Back to Journals » Research and Reports in Urology » Volume 12
Risk Factors for Anastomosis Leakage After Kidney Transplantation
Authors Jenjitranant P ![]() , Tansakul P
, Tansakul P ![]() , Sirisreetreerux P
, Sirisreetreerux P ![]() , Leenanupunth C, Jirasiritham S
, Leenanupunth C, Jirasiritham S
Received 23 July 2020
Accepted for publication 17 September 2020
Published 28 October 2020 Volume 2020:12 Pages 509—516
DOI https://doi.org/10.2147/RRU.S272899
Checked for plagiarism Yes
Review by Single anonymous peer review
Peer reviewer comments 3
Editor who approved publication: Dr Jan Colli
Pocharapong Jenjitranant,1 Pasu Tansakul,1 Pokket Sirisreetreerux,1 Charoen Leenanupunth,1 Sopon Jirasiritham2
1Division of Urology, Department of Surgery, Faculty of Medicine Ramathibodi Hospital, Mahidol University, Bangkok, Thailand; 2Division of Vascular and Transplant Surgery, Department of Surgery, Faculty of Medicine Ramathibodi Hospital, Mahidol University, Bangkok, Thailand
Correspondence: Pokket Sirisreetreerux
Division of Urology, Department of Surgery, Faculty of Medicine Ramathibodi Hospital, Mahidol University, 270 Rama VI Road, Thung Phaya Thai, Ratchathewi, Bangkok 10400, Thailand
Tel +66 2 2011315 ext.335
Email [email protected]
Purpose: Kidney transplantation is one of the best treatment options for end-stage renal disease with an incidence of urologic complications of 2.5 to 30%. One of the most serious and frequent urological complications is urinary leakage from ureteroneocystostomy anastomosis. The purpose of this study was to evaluate risk factors of urinary leakage from ureteroneocystostomy anastomosis after kidney transplantation.
Patients and Methods: A retrospective study was performed on patients who received kidney transplantation and were diagnosed with urinary leakage thereafter based on renal scan or drain creatinine per serum creatinine compared with patients in control group. Risk factor assessment was based on inpatient and outpatient information from hospital database.
Results: From 459 patients who received kidney transplantation in 2016– 2018, there were 20 patients who were diagnosed with urinary leakage after they underwent ureteroneocystostomy anastomosis. The significant risk factors for anastomosis leakage were size of suture materials and duration of ureteral stent insertion. No statistically significant difference in other factors such as underlying disease, surgical technique or duration of urinary catheter was found. About overall urological complication, gender and body mass index significantly affected the outcome.
Conclusion: The rate of urinary leakage complications was found to be about 4.36%. The risk factors of overall complication comprised gender and body mass index. Although a lot of previous studies revealed many risk factors that could affect urinary leakage, size of suture materials and duration of ureteral stent insertion were the significant risk factors in our study. Proper consideration should be given to the size of suture materials and optimal duration of ureteral stent.
Keywords: anastomotic leak, kidney transplantation, postoperative complications, risk factors
Introduction
Kidney transplantation is one of the best treatment options for end-stage renal disease. Although kidney transplantation increases the quality of life for patients, postoperative complications such as urinary tract infection (UTI), hypovolemia requiring blood transfusion or delayed graft function can occur.1 The overall incidence of urologic complications from various literature ranged from 2.5 to 30%.2–4 These urologic complications could lead to graft rejection, serious morbidity, and even death.2,5,6 The most common adverse events following kidney transplantation are urologic complications.5 One of the most serious and frequent urological complications is urinary leakage from ureteroneocystostomy anastomosis. The incidence of urinary leakage reported from various literature ranged from 1.2 to 8.9%.7–9 Our hospital is a tertiary level medical center that has the largest number of kidney transplantation patients in the country. There were 2158 patients who underwent kidney transplantation between 1986 and 2017. The incidence of urinary leakage in our hospital was about 4%. From a previous study, there were several reports that risk factors of urological complications were gender, race, and surgical technique.2 Our study focused on finding the risk factors of urinary leakage after ureteroneocystostomy anastomosis. The findings may guide the way to minimize this particular complication.
