Back to Journals » International Journal of Women's Health » Volume 13
Risk Factors Associated with Preterm Delivery in Singleton Pregnancy in a Tertiary Care Hospital in South India: A Case Control Study
Authors Sureshbabu RP, Aramthottil P, Anil N, Sumathy S ![]() , Varughese SA, Sreedevi A, Sukumaran SV
, Varughese SA, Sreedevi A, Sukumaran SV
Received 21 December 2020
Accepted for publication 9 March 2021
Published 9 April 2021 Volume 2021:13 Pages 369—377
DOI https://doi.org/10.2147/IJWH.S282251
Checked for plagiarism Yes
Review by Single anonymous peer review
Peer reviewer comments 2
Editor who approved publication: Dr Everett Magann
Raveena Pallithazath Sureshbabu,1 Parvathi Aramthottil,1 Neelanjana Anil,1 Sudha Sumathy,2 Steffi Ann Varughese,1 Aswathy Sreedevi,1 Sheejamol Velickakathu Sukumaran3
1Department of Community Medicine, Amrita Institute of Medical Sciences and Research Centre, Amrita Vishwa Vidyapeetham, Kochi, 682041, Kerala, India; 2Department of Obstetrics and Gynaecology, Amrita Institute of Medical Science, Amrita Vishwa Vidyapeetham, Kochi, 682041, Kerala, India; 3Department of Biostatistics, Amrita Institute of Medical Sciences and Research Centre, Amrita Vishwa Vidyapeetham, Kochi, 682041, Kerala, India
Correspondence: Aswathy Sreedevi
Department of Community Medicine, Amrita Institute of Medical Sciences and Research Centre, Amrita Vishwa Vidyapeetham, Kochi, Kerala, India
Tel +91-9447294260
Email [email protected]
Background: Preterm delivery is a major obstetric complication and a leading cause of neonatal mortality and morbidity. It is also associated with significant costs in terms of psychological and financial hardship, to the families.
Objective: The primary objective of this study was to determine the risk factors associated with all preterm deliveries in singleton pregnancy in a tertiary care hospital and the secondary objective was to determine the fetal outcomes among women with preterm delivery.
Materials and Methods: A case control study was conducted between January 2019 and June 2019 in the Department of Obstetrics and Gynecology of a tertiary care center in Central Kerala, India. Women who delivered before 37 completed weeks of gestation were taken as cases and those who delivered at or after 37 weeks were considered as controls in a 1:1 ratio, approximately. Data regarding 191 cases and 200 controls were taken from delivery room records of the years 2016 to 2018 with the help of a predesigned checklist. Univariate and multivariate analysis were done to determine the magnitude of association between the exposure factors and preterm delivery.
Results: The mean age of study participants among the cases was 29.3 ± 5.1 years and controls was 28.1 ± 4.4. Pregnancy induced hypertension (aOR = 14.60; 95% CI 4.8, 44.1; p< 0.001), abnormal amniotic fluid volume (aOR = 10.68; 95% CI 3.46, 32.98; p< 0.001), premature rupture of membranes (PROM) (aOR = 10.27; 95% CI 4.82, 21.86; p< 0.001), previous history of preterm delivery (aOR = 4.12; 95% CI 1.22, 13.85; p< 0.002), history of urinary tract infection (UTI) during pregnancy (aOR = 3.67; 95% CI 1.39, 9.68; p< 0.002), systemic diseases (aOR = 2.78; 95% CI 1.28, 6.39; p< 0.001), anaemia (aOR = 2.54; 95% CI 1.28, 5.03; p< 0.004) were found to be the independent risk factors for preterm delivery. On analyzing the fetal outcomes, the average birth weight of preterm babies was 2 ± 0.6 kg compared to 3.1kg among term babies.
Conclusion: Early detection and adequate treatment of various conditions like anaemia, pregnancy induced hypertension, UTI and systemic illness can help in reduction of the prevalence of preterm delivery.
