. 2019) at every 2nd clock hour. Removal of the deep scleral flap and closure of the superficial flap and conjunctiva with 8–0 polyglactin sutures.
Goniotomy with Kahook Dual Blade
Two temporal 1mm clear cornea incisions, one for an anterior chamber maintainer, the other for the blade. Local anesthesia with 1% intracameral lidocaine. Opening of Schlemm’s canal over 1 to 2 clock hours in each direction. Peeling of detached trabecular meshwork strips with 25G forceps. Pilocarpine 2% after surgery and three times daily from postoperative day 1 on.
Goniotomy with the Trabectome
1.8 mm clear cornea incision. Local anesthesia with 1% intracameral lidocaine. No use of viscoelastic substances. Opening of Schlemm’s canal over 1 to 2 clock hours into each direction. Trabectome energy set to 0.9 volts. Pilocarpine 2% after surgery and three times daily from postoperative day 1 on.
Statistics
Statistical analysis was performed using SAS Visual Statistics (SAS Institute Inc., Cary, USA) and Prism 6 (6.07, Graph Pad, La Jolla, USA). The t-test was used to determine statistical differences in the mean values of groups. We also applied the Chi-Square test and the exact Fisher test. Data are presented as mean ± standard error of the mean. P-values < 0.05 were regarded statistically significant. Due to very few severe bleeding events, multivariate analysis was not feasible.
Results
Study Population and Baseline Characteristics
