Back to Journals » Clinical Ophthalmology » Volume 12
Risk factors for neovascular glaucoma after vitrectomy in eyes with proliferative diabetic retinopathy
Authors Sakamoto M, Hashimoto R, Yoshida I ![]() , Ubuka M, Maeno T
, Ubuka M, Maeno T
Received 23 August 2018
Accepted for publication 16 October 2018
Published 14 November 2018 Volume 2018:12 Pages 2323—2329
DOI https://doi.org/10.2147/OPTH.S184959
Checked for plagiarism Yes
Review by Single anonymous peer review
Peer reviewer comments 4
Editor who approved publication: Dr Scott Fraser
Masashi Sakamoto, Ryuya Hashimoto, Izumi Yoshida, Makoto Ubuka, Takatoshi Maeno
Department of Ophthalmology, Toho University Sakura Medical Center, Shimoshizu, Sakura, Japan
Purpose: To investigate the potential risk factors for neovascular glaucoma (NVG) after vitrectomy in eyes with proliferative diabetic retinopathy.
Subjects and methods: In this retrospective, observational, comparative study, patients with proliferative diabetic retinopathy who underwent vitrectomy at Toho University Sakura Medical Center between December 2011 and November 2016 and who were followed for ≥12 months after surgery were included. Subject parameters examined included age, glycated hemoglobin (HbA1c), fasting blood glucose, administration of insulin, and estimated glomerular filtration rate. Ocular parameters examined included preoperative best-corrected visual acuity, preoperative IOP, operative history (specifically panretinal photocoagulation), lens status, ocular pathology (eg, iris/angle neovascularization, tractional retinal detachment, diabetic macular edema, vitreous hemorrhage, combined tractional retinal detachment), intraoperative retinal tamponade use, vitrectomy gauge, combined lens extraction/vitrectomy procedure, subsequent surgical procedures, and pre- and postoperative intravitreal bevacizumab. Correlations between variables and postoperative NVG development were examined using logistic regression analyses (backward elimination method).
Results: A total of 254 eyes of 196 consecutive subjects (146 men [74.5%], 54.0±10.8 years old) were included. Sixty of 254 eyes (23.6%) developed NVG. Several preoperative factors increased the risk of developing NVG, including iris/angle neovascularization (P=0.042), preoperative high IOP (P=0.005), low HbA1c (P=0.004), and administration of insulin (P=0.045). Intraoperative retinal tamponade also increased NVG risk (P=0.021, backward elimination method).
Conclusion: Preoperative parameters such as elevated IOP, iris/angle neovascularization, fasting blood sugar and HbA1c discrepancies, administration of insulin, as well as use of retinal tamponade during retinal surgery were identified as the risk factors for developing NVG.
Keywords: neovascular glaucoma, proliferative diabetic retinopathy, vitrectomy
Introduction
Postoperative neovascular glaucoma (NVG) is associated with vitrectomy in eyes with proliferative diabetic retinopathy (PDR) and occurs at an incidence of 2%–18%.1–6 Although treatment outcomes are improving, NVG can still result in severe visual impairment. Previously identified risk factors for NVG after vitrectomy include preoperative iris neovascularization, preoperative angle neovascularization, male sex, postoperative retinal detachment, undergoing a combination vitrectomy/lens extraction procedure, and prolonged vitreous hemorrhage (VH).7–17
The current study examines systemic state (age, glycated hemoglobin [HbA1c], fasting blood glucose, administration of insulin, and estimated glomerular filtration rate [eGFR]) and ocular characteristics (preoperative best-corrected visual acuity [BCVA] parameters, preoperative IOP, operative history [specifically panretinal photocoagulation {PRP}], lens status, ocular pathology [eg, iris/angle neovascularization, tractional retinal detachment {TRD}, diabetic macular edema {DME}, VH, combined TRD], intraoperative retinal tamponade use, vitrectomy gauge, combined lens extraction/vitrectomy procedure, subsequent surgical procedures, and pre- and postoperative intravitreal bevacizumab [IVB], pre-, intra-, and postoperative parameters) that may influence NVG risk in subjects with PDR who underwent vitrectomy. Because our study evaluated more parameters than previous studies, our results were expected to be different from those of past reports.
