Back to Journals » International Journal of General Medicine » Volume 13
Risk Factors for Residual Disease in Hysterectomy Specimens After Conization in Post-Menopausal Patients with Cervical Intraepithelial Neoplasia Grade 3
Authors Sun X ![]() , Lei H
, Lei H ![]() , Xie X, Ruan G
, Xie X, Ruan G ![]() , An J
, An J ![]() , Sun P
, Sun P ![]()
Received 14 September 2020
Accepted for publication 20 October 2020
Published 10 November 2020 Volume 2020:13 Pages 1067—1074
DOI https://doi.org/10.2147/IJGM.S280576
Checked for plagiarism Yes
Review by Single anonymous peer review
Peer reviewer comments 2
Editor who approved publication: Dr Scott Fraser
Xiaoqi Sun,1 Huifang Lei,2 Xiaoyan Xie,1 Guanyu Ruan,2 Jian An,2 Pengming Sun1,2
1Department of Gynecology, Fujian Maternity and Child Health Hospital, Affiliated Hospital of Fujian Medical University, Fuzhou, Fujian 350001, People’s Republic of China; 2Laboratory of Gynecologic Oncology, Fujian Maternity and Child Health Hospital, Affiliated Hospital of Fujian Medical University, Fuzhou, Fujian 350001, People’s Republic of China
Correspondence: Jian An; Pengming Sun Laboratory of Gynecologic Oncology
Fujian Provincial Maternity and Child Health Hospital, Affiliated Hospital of Fujian Medical University, 18 Daoshan Road, Fuzhou, Fujian 350001, People’s Republic of China
Email [email protected]; [email protected]
Background: Post-menopausal patients with cervical intraepithelial neoplasia (CIN) have a high rate of residual or recurrent lesions after treatment, and their risk for cervical cancer later in life is higher than the general population. Hence, management for this specific group of post-menopausal patients needs more attention.
Objective: The study aimed to identify risk factors associated with the presence of residual disease in hysterectomy specimens in post-menopausal patients with cervical intraepithelial neoplasia grade 3 (CIN 3).
Methods: This study was a retrospective analysis of data from post-menopausal women who had undergone hysterectomy following conization for CIN 3 from 2012 to 2018 at Fujian Maternity and Child Health Hospital. Factors extracted from the database included age, parity, Thinprep cytology results, human papillomavirus (HPV) genotype, biopsy results, pre-cone endocervical curettage (ECC) results, conization method, operating surgeon, cone dimension, margin status and glandular involvement. Univariate and multivariate analyses were performed to identify risk factors associated with residual disease in hysterectomy specimens.
Results: Analysis of data from 129 women was performed. The proportion of residual disease was 43.41% overall. A higher grade according to colposcopy biopsy, abnormal pre-cone ECC results, the cone method (LEEP vs CKC), a cone volume > 1.57 cm3, and positive margins in conization specimens were found to be significantly associated with residual lesions on univariable analysis. After multivariate analysis, only an abnormal pre-cone ECC result (odds ratio 3.99; 95% confidence interval (CI) 1.41– 11.33; p = 0.009) remained significant.
Conclusion: The rate of residual lesions in uterine specimens was high regardless of the cone margin status in post-menopausal women with CIN 3. Risk-based strategies are needed to identify patients who have abnormal pre-cone ECC results, and definitive treatment with hysterectomy should be considered in post-menopausal patients with an elevated risk for residual lesions.
