Back to Journals » International Journal of Women's Health » Volume 17
Risk Factors and a Preliminary Clinical Prediction Model for Postpartum Hemorrhage or the Need for Hemostatic Intervention in Twin Cesarean Deliveries
Authors Lei ZL ![]()
Received 19 July 2025
Accepted for publication 8 October 2025
Published 11 October 2025 Volume 2025:17 Pages 3641—3653
DOI https://doi.org/10.2147/IJWH.S554953
Checked for plagiarism Yes
Review by Single anonymous peer review
Peer reviewer comments 2
Editor who approved publication: Dr Matteo Frigerio
Zinan L Lei
Department of Obstetrics and Gynecology, Mianyang Central Hospital, Mianyang, Sichuan, People’s Republic of China
Correspondence: Zinan L Lei, Email [email protected]
Objective: Postpartum hemorrhage (PPH) remains the leading cause of maternal mortality globally. Twin pregnancies demonstrate significantly higher PPH risk compared to singleton gestations. The predictive capacity for PPH in twin pregnancies requires improvement. This study conducted a retrospective analysis of clinical cases involving twin pregnancies delivered by cesarean section to determine risk factors for PPH or required hemostatic interventions and to construct a preliminary prediction model. The findings aim to enhance clinical anticipation and management of PPH in twin cesarean deliveries.
Methods: This retrospective study analyzed twin pregnancies delivered by cesarean section with live births at Mianyang Central Hospital from March 6, 2020 to March 6, 2025. The primary outcome was postpartum hemorrhage, defined as a blood loss of≥ 1000 mL within 24 hours after delivery, or the requirement for hemostatic intervention. Risk factors were identified using logistic regression analysis. Based on these factors, a preliminary clinical prediction model was developed, visualized as a nomogram, and internally validated.
Results: Multivariate analysis revealed six independent risk factors (all P< 0.05): first twin birth weight (P=0.018), second twin amniotic fluid depth (P=0.042), prolonged operative time (P=0.008), employed status (P=0.016), placenta implantation (P=0.009), and general anesthesia (P=0.019). We developed a clinical nomogram incorporating these six independent risk factors. The prediction model demonstrated moderate discriminative ability in the training set (AUC=0.722, 95% CI: 0.656– 0.789) and clinically relevant predictive value in the validation set (AUC=0.613, 95% CI: 0.503– 0.722).
Conclusion: This study successfully identified independent risk factors for postpartum hemorrhage or the need for hemostatic intervention in twin cesarean deliveries and preliminarily established a clinical nomogram prediction model, aiming to facilitate early detection and management of high-risk populations for bleeding in twin cesarean sections.
Keywords: postpartum hemorrhage, twins, cesarean section, risk factors
Introduction
Postpartum hemorrhage (PPH) constitutes the leading cause of maternal mortality worldwide, accounting for approximately 25% of all maternal deaths. Beyond its life-threatening nature, PPH may precipitate severe complications including adult respiratory distress syndrome (ARDS), hemorrhagic shock, disseminated intravascular coagulation (DIC), acute renal failure, reproductive disability, Sheehan’s syndrome (pituitary necrosis), and psychological trauma.1–3 Postpartum hemorrhage (PPH) is quantitatively defined as blood loss exceeding 500mL following vaginal delivery or 1000mL during cesarean delivery. Cesarean delivery carries a significantly higher risk of hemorrhage compared to vaginal birth.4 The pathogenesis of postpartum hemorrhage has been clearly established to include four main mechanisms: uterine atony, placental factors, coagulation disorders, and birth canal trauma. With the increasing use of assisted reproductive technologies and rising maternal age, the incidence of twin pregnancies continues to grow. In twin pregnancies, overstretching of uterine fibers leads to weakened contractions, while the larger placental attachment area increases bleeding risk from placental factors, resulting in significantly higher postpartum hemorrhage risk compared to singleton pregnancies.5,6 Additionally, twin pregnancies demonstrate a higher rate of cesarean delivery and a greater potential for rapid blood loss. These differences reflect fundamentally distinct mechanisms of postpartum hemorrhage (PPH), indicating that risk factors for PPH in twins may not be directly extrapolated from models based on singleton pregnancy data. Owing to the lack of specialized data, clinical practice and research have frequently been compelled to extrapolate conclusions from singleton pregnancies to twin gestations. Current management of postpartum hemorrhage (PPH) following twin cesarean deliveries predominantly relies on protocols derived from singleton pregnancies or adopts reactive measures (initiating intervention only after hemorrhage occurs). This study redirects focus to the unique and exacerbated pathophysiological state characteristic of twin pregnancies, specifically examining the differential impacts of individual fetal weights and amniotic fluid depth on PPH risk. Collectively, our findings establish a critical evidence base for developing twin-specific, proactive risk management protocols.
While Corbetta-Rastelli et al reported that 73.8% of deliveries complicated by postpartum hemorrhage (PPH) lacked identifiable risk factors,7 the potentially severe consequences of PPH nevertheless necessitate continued investigation into potential predictors. It is essential to identify high-risk women who may benefit from intensified prevention and treatment protocols.8 This retrospective cohort study aimed to investigate the independent risk factors for postpartum hemorrhage or the need for hemostatic intervention in twin cesarean deliveries and to preliminarily develop a risk prediction model, with the ultimate goal of assisting obstetricians in formulating individualized hemostatic strategies.