Subjects and methods
The study protocol for this retrospective, observational, comparative study was reviewed and approved by the ethics committee at Toho University Sakura Medical Center (approval number S17005). The study adhered to the tenets of the Declaration of Helsinki, and written informed consent was obtained from all subjects. Consent was obtained after the study design and participation risks/benefits were explained using the Toho University Sakura Medical Center website in accordance with the guidelines for clinical research set out by the Japanese Ministry of Health, Labor, and Welfare.
Study subjects
This retrospective study included patients who had undergone vitrectomy to treat PDR at Toho University Sakura Medical Center between December 2011 and November 2016. To be included, patients had to have a postoperative follow-up of at least 12 months, which was defined as the time between vitrectomy and the final visit in eyes with no NVG and the time between vitrectomy and the first documentation of NVG in eyes with NVG. Furthermore, we defined NVG as the presence of iris/angle neovascularization and elevated IOP (≥22 mmHg). We did not examine the visual field and optic nerve state because we diagnosed NVG at the time when the IOP had elevated instantly. When an elevated IOP was first detected after pars plana vitrectomy, we searched for neovascularization of the iris with a slit lamp. If no neovascularization was present, gonioscopy was performed. Eyes with elevated IOP before vitrectomy were excluded (IOP ≥22 mmHg).
Data collection
The medical records of eligible patients were retrospectively reviewed. Subject characteristics examined included sex, age, HbA1c, fasting blood glucose, eGFR, administration of insulin, and the need for hemodialysis (HD). Ocular characteristics examined included preoperative BCVA, preoperative IOP, history of recent (within 3 months) PRP, lens status, intraoperative retinal tamponade, combined lens extraction/vitrectomy procedure, pre- and postoperative IVB, vitrectomy gauge, and repeat surgeries. The presence/absence of the following conditions was also noted: obvious iris/angle neovascularization, TRD, DME, VH, and combined TRD.
Surgical procedures
Subjects underwent lens removal via phacoemulsification or pars plana lensectomy. An intraocular lens (IOL) was implanted in the posterior chamber when phacoemulsification was performed. If the posterior capsule was not ruptured, the IOL was implanted in the capsular bag. In subjects who underwent pars plana lensectomy, the IOL was implanted in front of the anterior capsule (sulcus implantation) on the same day as the extraction or at a later date. A pars plana vitrectomy was performed using a 20G, 23G, or 25G three-port vitrectomy system (Accuras® or Constellation®; Alcon Laboratories, Inc., Fort Worth, TX, USA). Following vitrectomy, fibrovascular proliferative membranes were removed and retinal neovascularization was cauterized to create a posterior vitreous detachment as peripherally as possible. The vitreous base was then shaved via scleral compression, and PRP was performed using an intraocular laser at the vitreous base with scleral depression. Retinal tamponade was achieved with gas (air, 20% SF6, or 12% C3F8) or silicone oil in eyes with a retinal detachment or a surgically created retinal tear. We selected the tamponade type depending on the extent of retinal detachment and the estimated period of retinal detachment.
Statistical analyses
All statistical analyses were performed using SPSS statistical software (version 24.0; IBM Corporation, Armonk, NY, USA). Between-group comparisons for categorical variables (sex-related differences, PRP history, preoperative lens status, pseudophakia after surgery, ocular pathology presence/absence, combined lens extraction/vitrectomy procedure, retinal tamponade use, pre- and postoperative IVB, vitrectomy gauge, repeat surgery, need for HD, administration of insulin, and postoperative lens status) were performed using Fisher’s exact tests. Between-group comparisons for continuous variables (age, IOP, BCVA, HbA1c, fasting blood glucose, eGFR, and follow-up period duration) were performed using Mann–Whitney U tests. Univariate logistic regression analyses were also performed to identify the potential risk factors for developing NVG. Initially significant parameters were further analyzed using the backward elimination method for multivariate regression analysis to identify statistically significant NVG risk factors. With respect to the retinal tamponade, we adopted two types of variables: an ordinal scale (none: 0, air: 1, gas tamponade: 2, silicone oil: 3) and classifications based on the presence or absence of the tamponade (tamponade-, tamponade+) for the univariate logistic regression analysis. But we have adopted the variable of two classifications (tamponade-, tamponade+) to the backward elimination because it was difficult to rank between gas tamponade and silicone oil. The current study involved numerous parameters. We have selected the backward elimination method to reduce the possibility of missing the minimum essential factors to develop NVG after vitrectomy for PDR. Statistical significance was defined as P<0.05.
