Back to Journals » Clinical Interventions in Aging » Volume 20
Risk Factors and Prediction Model for Hypokalemia as a Complication in Older Adults with Acute Cerebral Hemorrhage
Authors Jing S, Zhang L ![]() , Xu L
, Xu L
Received 1 July 2025
Accepted for publication 6 November 2025
Published 21 November 2025 Volume 2025:20 Pages 2153—2162
DOI https://doi.org/10.2147/CIA.S550753
Checked for plagiarism Yes
Review by Single anonymous peer review
Peer reviewer comments 5
Editor who approved publication: Dr Maddalena Illario
Shanquan Jing,1,* Lizhuang Zhang,2,* Lifeng Xu1
1Department of Neurosurgery, The First Hospital of Hebei Medical University, Shijiazhuang, People’s Republic of China; 2Department of Rehabilitation Medicine, the First Hospital of Hebei Medical University, Shijiazhuang, People’s Republic of China
*These authors contributed equally to this work
Correspondence: Lifeng Xu, Department of Neurosurgery, The First Hospital of Hebei Medical University, No. 89 Donggang Road, Shijiazhuang, Hebei, 050031, People’s Republic of China, Tel +86-311-87155042, Email [email protected]
Objective: This study aimed to identify the key risk factors for hypokalemia in older adults with acute cerebral hemorrhage (ACH) and to develop a clinically practical risk predictive model based on logistic regression.
Methods: A total of 209 older adult ACH patients (age 60– 82 years) treated at The First Hospital of Hebei Medical University from July 2022 to July 2024 were included in this retrospective cohort study. Patients were divided into two groups: hypokalemic (serum potassium < 3.5 mmol/L, n = 56) and normokalemic (serum potassium 3.5– 5.5 mmol/L, n = 153). Clinical outcomes were compared, and logistic regression was used to identify risk factors for hypokalemia. A risk prediction model was constructed and presented as a nomogram. The diagnostic value of the model was assessed using receiver operating characteristic (ROC) curves.
Results: Hypokalemia was associated with significantly higher in-hospital mortality, poorer functional outcomes, longer hospital stays, and more frequent neurological deterioration (all P < 0.05). Univariate and multivariate logistic regression identified female gender (OR=2.713), higher NIHSS scores at admission (OR=2.375), GFR ≤ 60 mL/min/1.73 m2 (OR=2.316), and furosemide use > 20 mg/d (OR=2.351) as independent risk factors for hypokalemia. ROC analysis showed an area under the curve (AUC) for the multivariable predictive model of 0.859, which was superior to individual predictors.
Conclusion: Female gender, higher neurological deficit severity (NIHSS score), impaired renal function (GFR ≤ 60 mL/min/1.73 m2), and use of furosemide > 20 mg/d are significant independent risk factors for hypokalemia in older adult ACH patients. Given its association with adverse outcomes, early prediction is crucial. The predictive model and corresponding nomogram provide a practical tool for identifying high-risk patients, facilitating timely intervention.
Keywords: cerebral hemorrhage, hypokalemia, risk factors, clinical outcomes, risk prediction model, older adults
Introduction
Acute cerebral hemorrhage (ACH) in older adults is a critical and often fatal condition that contributes significantly to both mortality and disability rates worldwide.1 The onset of ACH frequently complicates clinical management due to the complex interactions between cerebrovascular pathology, comorbid conditions, and age-related physiological changes. A common but underrecognized complication in these patients is hypokalemia, a condition where serum potassium levels fall below the normal range. Hypokalemia is not merely an electrolyte disturbance; it can worsen clinical outcomes and may be associated with increased morbidity, including cardiac arrhythmias, muscle weakness, prolonged hospitalization, and even death.2,3 Potassium is a crucial electrolyte for maintaining cellular membrane potential, essential for nerve impulse transmission, muscle contraction, and normal heart function.