Materials and Methods
We conducted a retrospective analysis of electronic medical records for 471 twin pregnancies undergoing cesarean delivery at Mianyang Central Hospital between March 6, 2020 and March 6, 2025. The final study cohort consisted of 345 patients, with 241 allocated to the training set and 104 to the validation set, Figure 1. The initial selection of variables was based on general demographic characteristics, including maternal height, weight, body mass index (BMI), and age. All BMI values were measured within 3 days prior to delivery. Based on established risk factors for postpartum hemorrhage (PPH) documented in previous literature, and considering the unique pathophysiological mechanisms of twin pregnancies combined with clinical expertise, the following variables were incorporated: occupation, gestational age at delivery, gravidity, parity, fetal weight, amniotic fluid volume, maximum vertical pocket, platelet count, hemoglobin, fibrinogen, Prothrombin Time - International Normalized Ratio (PT-INR), operative time frame and duration, surgeon experience, tocolytic use, aspirin administration, embryo transfer, diabetes, hypertension, premature rupture of membranes, intrahepatic cholestasis of pregnancy, uterine fibroids or adenomyosis, placenta previa, placental abruption, placenta accreta spectrum, uterine scar, anterior placental attachment, general anesthesia, emergency cesarean delivery, preterm birth, fetal sex, and neonatal intensive care unit admission. We assessed postpartum blood loss using a combination of volumetric collection and gravimetric measurement. The volume of amniotic fluid aspirated by the suction device after amniotomy was recorded separately. All ultrasonographic measurements were obtained within 3 days prior to delivery. The single deepest pocket (SDP) method was selected over the amniotic fluid index (AFI) due to its operational simplicity, reduced susceptibility to subjective interpretation, and enhanced capability to accurately identify regional uterine wall tension. Preoperative hematological parameters were collected within 3 days before cesarean delivery, while postoperative hemoglobin levels were measured on postoperative day 3 to eliminate the confounding effects of hemoconcentration. Postpartum hemorrhage was defined as a blood loss of ≥1000 mL within 24 hours after delivery or a postoperative hemoglobin drop of ≥25 g/L. The composite outcome also included the requirement for hemostatic intervention, defined as the occurrence of any of the following procedures: uterine artery ligation, intrauterine tamponade, blood transfusion, or hysterectomy. Exclusion criteria comprised: cases with substantial missing data, gestational age <26 weeks, single or double intrauterine fetal demise, uterine rupture, or severe maternal organ dysfunction (including coagulopathy, severe hepatic/renal insufficiency, acute fatty liver of pregnancy, acute pancreatitis, severe cardiac disease, heart failure, or respiratory failure). Using a random seed number, the cohort was allocated into training (70%) and validation (30%) sets (Figure 1).
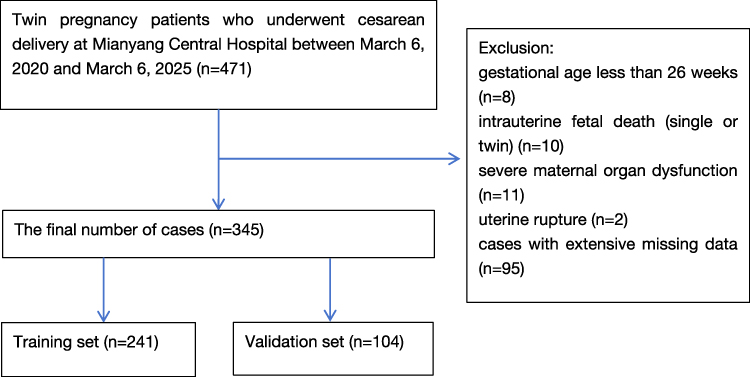 |
Figure 1 Flow chart. |
We implemented a rigorous statistical modeling protocol for risk factor analysis and predictive model development. Potential risk factors were initially screened through univariate logistic regression analysis, with statistically significant variables (P < 0.05) subsequently incorporated into multivariate logistic regression models. During the initial modeling process, we observed that the factor “emergency cesarean delivery” exhibited a variance inflation factor (VIF) greater than 10. To ensure the stability and interpretability of the model results, this variable was excluded from the multivariate analysis. Ultimately, independent risk factors for postpartum hemorrhage or haemostatic intervention in twin cesarean deliveries were identified. Based on the independent risk factors, we constructed a clinical prediction nomogram to visually demonstrate variable weights and their contribution to outcomes. Model predictive accuracy was assessed using receiver operating characteristic (ROC) curves, with calculation of the area under the curve (AUC) and 95% confidence intervals (CI). Calibration curves and Hosmer-Lemeshow goodness-of-fit tests evaluated the agreement between predicted and observed probabilities. The Hosmer-Lemeshow goodness-of-fit test classifies observations into ten groups of equal frequency based on deciles of predicted probabilities. It then computes a chi-square statistic by comparing predicted and observed event frequencies across these groups. A nonsignificant result (P > 0.05) suggests good model calibration. Decision curve analysis (DCA) was employed to assess clinical net benefit across various decision thresholds, thereby determining the model’s clinical utility. All statistical analyses were performed using R statistical software (version 4.3.2). Specifically, we utilized the following packages: the “rms” package for logistic regression, nomogram construction, and calibration plots; the “pROC” package for generating ROC curves; the “vcdExtra” package for conducting Hosmer-Lemeshow tests; and the “dcurves” package for decision curve analysis (DCA) to evaluate the clinical net benefit across various thresholds. Statistical tests were two-tailed, with P <0.05 considered statistically significant.
Results
The baseline characteristics of the study population, stratified by the presence of postpartum hemorrhage or hemostatic intervention, are presented in Table 1. Except for variables such as amniotic fluid volume, use of tocolytics, premature rupture of membranes, preterm birth, and anterior placenta, which showed imbalances between the groups, the remaining variables were well-balanced. Univariate logistic regression analysis identified several potential risk factors associated with postpartum hemorrhage or hemostatic intervention, including fetal weight 1, amniotic fluid depth of fetus 2, total amniotic fluid depth, duration of surgery, employment status, placental abruption, placenta accreta, placenta previa, general anesthesia, and emergency cesarean delivery, as detailed in Table 2.