Results
Data from 254 eyes of 196 consecutive patients (146 men, 50 women) with a mean age of 54.0±10.8 years were included. Subjects were followed for an average of 23.0±15.0 months. Sixty of 254 eyes (23.6%) developed NVG 7.2±6.2 months, on an average, after vitrectomy.
Nine patients developed NVG in both eyes; eight patients developed NVG unilaterally among the patients with vitrectomy performed in both eyes.
Pars plana lensectomy (PPL) was performed in 9 NVG patients and phacoemulsification and aspiration (PEA) in 42 NVG patients. PPL was performed in 23 patients without NVG and PEA in 144 patients without NVG.
DME was present in 37 patients (12 patients who had eyes with NVG and 25 patients who had eyes without NVG). In the 12 patients with NVG, we found cystoid macular edema (CME) in six eyes, serous detachment in three eyes, and diffuse edema in one eye. Both CME and serous detachment were found in two eyes with NVG. In the 25 patients without NVG, we found CME in nine eyes, serous detachment in seven eyes, and diffuse edema in one eye; combinations included both CME and serous detachment in five eyes, both CME and diffuse edema in one eye, and CME, serous detachment, and diffuse edema in two eyes.
Seven of 60 (11.7%) eyes with NVG were pseudophakic before vitrectomy, and we performed lens extraction at the time of vitrectomy in 51 of the 60 eyes (85.0%). Two eyes (3.3%) were phakic even after vitrectomy. Of the 194 eyes without NVG, 25 (12.9%) were pseudophakic before vitrectomy, and we performed lens extraction at the time of vitrectomy in 157 of the 194 eyes (80.9%). Twelve eyes (6.2%) remained phakic after vitrectomy.
A pars plana vitrectomy was performed using a 20G system in 53 subjects (11 eyes developed NVG, 42 eyes were without NVG), a 23G system in 31 subjects (6 eyes developed NVG, 25 eyes were without NVG), and a 25G system in 170 subjects (41 eyes developed NVG, 129 eyes were without NVG). Retinal tamponade was performed in 34 eyes with NVG with 20% SF6 in 20 eyes, 12% C3F8 in 7 eyes, and air in 7 eyes. Tamponade was also performed in 82 eyes without NVG with 20% SF6 in 50 eyes, 12% C3F8 in 10 eyes, air in 17 eyes, and silicone oil in 5 eyes.
Univariate analyses identified the preoperative presence of obvious iris/angle neovascularization, TRD, VH, and high preoperative IOP as potential risk factors for developing NVG after vitrectomy in eyes with PDR (Table 1). Additionally, logistic regression analysis revealed that obvious iris/angle neovascularization (P=0.016), TRD (P=0.014), VH (P=0.016), intraoperative retinal tamponade (P=0.050), and high preoperative IOP (P=0.022) before vitrectomy were significantly associated with NVG development (Table 2). There were no significant differences between eyes with and without NVG for intravitreal injections of antiangiogenic agents before and after surgery. After applying the backward elimination method, the preoperative risk factors for developing NVG were obvious iris/angle neovascularization, high preoperative IOP, low HbA1c, and administration of insulin. Intraoperative retinal tamponade was also identified as a significant risk factor (Table 2).