Keywords: cervical intraepithelial lesion, menopause, margin status, endocervical curettage
Introduction
To effectively reduce morbidity and mortality from cervical cancer, the most commonly used treatment modality for high-grade intraepithelial lesions (HSILs), or cervical intraepithelial neoplasia (CIN) grades 2–3, is excisional procedures, including the loop electrosurgical excision procedure (LEEP) and cold-knife conization (CKC).1 However, excisional treatments pose problems such as incomplete eradication with significantly higher risks of residual or recurrent lesions.2 Studies have reported that residual disease or recurrence of CIN 2+ after treatment ranges from 1.1% to 17.7%.3–11 In addition, the risk for cervical cancer in patients treated for CIN 2–3 can be fivefold higher than that in the general population.12 Therefore, to make more appropriate management decisions in clinical practice, many researchers have investigated risk factors that may predict residual disease after treatment for CIN 2–3.3,5–10,13–17 Some have found that menopausal status17 and older age (>45 years)15 are associated with a higher risk for residual disease after cervical conization. This specific group of post-menopausal or older patients needs more attention during treatment.
For post-menopausal patients, fertility requirements are not a concern. However, residual and recurrent disease or the potential of progression to cancer may cause substantial panic for these patients. Hence, researchers have proposed that definitive treatment with hysterectomy should be considered in post-menopausal patients with additional risk factors for recurrence after conization for HSILs.
To date, few previous studies have focused on post-menopausal patients with CIN 3, and few studies have examined the whole uterus after hysterectomy for the identification of residual lesions. This retrospective study was therefore designed to identify the risk factors for residual lesions in hysterectomy specimens after conization in post-menopausal patients with pathologically confirmed CIN 3.
Patients and Methods
Patients
Patients who underwent total hysterectomy after an excisional procedure for CIN 3 in the Department of Gynecology at Fujian Provincial Maternity and Child Health Hospital between October 2012 and December 2018 were included. Patients who were pre-menopausal, whose pathology reports after conization showed normal results, with CIN 1–2, with invasive cervical cancer, and adeno lesions were excluded (Figure 1). A detailed medical chart review was then performed to obtain information regarding clinical parameters from the database.
 |
Figure 1 Flow chart of post-menopausal patients underwent hysterectomy for cervical intraepithelial neoplasia grade 3 in the study. |
Clinical Data
The following parameters in medical records were abstracted: age, parity, menopausal status, cytology results, human papillomavirus (HPV) genotype, pre-cone endocervical curettage (ECC) results, cone method, operating surgeon (junior: worked in gynaecology ≤ 5 years; senior: worked in gynaecology >5 years), cone dimension (the cone volume was calculated using the formula (1/3) × π × (length/2) × (width/2) ×depth; the volumes were added when there were several pieces), and the pathological findings of conization and hysterectomy specimens.
Colposcopy and biopsy were performed by expert colposcopists in our centre. An abnormal pre-cone ECC result was considered to identify CIN in an endocervical sample obtained during colposcopy examination. The known pathologic diagnosis of the patients who were referred from other centres was verified by expert pathologists in our centre.
The LEEP or CKC was used for all conizations. Procedures were performed under colposcopic guidance and under general anaesthesia. First, all cervical transformations and cervical lesions were distinguished by the application of 5% acetic acid and Lugol’s iodine solution, and then a conical tissue sample extending to the endocervical area was excised using CKC or LEEP. When doing LEEP procedure, a rotary cut was performed to remove the entire transformation zone. As the squamocolumnar junction could not be observed, a portion of the endocervical canal from the cervix were removed from the endocervix additionally. The pathology results were classified as normal, CIN 1, CIN 2, CIN 3, or invasive cervical cancer. The resection margins of the excision specimen were not graded but were categorized as positive if precancer was present at the resection margin (endocervical, exocervical and lateral margins) or negative if the margins were free of neoplasia.18
Definitive treatment with hysterectomy was recommended for all post-menopausal patients, and patients were included in the study if the interval between conization and total hysterectomy was <6 months. Residual disease was defined as the presence of CIN 2+ or invasive cancer in hysterectomy specimens.
Ethical Considerations
The study was approved by our institutional review board (No: 2019–033), which waived the requirement for informed consent due to the retrospective nature of the study. We extracted data from the database and deidentified through anonymity to keep data confidentiality. This study was performed in compliance with the “Declaration of Helsinki.”