Between February 2019 and December 2020, 89 consecutive patients undergoing glaucoma surgery were included in this study. Goniotomy was performed in 44 patients (49.4%), 38 of whose were done with the Trabectome and 6 with the Kahook Dual Blade. Trabeculectomy was performed in 30 patients (33.7%), viscocanaloplasty in 9 (10.1%) and glaucoma drainage device implantation (Ahmed or Baerveldt) in 6 patients (6.7%).
Baseline patient characteristics are outlined in Table 2, the type of procedures and number of severe bleeding events are outlined in Table 3.
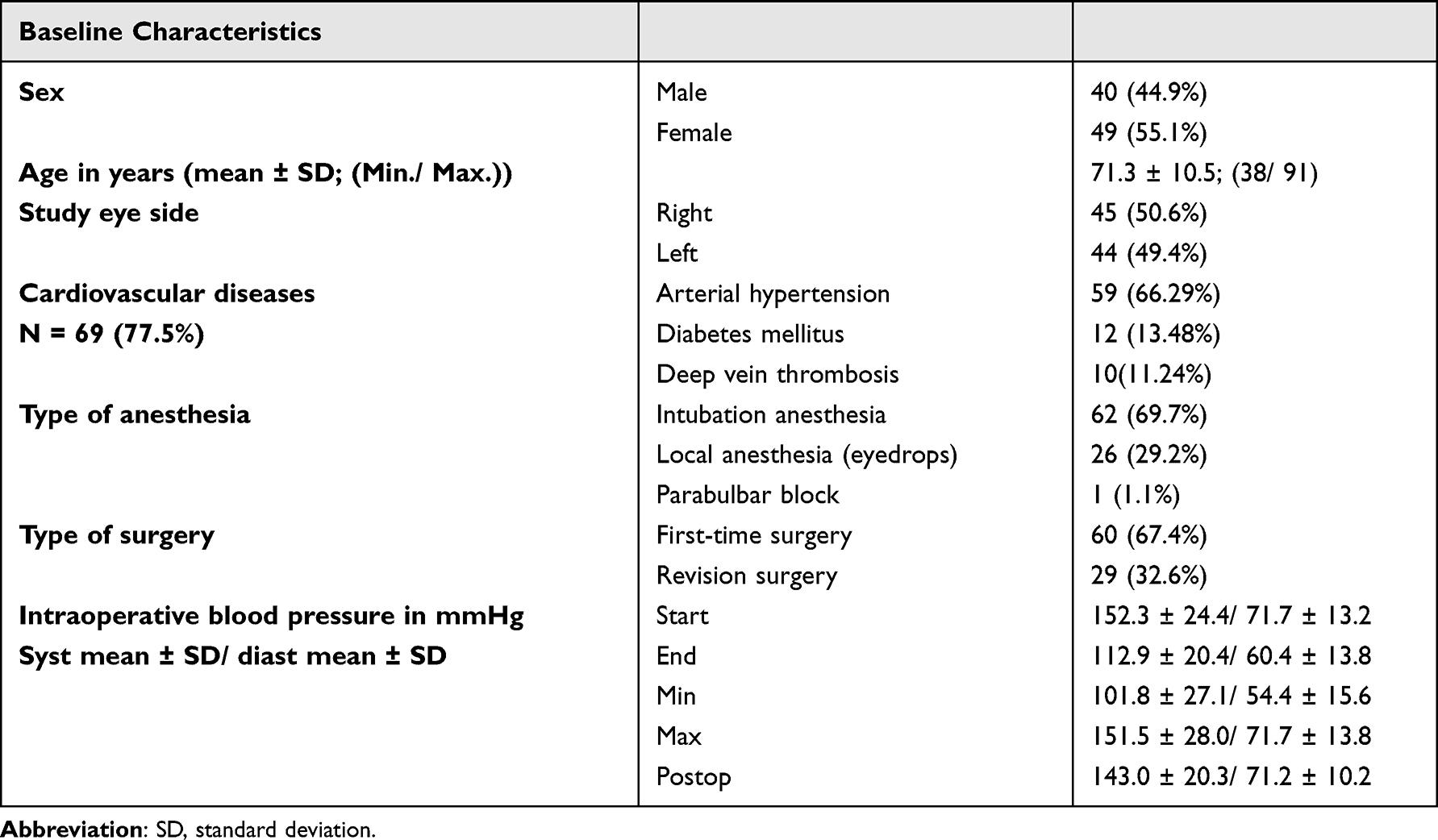 |
Table 2 Baseline Characteristics |
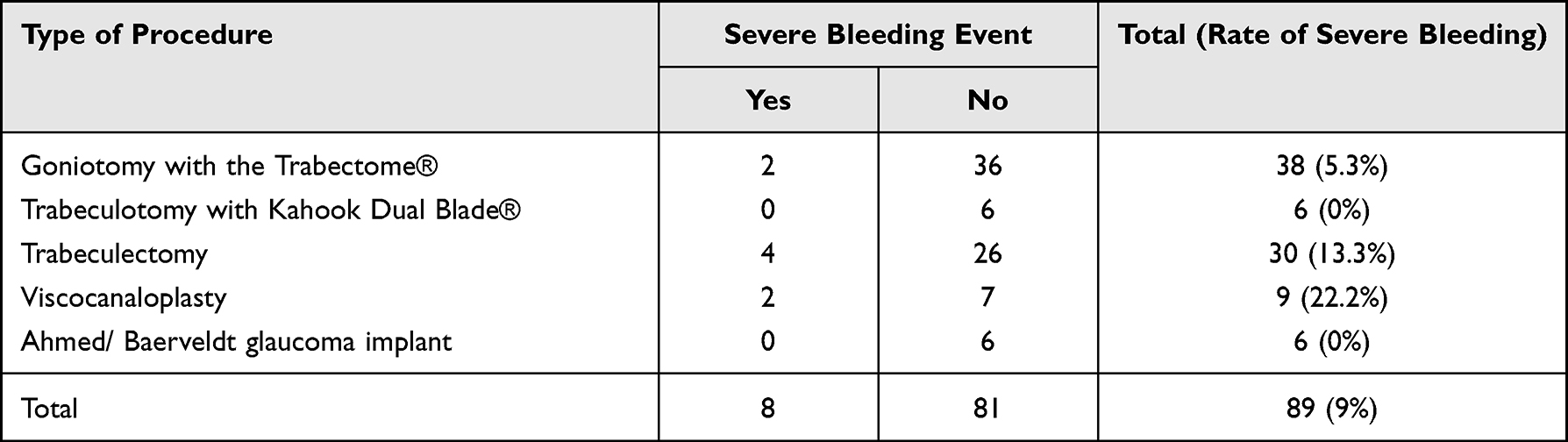 |
Table 3 Type of Procedures and Number of Severe Bleeding Events, Respectively |
Severe Intraoperative Bleeding Events
Of the 89 glaucoma procedures carried out, we registered 8 (9.0%) procedures involving severe intraoperative bleeding events. The severe bleeding events had different origins, with multiple origins possible per procedure. An overview of the total numbers for all bleeding origins is provided in Table 4. Origins for severe bleedings were the conjunctiva (n = 1, grade 3), trabecular meshwork/ iris (n = 2, grade 3), sclera/ ciliary body (n = 5, grade 3; n = 1, grade 4) and choroid (n = 1, grade 5). One patient suffered a vision-threatening hemorrhage, necessitating a second surgical procedure.