Keywords: preterm birth, risk factors, case control study, singleton pregnancy
Introduction
Preterm delivery is defined as any birth before 37 completed weeks of gestation, ie, 259 days since the first day of a woman’s last menstrual period (LMP).1 In India, the preterm deliveries constitute 23.6%2 of the world’s total. Preterm delivery is a major obstetric emergency and also a threat to population health. In developed countries such as the UK, preterm birth occurs in 7% to 11% of pregnancies and is responsible for 85% of neonatal deaths in normally formed infants without any congenital abnormalities.3
Preterm birth complications are also the leading cause of death among children under 5 years of age, responsible for approximately 1 million deaths in 2015.1 Compared to children born at term, preterm babies have increased risk of developing disabilities like neurodevelopmental impairment, cerebral palsy, learning disabilities, and respiratory illness.4 The economic and social costs of preterm birth is high. Most cases require neonatal intensive care and other advanced treatments, which are resource intensive.5 The consequences of preterm birth extend beyond the newborn period into infancy, adolescence and adulthood with enormous impact.6 There is evidence that premature children have a higher risk of respiratory illnesses with lower achieved lung growth and increased risk of type 2 diabetes, hypertension, and other chronic diseases earlier in adulthood than those born at term.7
Preterm births can be classified as spontaneous (due to spontaneous preterm labour or preterm prelabour rupture of membranes) or provider-initiated (caesarean or labour induction, for a maternal or foetal indication).6 Though the pathogenesis of preterm labour is not well understood, it probably represents early idiopathic activation of the normal labour process or the results of pathological insults. Preterm labour is now thought to be a syndrome initiated by multiple mechanisms, including infection or inflammation, uteroplacental ischaemia or haemorrhage, uterine overdistension, stress, and other immunologically mediated processes.8
The aetiology is multifactorial and therefore all preterm births have been taken into consideration. Studies show that education of the mother, age of 36 and above, history of preterm delivery, multiparity, maternal hypertension, diabetes, oligohydramnios, polyhydramnios, placenta previa, history of organic disorder (cardiac, renal, thyroid) and blood group A have significant correlation with recurrence of premature labour.6,9 In addition, factors such as urinary tract infections (UTI), and diabetes were reported as risk factors.10 Further, the poor mental health of mothers such as anxiety and depression has been associated with preterm birth consistently.11–13
The southern state of Kerala in India has shown a downward trend of neonatal mortality, infant mortality and maternal mortality rates, at 6 per 1000 live births, 7 per 1000 live births and 43 per 100,000 live births, respectively.14 The decline of infant mortality rates has shifted the focus now to perinatal mortality rates which is a good indicator of the quality of care for both mother and child.
Though significant advances have been made in the management of preterm delivery and related complications, focus on preventable factors have been lacking.
Therefore, identifying the risk factors associated with preterm delivery is important as this can help in early and appropriate risk-specific management. Therefore, this study intends to determine the risk factors associated with preterm delivery in a tertiary care hospital in Kerala.
Materials and Methods
This case control study was done by reviewing labour room records of women who delivered within a period of 3 years from 2016–2018, in the Department of Obstetrics and Gynecology of Amrita Institute of Medical Sciences, a tertiary care centre in Kochi, Kerala, India. The study was done with the help of a predesigned checklist created on the basis of a literature review search and finalized after discussion with experts. The study was conducted over 6 months, between January to June of 2019. Cases were defined as all singleton pregnancies who delivered before 37 completed weeks of gestation in the period between January 2016 to December 2018 and controls were defined as all deliveries at or after 37 weeks of gestation in the same period. All preterm deliveries including those for medical indications were considered.
Cases of terminated pregnancies before 22 weeks of gestation (miscarriage), still birth after 22 weeks of gestation, multiple births and intrauterine death expulsion were excluded.
Permission was obtained from the hospital administration. The hospital administration provided data after removing all personal identifiers. Ethical approval for the study was obtained from the Institutional Research Ethics Committee (IRB-AIMS-2019-267 dated November 10, 2019) of the Amrita Institute of Medical Sciences and Research Centre. As it was a record based study the informed consent from persons was waived. The study was in compliance with the Declaration of Helsinki. Following are some definitions which have been applied in the diagnosis of exposure variables in this study.
Based on the study conducted by Rao19 et al titled “A case control study on risk factors of preterm deliveries in a secondary care hospital, South India” the prevalence of cases exposed to gestational hypertension was found to be 21.4% and controls 7.8%; OR = 3.23; with 80% power at 95% confidence. Considering the common risk factors of gestational hypertension and PROM the minimum sample size varied from 106–130 in each arm. We rounded it to 200 controls and 191 cases in a ratio of approximately 1:1.