Patients and Methods
This study was ethically approved by Committee on Human Rights related to Research involving Human Subjects, Faculty of Medicine Ramathibodi hospital (No. MURA2017/249). According to the Ethical committee consensus, patient consent to review their medical records was not required because of the retrospective nature of the data collection. The patient data were kept confidentially and the study complied with the Declaration of Helsinki. The electronic medical records were retrospectively reviewed from January 2016 to December 2018. End-stage renal disease patients who underwent kidney transplantation for both living related kidney transplantation (LRKT) and deceased donor kidney transplantation (DDKT) were included in the study. Expanded criteria donor (ECD) was classified according to Port et al, including all donors equal to or older than the age of 60, plus those donors aged 50 and 59 years with at least two of the following three factors: serum creatinine greater than 1.5 mg/dL, cause of death from cerebrovascular accident, and history of hypertension. All organs were donated voluntarily with written informed consent, and the organ donations were conducted in accordance with the Declaration of Istanbul. Baseline characteristics of the patients were collected. Risk factors that were possible predictors of urinary complications were reviewed including era of transplant, sex, age, race, comorbidities, etiology of renal failure, donor characteristics, urine per day before transplantation, ureteroneocystostomy technique, operative time, surgeon, rejection and ischemia times, post-operative complication, serum creatinine urine after surgery, and length of hospital stay.
Ureteroneocystostomy anastomosis leakage was diagnosed by positive renal scan or creatinine from drain per serum creatinine ratio of more than 2.3,10,11 The information of patients who had been diagnosed with urinary leakage was recorded. The treatment information consisted of complication during post-operative period, conservative or intervention treatment, surgical technique, length of hospital stay, and result after treatment.
The two-tailed Mann–Whitney–Wilcoxon test for two independent samples, the χ2 test, and simple regressions with the Spearman rank correlation coefficient were used for analysis. The results were given either as median range or standard deviation. Statistical significance was defined as a P value of <0.05. The association between baseline characteristics, perioperative factors and postoperative complication was assessed by univariable and multivariable logistic regression, fitted to analyze the risk factors of urinary leakage. All analyses were performed using STATA® version 16.0 (StataCorp LP, College Station, TX, USA).
Results