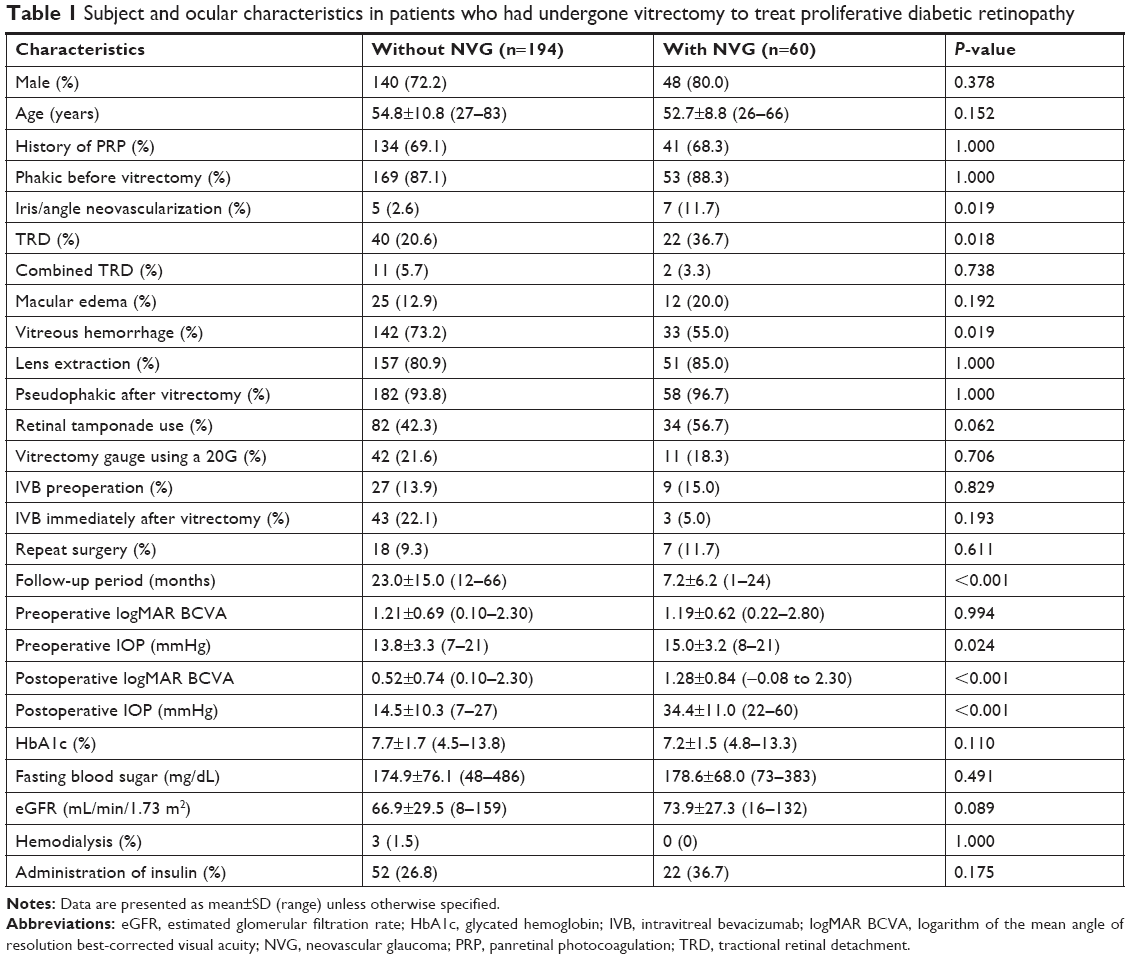 | Table 1 Subject and ocular characteristics in patients who had undergone vitrectomy to treat proliferative diabetic retinopathy |
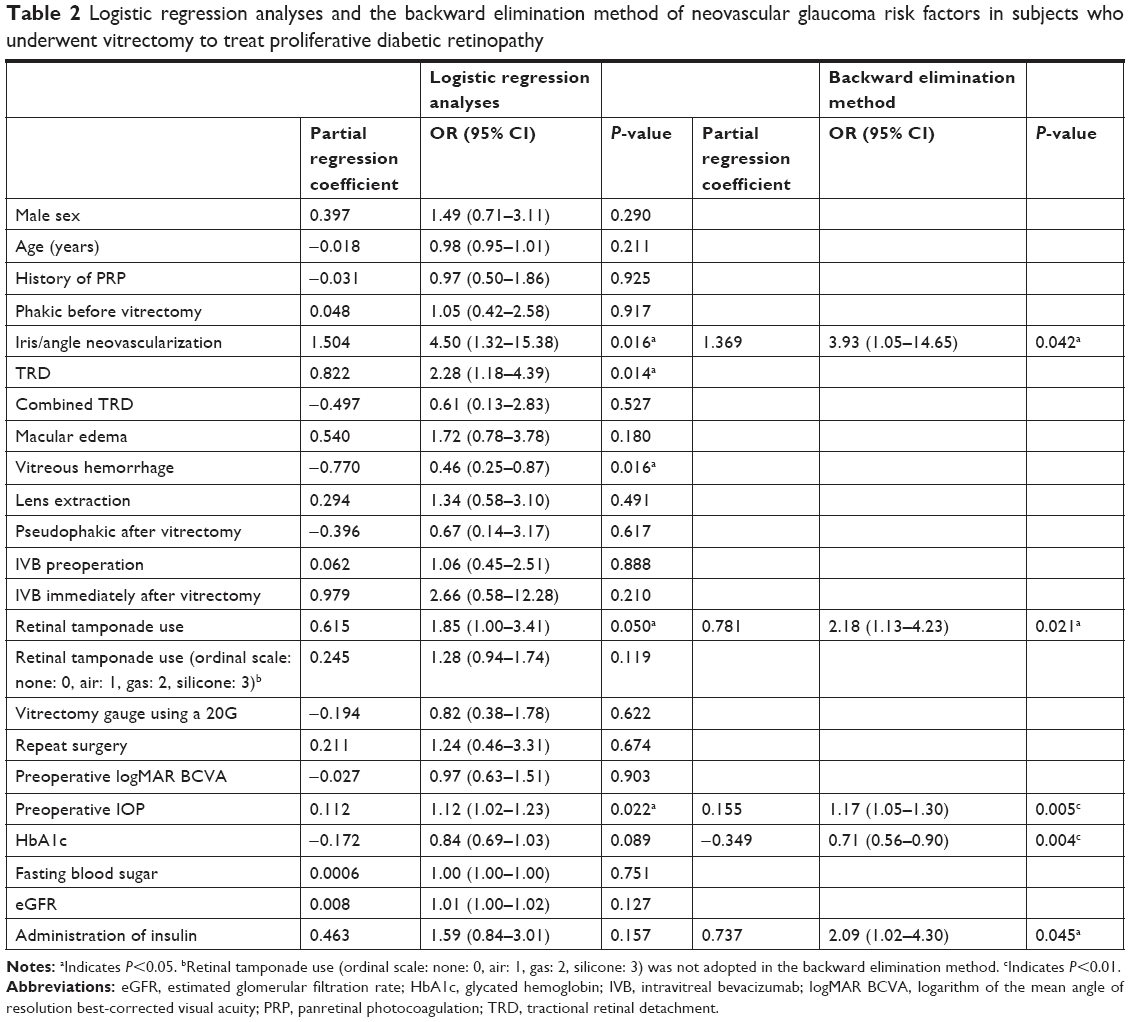 | Table 2 Logistic regression analyses and the backward elimination method of neovascular glaucoma risk factors in subjects who underwent vitrectomy to treat proliferative diabetic retinopathy |
Discussion
Preoperative risk factors for developing NVG after vitrectomy were obvious iris/angle neovascularization, high preoperative IOP, administration of insulin, and low HbA1c. The intraoperative use of retinal tamponade was also a risk factor. Previous studies have shown that obvious iris/angle neovascularization, male sex,11–14 preoperative ocular hypertension, postoperative retinal detachment, lens extraction during vitrectomy,3,7–9,15 and postoperative persistent VH were the risk factors for developing NVG.7–17 In contrast, we did not find male sex and lens extraction to be significant risk factors. However, this study showed for the first time that administration of insulin and low HbA1c before vitrectomy, and the use of retinal tamponade during vitrectomy, were the risk factors for NVG.
Previous studies have shown that NVG is more likely to develop in aphakic or pseudophakic eyes than in phakic eyes after vitreous surgery.3,8–10 However, the current study did not find an association between lens status and NVG incidence. The number of phakic eyes examined here was likely not large enough to detect significant postoperative differences between phakic and pseudophakic eyes.
