Back to Journals » Research and Reports in Urology » Volume 12
Risk Factors for Prostate Volume Progression After Prostate-Transurethral Resection
Authors Duarsa GWK, Dau DO, Pramana IBP ![]() , Tirtayasa PMW, Yudiana IW, Santosa KB, Oka AAG
, Tirtayasa PMW, Yudiana IW, Santosa KB, Oka AAG ![]() , Mahadewa TGB
, Mahadewa TGB ![]() , Ryalino C
, Ryalino C ![]()
Received 14 February 2020
Accepted for publication 20 April 2020
Published 5 May 2020 Volume 2020:12 Pages 175—178
DOI https://doi.org/10.2147/RRU.S249734
Checked for plagiarism Yes
Review by Single anonymous peer review
Peer reviewer comments 2
Editor who approved publication: Dr Jan Colli
Gede Wirya Kusuma Duarsa,1 Daniel Oktavianus Dau,1 Ida Bagus Putra Pramana,1 Pande Made Wisnu Tirtayasa,1 I Wayan Yudiana,1 Kadek Budi Santosa,1 Anak Agung Gde Oka,1 Tjokorda Gde Bagus Mahadewa,1 Christopher Ryalino2
1Department of Surgery, Faculty of Medicine, Udayana University, Bali, Indonesia; 2Department of Anesthesiology, Faculty of Medicine, Udayana University, Bali, Indonesia
Correspondence: Gede Wirya Kusuma Duarsa
Department of Surgery, Faculty of Medicine, Udayana University, Bali, Indonesia
Email [email protected]
Background: Many factors could contribute to the cases of residual benign prostate hypertrophy (BPH) volume after transurethral resection of the prostate (TURP), such as age, obesity, testosterone level, and inflammation. The goal of this study was to determine the risk of tumor necrosis factor-α (TNF-α), transforming growth factor-β (TGF-β) in prostate tissue, serum prostate-specific antigen (PSA), serum testosterone, and age in promoting prostate volume progression after TURP.
Patients and Methods: This was a prospective cohort study on 83 BPH patients who underwent TURP at five hospitals in Bali, Indonesia. Trans-rectal ultrasonography (TRUS) was carried out to examine the prostate’s size. Three years after, we redo the TRUS examination to collect the data of the latest prostate size. TNF-α, TGF-β, serum PSA, testosterone, and age were registered for analysis. We used Pearson’s and Spearman’s correlation tests and multivariate analytic linear regression test (coefficient β) by SPSS 13.0 software.
Results: Age, testosterone, PSA, TNF-α, TGF-β were positively correlated to prostate’s volume progression. The prostate volume was strongly correlated with age (r= 0.749, p < 0.001), PSA level (r=0.896, p < 0.001), testosterone level (r=0.818, p < 0.001), and TGF-β (r=0.609, p < 0.001). The TNF-α level has a weak correlation to prostate’s volume progression (r=0.392, p < 0.001).
Conclusion: TNF-α, TGF-β, PSA, testosterone, and age were significant as the risk factors in promoting the prostate volume progression after TURP.
Keywords: age, testosterone, PSA, TNF-α, TGF-β, BPH, TURP
Introduction
The gold standard surgical management for benign prostate hypertrophy (BPH) to date is still the transurethral resection of the prostate (TURP).1 Regardless, there were still 3–15% of cases with residual BPH that need reintervention.2 Many factors could contribute to the cases of residual BPH volume after TURP, such as age, obesity, testosterone level, and inflammation.