Statistical Analysis
Descriptive statistics were first performed. After that, univariate and multivariate analysis were performed. Univariate analysis used Chi-square test and Mann Whitney U-tests, and multivariate analysis used binary logistic regression. A p value of <0.05 was considered statistically significant. All statistical analyses were performed using SPSS version 24.0 for Windows (SPSS, Inc., Chicago, IL).
Results
Clinical Features and Pathological results
A review of the hospital records identified 150 post-menopausal patients for inclusion in this study. Among them, 73 patients (59.59%) were found to have no residual lesions. By contrast, 56 patients (43.41%) were found to have residual lesions: 4 patients (3.10%) with CIN2, 48 (37.21%) with CIN 3 and 4 (3.10%) with invasive cervical squamous cell carcinoma. The clinical features and pathological details following initial conization of these patients are shown in Table 1. The detailed characteristics of the 4 residual invasive cervical carcinoma patients are shown in Table 3.
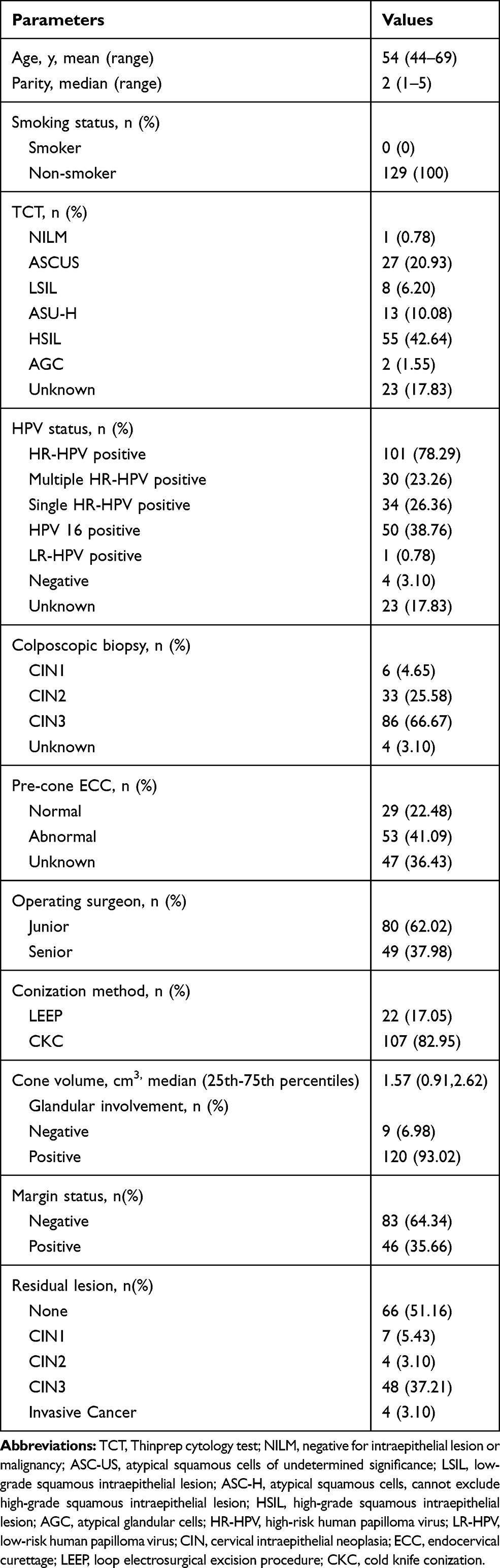 |