From January 2016 to December 2018, 459 end-stage renal disease patients underwent kidney transplantation in Ramathibodi Hospital. The baseline characteristics of the study population (459 consecutive kidney transplant recipients) are detailed in Table 1. From 459 patients, 59.69% is male and 40.31% is femaleswhich showed no significant difference. Mean ±SD age in leakage group was 40.10±12.04 years and non-leakage group was 42.95±12.77 years. BMI was 22.34 in non-leakage whereas 22.48 in leakage group. There were no significant differences in age and BMI between the two groups. Underlying, cause of ESRD, type of renal replacement therapy and urine volume per day were not significantly different in both groups. There were 72 patients from 200 living donors who underwent open surgery and 128 patients who underwent laparoscopic surgery. However, there was no statistically significant difference between the two groups.
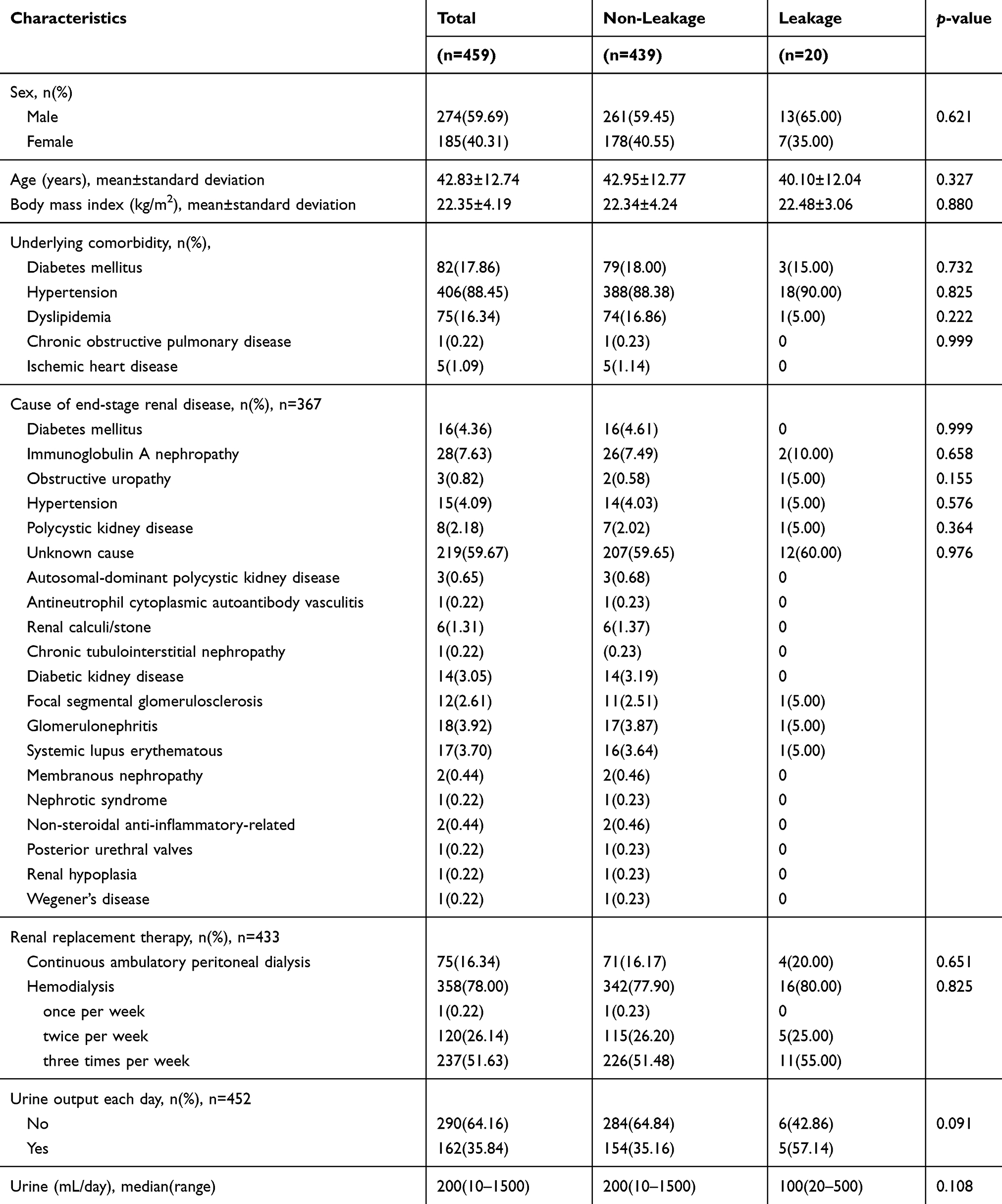 |
Table 1 Patients’ Baseline Characteristics |
Among 459 patients, 200 patients were living donors, 246 patients received transplanted kidney from deceased donors with standard criteria, and 13 patients from deceased donors with expanded criteria. The detail of patients’ perioperative factors were shown in Table 2. Median cold ischemic time (range) for the leakage group was 1103 (11–1812) which was statistically significantly longer than the non-leakage group. There were 20 patients who had ureteroneocystostomy anastomosis leakage diagnosed by either renal scan or positive drain creatinine per serum creatinine ratio. Median (IQR) time to urine leakage was 16 (7-396) days. Massive amount of fluid from the drain was the most common presentation. One patient died after KT because of severe sepsis. According to the treatment for leakage, 6 patients were successfully treated with Foley catheter insertion. Whereas, 14 patients underwent operative treatment including 8 patients with ureteroneocystostomy, 2 patients with ureteroureterostomy with native ureter and 2 patients underwent nephrectomy (Table 3). For the transplanted kidney function in the patients with anastomosis leakage, the mean follow-up time was 34.47 months (SD 13.36). Excluding 2 patients who underwent nephrectomy of transplanted kidney, 10 out of 18 patients (56%) had GFR less than 60 mL/min. Out of the anastomosis leakage patients who had LRKT, 2 out of 6 patients (33%) developed chronic kidney disease stage 3 or more with GFR less than 60 mL/min.
 |
Table 2 Comparison of Patients’ Perioperative Factors Between the Non-Leakage and Leakage Groups |
 |
Table 3 Clinical Presentation, Treatment, and Outcomes of Urinary Leakage |
Regarding the factors that were associated with urinary leakage complication, suture material size and duration of DJ stent statistically significantly affected the anastomosis leakage. The mean cold ischemic time in the urinary leakage group was 1103 minutes, compared with 789 minutes in the non-leakage group (p-value 0.024). Cold ischemic time was statistically significantly different between two groups of patients in univariate analysis, however there was not significance in multivariate analysis (Table 4). Table 5 showed odds ratio from univariate and multivariate analyses for the risk of overall urological complications. Female gender and BMI significantly increased the complication with the ORs of 3.592 (95% CI 2.35–5.48, p<0.01) and 1.073 (95% CI 1.02–1.13, p=0.006) as shown in Table 5.