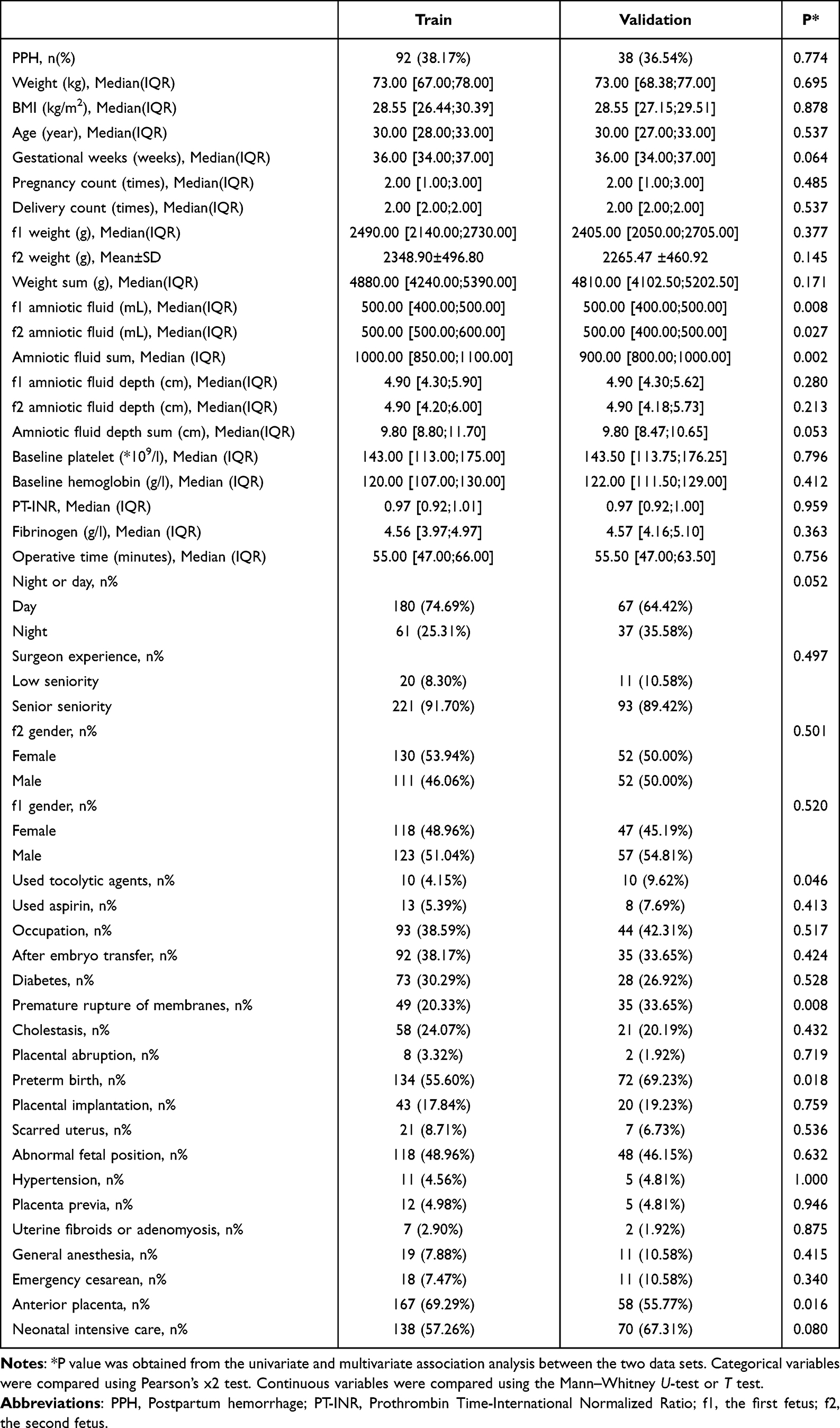 |
Table 1 Baseline Table |
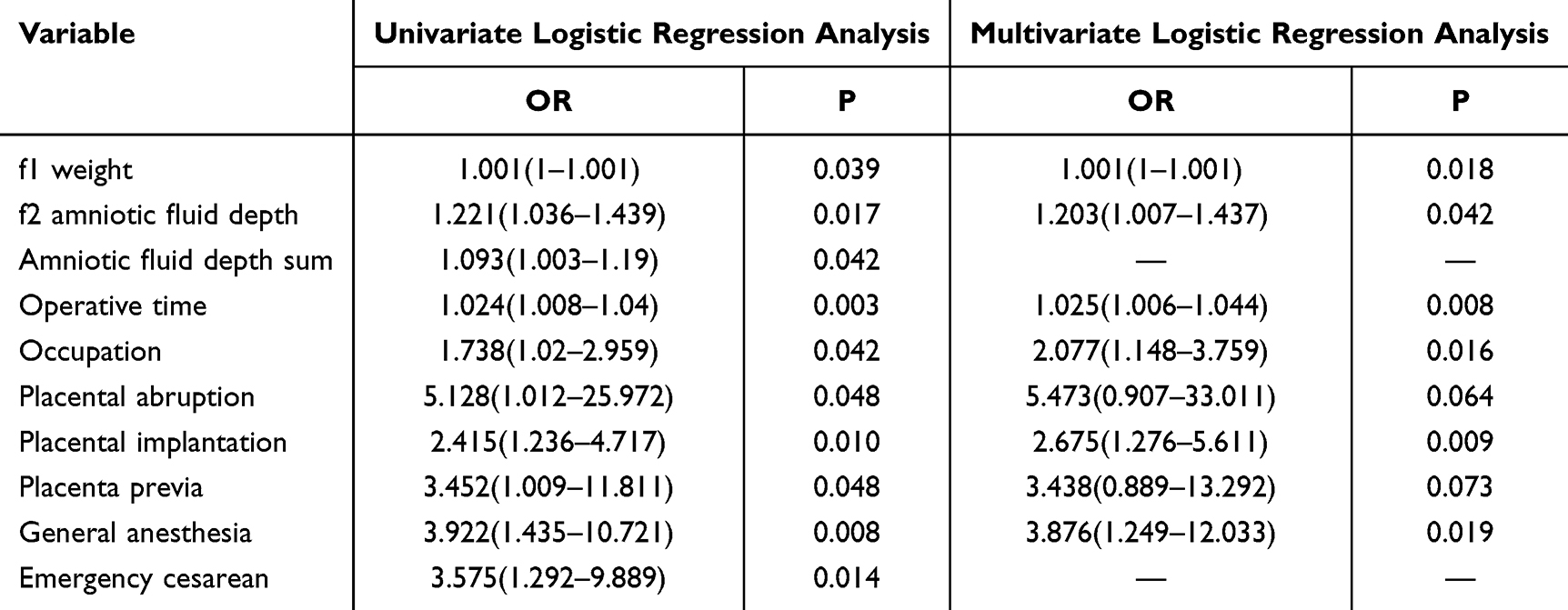 |
Table 2 Univariate and Multivariate Logistic Regression Analysis |
After excluding emergency cesarean delivery due to multicollinearity, the remaining variables were incorporated into a multivariate regression model for further adjustment. The final multivariate model, also shown in Table 2, revealed that fetal weight 1, amniotic fluid depth of fetus 2, duration of surgery, employment status, placenta accreta, and general anesthesia were independent risk factors. Among these, general anesthesia demonstrated the strongest association (aOR: 3.876, 95% CI: 1.249–12.033; P = 0.019), followed by placenta accreta (aOR: 2.675, 95% CI: 1.276–5.611; P = 0.009). Other significant independent risk factors included fetal weight 1 (aOR: 1.001, 95% CI: 1.000–1.001; P = 0.018), amniotic fluid depth of fetus 2 (aOR: 1.203, 95% CI: 1.007–1.437; P = 0.042), duration of surgery (aOR: 1.025, 95% CI: 1.006–1.044; P = 0.008), and employment status (aOR: 2.077, 95% CI: 1.148–3.759; P = 0.016). In contrast, total amniotic fluid depth, placental abruption, and placenta previa, which were significant in the univariate analysis, did not retain statistical significance after multivariate adjustment.