Table 1 General Characteristics of 129 Patients |
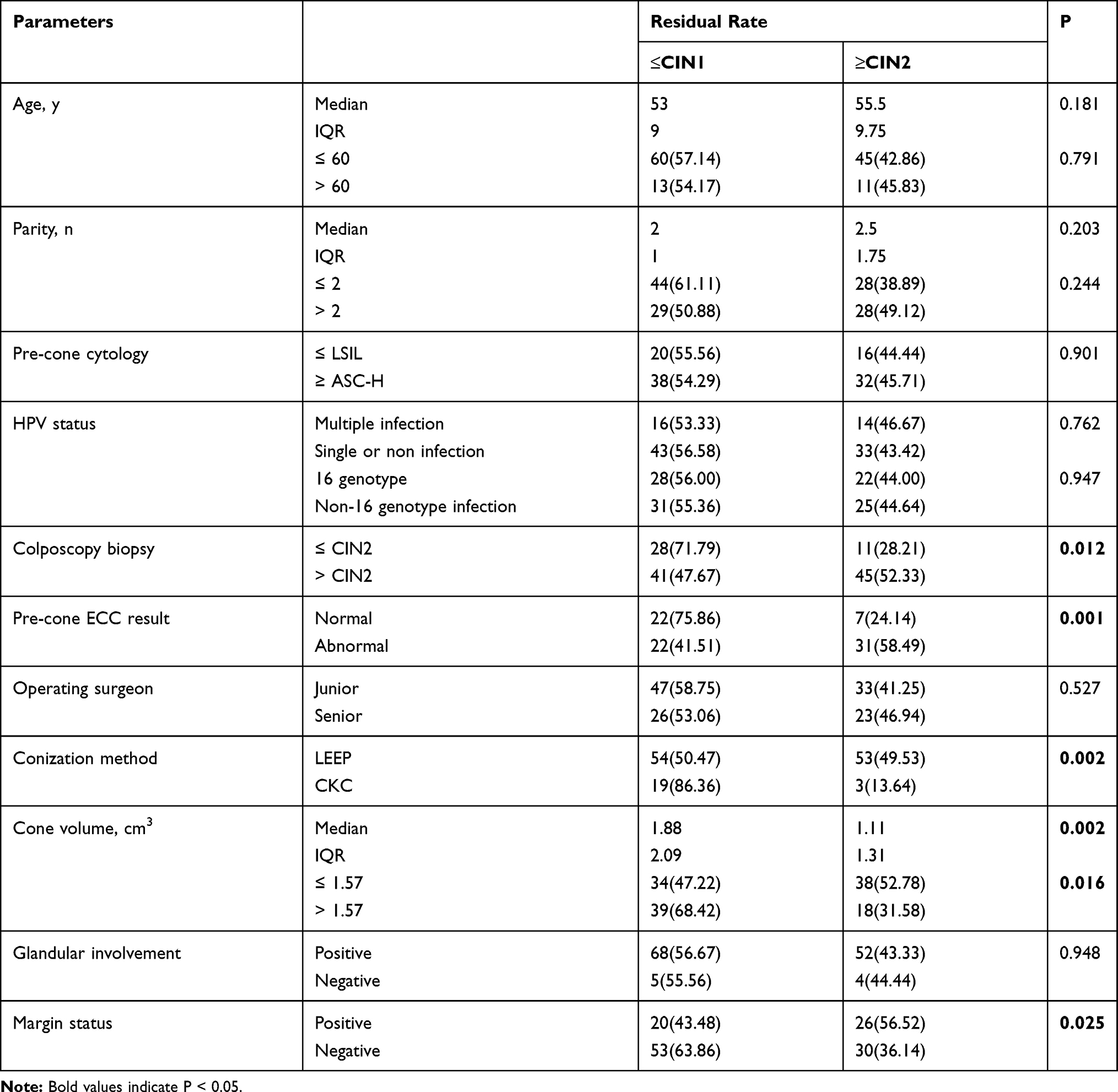 |
Table 2 Univariate Analysis on Factors Correlated with Residual Lesions in Hysterectomy Specimens |
Risk Factors for Residual Lesions After Conization
Univariate analysis showed that a higher grade according to colposcopy biopsy (>CIN2 vs ≤ CIN2), abnormal pre-cone ECC results, the cone method (LEEP vs CKC), a cone volume >1.57 cm3, and positive margins in the conization specimens were significantly associated with residual lesions (all p < 0.05, see Table 2). Age, parity, pre-cone cytology, HPV infection, colposcopy biopsy, operating surgeon, and glandular involvement were not significantly associated with residual lesions. Feasible variables that were found to be significantly associated with residual lesions on univariate analysis were entered into the logistic multiple factor regression equation. Logistic regression analysis revealed that abnormal pre-cone ECC results were an independent risk factor for residual disease (odds ratio 3.99; 95% confidence interval 1.41–11.33; p = 0.009), as shown in Table 4.