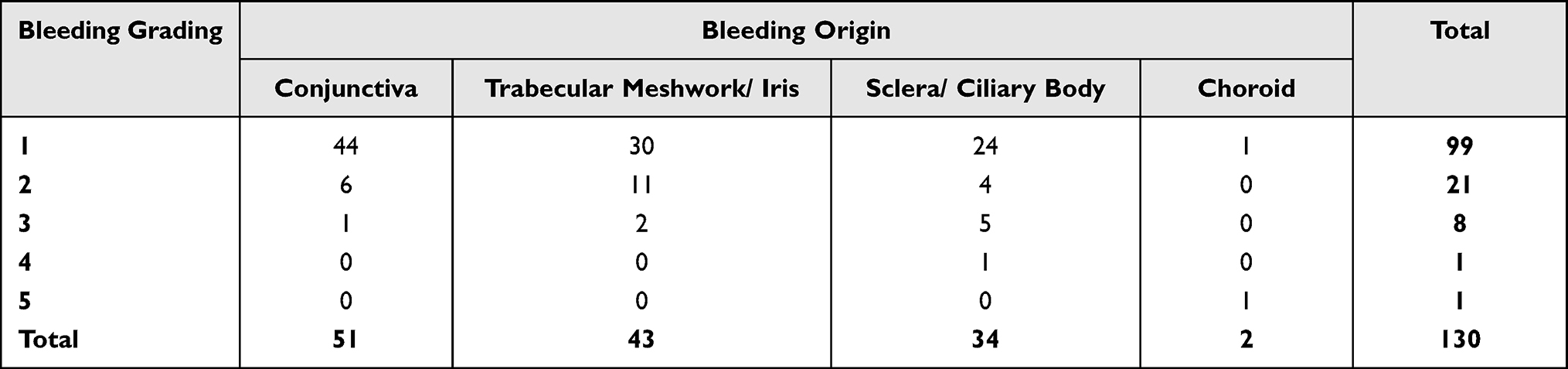 |
Table 4 Total Number of Bleeding Origins and Bleeding Severity |
Analysis of Influences and Risk Factors for Severe Intraoperative Bleeding Events in Glaucoma Surgery
Correlation to Age, Surgery Duration, Intraoperative Blood Pressure, Type of Anesthesia and First-Time or Revision Surgery
Patients suffering severe intraoperative bleeding were the same age as those without bleeding events (mean ± SD in years: 73.1 ± 7.5 vs 71.1 ± 10.8; P = 0.61). Most patients suffering intraoperative bleeding were male (7 vs 1, P = 0.01). The duration of surgery revealed a significant difference between patients with severe bleeding and those without, with longer durations in the severe-bleeding group (mean ± SD in min.: 49.6 ± 23.9 vs 33.7 ± 19.2, P = 0.044). However, there was no statistically significant difference in the procedure’s duration between first-time and revision surgery (P = 0.47). Additionally, we detected no significant correlation between severe intraoperative bleeding events and blood pressure measured at different time points, or with the type of anesthesia (P > 0.05).
Influence of Concomitant Cardiovascular Diseases
Patients suffering severe bleeding events (N = 8) frequently presented the following comorbidities: arterial hypertension (N = 4; 50%), deep vein thrombosis (N = 3, 37.5%), peripheral artery occlusive disease (N = 2; 25%) and a history of coronary stent implantation (N = 2; 25%). While the proportion of arterial hypertension in the group of severe bleeding events (50%) corresponded well with its frequency in the general population (66.3%), deep vein thrombosis, peripheral artery occlusive disease and history of coronary stent implantation were clearly overrepresented in the bleeding-event group (37.5% vs 11.2%; 25% vs 4.5% and 25.0% vs 9%). In Fisher’s exact test, we identified a significant correlation between deep vein thrombosis or peripheral artery occlusive disease and severe bleeding events (P = 0.04 and P = 0.04). There was no significant correlation between severe bleeding and a history of coronary stent implantation (P = 0.15).
Type of Procedure
Of the five different procedure categories, the most severe intraoperative bleeding events were seen in trabeculectomies (N = 4; 50%). Severe bleeding occurred in 2 patients in both the goniotomy and viscocanaloplasty groups (25% each). Considering the total number of different surgical procedures performed, trabeculectomies and viscocanaloplasties showed the highest rate of severe bleeding complications (13.3% and 22.2%). Compared with the study population, bleeding occurred with disproportionate frequency in trabeculectomy (50% of the severe bleedings registered compared to only 33.71% of the surgical procedures in total) and viscocanaloplasty procedures (25% of the severe bleedings compared to only 10.11% surgical procedures in total). For a detailed overview of these numbers, refer to Table 3.