The pattern of inflammation at the molecular level has been known to affect the growth of the prostate.3 The level of proinflammatory cytokines, such as tumor necrosis factor-alpha (TNF-α), transforming growth factor-beta (TGF-β), and interleukins.4 Inflammation-induced growth factors have long been linked linearly to the development of BPH.5 Testosterone was recognized to increase the prostate volume especially in testosterone replacement therapy. The active form of this hormone, dihydrotestosterone, activated androgen receptor, and promoted prostate development.6 Prostate-specific antigen (PSA), as a marker produced by prostate’s epithelial cells, should be strongly related to the increased volume of BPH. Aging showed an increasing transitional volume of the prostate with an unknown direct mechanism.7
This was the first study, to the best of our knowledge, that determine the risk of local factors (TNF-α and TGF-β in prostate tissue) and systemic factors (PSA, testosterone, age) in promoting prostate volume progression in subjects who previously underwent TURP.
Patients and Methods
This was a prospective, cohort study on 99 patients who underwent TURP procedure in five hospitals in Bali (Sanglah General Hospital, Surya Husada Hospital, Dharma Yadnya Hospital, Balimed Hospital, and Ganesha Hospital) in 2016. The study was approved by the Committee of Ethical Research of Udayana University. All subjects provided written informed consent to be included in this study. Inclusion criteria include 50–80 years old men with prostate enlargement volume of 20–80 g by ultrasound who underwent TURP in 2016. Exclusion criteria include hypertension, diabetes, history of medical castration prior to TUR-P, neurogenic bladder, other prostate surgeries other than a single TURP, and the presence of malignancy in pathology findings.
We obtained the blood sample before the surgery to check for PSA and testosterone levels. TNF-α and TGF-β were taken from prostate tissue obtained during TURP and tested with ELISA. The subjects were followed up from 2016 to 2019. A month after TURP, we performed trans-rectal ultrasonography (TRUS) to evaluate the prostate size using the D1xD2xD3x0.52 formula. Three years later, we repeated the TRUS examination to re-evaluate the prostate’s volume progression. All TRUS examinations were carried out by a similar operator.
Data were then processed descriptively to know the sample’s characteristics and analytically with Pearson’s and Spearman’s correlation tests. We analyzed the data for the correlation coefficient value (r) and followed up with a multivariate analytic linear regression test (coefficient β). Statistical analysis was carried out with SPSS 13.0 (IBM; SPSS, Chicago, IL, USA) for Windows.
Results
Out of 99 patients who underwent TURP in 2016, only 83 patients were able to be re-evaluated. The dropout rate was 16% due to mortality. The 83 patients were re-evaluated for their prostate volume after TURP (Table 1). In this study, we found a significant correlation between all variables (age, testosterone, PSA, TNF-α, TGF-β) and prostate volume progression after TURP (p <0.001) (Table 2).
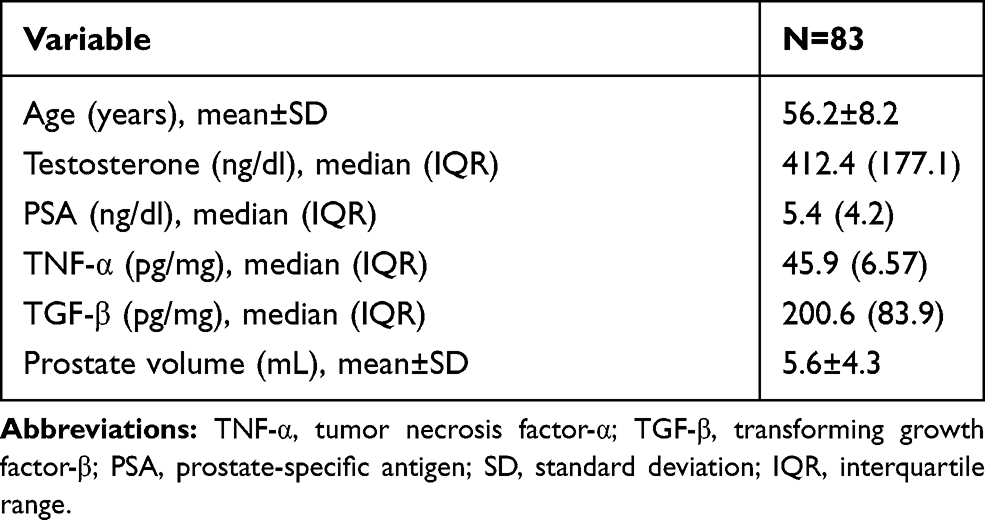 |
Table 1 Characteristics of the Subjects |
 |
Table 2 The Correlation Between Observed Variables and the Prostate Volume Progression After TURP |
We determined the correlation between the observed variables with volume progression of the prostate. We found that there was a strong correlation between age (r=0.749; p <0.001), PSA level (r=0.896; p <0.001), testosterone level (r=0.818; p <0.001), TGF-β (r=0.609; p <0.001) and volume progression of the prostate. The TNF-α level had a low correlation to prostate volume progression (r=0.392; p <0.001).