Some of the NVG risk factors identified here are in agreement with a previous report,7 including the presence of obvious iris/angle neovascularization and elevated IOP before vitrectomy. Several studies have shown that inflammation in PDR patients is caused by pars plana vitrectomy,18,19 which results in an increased cytokine concentration in the anterior chamber.20,21 In patients with iris/angle neovascularization before surgery, operative damage or postoperative inflammation may have activated angle neovascularization, which can result in elevated IOP. However, quantitative analyses of neovascularization have not been performed and it may be that retinal ischemia improves following vitreous surgery, resulting in suppression of neovascularization activity in patients with mild angle closure.22 Thus, quantitative assessment of iris/angle neovascularization should be performed. Furthermore, the current study showed that NVG risk increases following PDR surgery when preoperative IOP is elevated (≥22 mmHg). Even if the IOP before vitrectomy was 21 mmHg or less, IOP in patients with obvious iris/angle neovascularization was higher than those without iris/angle neovascularization in the current study (P=0.0464, Mann–Whitney U tests). Therefore, some cases of PDR with a higher IOP before vitrectomy (but ≤21 mmHg) might be associated with potential neovascularization that may not be detected by preoperative examination. Therefore, the increased risk of NVG may have resulted from early neovascularization that was not detected with gonioscopy.23,24 This suggests that highly accurate angle/iris examination should be performed with fluorescein fundus angiography (FA) of iris before surgery.