Data Collection and Variable Definition
Data for the same was obtained from labour room records and details regarding the probable risk factors of the participants who had a preterm delivery from the years 2016–2018 such as maternal age, belonging to an urban or rural area, parity index, infertility, history of abortion, pregnancy induced hypertension, gestational diabetes mellitus, hypothyroidism, anaemia, history of preterm delivery, location of placenta, premature rupture of membranes, amniotic fluid volume, history of UTI during pregnancy, history of any other infections during pregnancy and history of other medical conditions were abstracted from the records with the aid of the pre-designed checklist. Categorization to urban/rural area was based on local address of study participants belonging to Panchayats and Municipalities/Corporations. Other details regarding the fetal birth weight, fetal presentation, NICU admission and other comorbidities of the fetus were also collected from the records. From the identified cases and controls 20 in the cases and 15 in the controls were rejected due to incomplete data such as the absence of address, incorrect hospital number, etc.
Statistical Analysis
Data was entered into MS Excel software and statistical analysis was carried out with the help of SPSS software, version 20. Using the Chi-square test the distribution of socio-demographic, maternal, medical and reproductive histories according to preterm delivery status were examined. Frequencies, means, and proportions of variables were computed. Stepwise multivariate logistic regression analysis was used to predict the independent risk factors of premature birth. Predictors at a p value <0.2 in a bivariate analysis were included in the multivariate logistic regression model. The Nagaelker R2 was 0.453. The fit was checked with the Hosmer Lemeshow test. A P value of 0.794 shows that the given model fits the data well. Multicollinearity was checked by collinearity statistics such as tolerance and variance inflation factor. Quantitative variables such as age were compared with independent sample t test.
Results
The mean age of cases 29.27 ± 5.08 was significantly higher than that of the controls at 28.05 ± 4.38, (not in table). Among all the cases, 114 (59.7%) were multiparous compared to 111 (55.5%) among the controls and this difference was not significant.
Among the 191 cases, univariate analysis showed factors like pregnancy induced hypertension (PIH) (OR = 11.77; p<0.001), abnormal amniotic fluid volume (OR = 10.99; p<0.001), premature rupture of membranes (OR = 5.76; p<0.001), previous history of preterm labour (OR = 4.78; p = 0.003), presence of other systemic diseases such as bronchial asthma, chronic hypertension, cardiac abnormality and overt diabetes (OR = 4.41; p<0.001,) urinary tract infection (UTI) (OR = 3.77; p = 0.002), anaemia (OR = 2.30; p = 0.004), and gestational diabetes mellitus (OR = 1.88; p = 0.039) to be significantly associated risk factors. Factors like place of residence, parity index, history of infertility, abortion, hypothyroidism, position of placenta, vaginal infections and any other infections during pregnancy were statistically non-significant (Table 1).