We continued the data analysis with a multivariate analysis, where we found that each additional age correlates to the volume of prostate progression by 0.106 mL (p <0.002). Each 1 ng/dl increase in PSA level affects prostate volume by 0.232 mL (p <0.001). Each 1 ng/dl increase on testosterone level affects delta prostate by 0.009 mL (p <0.001). Each 1 pg/mg increase of TNF-α increases prostate volume by 0.28 mL (p=0.011). Furthermore, 1 pg/mg increase of TGF-β increases prostate volume by 0.015 (p<0.001), as displayed in Table 3.
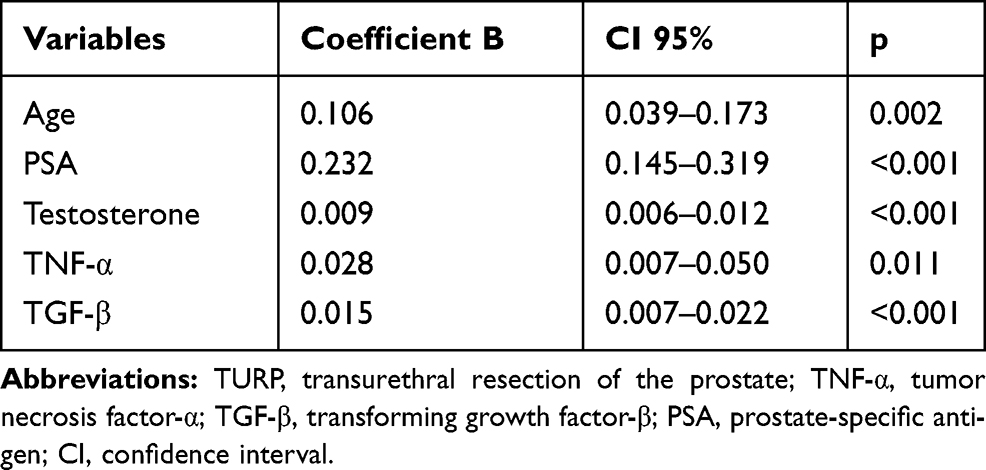 |
Table 3 Multivariate Analysis of Post TURP Prostate Volume Progression |
Discussion
BPH is associated with older age, and the prevalence increases with age. Ngai et al8 reported there was a correlation between prostate volume and patient’s age. The aging process is associated with inflammation and microvascular abnormalities, which will cause ischemia and oxidative stress, which then leads to the occurrence of BPH.9 Another study found that there was an autosomal dominant genetic predisposition in men older than 60 years old with a 72% increased risk of BPH and LUTS.10 In older age, significant prostate tissue remodeling happens, especially in a transitional zone, progressively after 70 years old.11–13 In this study, we found a significant correlation between age and prostate volume progression three years after TURP. In multivariate analysis, we found that age is a factor that has a role in prostate volume progression three years after TURP.