 |
Table 3 Characteristics of Patients with Residual Invasive Cervical Cancer |
 |
Table 4 Multivariate Analysis on Factors Correlated with Residual Lesions in Hysterectomy Specimens |
Discussion
Main Findings
Treatment with conization is both a diagnostic procedure and a therapeutic procedure that can effectively eradicate CIN2-3 in women at every stage of life. Treatment failure regarding residual and recurrent disease is an important concern after conization. Previous studies have reported that menopausal status and age are both associated with residual lesions after conization.15,17 In the present study, in 56 (43.41%) post-menopausal women, residual disease was discovered in hysterectomy specimens, representing a rate higher than previously reported data in younger patients. This may be explained by the specific study population of post-menopausal women and the identification of residual lesions in the hysterectomy specimens. Lower regression rate and higher surgical difficulty in postmenopausal patients could be the underlying reason. Therefore, with this high residual rate, consideration of definitive management with hysterectomy is reasonable in post-menopausal women in whom fertility is not a desire.
Furthermore, risk factors for residual lesions should be considered through a risk-based strategy for management from previous clinical information in post-menopausal women. In our study, using univariate and multivariate analyses, we found that an abnormal pre-cone ECC result was an independent risk factor for residual lesions. Several previous studies have evaluated clinical and pathological predictors of the persistence of or residual CIN and cervical cancer.3,5–10,13–17 However, only a few studies have examined whole uterine specimens after hysterectomy13 and have focused on post-menopausal patients alone. These studies differ from each other methodologically, including the study populations and analysis of variables. However, similar to our results, studies found that ECC positivity13,19,20 was a significant risk factor for residual disease. The finding that abnormal ECC results were independently associated with residual lesions in uterine specimens indicates the feasibility of identifying risk factors before conization and may be helpful in pre-procedural planning to optimize clinical management.
Interestingly, although pathologic margin status is generally considered a risk factor for the development of recurrent or persistent CIN,21,22 our results suggested that positive margins were significantly associated with residual lesions in univariate analysis but showed no significant relationship after multivariate analysis. That is, a free margin does not always indicate complete excision. Under this circumstance, in cases that invasive cancer exists and is unevaluated when the margin status is negative, simple follow-up may be inappropriate. On the other hand, undiagnosed cervical cancer may be present regardless of the margin status. For example, 4 patients were found to have invasive squamous cervical cancer after hysterectomy followed by missed diagnoses on initial conization. Even though all of them were followed, and no recurrence or metastasis occurred, a simple total hysterectomy was not adequate. The optimal treatment for post-menopausal patients with CIN 3 is still worth discussing.
Strengths and Limitations
The main strength of our study is the specific group of post-menopausal patients we included. In addition, we investigated residual lesions only in post-menopausal patients with CIN 3 disease confirmed by cone pathology. Considering that CIN 3 is the highest pathologic diagnosis before invasive cervical cancer and the difficulty of follow-up in this population, definitive treatment with hysterectomy were recommended for all postmenopausal patients in our institution. That is, decision for hysterectomy was made based on patients’ will. In other words, we have considered factors that may caused systematically biases in the conception stage and this is also a method of controlling bias. Moreover, all patients underwent hysterectomy within six months after conization so that residual disease was defined more accurately and there was little likelihood of new disease or regression/progression. However, this study had an unavoidable limitation of its retrospective design. For example, data on preoperative cytology and HPV tests were missing in some cases. Furthermore, we were not able to assess all variables potentially associated with residual lesions in the single study. Additionally, the small sample size involves only one hospital may have reduced the external validity of our results, and further prospective studies with larger sample size in a broader context are needed.