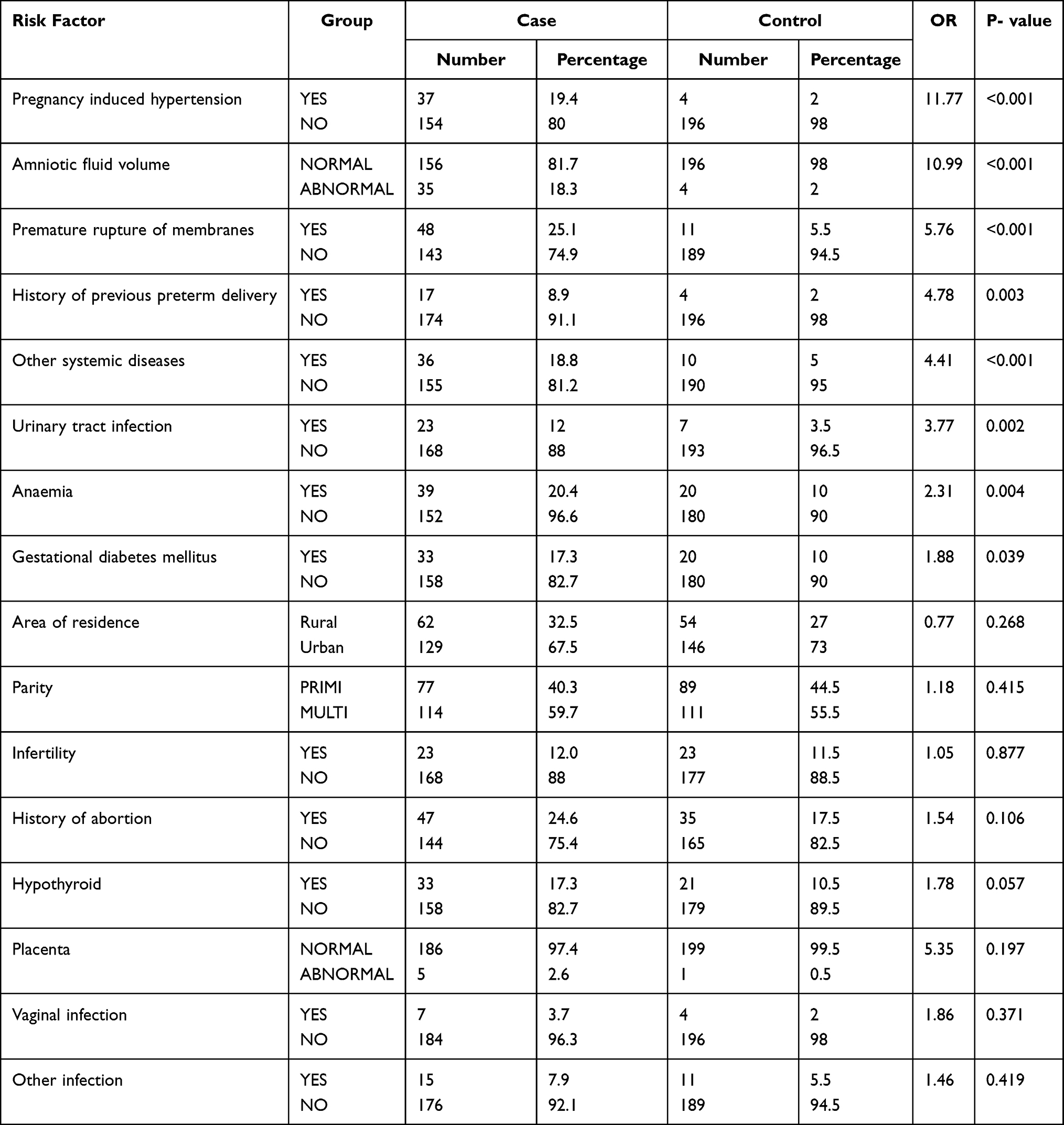 |
Table 1 Association of Risk Factors of Preterm Birth |
After multivariate regression analysis PIH, amniotic fluid volume, premature rupture of membranes, history of previous preterm delivery, UTI, anaemia, other systemic illness such as bronchial asthma, cardiac abnormalities, gestational diabetes mellites, chronic hypertension were found to be independently associated with premature labour (Table 2).
 |
Table 2 Independent Risk Factors of Preterm Birth |
About a fifth (19.4%) of the cases had PIH compared to 2% among the controls. After multivariate regression, women suffering from PIH, had 14.6 times higher risk of having preterm delivery than women who did not have PIH (aOR = 14.61; 95% CI 4.8, 44.1; p<0.001) which is why it is also a medical indication for intervention.
Women with extremes of amniotic fluid volume, oligo and polyhydramnios were found to have 11 times more risk of preterm delivery than women with normal amniotic fluid volume (aOR = 10.99; 95% CI 3.45, 32.97; p<0.001). The crude odds of women with premature rupture of membrane having a preterm delivery was 5.76 which doubled to 10.26 (95% CI 4.82, 21.85; p<0.001) after multivariate regression. It was found that in women with a previous history of preterm delivery there is 4 times more risk of having preterm delivery than women who did not have previous history (aOR = 4.11; 95% CI 1.22, 13.85; p=0.002). The proportion of UTI among cases was four times more among cases at 12% compared to 3.5% in controls. After regression the adjusted odds was 3.67 (95% CI 1.39, 9.68; p=0.002).
Systemic diseases such as overt diabetes mellitus, chronic hypertension, bronchial asthma and cardiac abnormalities were documented in the records of 18.8% of cases compared to 5% of controls with a crude odds of 4.4 (p<0.001). After regression, systemic diseases continued to be an independent risk factor albeit with a reduced odds of 2.78 (95% CI 1.28, 6.39; p<0.001). A very treatable and preventable condition such as anaemia was also found to be an independent predictor increasing the risk of preterm deliveries by 2.5 times (OR = 2.54; 95% CI 1.28, 5.02; p=0.004) (Table 2). Among all the independent risk factors, PIH and other systemic diseases are medically manageable by adequate treatment at the proper time. Anaemia is eminently preventable and so is UTI by adequate intake of iron supplements, iron rich food and fluid respectively during the antenatal period.