Based on these factors, we developed a visual scoring tool (nomogram) for individualized assessment of hemorrhage risk, Figure 2. The prediction model demonstrated moderate discriminative ability in the training dataset, with an area under the receiver operating characteristic curve (AUC) of 0.722 (95% confidence interval [CI]: 0.656–0.789), Figure 3. In the validation cohort, the nomogram maintained discriminative capacity with an AUC of 0.613 (95% CI: 0.503–0.722), Figure 4. In the training set, the Hosmer-Lemeshow goodness-of-fit test revealed satisfactory calibration between predicted and observed outcomes (χ²=3.92, df =8, p =0.865), indicating good agreement between predicted and actual risks, Figure 5. In the validation set, the test showed no significant deviation (χ²=7.20, df =8, p=0.515), confirming adequate calibration, Figure 6. In the training set, Decision curve analysis (DCA) showed that when the clinical decision threshold was set at≥7%, the predictive model provided greater net clinical benefit compared to either treating all or no patients, Figure 7. For the validation set, the model exhibited multiple threshold ranges (9–26%, 33–42%, and 82–87%) where the model provided net benefit, suggesting clinical utility for risk stratification of postpartum hemorrhage in different patient subgroups, Figure 8.
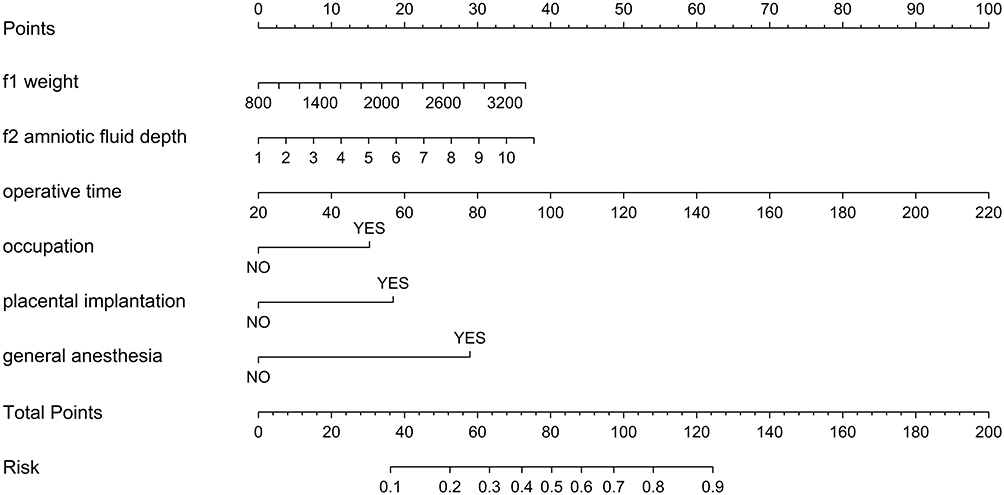 |
Figure 2 Clinical Nomogram for Predicting Postpartum Hemorrhage or Hemorrhage-Associated Intervention in Twin Cesarean Deliveries, with a Total Nomogram Score Range of 0 to 200 Points. |
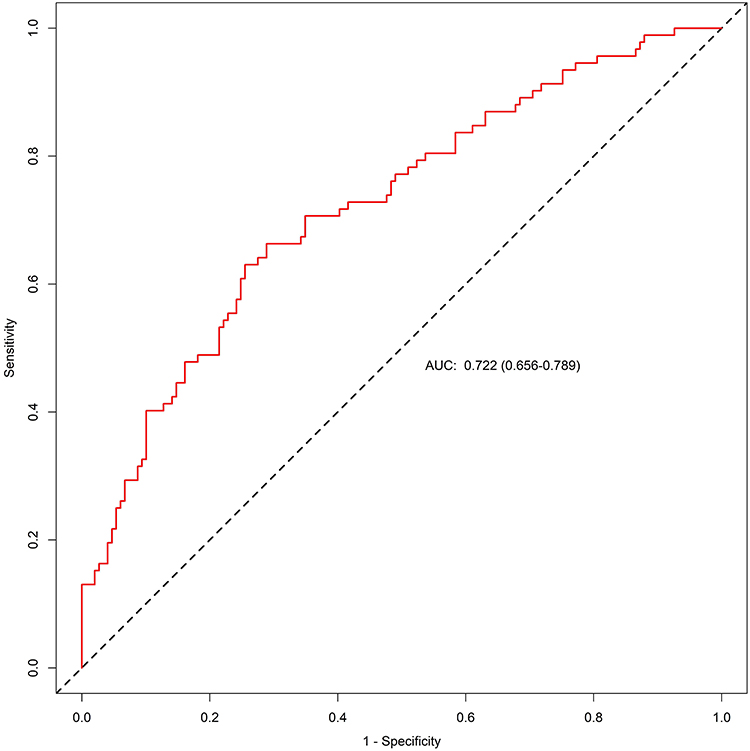 |
Figure 3 Receiver operating characteristic (ROC) curves of the nomogram in the training set. Abbreviation: AUC, area under the curve. |
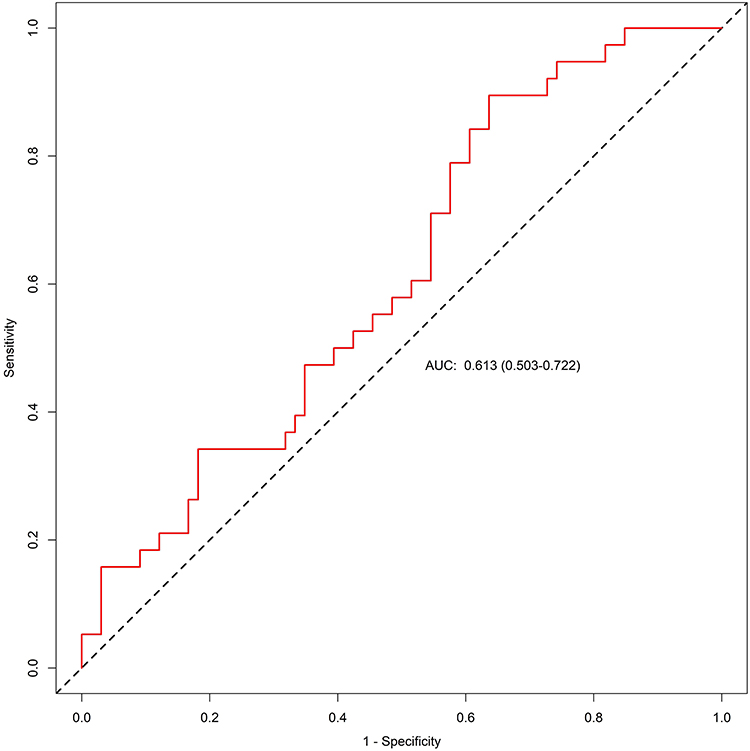 |
Figure 4 Receiver operating characteristic (ROC) curves of the nomogram in the validation set. |
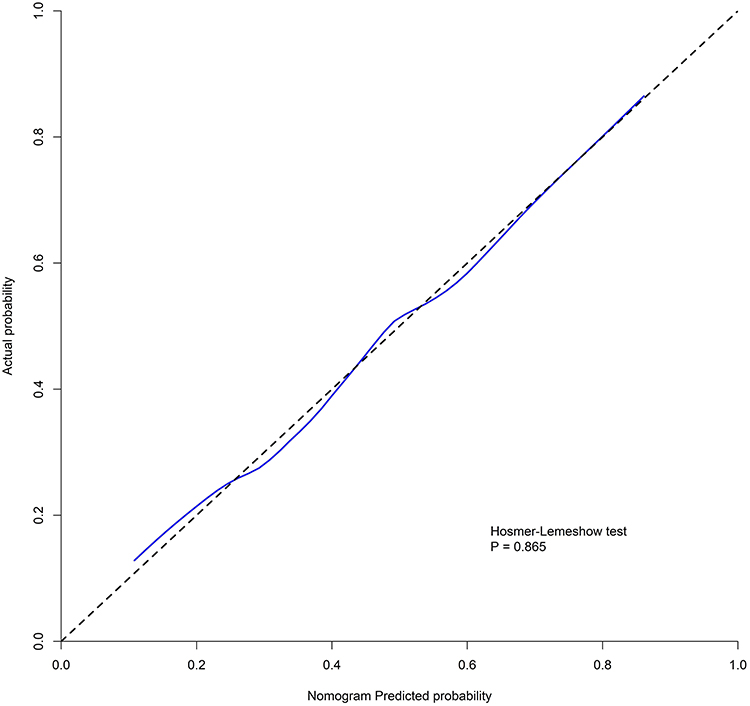 |
Figure 5 Calibration curves of the nomogram in the training set. |
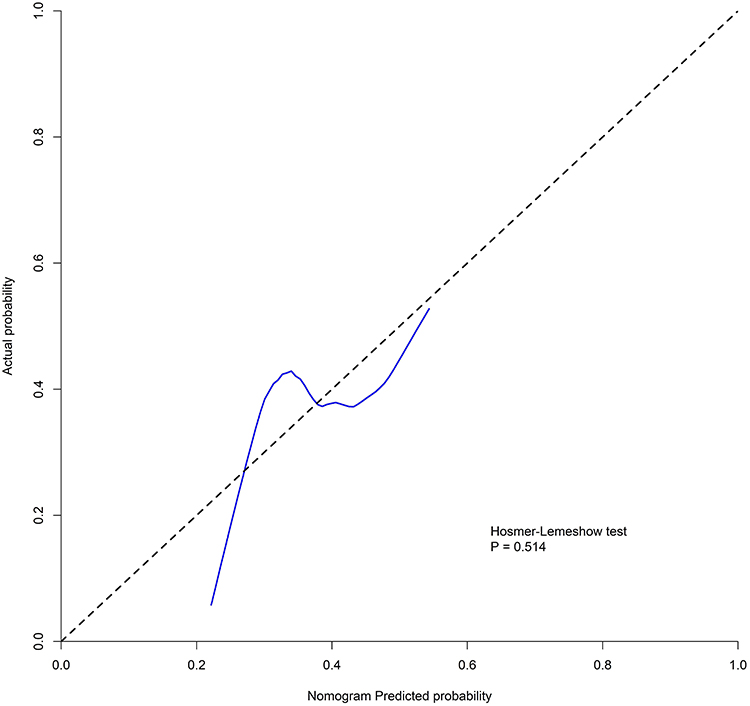 |
Figure 6 Calibration curves of the nomogram in the validation set. |
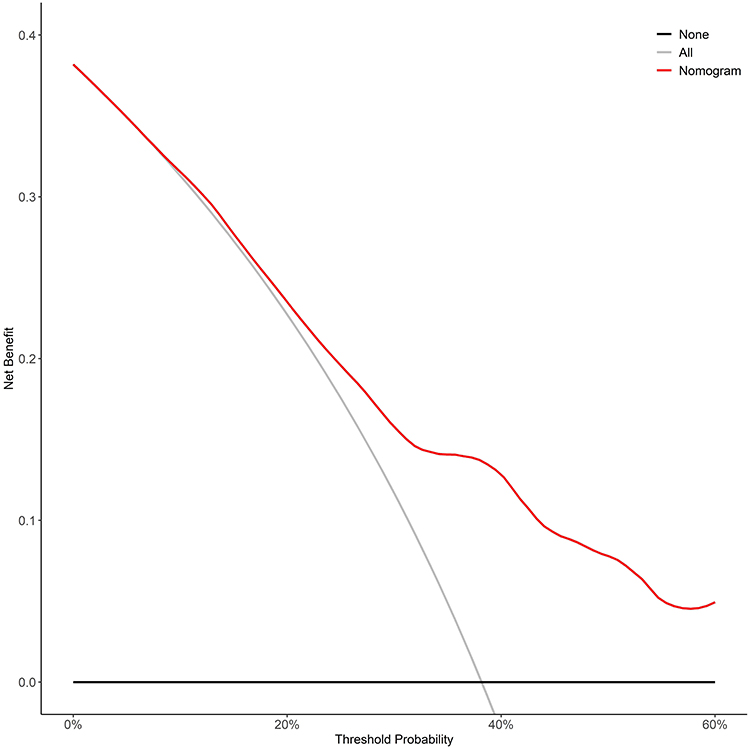 |
Figure 7 Decision curve analysis of the clinical nomogram in the training set. |
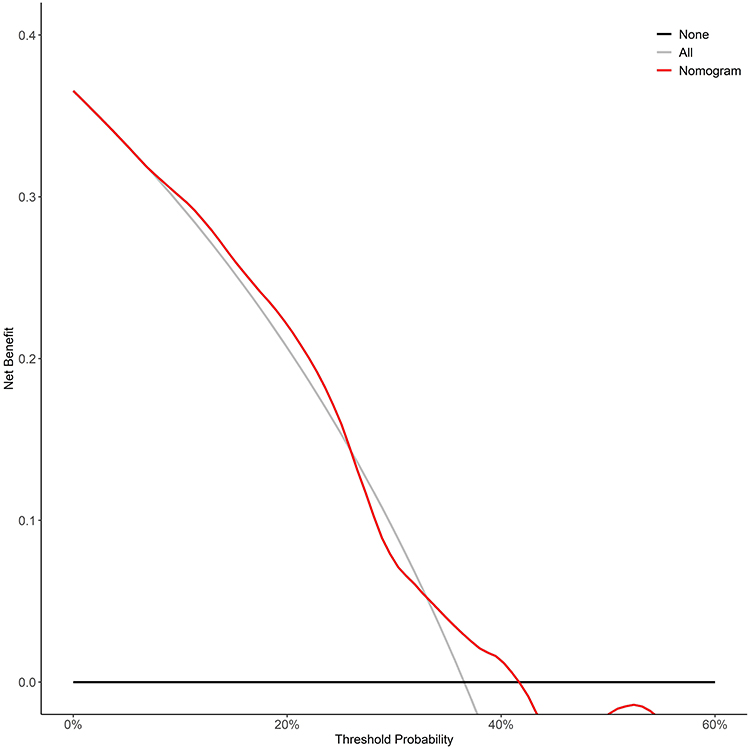 |
Figure 8 Decision curve analysis of the clinical nomogram in the validation set. |