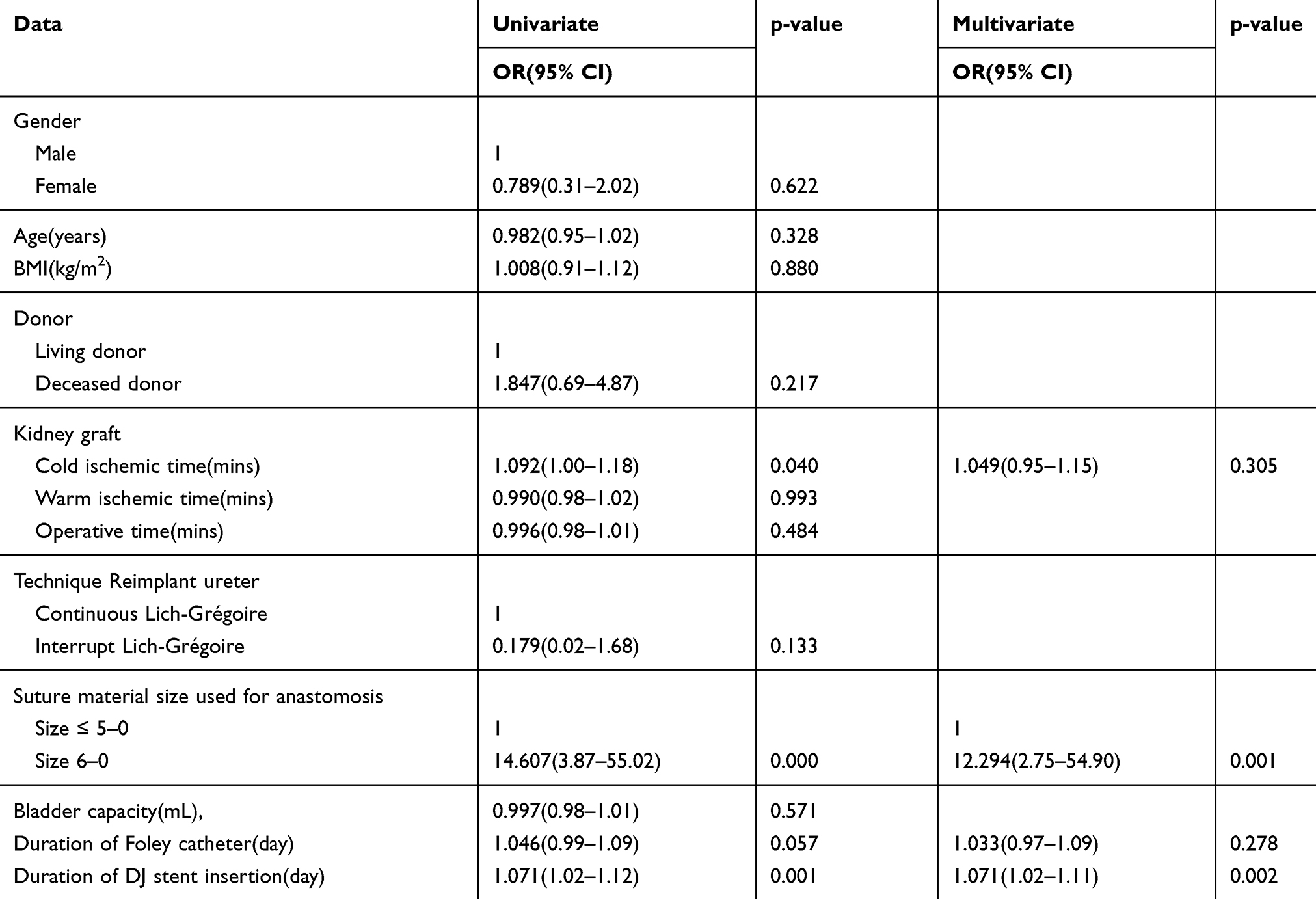 |
Table 4 Univariate and Multivariate Analyses for the Risk Factors for Urinary Leakage Complications |
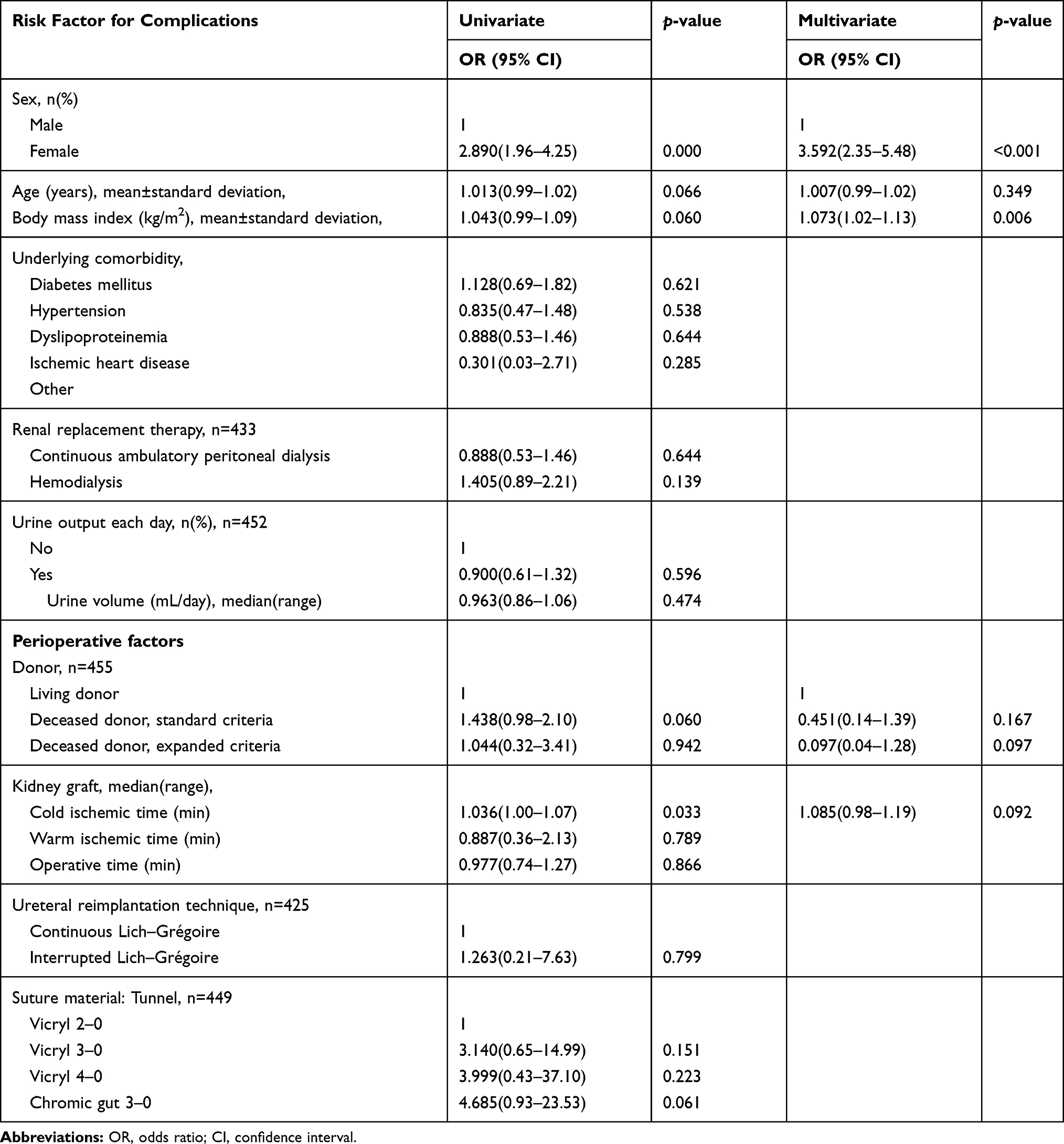 |
Table 5 Univariate and Multivariate Analyses for the Risk Factors of Overall Urological Complications |
Discussion
The incidence of early and late urological complications with kidney transplantation was reported varying between 1.2 and 8.9%.7,12 At Ramathibodi Hospital, the incidence of urinary leakage during three years of study was 4.3%, which is not different from other studies. From our report, it was found that the most common initial symptom was massive amount of fluid from the drain, but there were 4 people who presented with UTI and fluid collection that was detected from ultrasound. Therefore, we should always consider that the symptoms of urinary leakage may present in many ways. This information from this study will be useful for early detection of urinary leakage complication after kidney transplantation. Like many centers, we now use laparoscopic donor nephrectomy to procure approximately 95% of living donor kidneys. Contrary to other published reports, laparoscopic donor nephrectomy was not associated with more urinary complications.13–15 Moreover, laparoscopic donor nephrectomy may have fewer complications compared with open living donor nephrectomy. This finding could be related to meticulous attention given to preserve periureteral tissue. Another reason is that laparoscopic surgery is still a minimally invasive surgery that can reduce pain and length of hospital stay for living donor.