While extensive tissue damage from any acute injury can cause hyperkalemia due to cell lysis, the acute systemic stress response following ACH often results in hypokalemia. This paradoxical effect is primarily driven by sympathetic nervous system activation and the release of catecholamines.4–6 These hormones, particularly adrenaline, activate β2-adrenergic receptors on cell membranes, which enhances the activity of Na⁺-K⁺-ATPase pumps and facilitates the influx of potassium ions into cells, thereby reducing serum potassium levels.7 In addition, the clinical management of cerebral hemorrhage often involves the use of dehydrating agents like the loop diuretic furosemide to reduce cerebral edema and mitigate the risk of brain herniation. While these agents are critical in preventing secondary neurological damage, they can also disrupt the balance of electrolytes, further increasing the risk of hypokalemia.8
Despite the clinical relevance of hypokalemia in older adult ACH patients, the identification of specific risk factors and the development of predictive models remain limited.9,10 Previous studies have often focused on electrolyte disturbances in the general stroke population, without specifically addressing the unique pathophysiology and risk profile of older adults with hemorrhagic stroke.11,12 This research gap impedes the timely diagnosis and appropriate management of hypokalemia, which can have detrimental effects on recovery.13 Early identification of at-risk patients would allow for proactive strategies, such as intensified monitoring or pre-emptive potassium supplementation, potentially mitigating adverse outcomes.14 Therefore, this study aimed to identify the key risk factors for hypokalemia in older adults with ACH and to develop a predictive model based on logistic regression. Such a model could guide clinicians in assessing the likelihood of hypokalemia in individual patients, enabling proactive intervention.
In this study, we hypothesize that factors such as gender, the severity of neurological impairment at admission, renal function parameters, and the use of certain medications—particularly diuretics—are significant predictors of hypokalemia in older adult ACH patients. Furthermore, we sought to establish the clinical impact of hypokalemia by examining its association with key patient outcomes. To this end, we conducted a retrospective analysis of clinical data from 209 older adult ACH patients, constructed a risk prediction model based on the identified risk factors, and developed a nomogram to serve as a practical tool for clinical use. The goal was to establish a tool that could assist healthcare providers in identifying patients at high risk for hypokalemia, thus improving patient care and outcomes.
Materials and Methods
Participants
A retrospective analysis was conducted on 209 patients with acute cerebral hemorrhage who were treated at The First Hospital of Hebei Medical University between July 2022 and July 2024. The cohort included 135 males and 74 females, aged 60 to 82 years (mean age: 71.32 ± 2.71 years). Based on admission serum potassium levels, patients were divided into two groups: the hypokalemia group (serum potassium < 3.5 mmol/L, n = 56) and the normokalemia group (serum potassium 3.5–5.5 mmol/L, n = 153). Patients with hyperkalemia (serum potassium > 5.5 mmol/L) at admission were excluded from this study.
Inclusion Criteria: (1) Diagnosed with acute cerebral hemorrhage according to the Chinese Guidelines for the Diagnosis and Treatment of Cerebral Hemorrhage (2019);15 (2) First-ever, spontaneous intracerebral parenchymal hemorrhage confirmed by an initial cranial computed tomography (CT) scan; (3) Time from symptom onset to hospital admission < 72 hours; (4) Age > 60 years; (5) No prior intravenous thrombolytic therapy before enrollment; (6) All patients received enteral nutrition.
Exclusion Criteria: (1) Presence of traumatic brain injury (to isolate spontaneous ACH); (2) Diagnosis of malignant tumors (to avoid confounding from paraneoplastic syndromes); (3) Known coagulation dysfunction (to exclude hemorrhages primarily due to systemic coagulopathies); (4) Severe congenital heart disease (to avoid confounding from complex cardiac conditions); (5) Documented history of severe dementia or other major neurocognitive disorders (to ensure reliability of neurological assessments); (6) Aneurysmal subarachnoid hemorrhage with or without intracerebral hematoma.
This study was a retrospective analysis of anonymized data.
Methods
Data for this retrospective study were extracted from The First Hospital of Hebei Medical University’s electronic health record (EHR) system. Two trained researchers independently reviewed patient records and used a standardized data abstraction form to systematically collect the following variables: gender, age, smoking history, alcohol consumption history, history of hypertension, history of diabetes, body mass index (BMI), hemorrhage location, systolic and diastolic blood pressure at admission, hemorrhage volume, time from onset to admission, National Institutes of Health Stroke Scale (NIHSS) score at admission, blood urea nitrogen (BUN) at admission, serum creatinine (SCr) at admission, glomerular filtration rate (GFR), and furosemide dosage. In light of their potential influence on potassium homeostasis, data on admission serum magnesium levels and in-hospital use of mannitol were also collected. Clinical outcome data were also collected, including in-hospital mortality, length of hospital stay, functional status at discharge assessed by the modified Rankin Scale (mRS), and in-hospital neurological deterioration (defined as an increase of ≥2 points in the NIHSS score from admission).