Discussion
Loussert et al found that fetal weight is a risk factor for uterine atony by inducing uterine overdistension, with every 500g increase in total birth weight associated with a 36% increased risk.9 Cao et al found that in dichorionic twin pregnancies, fetal growth discordance, especially when combined with fetal growth restriction, was associated with an increased risk of postpartum hemorrhage after cesarean delivery. They observed an association between placental histological abnormalities and birth weight discordance, which may contribute to the mechanism of postpartum hemorrhage.10 Our study identified the birth weight of the first delivered twin as a risk factor for postpartum hemorrhage or hemostatic intervention in twin cesarean deliveries. This may be related to uterine atony caused by uterine overdistension. Additionally, larger fetal size is often associated with greater placental surface area, resulting in more bleeding after placental separation. Moreover, obstetricians may need to make larger uterine incisions to deliver larger fetuses, thereby increasing the risk of incision-related bleeding.
Current literature contains limited investigations regarding occupational factors and postpartum hemorrhage risk. Watkins et al examined the association between occupational physical exertion and postpartum hemorrhage, demonstrating no statistically significant difference in hemorrhage risk when comparing groups with higher versus lower occupational activity scores.11 Although our multivariate model identified employment status as an independent factor associated with the outcome (aOR: 2.077, 95% CI: 1.148–3.759; p = 0.016), the causal pathway underlying this association remains unclear. It is unlikely that employment status per se represents a direct biological cause, but rather it may serve as a proxy for other unmeasured or residual socioeconomic, nutritional, or psychological confounders—such as occupational stress, physical job demands, or access to prenatal care. This finding underscores the potential importance of socioeconomic factors in perinatal outcomes and warrants further investigation using more granular data on job type, work environment, and social support to better understand the nature of this relationship.