Correlation Between the Questionnaire Score and Incidence of Major Bleeding Complications
We identified no significant correlation between the questionnaire score and likelihood of a severe bleeding event (P = 0.39). Nor did we observe any association between the incidence of bleeding complications and any of the 12 different criteria mentioned in the questionnaire.17
AP and AC Agents
At the time of the surgery, 32 (36%) patients were taking an AP (N = 23; 71.8%) or AC (N = 8; 25%) agent or supplementals having a potential effect on hemostasis (N = 5, 15.6%) among their medications (combination of AP and AC possible). Of these patients, 13 (40.6%) continued with their medication unchanged. In 21 (65.6%) patients, AP or AC agents were discontinued, and 2 (6.3%) patients underwent bridging with heparin. Detailed information on changes in medication with AP or AC agents is shown in Table 4. Changes in the use of AP or AC agents were either recommended by the referring ophthalmologist or family doctor. Of the 32 patients taking AP or AC agents among their medications, 5 (15.6%) patients experienced a severe bleeding event during surgery. Of these 5 bleeding events, 4 occurred under AP agents and 2 under AC agents (combination of AP and AC agents possible). 3 (5.3%) severe bleeding events occurred in the group of patients taking no AP or AC agents. The use of AP or AC agents showed no significant association with the risk of severe bleeding complications (P = 0.13) (Tables 5 and 6). None of the AC-taking patients who suffered bleeding complications had an INR> 2.5.
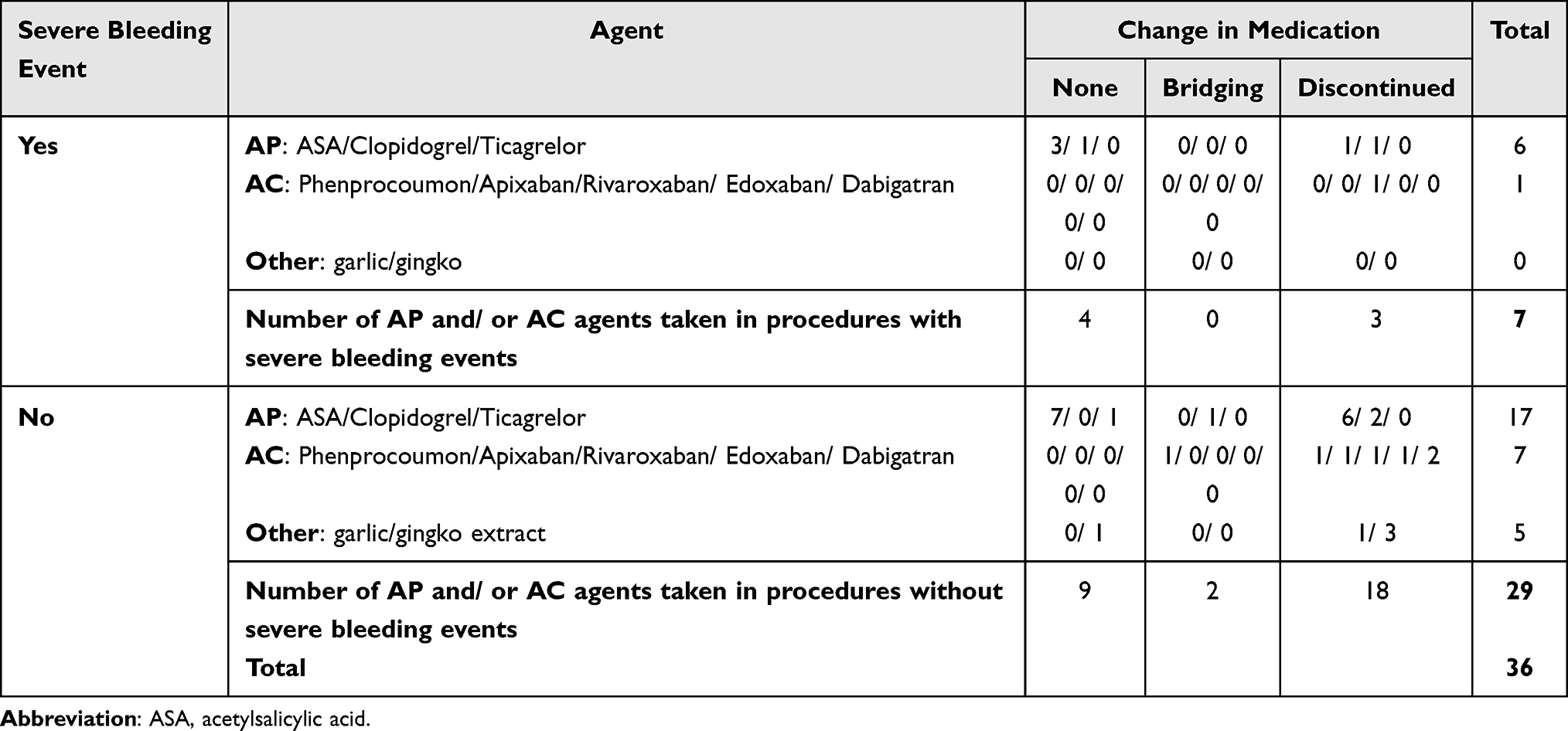 |
Table 5 Severe Bleeding Events and Change in Medication (Numbers), Total Numbers are Higher Than the Number of Severe Bleeding Events as a Combination of Different Agents Was Possible |
 |
Table 6 Severe Bleeding Events with and without AP and AC Agents, Difference Not Significant (P = 0.13) |
Discussion
In this prospective study, we analyzed data from 89 patients undergoing glaucoma surgery to identify influences and risk factors for severe intraoperative bleeding complications, and to investigate the role of antiplatelet (AP) and anticoagulative (AC) agents. A severe intraoperative bleeding event was observed in 8 patients (9%). The concomitant diseases deep vein thrombosis and peripheral artery occlusive disease, as well as the glaucoma procedures viscocanaloplasty and trabeculectomy, were found to be significantly associated with severe bleeding events. However, the use of AP and/or AC agents, as well as the intraoperative blood pressure showed no significant influence.
Strengths and Limitations of the Presented Study