Conclusion
In summary, the results of this study suggest that the rate of residual lesions from uterine specimens is high regardless of the cone margin status in post-menopausal women with CIN 3. An abnormal pre-cone ECC result was an independent risk factor for residual lesions. The application of risk factors associated with residual lesions may provide evidence of intensive follow-up or preventive hysterectomy and may reduce the incidence of delayed treatment and inadequate treatment for post-menopausal patients with CIN 3 in clinical practice.
Funding
There is no funding to report.
Disclosure
The authors declare no conflicts of interest.
References
1. Martin-Hirsch PP, Paraskevaidis E, Bryant A, Dickinson HO, Keep SL. Surgery for cervical intraepithelial neoplasia. Cochrane Database Syst Rev. 2010;6.
2. Simoes RB, Campaner AB. Post-cervical conization outcomes in patients with high-grade intraepithelial lesions. APMIS. 2013;121(12):1153–1161. doi:10.1111/apm.12064
3. Baloglu A, Uysal D, Bezircioglu I, Bicer M, Inci A. Residual and recurrent disease rates following LEEP treatment in high-grade cervical intraepithelial lesions. Arch Gynecol Obstet. 2010;282(1):69–73. doi:10.1007/s00404-009-1298-3
4. Melnikow J, McGahan C, Sawaya GF, et al. Cervical intraepithelial neoplasia outcomes after treatment: long-term follow-up from the British Columbia Cohort Study. J Natl Cancer Inst. 2009;101(10):721–728. doi:10.1093/jnci/djp089
5. Kang WD, Kim SM. Human papillomavirus genotyping as a reliable prognostic marker of recurrence after loop electrosurgical excision procedure for high-grade cervical intraepithelial neoplasia (CIN2-3) especially in postmenopausal women. Menopause. 2016;23(1):81–86. doi:10.1097/GME.0000000000000488
6. Katki HA, Schiffman M, Castle PE, et al. Five-year risk of recurrence after treatment of CIN 2, CIN 3, or AIS: performance of HPV and Pap cotesting in posttreatment management. J Low Genit Tract Dis. 2013;17:S78–84. doi:10.1097/LGT.0b013e31828543c5
7. Kocken M, Helmerhorst TJ, Berkhof J, et al. Risk of recurrent high-grade cervical intraepithelial neoplasia after successful treatment: a long-term multi-cohort study. Lancet Oncol. 2011;12(5):441–450. doi:10.1016/S1470-2045(11)70078-X
8. Alonso I, Torne A, Puig-Tintore LM, et al. Pre- and post-conization high-risk HPV testing predicts residual/recurrent disease in patients treated for CIN 2-3. Gynecol Oncol. 2006;103(2):631–636. doi:10.1016/j.ygyno.2006.04.016
9. Del Mistro A, Matteucci M, Insacco EA, et al. Long-term clinical outcome after treatment for high-grade cervical lesions: a retrospective monoinstitutional cohort study. Biomed Res Int. 2015;2015:1–8. doi:10.1155/2015/984528
10. Leguevaque P, Motton S, Decharme A, et al. Predictors of recurrence in high-grade cervical lesions and a plan of management. Eur J Surg Oncol. 2010;36(11):1073–1079. doi:10.1016/j.ejso.2010.08.135
11. Lili E, Chatzistamatiou K, Kalpaktsidou-Vakiani A, et al. Low recurrence rate of high-grade cervical intraepithelial neoplasia after successful excision and routine colposcopy during follow-up. Medicine. 2018;97(4):e9719. doi:10.1097/MD.0000000000009719
12. Brown JV, Peters WA, Corwin DJ. Invasive carcinoma after cone biopsy for cervical intraepithelial neoplasia. Gynecol Oncol. 1991;40(1):25–28. doi:10.1016/0090-8258(91)90079-K
13. Jing L, Dan W, Zhunan L, et al. Residual lesions in uterine specimens after loop electrosurgical excision procedure in patients with CIN. Arch Gynecol Obstet. 2018;298(4):805–812. doi:10.1007/s00404-018-4881-7
14. Ayhan A, Tuncer Hasan A, Reyhan NH, et al. Risk factors for residual disease after cervical conization in patients with cervical intraepithelial neoplasia grades 2 and 3 and positive surgical margins. Eur J Obstet Gynecol Reprod Biol. 2016;201:1–6. doi:10.1016/j.ejogrb.2016.03.021
15. Swift Brenna E, Wang L, Jembere N, et al. Risk of recurrence after treatment for cervical intraepithelial neoplasia 3 and adenocarcinoma in situ of the cervix: recurrence of CIN 3 and AIS of cervix. J Low Genit Tract Dis. 2020;24(3):252–258.