NIHSS Score
The NIHSS was assessed at admission, comprising 15 items with a total score of 42 points. Higher scores indicate more severe neurological deficits. This admission score was used as the primary predictor variable in our risk model.
Hemorrhage Volume
Hemorrhage volume was measured at admission using a GE F-II multi-slice spiral CT scanner. The ABC/2 method was employed to calculate hemorrhage volume, where A is the maximum hemorrhage diameter, B is the diameter perpendicular to A, and C is the approximate product of the number of CT slices and slice thickness.
Statistical Analysis
Statistical analysis was performed using SPSS 26.0 software. Normally distributed continuous data were expressed as mean ± standard deviation (x ± s) and compared using independent samples t-tests. Categorical data were expressed as percentages and analyzed using the χ2-test or Fisher’s exact test where appropriate. Logistic regression analysis was employed to identify potential risk factors for hypokalemia. Receiver operating characteristic (ROC) curve analysis was used to evaluate the diagnostic performance of the final predictive model. Based on the multivariate logistic regression model, a nomogram was constructed using the “rms” package in R software (version 4.2.1) to create a visual tool for predicting the probability of hypokalemia. A post-hoc power analysis was conducted using G*Power software (version 3.1). For the multivariate logistic regression with four predictors, a sample size of 209 (56 cases, 153 controls), and an alpha of 0.05, the analysis revealed a power of >0.95 to detect an odds ratio of 2.5 (a conservative estimate based on our results), indicating that the sample size was adequate. A P-value < 0.05 was considered statistically significant.
Collinearity Diagnostics
To address potential multicollinearity among renal function indicators (BUN, SCr, and GFR), a collinearity diagnostic analysis was performed on the variables included in the multivariate logistic regression model. The Variance Inflation Factor (VIF) was calculated for each predictor. All VIF values were below 2.0 (BUN: 1.89; SCr: 1.95), indicating that multicollinearity was not a significant issue in our model.
Results
Comparison of General Clinical Data
The hypokalemia group had a significantly higher proportion of females (53.6% vs 28.8%, P < 0.001), higher NIHSS scores at admission (18.60 ± 2.70 vs 14.70 ± 1.75, P < 0.001), elevated blood urea nitrogen (BUN) levels at admission (5.75 ± 2.40 mmol/L vs 4.65 ± 1.45 mmol/L, P < 0.001), higher serum creatinine (SCr) levels (82.60 ± 21.10 μmol/L vs 71.60 ± 18.40 μmol/L, P = 0.001), a higher proportion of patients with a glomerular filtration rate (GFR) ≤ 60 mL/min/1.73 m2 (51.8% vs 28.8%, P = 0.008), and a higher proportion of patients receiving furosemide doses > 20 mg/d (53.6% vs 32.7%, P = 0.004) compared to the normokalemia group. However, there were no significant differences between the two groups in terms of age, smoking history, alcohol consumption history, history of hypertension, history of diabetes, or body mass index (BMI) (P > 0.05) (Table 1).
 |
Table 1 Comparison of General Clinical Data Between the Hypokalemia and Normokalemia Groups |
Clinical Outcomes Associated with Hypokalemia
To assess the clinical significance of hypokalemia, we compared key outcomes between the two groups (Table 2). The hypokalemia group exhibited a significantly higher rate of in-hospital mortality (16.1% vs 5.9%, P = 0.021), a greater proportion of patients with poor functional outcome (mRS > 3) at discharge (73.2% vs 45.1%, P < 0.001), a longer mean hospital stay (18.5 ± 5.2 days vs 14.1 ± 4.5 days, P < 0.001), and a higher incidence of neurological deterioration (25.0% vs 11.1%, P = 0.015) compared to the normokalemia group.