With a mean age of 71.3 years and a balanced proportion of female and male patients and right and left study eyes, our patient population is a representative cohort for the glaucoma interventions we investigated.18 In direct comparison with our parallel study in retinal patients,7 the number of patients included in this study is significantly lower (89 vs 374 patients). However, this study’s prospective and monocentric nature allowed for well-controlled inclusion and assessment of our patients. Given the 9% incidence of severe bleeding complications we witnessed, the size of our study cohort suffices for global analyses, but not for detailed subgroup analyses.
Preoperative Bleeding Questionnaire
There is anesthesiological evidence that a standardized documentation of bleeding history is superior to the preoperative screening of standard coagulation parameters in predicting a patient’s intraoperative bleeding risk.17,19 Therefore, one aim of this study was to investigate the questionnaire’s applicability in glaucoma surgery. Remarkably, respective questionnaire scores showed no significant correlation with major bleeding events. These results are in line with the findings of our parallel study of vitreoretinal procedures.7 However, it must be kept in mind here that the questionnaire mainly targets congenital coagulation disorders, all of which are very rare overall and thus probably did not occur in this small cohort.
Bleeding Severity Grading
To date, there is no established grading system for intraoperative bleeding events in glaucoma surgery. In comparable studies, bleeding has only been subdivided according to its respective origin.8,12,13,15 To differentiate the extent of bleeding and distinguish relevant from less relevant bleeding events, we introduced a 5-level grading system (Table 1). The surgeon graded the bleeding immediately after the intervention. This intervention-centered grading-system perspective means that it does not consider the surgical outcome, such as IOP reduction, or the occurrence of postoperative complications, such as postoperative hyphema, intraocular pressure elevation, or fibrosis in filtration surgery. However, we believe that asking the surgeon about the extent to which bleeding affected the procedure is the necessary first step. Once the reliablity of this grading system has been proven, we may add additional factors. Despite a relatively precise definition, grading remains subjective. However, our monocentric design with only two surgeons should have enabled a fair amount of consistency.
The number of relevant bleeding events in this study was quite low because we carried out our standardized bleeding grading for each bleeding incident, reducing the number of registered hemorrhages drastically, as each patient showed signs of intraoperative bleeding in various degrees. Nevertheless, our numbers are in line with other studies. Law et al registered a bleeding rate of 6.9% in an evaluation of 694 glaucoma surgeries.13 However, as mentioned above, they did not grade the bleeding, and only defined the bleeding sources, moreover, as their evaluation was retrospective, severe bleeding events may have been overlooked.