The fit was checked using the Hosmer Lemeshow test. A p value of 0.794 shows that the given model fits the data well. Multicollinearity was also checked with collinearity statistics. All the predictors tolerance value were close to 1 and VIF<2.5 shows the absence of collinearity (Table 3).
 |
Table 3 Collinearity Statistics |
Fetal Outcomes
The average birth weight of preterm babies was significantly lower at 2.1kg ± 0.6, compared to 3kg ± 0.4 (p<0.01) among the term babies. The fetal outcomes were also poor in the preterm group with 4 (2.1%) deaths compared to none in the control group. Among 191 preterm babies, 30 (15.7%) were in breech position, while among the 200 term babies only 4 (2%) babies were breech deliveries. More than a half (51.8%) of the preterm babies required neonatal intensive care unit (NICU) admission, while only 14 (7%) of term babies had NICU admission. About 9 (4.7%) preterm babies had intrauterine growth retardation (IUGR), whereas only 6 (3%) term babies had IUGR. Among the preterm babies, 13 (6.8%) had a cardiac abnormality, 5 (2.5%) had renal abnormalities and 5 (2.5%) had respiratory distress.
Discussion
Our study was done with the purpose of finding out the risk factors associated with preterm labour in a state with low neonatal mortality rate and good indices of maternal and child health care. The current study shows that pregnancy induced hypertension (PIH), abnormal amniotic fluid volume, premature rupture of membranes, a history of previous preterm delivery, a history of urinary tract infections during pregnancy, systemic illness like bronchial asthma, cardiac abnormalities, anaemia, overt diabetes mellitus and chronic hypertension are independent risk factors for preterm labour. Though the precise mechanism of preterm birth is not known in many cases, the factors associated with preterm birth but not in the causal pathway can be used to explain preterm birth.5
In the present study the mean maternal age is 29±5.08 yrs which is comparable with a study in central Kerala20 where 42.6% of the women with preterm delivery were in the 26 to 30 years age group and in the north Indian state of Punjab where the mean age was 24.67±4.08 years.21
About 12% (aOR: 3.67; 95% CI 1.3, 9.6) of the women with preterm delivery had UTI, which was comparable to that in the northern Indian state of Punjab at 13%.22 However, some studies in Kerala and Haryana have reported UTI at double the proportion at 30% to 34%.20,23 The spontaneous preterm births are largely due to PPROM and in a hospital-based study in Uttar Pradesh24 39% of the patients with PPROM were found to have a UTI infection. UTI when diagnosed early and treated adequately can prevent preterm delivery. Preventive habits such as adequate fluid intake and maintaining personal hygiene should also be an essential part of the antenatal advice.
Premature rupture of membranes is a common risk factor for preterm delivery. In our study 25.1% of the cases had premature membrane rupture, which is comparable with the other studies where it varied between a fourth to a fifth.22,25 Special attention and conservative management of women with risk factors of premature rupture of membranes like history of abortion, previous PROM can also be beneficial.
PIH was the commonest obstetric risk factor in the study in Karnataka19 with more than a fifth, 21.4% of the women with preterm delivery having PIH. In our study also PIH occurred among a fifth of the women (19.4%) with preterm labour, in concordance with the previous studies.19,24 In a study from Bangalore hypertensive disorders were the commonest risk factor at 32.9% whereas in Uttar Pradesh it was much lower at (18.6%) corresponding to the lower levels of hypertension in the community.23,24 Early detection and adequate treatment of pregnancy induced hypertension is critical as those with PIH are 15 times (95% CI: 4.8–44.1) more likely to have premature delivery resulting in poor outcomes. Uncontrolled PIH can also be an indication for early intervention.