 |
Table 2 Clinical Outcomes Associated with Hypokalemia |
Univariate and Multivariate Logistic Regression Analysis
Univariate logistic regression analysis revealed that female gender, higher NIHSS score at admission, elevated BUN, higher SCr levels, GFR ≤ 60 mL/min/1.73 m2, and furosemide dosage > 20 mg/d were significant risk factors for hypokalemia in older adults with ACH (P < 0.05) (Table 3). To control for potential confounders and identify independent predictors, these variables were included in a multivariate logistic regression analysis. The results confirmed that female gender (OR = 2.713, 95% CI: 1.253–5.875, P = 0.012), NIHSS score at admission (OR = 2.375, 95% CI: 1.735–3.251, P < 0.001), GFR ≤ 60 mL/min/1.73 m2 (OR = 2.316, 95% CI: 1.062–5.053, P = 0.035), and furosemide dosage > 20 mg/d (OR = 2.351, 95% CI: 1.101–5.020, P = 0.027) were independent risk factors for hypokalemia (Table 4).
 |
Table 3 Univariate Logistic Regression Analysis of Risk Factors for Hypokalemia |
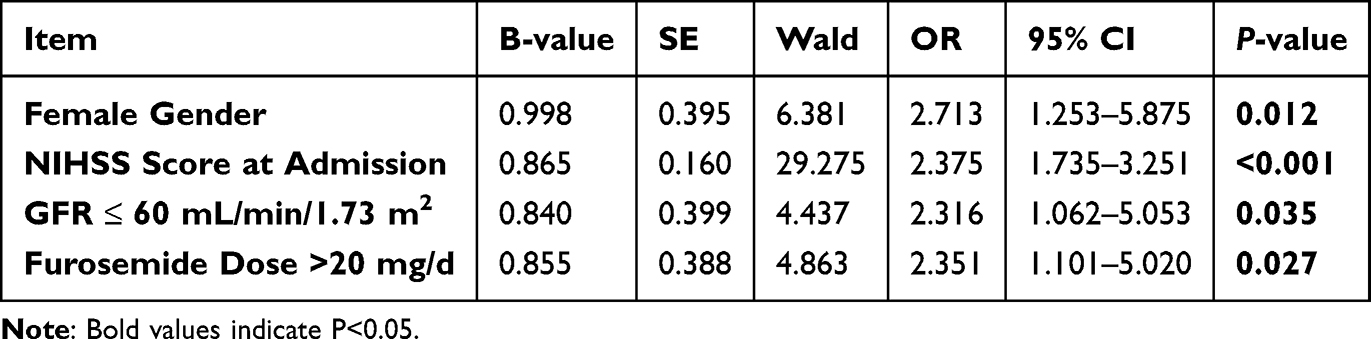 |
Table 4 Multivariate Logistic Regression Analysis of Independent Risk Factors for Hypokalemia |
Development and Validation of a Predictive Model
A multivariable predictive model for hypokalemia was constructed based on the four independent risk factors identified. The model’s discriminative ability was evaluated using ROC curve analysis. The areas under the curve (AUC) for the individual risk factors—female gender, NIHSS score at admission, GFR ≤ 60 mL/min/1.73 m2, and furosemide dosage > 20 mg/d—were 0.623, 0.825, 0.604, and 0.615, respectively. The final multivariable predictive model demonstrated excellent discrimination, with an AUC of 0.859 (95% CI: 0.795–0.923), which was significantly higher than that of most individual predictors (Table 5 and Figure 1). To provide a user-friendly tool for clinical practice, we developed a nomogram based on the four independent risk factors (Figure 2). The nomogram allows for the calculation of a total point score for an individual patient, which corresponds to a specific predicted probability of developing hypokalemia.
 |
Table 5 Diagnostic Performance of the Predictive Model and Individual Risk Factors for Hypokalemia |
 |
Figure 1 ROC Curve Analysis of the Predictive Model for Hypokalemia. The figure shows the receiver operating characteristic (ROC) curves for individual predictors (Female gender, NIHSS score at admission, GFR ≤ 60 mL/min/1.73 m2, Furosemide dose >20 mg/d) and the final multivariable predictive model. The predictive model demonstrates the highest diagnostic performance (AUC = 0.859). |
 |
Figure 2 Nomogram for Predicting the Risk of Hypokalemia in Older Adults with ACH. To use the nomogram, locate the patient’s characteristics on each axis. Draw a vertical line up to the “Points” axis to determine the score for each variable. Sum the scores to get a total point value, then draw a vertical line from the “Total Points” axis down to the “Risk of Hypokalemia” axis to find the patient’s predicted probability. |
Analysis of Potential Confounders
To address potential confounding from co-administered medications and baseline electrolyte status, we analyzed admission serum magnesium levels and in-hospital mannitol use. The hypokalemia group had significantly lower mean serum magnesium levels compared to the normokalemia group (0.78 ± 0.11 mmol/L vs 0.85 ± 0.13 mmol/L, P = 0.002). However, there was no significant difference in the proportion of patients who received mannitol between the two groups (48.2% vs 44.4%, P = 0.638). These results are detailed in Supplementary Table 1.