16. Tasci T, Turan T, Ureyen I, et al. Is there any predictor for residual disease after cervical conization with positive surgical margins for HSIL or microinvasive cervical cancer? J Low Genit Tract Dis. 2015;19:115–118. doi:10.1097/LGT.0000000000000079
17. Bilibio JP, Monego HI, Binda MLA, et al. Menopausal status is associated with a high risk for residual disease after cervical conization with positive margins. PLoS One. 2019;14:e0217562. doi:10.1371/journal.pone.0217562
18. Bulten J, Horvat R, Jordan J, Herbert A, Wiener H, Arbyn M. European guidelines for quality assurance in cervical histopathology. Acta Oncol. 2011;50(5):611–620. doi:10.3109/0284186X.2011.555779
19. Diaz ES, Aoyama C, Baquing MA, et al. Predictors of residual carcinoma or carcinoma-in-situ at hysterectomy following cervical conization with positive margins. Gynecol Oncol. 2014;132(1):76–80. doi:10.1016/j.ygyno.2013.11.019
20. Kim HJ, Kim KR, Mok JE, et al. Pathologic risk factors for predicting residual disease in subsequent hysterectomy following LEEP conization. Gynecol Oncol. 2007;105(2):434–438.
21. Arbyn M, Redman C, Verdoodt F, et al. Incomplete excision of cervical precancer as a predictor of treatment failure: a systematic review and meta-analysis. Lancet Oncol. 2017;18:1665–1679. doi:10.1016/S1470-2045(17)30700-3
22. Serati M, Siesto G, Carollo S, et al. Risk factors for cervical intraepithelial neoplasia recurrence after conization: a 10-year study. Eur J Obstet Gynecol Reprod Biol. 2012;165(1):86–90. doi:10.1016/j.ejogrb.2012.06.026
 © 2020 The Author(s). This work is published and licensed by Dove Medical Press Limited. The
full terms of this license are available at https://www.dovepress.com/terms
and incorporate the Creative Commons Attribution
- Non Commercial (unported, 3.0) License.
By accessing the work you hereby accept the Terms. Non-commercial uses of the work are permitted
without any further permission from Dove Medical Press Limited, provided the work is properly
attributed. For permission for commercial use of this work, please see paragraphs 4.2 and 5 of our Terms.
© 2020 The Author(s). This work is published and licensed by Dove Medical Press Limited. The
full terms of this license are available at https://www.dovepress.com/terms
and incorporate the Creative Commons Attribution
- Non Commercial (unported, 3.0) License.
By accessing the work you hereby accept the Terms. Non-commercial uses of the work are permitted
without any further permission from Dove Medical Press Limited, provided the work is properly
attributed. For permission for commercial use of this work, please see paragraphs 4.2 and 5 of our Terms.