Risk Factors for Severe Bleeding Events
Overall, as we observed only 8 major bleeding events in the 89 surgeries performed (9%), the rate of severe bleeding was as expected but the number of severe bleeding incidents was low in this study. However, this figure compares well with the study by Law et al, who reported a rate of 6.9%.13
Considering the risk factors analyzed for severe bleeding events, we found – like before in vitreoretinal surgery – that the intraoperative blood pressure exerted no significant influence. However, in terms of the surgery’s duration, those involving severe bleeding lasted significantly longer. This is attributable to the disproportionately high number of longer-lasting surgical procedures (trabeculectomy, viscocanaloplasty) in the severe bleeding group.
Considering underlying diseases, deep vein thrombosis, history of coronary stent implantation and peripheral artery occlusive diseases were overrepresented in patients suffering severe bleeding. Nevertheless, the significance of these figures remains limited due to the low number of severe bleeding events.
Considering the type of the surgical procedure, trabeculectomies and viscocanaloplasties showed the highest rates for severe intraoperative bleeding events. In contrast to our study with vitreoretinal procedures, peribulbar anaesthesia was rare (1.1%) and therefore did not show any influence on the risk of severe bleeding events.
Influence of AP/ AC Agents
There is controversy in the literature as to whether AP and AC agents should be discontinued before eye surgery.2,20–22 In vitreoretinal surgery there is a rising number of studies showing that the perioperative intake of such medications is not associated with an increased risk of intraoperative bleeding.10,20–25 Nevertheless, specialists in glaucoma surgery are more reluctant to make such statements. Rather, there seems to be consensus that the each patient’s bleeding risk should be individually assessed.15 In a retrospective evaluation of 367 trabeculectomies, Cobb et al noted that taking ASA100 raised the risk of hyphema, but had no impact on surgical success. However, taking warfarin resulted in significantly worse outcomes.12 Regarding ASA100 our results are comparable, as we likewise observed no significantly increased risk for severe bleeding. The statement by Cobb et al regarding warfarin needs to be viewed critically, as only 5 patients in their cohort were taking warfarin. Only 2 of our study patients were taking a vitamin k antagonist, thus enabling no comparison. Law et al retrospectively compared glaucoma interventions in 347 patients taking AP and/ or AC agents with 347 controls.13 Risk for bleeding complications was higher in the study group (10.1% vs 3.7%) with the overall highest risk for patients on AC medication (22.9%). Their overall recorded risk of bleeding resembled our study’s (6.9% vs 9%). However, the 22.9% risk increase in their patients taking AC agents could have been partly caused by the study`s population, which revealed significant differences between groups regarding underlying diseases, such as arterial hypertension, cardiac arrhythmia and coronary artery disease. Furthermore, as they did not grade the registered bleeding events, the effect of each bleeding event is unclear. There is a limitation associated with our study’s observational design, that is, patients were included who continued to take their AP and/or AC agents as usual, as were those who discontinued them or bridged AC agents by using heparin. This heterogeneity made analysis challenging, but it reflects the real-world clinical situation (at least in Germany).
Perspectives
Our aim was to establish a uniform grading system for intraoperative bleeding events and then to apply this grading system to evaluate the influence of various factors such as AP and/ or AC agents only on clinically relevant, severe (grade 3 or higher) bleeding events. As in our parallel study of retinal patients, this grading revealed rather few patients suffering a severe intraoperative hemorrhage. Our ability to statistically claim an increased risk for a severe bleeding event due to AP and/ or AC agents is thus limited. However, to strengthen the evidence of this study’s results, a prospective, randomized, blinded (ideally a multicenter) study would be desirable involving a larger study population to account for the few severe bleeding events, and with a blinded bleeding severity grading setup. In such a trial, the individual effect of AP/AC medication and especially novel oral anticoagulative agents and laboratory parameters such as INR or aPTT could be analyzed, as Dayani and coworkers did, as they demonstrated a higher risk of bleeding in patients with higher INR values.20 In addition, it could then be investigated whether increased conjunctival hyperemia due to the use of pressure-lowering eye drops influences the risk of severe intraoperative bleeding events.