Testosterone is the most important androgen hormone in humans. Dihydrotestosterone (DHT) is an androgen metabolite that is very important in prostate gland cell growth. DHT is formed from testosterone by 5α-reductase.14 Roehrborn15 found that the activity of DHT is higher in prostate with BPH compared to healthy prostate tissue. Testosterone was also directly affected prostate growth.16 This is in line with this study, where the level of testosterone hormone affects prostate volume. For each 1 ng/mL increase in testosterone hormone will cause prostate volume progression after TURP by 0.009 mL (p <0.001).
PSA was a promising biomarker for prostate growth. In this study, it was found that each 1 ng/mL increase of serum PSA will cause prostate volume progression by 0.232 mL and with a highly significant correlation. Milonas et al17 reported that the growth of the prostate gland could be predicted based on the PSA level. Duarsa et al6 previously found that high PSA level (>4 ng/mL) promoted LUTS and prostate volume.
In this study, TNF-α in prostate tissue, which was taken during TURP, has a moderate correlation with prostate volume progression after TURP. This is probably because TNF-α is an acute inflammation mediator. Meanwhile, prostate enlargement is caused by chronic inflammation.9 TGF-β from prostate tissue taken during TURP has a strong significant correlation with prostate volume progression after TURP. A 1 pg/mL increase of TGF β will make prostate volume after TURP had a progression of 0.015 mL. TGF-β cytokine has a role in the regulation of cell proliferation, apoptosis, cell differentiation, and cell migration.18 In BPH, TGF-β will delay the proliferation and induce stromal cell differentiation, synthesize stromal cell collagen, and increase apoptosis.19 Prostate cells’ apoptosis rate control is controlled by TGF-β, a cytokine that affects cell proliferation, cell differentiation, and cell apoptosis. Overexpression and increase of TGF-βsignaling activity can be found in BPH’s epithelial and stromal components.20
Overall, all variables tested in this study showed a significant correlation with the residual volume progression of the prostate. This study was the first study that analyzed factors that contributed to the volume progression of the prostate after TURP. The limitation of this study was the 16% level of drop out rate due to mortality.
Conclusion
The TNF-α, TGF-β, PSA, testosterone, and age were significant as the risk factors in promoting the prostate volume progression after TURP.
Disclosure
The authors report no conflicts of interest in this study.
References
1. Patel ND, Parsons JK. Epidemiology and etiology of benign prostatic hyperplasia and bladder outlet obstruction. Indian J Urol. 2014. doi:10.4103/0970-1591.126900
2. Lepor H. Evaluating men with benign prostatic hyperplasia. Rev Urol. 2004;6:S8.
3. Taoka R, Kakehi Y. The influence of asymptomatic inflammatory prostatitis on the onset and progression of lower urinary tract symptoms in men with histologic benign prostatic hyperplasia. Asian J Urol. 2017;4(3):158–163. doi:10.1016/j.ajur.2017.02.004
4. Oka AAG, Duarsa GWK, Novianti PA, Mahadewa TGB, Ryalino C. The impact of prostate-transurethral resection on erectile dysfunction in benign prostatic hyperplasia. Res Rep Urol. 2019;11:91–96. doi:10.2147/RRU.S189414
5. Giri D, Ittmann M. Interleukin-8 is a paracrine inducer of fibroblast growth factor 2, a stromal and epithelial growth factor in benign prostatic hyperplasia. Am J Pathol. 2001;159(1):139–147. doi:10.1016/S0002-9440(10)61681-1
6. Duarsa GWK, Oka AAG, Maliawan S, et al. Elevated tumor necrosis factor-α and transforming growth factor-β in prostatic tissue are risk factors for lower urinary tract symptoms after transurethral resection of the prostate in benign prostatic hyperplasia patients with urinary retention. Open Urol Nephrol J. 2018;11(1):46–53. doi:10.2174/1874303x01811010046
7. Zhang SJ, Qian HN, Zhao Y, et al. Relationship between age and prostate size. Asian J Androl. 2013;15(1):116–120. doi:10.1038/aja.2012.127
8. Ngai HY, Yuen KKS, Ng CM, Cheng CH, Chu SKP. Metabolic syndrome and benign prostatic hyperplasia: an update. Asian J Urol. 2017;4(3):164–173. doi:10.1016/j.ajur.2017.05.001