Amniotic fluid volume is rigorously regulated, with disturbances potentially indicating maternal or fetal abnormalities. Ultrasonographic assessment of amniotic fluid serves as a real-time monitoring tool for evaluating the maternal-fetal-placental unit. Whittington et al found that both polyhydramnios and oligohydramnios were associated with increased rates of cesarean delivery and elevated risks of postpartum hemorrhage.12 A meta-analysis demonstrated that idiopathic polyhydramnios is associated with an increased risk of perinatal complications, particularly postpartum hemorrhage (RR 1.98, 95% CI 1.22–3.22; I² = 84%).13 Aviram et al conducted a retrospective cohort study in singleton pregnancies demonstrating that mild polyhydramnios was significantly associated with an increased cesarean delivery rate: 12.1% versus 5.1% (OR=2.6, 95% CI 1.7–4.0).14 Another prospective cohort study in singleton pregnancies demonstrated significantly elevated risks of postpartum hemorrhage (7.8% vs 2.2%; OR: 1.60; 95% CI: 1.09–2.34) and cesarean delivery (51.11% vs 21.11%; OR: 1.88; 95% CI: 1.42–2.50) in cases with idiopathic polyhydramnios (P<0.05).15 The authors proposed that polyhydramnios may lead to uterine overdistension and subsequent uterine atony. This study demonstrated that increased amniotic fluid depth in the second twin was associated with higher postpartum hemorrhage risk in twin pregnancies. The potential mechanisms may involve uterine atony caused by overdistension and greater blood loss from the placental separation surface due to increased traction on the umbilical cord and placenta following membrane rupture when amniotic fluid volume is larger.
Previous studies have demonstrated that prolonged operative time during primary cesarean delivery is significantly associated with both extended duration of subsequent cesarean procedures and increased risk of postpartum hemorrhage.16 Our study identified prolonged operative time as an independent risk factor for postpartum hemorrhage (OR 1.025, 95% CI 1.006–1.044; P=0.008). This association may be attributed to factors such as surgeon inexperience, prolonged adhesiolysis, and suboptimal hemostatic techniques. Furthermore, hemorrhage itself may necessitate additional time for hemostatic procedures, potentially exacerbating the duration-risk relationship. We recommend maintaining surgical quality while minimizing operative time to reduce hemorrhage risk.