Conclusion
According to the results of our study cohort, this study identified deep vein thrombosis, peripheral artery occlusive disease, and the glaucoma procedures viscocanaloplasty and trabeculectomy as risk factors for severe bleeding events during glaucoma surgery. The documentation of the intraoperative bleeding history before surgery does not seem to provide sufficient information to discover which patient carries a particularly high risk of severe intraoperative bleeding. Like our parallel study in vitreoretinal surgery, the present investigation also failed to detect a significant effect of AP or AC agents on intraoperative bleeding. However, since the number of registered severe hemorrhages was relatively low and severe bleeding - due to the lack of compression options in glaucoma surgery - may have a direct impact on the surgical outcome, we are reluctant to make a recommendation regarding the perioperative management of anticoagulants. A prospective, randomized, blinded study should be conducted to answer this highly relevant question.
Funding
We acknowledge support by the Open Access Publication Funds of the Göttingen University.
Disclosure
Adj. Prof. Dr. J. Koscielny: speaker honoraria from Aspen, Bayer Health Care Pharmaceuticals, Biotest, Chugai, Daiichi Sankyo, Boehringer Ingelheim, CSL Behring, Pfizer, LFB, BMS, Mitsubishi, Roche, Sanofi, Novo Nordisk, and Shire (Takeda). Adj. Prof. Dr. Koscielny is also a medical advisor for CSL Behring International, Bayer HealthCare Pharmaceuticals (national and international), and Novo Nordisk (national). He reports grants from Biomarin. Prof. Dr. Nicolas Feltgen reports grants and/or personal fees for speaker, advisory boards, and/or clinical studies from Novartis, Bayer, Allergan, Alimera, Roche, and Heidelberg, outside the submitted work. The authors report no other conflicts of interest in this work.
References
1. Makuloluwa AK, Tiew S, Briggs M. Peri-operative management of ophthalmic patients on anti-thrombotic agents: a literature review. Eye. 2019;33:1044–1059. doi:10.1038/s41433-019-0382-6
2. Oh J, Smiddy WE, Kim SS. Antiplatelet and anticoagulation therapy in vitreoretinal surgery. Am J Ophthalmol. 2011;151(934–939.e3):934–939.e3. doi:10.1016/j.ajo.2010.09.035
3. Hsueh WD, Hwang PH, Abuzeid WM. Perioperative management of antithrombotic therapy in common otolaryngologic surgical procedures: state of the art review. Otolaryngol Head Neck Surg. 2015;153:493–503. doi:10.1177/0194599815600409
4. Douketis JD, Spyropoulos AC, Spencer FA, et al. Perioperative management of antithrombotic therapy: antithrombotic Therapy and Prevention of Thrombosis, 9th ed: American college of chest physicians evidence-based clinical practice guidelines. Chest 141. 2012;141:e326S–e350S. doi:10.1378/chest.11-2298
5. Douketis JD, Spyropoulos AC, Kaatz S, et al. Perioperative bridging anticoagulation in patients with atrial fibrillation. N Engl J Med. 2015;373:823–833. doi:10.1056/NEJMoa1501035
6. Lauermann P, Dülk J, van Oterendorp C, et al. Reorganization of the perifoveal microvasculature after macular hole closure assessed via optical coherence tomography angiography. Exp Eye Res. 2020;198:108132. doi:10.1016/j.exer.2020.108132
7. Lauermann P, Klingelhöfer A, Mielke D, et al. Risk factors for severe bleeding complications in vitreoretinal surgery and the role of antiplatelet or anticoagulant agents. Ophthalmol Retina. 2021;5(8):e23–e29. doi:10.1016/j.oret.2021.04.013
8. Alwitry A, King AJ, Vernon SA, Alwitry A, King AJ, Vernon SA. Anticoagulation therapy in glaucoma surgery. Graefes Arch Clin Exp Ophthalmol. 2008;246:891–896. doi:10.1007/s00417-008-0792-9
9. Chandra A, Jazayeri F, Williamson TH. Warfarin in vitreoretinal surgery: a case controlled series. Br J Ophthalmol. 2011;95:976–978. doi:10.1136/bjo.2010.187526
10. Louison S, Gabrielle P-H, Soudry A, et al. Perioperative risk of bleeding with antithrombotic agents in macular surgery: a national, prospective, multicentre study. Acta Ophthalmol. 2020;98. doi:10.1111/aos.14434
11. Meillon C, Gabrielle PH, Luu M, et al. Antiplatelet and anticoagulant agents in vitreoretinal surgery: a prospective multicenter study involving 804 patients. Graefes Arch Clin Exp Ophthalmol. 2018;256:461–467. doi:10.1007/s00417-017-3897-1