Discussion
Acute cerebral hemorrhage is a prevalent clinical cerebrovascular condition, accounting for 6.50% to 19.60% of all stroke cases, according to epidemiological studies.16 Current clinical management primarily focuses on reducing intracranial pressure; however, patients are at risk of electrolyte imbalances, including hypokalemia, during treatment.17 Importantly, our study reveals that the presence of hypokalemia is not a benign laboratory finding; it is significantly associated with poorer clinical outcomes, including higher in-hospital mortality, worse functional status at discharge, longer hospital stays, and increased neurological deterioration. These findings are consistent with recent studies linking serum potassium dysregulation with unfavorable outcomes in stroke patients18 and underscore the clinical urgency of identifying patients at risk for hypokalemia to enable prompt intervention. This study aimed to identify the factors influencing hypokalemia and develop a tool for early risk stratification.
Our study identified four independent risk factors for hypokalemia in older adult ACH patients: female gender, higher NIHSS score at admission, GFR ≤ 60 mL/min/1.73 m2, and furosemide use > 20 mg/d. These findings provide a clearer understanding of the patient profiles most vulnerable to this complication.
The higher incidence of hypokalemia in females, particularly in an older, likely postmenopausal cohort, is complex. While our study population is over 60 and therefore past active menstrual changes, physiological differences persist. It is hypothesized that sex-based differences in renal handling of electrolytes, body composition, and neurohormonal responses to acute stress may persist into later life.19–21 Postmenopausal changes in the renin-angiotensin-aldosterone system and differential responses to stress may also contribute. Our findings, consistent with some previous reports,6,22 highlight that female sex is a non-modifiable risk factor that should raise clinical suspicion.
The NIHSS score is a well-established measure of stroke severity.23 A higher NIHSS score reflects more extensive brain damage. In the context of cerebral hemorrhage, severe neurological injury triggers a profound systemic stress response, leading to hypothalamic stimulation and a surge in catecholamines. This cascade activates the renin-angiotensin-aldosterone system and increases insulin secretion, both of which drive potassium into cells and reduce serum levels.24,25 Impaired renal function, manifested as a reduced GFR, is another key risk factor. The cut-off value of GFR ≤ 60 mL/min/1.73 m2 was selected as it is the standard threshold for diagnosing chronic kidney disease (CKD) according to the Kidney Disease: Improving Global Outcomes (KDIGO) guidelines.26 While acute brain injury can transiently decrease renal perfusion,27 pre-existing renal insufficiency compromises the kidney’s ability to conserve potassium, particularly when tubular function is impaired.28 While our study identifies an association between low GFR and hypokalemia, the retrospective design does not allow for the determination of causality, as the relationship may be bidirectional.
Furosemide, a commonly used loop diuretic, is crucial for managing intracranial pressure in ACH.29 In our cohort, furosemide was administered post-admission specifically for the management of cerebral edema. The 20 mg/d cut-off for furosemide was chosen as it represents a common starting dose in clinical practice for managing cerebral edema, beyond which the risk of electrolyte disturbance is known to increase. While a 20 mg/d dose may be considered low, in critically ill older adults with acute neurological injury and potential subclinical renal dysfunction, this dose may be sufficient to disrupt a fragile electrolyte balance. By inhibiting the Na-K-2Cl cotransporter in the loop of Henle, furosemide increases distal tubular flow and sodium delivery, thereby enhancing potassium excretion.8 Our study confirms that even relatively common doses can significantly increase the risk of hypokalemia in this vulnerable population.
A key strength of our study is the development and validation of a multivariable predictive model, culminating in a practical nomogram. The model demonstrated strong predictive accuracy (AUC = 0.859) and provides a quantitative tool for risk stratification. By integrating these four readily available clinical variables—gender, NIHSS score, GFR, and furosemide use—clinicians can identify high-risk individuals upon admission. This allows for the implementation of targeted strategies, such as more frequent potassium monitoring or prophylactic supplementation, thereby potentially preventing the adverse outcomes we have shown to be associated with hypokalemia.