Moroz et al reported that accelerated surgical intervention (defined as ≤2 minutes from skin incision to fetal delivery) was associated with increased risks of maternal blood transfusion (6.5% vs 1.8%, P<0.01), uterine artery ligation (8.3% vs 1.5%, P<0.01), and broad ligament hematoma formation (3.7% vs 0.4%, P<0.01).17 Emergency cesarean delivery was the only factor in this study that demonstrated severe multicollinearity. This finding is clinically expected, as emergency cesarean sections typically represent management endpoints for various obstetric complications and are inherently strongly correlated with multiple pathological conditions. This suggests that the risk associated with emergency cesarean delivery is largely attributable to its underlying obstetric indications rather than representing an independent risk factor per se. Consequently, emergency cesarean delivery was excluded from the final model to prevent multicollinearity from compromising the stability of parameter estimates.
Multiple studies have identified general anesthesia as a risk factor for postpartum hemorrhage. Volatile anesthetics can induce significant uterine relaxation, leading to dose-dependent uterine atony. Furthermore, potential confounding cannot be entirely ruled out, as anesthesiologists may preferentially select general anesthesia for patients at higher risk of postpartum hemorrhage.4,18,19 In our study, general anesthesia emerged as an independent risk factor for postpartum hemorrhage (OR 3.876, 95% CI 1.249–12.033; P=0.019), consistent with previous research findings.
Postpartum hemorrhage has been well-established to be significantly associated with placental abnormalities, including placenta previa, placental abruption, and placenta implantation, based on previous studies.8,20 Placenta previa frequently coexists with placenta implantation. The combination of low placental implantation and thin lower uterine segment with poor contractility often leads to inadequate closure of venous sinuses after placental separation. Placental abruption may contribute to postpartum hemorrhage through multiple mechanisms: bleeding from the detachment site, uterine atony, and coagulation disorders. In our study, placenta implantation was identified as an independent risk factor for postpartum hemorrhage or hemostatic Intervention following twin cesarean delivery (OR 2.675, 95% CI 1.276–5.611; P=0.009). These findings underscore the critical importance of vigilant clinical management of placental abnormalities due to their significant hemorrhagic potential.
Clinically, the integration of risk assessment tools within electronic medical record systems, coupled with automated intervention triggers, could significantly enhance diagnostic and therapeutic decision-making capacity.21 This would require engineering support to configure the EMR to automatically pull key variables—such as fetal weight, amniotic fluid depth, planned anesthesia method, ultrasonographic placental findings, and employment status—from structured data fields during the perinatal period. A backend calculation engine would then generate individualized risk scores, triggering instant clinical decision support alerts. By facilitating early recognition and proactive management, this integrated approach aims to improve outcomes and reduce the severity of postpartum hemorrhage.
Strengths and Limitations
This study investigates risk factors for postpartum hemorrhage (PPH) following twin cesarean deliveries and establishes a preliminary prediction model, addressing a knowledge gap in current literature which predominantly focuses on singleton pregnancies. Utilizing clinically accessible variables, our findings reveal several novel risk factors beyond established placental factors and previously reported general anesthesia risks. Specifically, we identified increased fetal weight, greater amniotic fluid depth, longer operation duration and maternal occupational status as significant contributors to PPH risk in twin pregnancies. These evidence-based insights provide valuable guidance for clinical decision-making. However, this study has several limitations. First, its single-center retrospective design and relatively limited sample size (345 cases) may restrict the generalizability and broader applicability of the findings. The performance of our preliminary prediction model decreased in the validation set, with the AUC declining from 0.722 to 0.613. Although the model demonstrates some clinical relevance, its predictive ability remains limited. Potential reasons may include the single-center retrospective design, a relatively small sample size, and insufficient specificity of the predictor variables. Additionally, predicting postpartum hemorrhage in twin deliveries remains particularly challenging due to the clinically complex and multifactorial nature of this obstetric emergency. The generalizability of the predictive model and risk factors identified in this study requires further validation in broader, multi-center prospective cohorts. Future investigations should aim to incorporate machine learning methods for integrating multivariate data to develop more accurate and individualized risk stratification systems. The inclusion of genetic markers could offer additional predictive refinement and enhance clinical applicability.
Conclusion
The present study identified six independent predictors of postpartum hemorrhage following twin cesarean delivery: birth weight of the first twin, amniotic fluid depth of the second twin, duration of surgery, maternal occupation, presence of placenta accreta, and use of general anesthesia. While these findings are clinically informative and generate important hypotheses, the model’s predictive utility requires confirmation in multi-center, prospective studies before it can be recommended for widespread clinical application. Consequently, these results should be interpreted as a foundation for future research rather than for direct clinical implementation. Ultimately, validating and refining this model could help inform targeted surveillance protocols and individualized management strategies for at-risk pregnancies, with the goal of reducing hemorrhagic complications and improving perinatal outcomes in twin gestations.
Data Sharing Statement
The data that support the findings of this study are available on request from the corresponding author.
Ethics Approval and Consent to Participate
All procedures performed in the study involving human participants conform to the 1964 helsinki Declaration and its later amendments or comparable ethical standards. This study received ethics approval from the Human Ethics Committee of Mianyang Central Hospital, (Approval No. 20250207×2). Additionally, this is a retrospective study; no interventions were applied to the subjects, so written informed consent from participants is not required.
Acknowledgments
The author sincerely thanks all study participants and acknowledges the essential contributions of the information center personnel in facilitating data acquisition for this research.
Author Contributions
All authors made a significant contribution to the work reported, whether that is in the conception, study design, execution, acquisition of data, analysis and interpretation, or in all these areas; took part in drafting, revising or critically reviewing the article; gave final approval of the version to be published; have agreed on the journal to which the article has been submitted; and agree to be accountable for all aspects of the work.
Funding
This research received no specific grant from any funding agency in the public, commercial, or not-for-profit sectors.
Disclosure
The author declares no known competing financial interests or personal relationships that could influence the content reported in this study.