Knowing whether intraoperative gas tamponade is a risk factor for NVG is important because of its frequent use. It has previously been shown that IOP is elevated after vitreous surgery to repair idiopathic macular holes (in patients without PDR)25 and with rhegmatogenous retinal detachment26 because of late-stage inflammation caused by surgery. Previous studies have reported increased vascular endothelial growth factor levels in aqueous humor in patients with NVG.20,21,27 A possible mechanism is inflammation of the anterior chamber in response to retinal tamponade and subsequent angle neovascularization induced by inflammatory cytokines, which directly increases the susceptibility to organic angle closure and trabecular dysfunction. These pathogenic processes also likely promote NVG development. Patients with preoperative iris/angle neovascularization are considered to have a more severe ischemic state and to be more easily affected by operative stress even if the state is improved by vitrectomy and endophotocoagulation. In the current study, there was no significant difference in the gauge of vitrectomy between eyes with NVG and without NVG. However, future studies should investigate whether the flare after vitrectomy is related to the rate of development of NVG.
Diabetic retinopathy is exacerbated when HbA1c is 6.5% or higher.28 In our study population, mean HbA1c was 7.3% in patients with NVG and 7.7% in patients without NVG. Therefore, retinopathy was likely exacerbated in both groups. However, we did observe a negative correlation between HbA1c and NVG onset. All of our subjects were taking blood glucose-lowering medications, but retinal ischemia may have been exacerbated, subsequently increasing NVG risk, in eyes with long-term PDR. Additionally, HbA1c level may have plateaued at the lowest value. Based on these findings, PDR patients who have not had strict, long-term blood sugar control are highly likely to develop NVG after vitreous surgery. Furthermore, even if HbA1c is 7%, patients with large circadian variations in blood sugar develop microvascular damage from blood sugar fluctuations,29 which may suggest ischemia progression. Cases with NVG were associated with more insulin administered than the cases without NVG. Therefore, the HbA1c of cases with NVG was lower. Although we would need to investigate the duration of diabetes mellitus, PDR with low HbA1c may be caused by severe diabetes mellitus in some cases. It is possible that there is a negative correlation between HbA1c and NVG onset. Only three patients were treated with HD; these patients were without NVG. No patient with NVG was treated with HD. The value of HbA1c in the patients treated with HD is not reliable. However, the average of HbA1c of the three patients was 5.6, less than the average of all the patients without NVG. The average of HbA1c was lower in patients with NVG than in those without NVG in the current study; hence, we believe that the influence of HD on the value of HbA1c of the patients was low in the current study.
The current study had several limitations due to its retrospective design. First, this cross-sectional study did not include a detailed examination of diabetes history or treatment prior to surgery. Second, it is possible that iris/angle neovascularization was not detected in some patients before surgery. Slit-lamp and gonioscopic examinations were used to obtain study data, but preoperative FA would increase detection rates. Many patients with VH and TRD did not undergo FA testing, making the preoperative assessment of intraocular ischemia inadequate. Because a larger ischemic area increases NVG risk, retinal ischemia should be evaluated with FA and optical coherence tomography angiography after surgery. Third, this study did not evaluate how the number of PRP laser shots influenced NVG risk. Before surgery, we did not assess the amount of photocoagulation due to preoperative VH. In the future, we should evaluate the amount of photocoagulation before vitrectomy to assess the risk factors for developing NVG after vitrectomy in eyes with PDR. Fourth, the follow-up period duration varied between subjects; it is likely that longer follow-up periods would result in more NVG cases. Fifth, we did not perform gonioscopy in all cases at the time when NVG occurred to assess the peripheral anterior synechia index. Spectral-domain anterior segment optical coherence tomography or gonioscopy enabling more accurate assessment of the peripheral anterior synechia index should be used in future studies. Sixth, the current study included patients with vitrectomy performed for both eyes. This influences the state, especially the systemic state such as fasting blood glucose, HbA1c, and eGFR. We need to utilize only data from one eye from each patient in the further study. Finally, the cause for performing a second surgery was not examined, but included postoperative retinal detachment and persistent VH. Therefore, future prospective studies with a set follow-up visit schedule are needed. These should include examination of postoperative retinal detachment (traction associated with regrowth or rhegmatogenous detachment with atrophic changes) and persistent VH (simple VH or VH associated with anterior vitreous fibril vascular proliferation) etiology.