This study also highlights the importance of hypokalemia on not just short-term stability but also on longer-term recovery. The association with poorer functional outcomes (mRS > 3) at discharge suggests that in-hospital hypokalemia may have lasting consequences on neurological recovery. Potential mechanisms include its impact on neuronal excitability, muscle function essential for rehabilitation, and cardiovascular stability.30 Future prospective studies should focus on whether the prevention and prompt correction of hypokalemia can improve these long-term functional outcomes.
An important consideration in the management of ACH is the use of other medications that can influence electrolyte balance. As requested by reviewers, we specifically investigated serum magnesium and the use of mannitol. Our data showed that lower admission magnesium was indeed associated with hypokalemia (Supplementary Table 1), which aligns with existing literature identifying hypomagnesemia as a key contributor to refractory hypokalemia.31,32 While magnesium was not included in our final predictive model to maintain simplicity with a focus on readily available risk factors, clinicians should be aware of this link and consider monitoring magnesium levels in high-risk patients. Conversely, the use of mannitol, another osmotic agent, did not differ significantly between the groups, suggesting it was not a major confounder for hypokalemia in our cohort.
Conclusion
Female gender, higher neurological deficit severity (NIHSS score), impaired renal function (GFR ≤ 60 mL/min/1.73 m2), and the use of furosemide > 20 mg/d are significant independent risk factors for the development of hypokalemia in older adults with ACH. The developed predictive model and nomogram offer a practical, non-invasive tool for early risk stratification at the patient’s bedside. Integration of this model into electronic health records could trigger automated alerts, prompting clinicians to intensify potassium monitoring and consider pre-emptive potassium supplementation in high-risk individuals. However, this study has limitations. Its main weaknesses are the single-center, retrospective design and a relatively small sample size, which may introduce biases. Although we have now analyzed serum magnesium, our initial analysis did not include other electrolytes like sodium or chloride. Hypomagnesemia, as shown in our supplementary analysis, is a known contributor to refractory hypokalemia and represents an important factor to consider clinically. While our analysis showed mannitol use was not a confounder in our cohort, we did not collect systematic data on other medications like corticosteroids. Therefore, before widespread clinical adoption, future multi-center, large-sample, prospective cohort studies are needed to further validate these findings and the predictive utility of the nomogram.
Data Sharing Statement
The datasets generated and analyzed during the current study are available from the corresponding author on reasonable request.
Ethics Approval and Consent to Participate
The study protocol was approved by the Ethics Committee of Hebei Medical University (Protocol No. S00358), and the study was performed in accordance with the Helsinki II declaration. Informed consent to participate was waived by the Ethics Committee of Hebei Medical University because the research was retrospective and conducted on anonymized data.
Author Contributions
All authors made a significant contribution to the work reported, whether that is in the conception, study design, execution, acquisition of data, analysis and interpretation, or in all these areas; took part in drafting, revising or critically reviewing the article; gave final approval of the version to be published; have agreed on the journal to which the article has been submitted; and agree to be accountable for all aspects of the work.
Funding
This study was funded by Medical Science Research Project of Hebei (No. 20160702), and the medical key projects of Hebei Province Health Department (No. 20150653).
Disclosure
The authors declare that they have no competing interests.