References
1. Shields LE, Goffman D, Caughey AB. Practice bulletin No. 183: postpartum hemorrhage. Obstetrics Gynecol. 2017;130(4):e168–e186. doi:10.1097/AOG.0000000000002351
2. Giouleka S, Tsakiridis I, Kalogiannidis I, et al. Postpartum hemorrhage: a comprehensive review of guidelines. Obstetrical Gynecol Surv. 2022;77(11):665–682. doi:10.1097/OGX.0000000000001061
3. Hofer S, Blaha J, Collins PW, et al. Haemostatic support in postpartum haemorrhage: a review of the literature and expert opinion. European J Anaesthesiol. 2023;40(1):29–38. doi:10.1097/EJA.0000000000001744
4. Waterstone M, Bewley S, Wolfe C. Incidence and predictors of severe obstetric morbidity: case-control study. BMJ. 2001;322(7294):1089–1093. discussion 1093-1084. doi:10.1136/bmj.322.7294.1089
5. Li S, Gao J, Liu J, et al. Incidence and risk factors of postpartum hemorrhage in China: a multicenter retrospective study. Front Med. 2021;8:673500. doi:10.3389/fmed.2021.673500
6. Wan X, Zhao W, Zhao L, Li N, Wen H. Risk factors for postpartum hemorrhage after elective cesarean deliveries for twin pregnancies. Ginekologia polska. 2024;95(7):531–535. doi:10.5603/GP.a2023.0071
7. Corbetta-Rastelli CM, Friedman AM, Sobhani NC, Arditi B, Goffman D, Wen T. Postpartum hemorrhage trends and outcomes in the United States, 2000-2019. Obstetrics Gynecol. 2023;141(1):152–161. doi:10.1097/AOG.0000000000004972
8. Yunas I, Islam MA, Sindhu KN, et al. Causes of and risk factors for postpartum haemorrhage: a systematic review and meta-analysis. Lancet. 2025;405(10488):1468–1480. doi:10.1016/S0140-6736(25)00448-9
9. Loussert L, Schmitz T, Korb D, et al. Risk of severe postpartum hemorrhage in twin pregnancies according to the sum of birth weights. Obstetrics Gynecol. 2022;140(6):958–964. doi:10.1097/AOG.0000000000004993
10. Cao X, Luo Y, Zhou S, et al. Twin growth discordance and risk of postpartum hemorrhage: a retrospective cohort study. Front Med. 2022;9:876411. doi:10.3389/fmed.2022.876411
11. Watkins VY, O’Donnell CM, Perez M, et al. The impact of physical activity during pregnancy on labor and delivery. Am J Clin Exp Obstet Gynecol. 2021;225(4):
12. Whittington JR, Ghahremani T, Friski A, Hamilton A, Magann EF. Window to the womb: amniotic fluid and postnatal outcomes. Int J Women’s Health. 2023;15:117–124. doi:10.2147/IJWH.S378020
13. Kechagias KS, Triantafyllidis KK, Zouridaki G, Savvidou M. Obstetric and neonatal outcomes in pregnant women with idiopathic polyhydramnios: a systematic review and meta-analysis. Sci Rep. 2024;14(1):5296. doi:10.1038/s41598-024-54840-0
14. Aviram A, Salzer L, Hiersch L, et al. Association of isolated polyhydramnios at or beyond 34 weeks of gestation and pregnancy outcome. Obstetrics Gynecol. 2015;125(4):825–832. doi:10.1097/AOG.0000000000000740
15. Vanda R, Bazrafkan M, Rouhani M, Bazarganipour F. Comparing pregnancy, childbirth, and neonatal outcomes in women with idiopathic polyhydramnios: a prospective cohort study. BMC Pregnancy Childbirth. 2022;22(1):399. doi:10.1186/s12884-022-04625-y
16. Lang Ben Nun E, Sela HY, Joseph J, Rudelson G, Grisaru-Granovsky S, Rottenstreich M. Prolonged operative time of cesarean is a risk marker for subsequent cesarean maternal complications. Arch Gynecol Obstetrics. 2023;307(3):739–746. doi:10.1007/s00404-022-06575-4
17. Moroz L, DiNapoli M, D’Alton M, Gyamfi-Bannerman C. Surgical speed and risk for maternal operative morbidity in emergent repeat cesarean delivery. Am J Clin Exp Obstet Gynecol. 2015;213(4):
18. Lan Y, Xu A, Lu X, et al. Risk factors for postpartum hemorrhage in twin pregnancies with cesarean section. Front Med. 2023;10:1301807. doi:10.3389/fmed.2023.1301807
19. Seo GH, Kim JY, Lee DY, Lee C, Lee J. Risk factors for severe postpartum hemorrhage requiring blood transfusion after cesarean delivery for twin pregnancy: a nationwide cohort study. Anesthesia Pain Med. 2023;18(4):367–375. doi:10.17085/apm.23019
20. Liu CN, Yu FB, Xu YZ, et al. Prevalence and risk factors of severe postpartum hemorrhage: a retrospective cohort study. BMC Pregnancy Childbirth. 2021;21(1):332. doi:10.1186/s12884-021-03818-1
21. Ende HB. Risk assessment tools to predict postpartum hemorrhage. Best Pract Res Clin Anaesth. 2022;36(3–4):341–348. doi:10.1016/j.bpa.2022.08.003
 © 2025 The Author(s). This work is published and licensed by Dove Medical Press Limited. The
full terms of this license are available at https://www.dovepress.com/terms
and incorporate the Creative Commons Attribution
- Non Commercial (unported, 4.0) License.
By accessing the work you hereby accept the Terms. Non-commercial uses of the work are permitted
without any further permission from Dove Medical Press Limited, provided the work is properly
attributed. For permission for commercial use of this work, please see paragraphs 4.2 and 5 of our Terms.
© 2025 The Author(s). This work is published and licensed by Dove Medical Press Limited. The
full terms of this license are available at https://www.dovepress.com/terms
and incorporate the Creative Commons Attribution
- Non Commercial (unported, 4.0) License.
By accessing the work you hereby accept the Terms. Non-commercial uses of the work are permitted
without any further permission from Dove Medical Press Limited, provided the work is properly
attributed. For permission for commercial use of this work, please see paragraphs 4.2 and 5 of our Terms.
Recommended articles
Risk Factors for Postpartum Hemorrhage Following Vaginal Deliveries in China: A Case-Control Study of Second Births After IUD Removal
Shen L, Xu Y, Li B, Long Y
International Journal of Women's Health 2025, 17:1203-1214
Published Date: 1 May 2025