9. Chughtai B, Lee R, Te A, Kaplan S. Role of inflammation in benign prostatic hyperplasia. Rev Urol. 2011;13:147.
10. Parsons JK. Benign prostatic hyperplasia and male lower urinary tract symptoms: epidemiology and risk factors. Curr Bladder Dysfunct Rep. 2010;5(4):212–218. doi:10.1007/s11884-010-0067-2
11. Choi H, Kim JH, Shim JS, et al. Prediction of persistent storage symptoms after transurethral resection of the prostate in patients with benign prostatic enlargement. Urol Int. 2014;93(4):425–430. doi:10.1159/000357626
12. Putra IBOW, Hamid ARAH, Mochtar CA, Umbas R. Relationship of age, prostate-specific antigen, and prostate volume in Indonesian men with benign prostatic hyperplasia. Prostate Int. 2016;4(2):43–48. doi:10.1016/j.prnil.2016.03.002
13. Deori R, Das B, Rahman MA. A study of relationship of prostate volume, prostate specific antigen and age in benign prostatic hyperplasia. Int J Contemp Med Res. 2017;4(7):1582–1586.
14. Kosaka T, Miyajima A, Oya M. Is DHT production by 5a-reductase friend or foe in prostate cancer? Front Oncol. 2014;4. doi:10.3389/fonc.2014.00247.
15. Roehrborn CG. Pathology of benign prostatic hyperplasia. Int J Impot Res. 2008;20(S3):
16. Lee CL, Kuo HC. Pathophysiology of benign prostate enlargement and lower urinary tract symptoms: current concepts. Tzu Chi Med J. 2017. doi:10.4103/tcmj.tcmj_20_17
17. Milonas D, Verikaite J, Jievaltas M. The effect of complete transurethral resection of the prostate on symptoms, quality of life, and voiding function improvement. Cent Eur J Urol. 2015;68(2). doi:10.5173/ceju.2015.507
18. De Nunzio C, Cindolo L, Gacci M, et al. Metabolic syndrome and lower urinary tract symptoms in patients with benign prostatic enlargement: a possible link to storage symptoms. Urology. 2014;84(5):1181–1187. doi:10.1016/j.urology.2014.07.018
19. Kramer G, Marberger M. Could inflammation be a key component in the progression of benign prostatic hyperplasia? Curr Opin Urol. 2006. doi:10.1097/01.mou.0000193368.91823.1b
20. Lee C, Jia Z, Rahmatpanah F, et al. Role of the adjacent stroma cells in prostate cancer development and progression: synergy between TGFβ and IGF signaling. Biomed Res Int. 2014;2014:1–8. doi:10.1155/2014/502093
 © 2020 The Author(s). This work is published and licensed by Dove Medical Press Limited. The
full terms of this license are available at https://www.dovepress.com/terms
and incorporate the Creative Commons Attribution
- Non Commercial (unported, 3.0) License.
By accessing the work you hereby accept the Terms. Non-commercial uses of the work are permitted
without any further permission from Dove Medical Press Limited, provided the work is properly
attributed. For permission for commercial use of this work, please see paragraphs 4.2 and 5 of our Terms.
© 2020 The Author(s). This work is published and licensed by Dove Medical Press Limited. The
full terms of this license are available at https://www.dovepress.com/terms
and incorporate the Creative Commons Attribution
- Non Commercial (unported, 3.0) License.
By accessing the work you hereby accept the Terms. Non-commercial uses of the work are permitted
without any further permission from Dove Medical Press Limited, provided the work is properly
attributed. For permission for commercial use of this work, please see paragraphs 4.2 and 5 of our Terms.