Extremes in amniotic fluid – oligohydramnios and polyhydramnios were found to be associated with preterm delivery.5 In this study too we found that 18.3% of the women with preterm delivery had abnormal amniotic fluid volume, though the study conducted by Chythra et al19 in the neighbouring state did not find any association. In another study in Bangalore only 9.7% with extremes of amniotic fluid had preterm birth.25
In a study by Kusum et al22 about a half (48%) of subjects were found to be anaemic compared to about a fifth in this study. We also found that anaemic women were three times more prone to have preterm delivery. The lower levels of anaemic patients may be due to the better antenatal care and higher awareness in the state. Other studies across the world have also shown that low nutritional status as indicated by low BMI26–28 and low levels of folate27 can lead to preterm birth. Low concentrations of minerals such as iron are associated with decreased blood flow and increased maternal infections.28,29 In fact, eating disorders during pregnancy have been associated with preterm birth in 36% of studies in a review article.30 Anaemia can be prevented by adequate maternal nourishment during the period of gestation and by the provision of prophylactic iron doses for 100 days through the iron deficiency anaemia prevention program of the Govt of India.31 The importance of adherence to intake of iron and folic should also be stressed to the antenatal women.
The average birth weight of preterm babies is 2.1 ± 0.6 kg, while that of term babies are 3±0.4 kg. Out of the 191 preterm babies, 4 (2.1%) died and 51.8% required NICU admissions. Among the preterm babies, 13 (6.8%) had a cardiac abnormality, 5 (2.6%) babies had renal abnormalities, 5 (2.5%) had respiratory distress and 9 (4.7%) had IUGR. In a similar study in Bangalore, the neonatal mortality was 6.9% and the NICU admissions was 66.5%.25 The NICU admissions were either for observation for prematurity and various other complications like perinatal asphyxia, respiratory distress syndrome and sepsis. Thus, identifying women at risk of preterm labour and their proper treatment and care can reduce poor outcomes.
Strengths of the study include the fact that factors like confounding were addressed by doing a multivariate analysis and strong association was found with risk factors like PIH (14.608), AF volume (10.679) and PROM (10.269), followed by a history of previous preterm delivery (4.118), UTI (3.669) and anaemia (2.537). Collinearity has also been ruled out among the independent variables. High p values rule out the possibility of it being due to chance.
Some of the limitations of the study include the possibility of selection bias. The study was conducted in a hospital setting and may not be representative of the entire population of women with preterm delivery in Kerala. However, as the study is done in the state of Kerala where 99% of the deliveries are institutional the study can be considered to be representative of the population.32 About 9.09% and 13.5% of records each of cases and controls was discarded as these records did not have the correct hospital registration number or address of the patients mentioned. Since it was a record-based study, the information on BMI, maternal education, and economic background were not available. Hence these variables were not included in the study. Non-obstetrical risk factors like maternal malnutrition, SES, trauma, alcohol use, exposure to second hand smoking, physical activity, and depression were not looked into as the data was obtained from hospital records. Another limitation is that, though there are studies in other parts of the world where air pollution such as the presence of sulfur dioxide is associated with adverse birth outcomes,33 it could not be considered due to lack of data. Measurement of exposure variables such as anaemia was made based on the Hb values recorded in the first trimester which may have improved, thus overestimating effect.
Conclusion
Addressing the burden of preterm birth is crucial to achieving Sustainable Development Goal 3 and for reducing preterm-related neonatal and child mortality.34 Most efforts so far have been focussed on tertiary interventions. These measures have reduced perinatal morbidity and mortality, but the incidence of preterm birth is increasing. The clinical implications for this are that advances in primary and secondary care are necessary such as preventing anaemia, UTI and controlling blood pressure through adequate medication.35 Women with systemic diseases require additional care to prevent the risk of preterm birth.
Acknowledgment
The authors acknowledge the support of the hospital administration and of the unknown women.
Author Contributions
- Raveena PS – Concept, Data Collection, and Implementation of the study.
- Parvathy A – Concept, Data Collection, and Implementation of the study.
- Neelanjana A – Concept, Data Collection, and Implementation of the study.
- Sudha S – Guidance in Concept, Data Collection, and Implementation of the study.
- Steffi Ann Varughese – Editing and analysis of the draft manuscript.
- *Aswathy Sreedevi – Concept development, Analysis and Editing the draft manuscript.
- Sheejamol S – Analysis and Statistical guidance.
All authors made substantial contributions to conception and design, acquisition of data, or analysis and interpretation of data; took part in drafting the article or revising it critically for important intellectual content; agreed to submit to the current journal; gave final approval of the version to be published; and agree to be accountable for all aspects of the work.
Disclosure
The authors declare that there are no conflicts of interests in relation to this work.
References
1. Preterm Birth-WHO. Fact sheet; 2018. Available from: www.who.int.
2. Kuppusamy N, Vidhyadevi A. Prevalence of preterm admissions and the risk factors of preterm labor in rural Medical College Hospital. Int J Sci Stud. 2016;4(9):125–128.