Conclusion
The time between PDR surgery and NVG onset should also be evaluated in patients with elevated IOP, obvious iris/angle neovascularization, TRD, and/or diabetic maculopathy before and after surgery. The effects of fasting blood sugar and HbA1c discrepancies, glycemic variation, and hypoglycemia should also be evaluated in patients who undergo retinal tamponade during retinal surgery.
Acknowledgment
We would like to thank Chiaki Nishimura for statistical consultation and Editage Author Services for manuscript editing.
Author contributions
Design and conduct of the study: MS, IY. Data collection: MS, IY, RH, MU. Management, analysis, and interpretation of the data: MS, IY, TM. Preparation, review, or approval of the manuscript: MS, IY, RH, MU, TM. All authors contributed to data analysis, drafting and revising the article, gave final approval of the version to be published, and agree to be accountable for all aspects of the work.
Disclosure
The authors report no conflicts of interest in this work.
References
Aaberg TM, Van Horn DL. Late complications of pars plana vitreous surgery. Ophthalmology. 1978;85(2):126–140. | ||
Blankenship GW, Machemer R. Long-term diabetic vitrectomy results. Report of 10 year follow-up. Ophthalmology. 1985;92(4):503–506. | ||
Summanen P. Neovascular glaucoma following vitrectomy for diabetic eye disease. Acta Ophthalmol (Copenh). 1988;66(1):110–116. | ||
Oldendoerp J, Spitznas M. Factors influencing the results of vitreous surgery in diabetic retinopathy. I. Iris rubeosis and/or active neovascularization at the fundus. Graefes Arch Clin Exp Ophthalmol. 1989;227(1):1–8. | ||
Sima P, Zoran T. Long-term results of vitreous surgery for proliferative diabetic retinopathy. Doc Ophthalmol. 1994;87(3):223–232. | ||
Kumagai K, Furukawa M, Ogino N, Larson E, Iwaki M, Tachi N. Long-term follow-up of vitrectomy for diffuse nontractional diabetic macular edema. Retina. 2009;29(4):464–472. | ||
Goto A, Inatani M, Inoue T, et al. Frequency and risk factors for neovascular glaucoma after vitrectomy in eyes with proliferative diabetic retinopathy. J Glaucoma. 2013;22(7):572–576. | ||
Blankenship GW. The lens influence on diabetic vitrectomy results. Report of a prospective randomized study. Arch Ophthalmol. 1980;98(12):2196–2198. | ||
Rice TA, Michels RG, Rice EF. Vitrectomy for diabetic traction retinal detachment involving the macula. Am J Ophthalmol. 1983;95(1):22–33. | ||
Aaberg TM. Clinical results in vitrectomy for diabetic traction retinal detachment. Am J Ophthalmol. 1979;88(2):246–253. | ||
Every SG, Molteno AC, Bevin TH, Herbison P. Long-term results of Molteno implant insertion in cases of neovascular glaucoma. Arch Ophthalmol. 2006;124(3):355–360. | ||
Yazdani S, Hendi K, Pakravan M, Mahdavi M, Yaseri M. Intravitreal bevacizumab for neovascular glaucoma: a randomized controlled trial. J Glaucoma. 2009;18(8):632–637. | ||
Saito Y, Higashide T, Takeda H, Murotani E, Ohkubo S, Sugiyama K. Clinical factors related to recurrence of anterior segment neovascularization after treatment including intravitreal bevacizumab. Am J Ophthalmol. 2010;149(6):964–972.e1. | ||
Saito Y, Higashide T, Takeda H, Ohkubo S, Sugiyama K. Beneficial effects of preoperative intravitreal bevacizumab on trabeculectomy outcomes in neovascular glaucoma. Acta Ophthalmol. 2010;88(1):96–102. | ||
Scuderi JJ, Blumenkranz MS, Blankenship G. Regression of diabetic rubeosis iridis following successful surgical reattachment of the retina by vitrectomy. Retina. 1982;2(4):193–196. | ||
Wand M, Madigan JC, Gaudio AR, Sorokanich S. Neovascular glaucoma following pars plana vitrectomy for complications of diabetic retinopathy. Ophthalmic Surg. 1990;21(2):113–118. | ||
Wakabayashi Y, Usui Y, Okunuki Y, et al. Intraocular VEGF level as a risk factor for postoperative complications after vitrectomy for proliferative diabetic retinopathy. Invest Ophthalmol Vis Sci. 2012;53(10):6403–6410. | ||