According to the previous studies, the risk factors affecting urinary complications are sex, race, and the U-stitch anastomotic technique.10,16 Whereas, our study found that size of suture materials and duration of DJ stent insertion significantly affect the risk of anastomosis leakage complication according to multivariate analysis. About the DJ stent duration, Visser et al reported the systematic review and meta-analysis about the timing of ureteric stent removal and the occurrence of urological complications. They concluded that earlier stent removal of less than 3 weeks after KT was associated with decreasing the UTIs but did not increase the incidence of urinary leakage compared to later removal of more than 3 weeks. As a result, they recommended the routine removal of ureteric stents around 3 weeks post-operatively.17 This finding corresponded to the result from Yuksel et al that recommended the optimal time for stent removal of 14 to 21 days after KT.18 About the size of suture materials, we hypothesized that using the small size suture material along with interrupted suturing technique may cause the gap between the stitch if there is too much distance between each stitch, resulting in inadequate tissue healing, so anastomosis leakage occurs. In addition, it is worth noting that the duration of urinary catheterization did not significantly affect the rate of complications in both previous studies and our study. Therefore, it may be useful regarding the decision of when to remove the urinary catheter. These findings will be beneficial to be better aware and inform the patients about the risks of postoperative complications and to aid the surgeons in making decisions about management.
Our study was designed as a retrospective, single center cohort analysis. There were some limitations in this study. Firstly, there were some risk factors that could not be assessed due to the retrospective nature but which may significantly affect the risk of urinary leakage complication such as periureteral tissue, length of ureter, etcetera. In addition, the mediation of their effects may be complex, unexplored interactions among the factors may exist and additional confounders may remain unmeasured and uncharacterized.
Conclusion
The rate of urinary leakage complications was found to be about 4.36% in Ramathibodi Hospital. The risk factors of overall complication comprised gender and body mass index. Although a lot of previous studies revealed many risk factors that could affect risk of urinary leakage, size of suture materials and duration of ureteral stent insertion were the significant risk factors in our study. Proper consideration should be given regarding the size of suture materials and optimal duration of ureteral stent.
Disclosure
The authors report no conflicts of interest in this work.
References
1. Rezapour S, Yarmohammadi A, Tavakkoli M. One-year survival rate of renal transplant: factors influencing the outcome. Transplant Res Risk Management. 2017;9:49–56. doi:10.2147/TRRM.S150080
2. Englesbe MJ, Dubay DA, Gillespie BW, et al. Risk factors for urinary complications after renal transplantation. Am J Transplant. 2007;7(6):1536–1541. doi:10.1111/j.1600-6143.2007.01790.x
3. Streeter EH, Little DM, Cranston DW, Morris PJ. The urological complications of renal transplantation: a series of 1535 patients. BJU Int. 2002;90(7):627–634. doi:10.1046/j.1464-410X.2002.03004.x
4. Zavos G, Pappas P, Karatzas T, et al. Urological complications: analysis and management of 1525 consecutive renal transplantations. Transplant Proc. 2008;40(5):1386–1390. doi:10.1016/j.transproceed.2008.03.103
5. Kayler L, Kang D, Molmenti E, Howard R. Kidney transplant ureteroneocystostomy techniques and complications: review of the literature. Transplant Proc. 2010;42(5):1413–1420. doi:10.1016/j.transproceed.2010.04.016