3. Copper RL, Goldenberg RL, Creasy RK, et al. A multicenter study of preterm birth weight and gestational age-specific neonatal mortality. Am J Obstet Gynecol. 1993;168(1):78–84. doi:10.1016/S0002-9378(12)90889-3
4. Institute of Medicine (US) Committee on Understanding Premature Birth and Assuring Healthy Outcomes; Behrman RE, Butler AS, editors. Preterm Birth: Causes, Consequences, and Prevention. Washington (DC): National Academies Press (US); 2007. 10, Mortality and Acute Complications in Preterm Infants.
5. Goldenberg RL, Culhane JF, Iams JD, Romero R. Epidemiology and causes of preterm birth. Lancet. 2008;371(9606):75–84. doi:10.1016/S0140-6736(08)60074-4
6. Covarrubias LO, Aguirre GER, Chapuz JR, May AIL, Velázquez JD, Eguiluz ME. Maternal factors associated to prematurity. Ginecol Obstet Mex. 2008;76(9):526–536.
7. The unfinished agenda of preterm births. Editorial. Lancet. 2016;388(10058):P2323
8. Romero R, Espinoza J, Kusanovic J, et al. The preterm parturition syndrome. BJOG. 2006;113:17–42.
9. O’Shea TM, Allred EN, Dammann O, et al. The ELGAN study of the brain and related disorders in extremely low gestational age newborns. Early Hum Dev. 2009;85(11):719–725. doi:10.1016/j.earlhumdev.2009.08.060
10. Soundarajan P, Muthuramu P, Veerapandi M, Mariappan R. Retrospective study factors related to preterm birth in Government Raja Mirasudar hospital and obstetric and perinatal outcome. Int J Reprod Contracept Obstet Gynecol. 2017;5(9):3006–3010.
11. Campbell EE, Gilliland J, Dworatzek PDN, de Vrijer B, Penava D, Seabrook JA. Socioeconomic status and adverse birth outcomes: a population-based Canadian sample. J Biosoc Sci. 2018;50(1):102–113.
12. Smith A, Twynstra J, Seabrook JA. Antenatal depression and offspring health outcomes. Obstet Med. 2020;13(2):55–61. doi:10.1177/1753495X19843015
13. Wong SPW, Twynstra J, Gilliland JA, Cook JL, Seabrook JA. Risk factors and birth outcomes associated with teenage pregnancy: a Canadian sample. J Pediatr Adolesc Gynecol. 2020;33(2):153–159. doi:10.1016/j.jpag.2019.10.006
14. Zupan J, Åhman E. Neonatal and perinatal mortality: country, regional and global estimates. Geneva: World Health Organization; 2006. 69.
15. Chronic Hypertension and Pregnancy. Nephrology, Department of Medicine, University of Rochester Medical Center. Rochester, NY: University of Rochester Medical Center [Internet]. Available from: https://www.urmc.rochester.edu/medicine/nephrology/patient-care/conditions/chronic-hypertension-and-pregnancy.aspx.
16. Kintiraki E, Papakatsika S, Kotronis G, Goulis DG, Kotsis V. Pregnancy-Induced hypertension. Hormones. 2015;14(2):211–223. doi:10.14310/horm.2002.1582
17. Lord M, Marino S, Kole M. Amniotic Fluid Index. [Updated 2021 Jan 6]. In: StatPearls [Internet]. Treasure Island (FL): StatPearls Publishing; Jan 2021. 1–5.
18. Zupan J, Åhman E. Neonatal and perinatal mortality: country, regional and global estimates. Geneva: World Health Organization; 2006:69.
19. Rao CR, de Ruiter LEE, Bhat P, Kamath V, Kamath A, Bhat V. A case-control study on risk factors for preterm deliveries in a secondary care hospital, southern India. ISRN Obstet Gynecol. 2014;2014:935982. doi:10.1155/2014/935982
20. Mathew SM, Kumar A. A prospective analysis of the risk factors and the perinatal Outcome of preterm labour. Int J Reprod Contracept Obstet Gynecol. 2018;7(12):4833–4839. doi:10.18203/2320-1770.ijrcog20184924
21. Mahajan A, Magon S. Study of risk factors for preterm births in a teaching hospital: a prospective study. Int J MedDental Sci. 2017;6(1):1407–1424. doi:10.19056/ijmdsjssmes/2017/v6i1/125563
22. Kusum, Anantbir SL, Harbhajan KS, Amritpal K. A study of evaluation of etiological factors of preterm labour in a tertiary hospital. Sch J App Med Sci. 2017;5(2B):396–400.