12. Cobb CJ, Chakrabarti S, Chadha V, et al. The effect of aspirin and warfarin therapy in trabeculectomy. Eye. 2007;21:598–603. doi:10.1038/sj.eye.6702277
13. Law SK, Song BJ, Yu F, et al. Hemorrhagic complications from glaucoma surgery in patients on anticoagulation therapy or antiplatelet therapy. Am J Ophthalmol. 2008;145:736–746. doi:10.1016/j.ajo.2007.12.007
14. Shukla AG, Ramulu PY. Management of anticoagulation and antiplatelet therapy in glaucoma surgery. J Glaucoma. 2020;29:732–741. doi:10.1097/IJG.0000000000001594
15. Sozeri Y, Salim S. Anticlotting agents and the surgical management of glaucoma. Curr Opin Ophthalmol. 2018;29:185–189. doi:10.1097/ICU.0000000000000456
16. Herranz-Heras JC, Alcalde-Blanco L, Cañas-Zamarra I, et al. Actualización en el manejo perioperatorio de antiagregantes y anticoagulantes en cirugía oftalmológica (Update on the perioperative management of antiplatelets and anticoagulants in ophthalmic surgery). Arch Soc Esp Oftalmol. 2020;96:52–55. doi:10.1016/j.oftal.2020.11.006
17. Koscielny J, Ziemer S, Radtke H, et al. A practical concept for preoperative identification of patients with impaired primary hemostasis. Clin Appl Thromb Hemost. 2004;10:195–204. doi:10.1177/107602960401000301
18. Wolfram C, Pfeiffer N (2012) White paper on the situation of ophthalmic care in Germany. Deutsche Ophthalmologische Gesellschaft.
19. Pfanner G, Koscielny J, Pernerstorfer T, et al. Preoperative evaluation of the bleeding history. recommendations of the working group on perioperative coagulation of the austrian society for anaesthesia, resuscitation and intensive care (preoperative evaluation of the bleeding history. recommendations of the working group on perioperative coagulation of the austrian society for anaesthesia, resuscitation and intensive care). Der Anaesthesist. 2007;56:604–611. doi:10.1007/s00101-007-1182-0
20. Dayani PN, Grand MG. Maintenance of warfarin anticoagulation for patients undergoing vitreoretinal surgery. Trans Am Ophthalmol Soc. 2006;104:149–160.
21. Fu AD, McDonald HR, Williams DF, et al. Anticoagulation with warfarin in vitreoretinal surgery. Retina. 2007;27:290–295. doi:10.1097/01.iae.0000243033.39301.10
22. Brown JS, Mahmoud TH. Anticoagulation and clinically significant postoperative vitreous hemorrhage in diabetic vitrectomy. Retina. 2011;31: 1983–1987. doi:10.1097/IAE.0b013e31821800cd
23. Feltgen N, Mele B, Dietlein T, et al. Management of anticoagulants in ophthalmic surgery-a survey among ophthalmic surgeons in Germany (management of anticoagulants in ophthalmic surgery-a survey among ophthalmic surgeons in Germany). Ophthalmologe. 2018;115:585–591. doi:10.1007/s00347-018-0732-y
24. Bemme S, Lauermann P, Striebe NA, et al. Risk of perioperative bleeding complications in rhegmatogenous retinal detachment surgery: a retrospective single-center study. Graefes Arch Clin Exp Ophthalmol. 2020;258:961–969. doi:10.1007/s00417-019-04554-1
25. Grand MG, Walia HS. Hemorrhagic risk of vitreoretinal surgery in patients maintained on novel oral anticoagulant therapy. Retina. 2016;36:299–304. doi:10.1097/IAE.0000000000000783
 © 2022 The Author(s). This work is published and licensed by Dove Medical Press Limited. The
full terms of this license are available at https://www.dovepress.com/terms
and incorporate the Creative Commons Attribution
- Non Commercial (unported, 3.0) License.
By accessing the work you hereby accept the Terms. Non-commercial uses of the work are permitted
without any further permission from Dove Medical Press Limited, provided the work is properly
attributed. For permission for commercial use of this work, please see paragraphs 4.2 and 5 of our Terms.
© 2022 The Author(s). This work is published and licensed by Dove Medical Press Limited. The
full terms of this license are available at https://www.dovepress.com/terms
and incorporate the Creative Commons Attribution
- Non Commercial (unported, 3.0) License.
By accessing the work you hereby accept the Terms. Non-commercial uses of the work are permitted
without any further permission from Dove Medical Press Limited, provided the work is properly
attributed. For permission for commercial use of this work, please see paragraphs 4.2 and 5 of our Terms.