References
1. Chhabra N, Crepeau AZ, Demaerschalk BM, et al. Does initiation of prophylactic antiseizure medication improve neurological outcomes in patients with acute intracerebral hemorrhage?: a critically appraised topic. Neurologist. 2023;28(6):422–425. doi:10.1097/NRL.0000000000000537
2. Logan Ellis H, Llewellyn D, Mendis J, Whyte M. Admission plasma potassium and length of hospital stay: a meta-analysis. BMJ open. 2023;13(8):e068387. doi:10.1136/bmjopen-2022-068387
3. Skogestad J, Aronsen JM. Hypokalemia-induced arrhythmias and heart failure: new insights and implications for therapy. Front Physiol. 2018;9:1500. doi:10.3389/fphys.2018.01500
4. Ok SH, Chung YW, Sohn JT, Jung JM, Chung YK. Severe hypokalemia occurring during barbiturate coma therapy in a patient with severe acute head injury. Acta anaesthesiologica Scandinavica. 2005;49(6):883–884. doi:10.1111/j.1399-6576.2005.00728.x
5. Kuo PJ, Huang CY, Hsu SY, Hsieh CH. Evaluating the prognostic value of the stress index in trauma patients. Heliyon. 2024;10(17):e36884. doi:10.1016/j.heliyon.2024.e36884
6. Baker MB, Binda DD, Nozari A, Baker WE. The silent threat of hypokalemia after high voltage electrical injuries: a case study and review of the literature. J Clin Med. 2024;13(10):2852. doi:10.3390/jcm13102852
7. Kildegaard H, Brabrand M, Forberg JL, Platonov P, Lassen AT, Ekelund U. Prevalence and prognostic value of electrocardiographic abnormalities in hypokalemia: a multicenter cohort study. J Internal Med. 2024;295(4):544–556. doi:10.1111/joim.13757
8. Beaulieu C, Kurczewski L. Characterization of the effect of prolonged therapeutic hypothermia on serum magnesium and potassium following neurological injury. Ther Hypothermia Temp Manag. 2019;9(4):231–237. doi:10.1089/ther.2018.0037
9. Qureshi AI, Tuhrim S, Broderick JP, Batjer HH, Hondo H, Hanley DF. Spontaneous intracerebral hemorrhage. New Engl J Med. 2001;344(19):1450–1460. doi:10.1056/NEJM200105103441907
10. Caruso BJ, Cotant CL, Mielke BA, Pfeiffer DC. Hypertension With Hypokalemia: a Quiz. Am J Kidney Dis. 2022;80(6):A12–a14. doi:10.1053/j.ajkd.2022.07.011
11. Jensen HK, Brabrand M, Vinholt PJ, Hallas J, Lassen AT. Hypokalemia in acute medical patients: risk factors and prognosis. Am J Med. 2015;128(1):60–67.e61. doi:10.1016/j.amjmed.2014.07.022
12. Mattsson N, Kumarathurai P, Larsen BS, Nielsen OW, Sajadieh A. Mild hypokalemia and supraventricular ectopy increases the risk of stroke in community-dwelling subjects. Stroke. 2017;48(3):537–543. doi:10.1161/STROKEAHA.116.015439
13. Ybanez N, Agrawal V, Tranmer BI, Gennari FJ. Severe hypokalemia in a patient with subarachnoid hemorrhage. Am J Kidney Dis. 2014;63(3):530–535. doi:10.1053/j.ajkd.2013.07.005
14. Montepara CA, Bortmas MR, Cochenour CJ, et al. The effect of potassium supplementation and concomitant medications on potassium homeostasis for hospitalized patients. Am J Health Syst Pharm. 2024;81(6):183–189. doi:10.1093/ajhp/zxad310
15. Cao Y, Yu S, Zhang Q. Chinese stroke association guidelines for clinical management of cerebrovascular disorders: executive summary and 2019 update of clinical management of intracerebral haemorrhage. Stroke Vasc Neurol. 2020;5(4):396–402. doi:10.1136/svn-2020-000433
16. Kozberg MG, Perosa V, Gurol ME, van Veluw SJ. A practical approach to the management of cerebral amyloid angiopathy. Int J Stroke. 2021;16(4):356–369. doi:10.1177/1747493020974464
17. Connolly SJ, Sharma M, Cohen AT, et al. Andexanet for factor xa inhibitor-associated acute intracerebral hemorrhage. New Engl J Med. 2024;390(19):1745–1755. doi:10.1056/NEJMoa2313040
18. Hossain MF, Kharel M, Husna AU, Khan MA, Aziz SN, Taznin T. Prevalence of electrolyte imbalance in patients with acute stroke: a systematic review. Cureus. 2023;15(8):e43149. doi:10.7759/cureus.43149
19. Elsheikh S, Elbaz A, Rau A. Accuracy of automated segmentation and volumetry of acute intracerebral hemorrhage following minimally invasive surgery using a patch-based convolutional neural network in a small dataset. Neuroradiology. 2024;66(4):601–608. doi:10.1007/s00234-024-03311-4