23. Garg S, Kaur T, Saran AS, Yadav M. A study of etiology and outcome of preterm birth at a tertiary care centre. Int J Reprod Contracept Obstet Gynecol. 2017;6(10):4488. doi:10.18203/2320-1770.ijrcog20174429
24. Jamal S, Srivastava R. A retrospective analytical study of the epidemiology and causes of preterm birth. Int J Reprod Contracept Obstet Gynecol. 2017;6(12):5453–5457. doi:10.18203/2320-1770.ijrcog20175259
25. Shetty MB, M KB, Malyala M, Swarup A, Pathadan DS, Pocha S. Preterm birth: associated risk factors and outcome in tertiary care center. Int J Reprod Contracept Obstet Gynecol. 2017;6(8):3271–3274. doi:10.18203/2320-1770.ijrcog20173258
26. Hendler I, Goldenberg RL, Mercer BM, et al. The Preterm Prediction Study: association between maternal body mass index and spontaneous and indicated preterm birth. Am J Obstet Gynecol. 2005;192(3):882–886. doi:10.1016/j.ajog.2004.09.021
27. Tamura T, Goldenberg RL, Freeberg LE, Cliver SP, Cutter GR, Hoffman HJ. Maternal serum folate and zinc concentrations and their relationships to pregnancy outcome. Am J Clin Nutr. 1992;56(2):365–370. doi:10.1093/ajcn/56.2.365
28. Garfield RE, Gasc JM, Baulieu EE. Effects of the antiprogesterone RU 486 on preterm birth in the rat. Am J Obstet Gynecol. 1987;157(5):1281–1285. doi:10.1016/S0002-9378(87)80315-0
29. Meis PJ, Klebanoff M, Thom E, et al. Prevention of recurrent preterm delivery by 17 alpha-hydroxyprogesterone caproate. N Engl J Med. 2003;348(24):2379–2385. doi:10.1056/NEJMoa035140
30. Charbonneau KD, Seabrook JA. Adverse birth outcomes associated with types of eating disorders: a review. Can J Diet Pract Res. 2019;80(3):131–136. doi:10.3148/cjdpr-2018-044
31. Anaemia during pregnancy. National Health portal. Available from: www.nhp.gov.in.
32. Deliveries. Institutional deliveries/NITI Aayog. Accessed from: http://niti.gov.in/content/institutional-deliveries.
33. Seabrook JA, Smith A, Clark AF, Gilliland JA. Geospatial analysis of adverse birth outcomes in South western Ontario: examining the impact of environmental factors. Environ Res. 2019;172:18–26. doi:10.1016/j.envres.2018.12.068
34. Hug L, Alexander M, You D, Alkema L. National, regional, and global levels and trends in neonatal mortality between 1990 and 2017, with scenario-based projections to 2030: a systematic analysis. Lancet Global Health. 2019;7(6):e710–20. doi:10.1016/S2214-109X(19)30163-9
35. Iams JD, Romero R, Culhane JF, Goldenberg RL. Primary, secondary, and tertiary interventions to reduce the morbidity and mortality of preterm birth. Lancet. 2008;371(9607):164–175. doi:10.1016/S0140-6736(08)60108-7
 © 2021 The Author(s). This work is published and licensed by Dove Medical Press Limited. The
full terms of this license are available at https://www.dovepress.com/terms
and incorporate the Creative Commons Attribution
- Non Commercial (unported, 3.0) License.
By accessing the work you hereby accept the Terms. Non-commercial uses of the work are permitted
without any further permission from Dove Medical Press Limited, provided the work is properly
attributed. For permission for commercial use of this work, please see paragraphs 4.2 and 5 of our Terms.
© 2021 The Author(s). This work is published and licensed by Dove Medical Press Limited. The
full terms of this license are available at https://www.dovepress.com/terms
and incorporate the Creative Commons Attribution
- Non Commercial (unported, 3.0) License.
By accessing the work you hereby accept the Terms. Non-commercial uses of the work are permitted
without any further permission from Dove Medical Press Limited, provided the work is properly
attributed. For permission for commercial use of this work, please see paragraphs 4.2 and 5 of our Terms.