Yoshida S, Kobayashi Y, Nakama T, et al. Increased expression of M-CSF and IL-13 in vitreous of patients with proliferative diabetic retinopathy: implications for M2 macrophage-involving fibrovascular membrane formation. Br J Ophthalmol. 2015;99(5):629–634. | ||
Yoshida S, Kubo Y, Kobayashi Y, et al. Increased vitreous concentrations of MCP-1 and IL-6 after vitrectomy in patients with proliferative diabetic retinopathy: possible association with postoperative macular oedema. Br J Ophthalmol. 2015;99(7):960–966. | ||
Tripathi RC, Li J, Tripathi BJ, Chalam KV, Adamis AP. Increased level of vascular endothelial growth factor in aqueous humor of patients with neovascular glaucoma. Ophthalmology. 1998;105(2):232–237. | ||
Kim YG, Hong S, Lee CS, et al. Level of vascular endothelial growth factor in aqueous humor and surgical results of Ahmed glaucoma valve implantation in patients with neovascular glaucoma. J Glaucoma. 2009;18(6):443–447. | ||
Kadonosono K, Matsumoto S, Uchio E, Sugita M, Akura J, Ohno S. Iris neovascularization after vitrectomy combined with phacoemulsification and intraocular lens implantation for proliferative diabetic retinopathy. Ophthalmic Surg Lasers. 2001;32(1):19–24. | ||
Hamanaka T, Akabane N, Yajima T, Takahashi T, Tanabe A. Retinal ischemia and angle neovascularization in proliferative diabetic retinopathy. Am J Ophthalmol. 2001;132(5):648–658. | ||
Azad R, Arora T, Sihota R, et al. Retcam fluorescein gonioangiography: a new modality for early detection of angle neovascularization in diabetic retinopathy. Retina. 2013;33(9):1902–1907. | ||
Fujikawa M, Sawada O, Kakinoki M, Sawada T, Kawamura H, Ohji M. Long-term intraocular pressure changes after vitrectomy for epiretinal membrane and macular hole. Graefes Arch Clin Exp Ophthalmol. 2014;252(3):389–393. | ||
Yamamoto K, Iwase T, Terasaki H. Long-term changes in intraocular pressure after vitrectomy for rhegmatogenous retinal detachment, epi-retinal membrane, or macular hole. PLoS One. 2016;11(11):e0167303. | ||
Matsuyama K, Ogata N, Jo N, Shima C, Matsuoka M, Matsumura M. Levels of vascular endothelial growth factor and pigment epithelium-derived factor in eyes before and after intravitreal injection of bevacizumab. Jpn J Ophthalmol. 2009;53(3):243–248. | ||
Jin P, Peng J, Zou H, et al. A five-year prospective study of diabetic retinopathy progression in Chinese type 2 diabetes patients with “well-controlled” blood glucose. PLoS One. 2015;10(4):e0123449. | ||
Lachin JM, Bebu I, Bergenstal RM, et al. Association of glycemic variability in type 1 diabetes with progression of microvascular outcomes in the diabetes control and complications trial. Diabetes Care. 2017;40(6):777–783. |
 © 2018 The Author(s). This work is published and licensed by Dove Medical Press Limited. The
full terms of this license are available at https://www.dovepress.com/terms
and incorporate the Creative Commons Attribution
- Non Commercial (unported, 3.0) License.
By accessing the work you hereby accept the Terms. Non-commercial uses of the work are permitted
without any further permission from Dove Medical Press Limited, provided the work is properly
attributed. For permission for commercial use of this work, please see paragraphs 4.2 and 5 of our Terms.
© 2018 The Author(s). This work is published and licensed by Dove Medical Press Limited. The
full terms of this license are available at https://www.dovepress.com/terms
and incorporate the Creative Commons Attribution
- Non Commercial (unported, 3.0) License.
By accessing the work you hereby accept the Terms. Non-commercial uses of the work are permitted
without any further permission from Dove Medical Press Limited, provided the work is properly
attributed. For permission for commercial use of this work, please see paragraphs 4.2 and 5 of our Terms.