20. McDonough AA, Layton AT. Sex differences in renal electrolyte transport. Curr Opin Nephrol Hypertens. 2023;32(5):467–475. doi:10.1097/MNH.0000000000000909
21. McDonough AA, Harris AN, Xiong LI, Layton AT. Sex differences in renal transporters: assessment and functional consequences. Nat Rev Nephrol. 2024;20(1):21–36. doi:10.1038/s41581-023-00757-2
22. Hu R, McDonough AA, Layton AT. Sex differences in solute and water handling in the human kidney: modeling and functional implications. iScience. 2021;24(6):102667. doi:10.1016/j.isci.2021.102667
23. Chen L, Jin Y, Wang L, et al. Impact of human serum albumin level on symptomatic cerebral vasospasm in patients with aneurysmal subarachnoid hemorrhage. Neurol Sci. 2024;45(1):213–222. doi:10.1007/s10072-023-07014-1
24. Qiu L, Fu F, Zhang W, He J, Zhan Z, Cheng Z. Prevalence, risk factors, and clinical outcomes of remote intracerebral hemorrhage after intravenous thrombolysis in acute ischemic stroke: a systematic review and meta-analysis. J Neurol. 2023;270(2):651–661. doi:10.1007/s00415-022-11414-2
25. Wolf S, Mielke D, Barner C, et al. Effectiveness of lumbar cerebrospinal fluid drain among patients with aneurysmal subarachnoid hemorrhage: a randomized clinical trial. JAMA Neurol. 2023;80(8):833–842. doi:10.1001/jamaneurol.2023.1792
26. Madero M, Levin A, Ahmed SB. Evaluation and management of chronic kidney disease: synopsis of the kidney disease: improving global outcomes 2024 clinical practice guideline. Ann Internal Med. 2025;178(5):705–713. doi:10.7326/ANNALS-24-01926
27. Roh DJ, Boehme A, Mamoon R. Relationships of hemoglobin concentration, ischemic lesions, and clinical outcomes in patients with intracerebral hemorrhage. Stroke. 2023;54(4):1021–1029. doi:10.1161/STROKEAHA.122.041410
28. Durand NC, Kim HG, Patel VN, et al. Mesenchymal stem cell therapy in acute intracerebral hemorrhage: a dose-escalation safety and tolerability trial. Neurocritical Care. 2024;41(1):59–69. doi:10.1007/s12028-023-01897-w
29. Southerland AM, Mayer SA, Chiota-McCollum NA. Glucose control and risk of symptomatic intracerebral hemorrhage following thrombolysis for acute ischemic stroke: a SHINE trial analysis. Neurology. 2024;102(9):e209323. doi:10.1212/WNL.0000000000209323
30. Gao F, Wang CT, Chen C, et al. Effect of hypokalemia on functional outcome at 3 months post-stroke among first-ever acute ischemic stroke patients. Medical Science Monitor. 2017;23:2825–2832. doi:10.12659/MSM.902464
31. Whang R, Flink EB, Dyckner T, Wester PO, Aikawa JK, Ryan MP. Magnesium depletion as a cause of refractory potassium repletion. Arch Intern Med. 1985;145(9):1686–1689. doi:10.1001/archinte.1985.00360090162024
32. Whang R, Whang DD, Ryan MP. Refractory potassium repletion. A consequence of magnesium deficiency. Arch Intern Med. 1992;152(1):40–45. doi:10.1001/archinte.1992.00400130066006
 © 2025 The Author(s). This work is published and licensed by Dove Medical Press Limited. The
full terms of this license are available at https://www.dovepress.com/terms
and incorporate the Creative Commons Attribution
- Non Commercial (unported, 4.0) License.
By accessing the work you hereby accept the Terms. Non-commercial uses of the work are permitted
without any further permission from Dove Medical Press Limited, provided the work is properly
attributed. For permission for commercial use of this work, please see paragraphs 4.2 and 5 of our Terms.
© 2025 The Author(s). This work is published and licensed by Dove Medical Press Limited. The
full terms of this license are available at https://www.dovepress.com/terms
and incorporate the Creative Commons Attribution
- Non Commercial (unported, 4.0) License.
By accessing the work you hereby accept the Terms. Non-commercial uses of the work are permitted
without any further permission from Dove Medical Press Limited, provided the work is properly
attributed. For permission for commercial use of this work, please see paragraphs 4.2 and 5 of our Terms.