6. Tavakoli A, Surange RS, Pearson RC, Parrott NR, Augustine T, Riad HN. Impact of stents on urological complications and health care expenditure in renal transplant recipients: results of a prospective, randomized clinical trial. J Urol. 2007;177(6):2260–2264. doi:10.1016/j.juro.2007.01.152
7. Choi YS, Kim KS, Choi SW, et al. Ureteral Complications in Kidney Transplantation: analysis and Management of 853 Consecutive Laparoscopic Living-Donor Nephrectomies in a Single Center. Transplant Proc. 2016;48(8):2684–2688. doi:10.1016/j.transproceed.2016.06.054
8. Shoskes DA, Hanbury D, Cranston D, Morris PJ. Urological complications in 1000 consecutive renal transplant recipients. J Urol. 1995;153(1):18–21. doi:10.1097/00005392-199501000-00008
9. Nie Z-L, Zhang K-Q, Li Q-S, Jin F-S, Zhu F-Q, Huo W-Q. Treatment of urinary fistula after kidney transplantation. Transplant Proc. 2009;41(5):1624–1626. doi:10.1016/j.transproceed.2008.10.103
10. Baston C, Harza M, Preda A, et al. Comparative urologic complications of ureteroneocystostomy in kidney transplantation: transvesical Leadbetter-Politano versus extravesical Lich-Gregoir technique. Transplant Proc. 2014;46(1):176–179. doi:10.1016/j.transproceed.2013.12.003
11. Flores-Gama F, Bochicchio-Riccardelli T, Mondragón-Ramírez G. [Determination of creatinine in drained liquid. Urinary leak or lymphocele?]. Cirugia Ycirujanos. 2010;78(4):327–332.
12. Duty BD, Barry JM. Diagnosis and management of ureteral complications following renal transplantation. Asian J Urol. 2015;2(4):202–207. doi:10.1016/j.ajur.2015.08.002
13. Philosophe B, Kuo PC, Schweitzer EJ, et al. Laparoscopic versus open donor nephrectomy: comparing ureteral complications in the recipients and improving the laparoscopic technique. Transplantation. 1999;68(4):497–502. doi:10.1097/00007890-199908270-00009
14. Nogueira JM, Cangro CB, Fink JC, et al. A comparison of recipient renal outcomes with laparoscopic versus open live donor nephrectomy. Transplantation. 1999;67(5):722–728. doi:10.1097/00007890-199903150-00014
15. Kuo PC, Cho ES, Flowers JL, Jacobs S, Bartlett ST, Johnson LB. Laparoscopic living donor nephrectomy and multiple renal arteries. Am J Surg. 1998;176(6):559–563. doi:10.1016/S0002-9610(98)00260-8
16. Szabo-Pap M, Zadori G, Fedor R, et al. Surgical Complications Following Kidney Transplantations: A Single-Center Study in Hungary. Transplant Proc. 2016;48(7):2548–2551. doi:10.1016/j.transproceed.2016.07.012
17. Visser IJ, van der Staaij JPT, Muthusamy A, Willicombe M, Lafranca JA, Dor F. Timing of Ureteric Stent Removal and Occurrence of Urological Complications after Kidney Transplantation: A Systematic Review and Meta-Analysis. J Clin Med. 2019;8:5. doi:10.3390/jcm8050689
18. Yuksel Y, Tekin S, Yuksel D, et al. Optimal Timing for Removal of the Double-J Stent After Kidney Transplantation. Transplant Proc. 2017;49(3):523–527. doi:10.1016/j.transproceed.2017.01.008
 © 2020 The Author(s). This work is published and licensed by Dove Medical Press Limited. The
full terms of this license are available at https://www.dovepress.com/terms
and incorporate the Creative Commons Attribution
- Non Commercial (unported, 3.0) License.
By accessing the work you hereby accept the Terms. Non-commercial uses of the work are permitted
without any further permission from Dove Medical Press Limited, provided the work is properly
attributed. For permission for commercial use of this work, please see paragraphs 4.2 and 5 of our Terms.
© 2020 The Author(s). This work is published and licensed by Dove Medical Press Limited. The
full terms of this license are available at https://www.dovepress.com/terms
and incorporate the Creative Commons Attribution
- Non Commercial (unported, 3.0) License.
By accessing the work you hereby accept the Terms. Non-commercial uses of the work are permitted
without any further permission from Dove Medical Press Limited, provided the work is properly
attributed. For permission for commercial use of this work, please see paragraphs 4.2 and 5 of our Terms.