Back to Journals » International Medical Case Reports Journal » Volume 18
Right Internal Jugular Vein Access for Micra Leadless Pacemaker Implantation in a High-Risk Patient with Severe Iliac Vein Stenosis: A Case Report
Authors Xu H, Qian J ![]() , Pan W
, Pan W ![]() , Fan J
, Fan J ![]()
Received 21 March 2025
Accepted for publication 14 June 2025
Published 19 June 2025 Volume 2025:18 Pages 727—733
DOI https://doi.org/10.2147/IMCRJ.S529596
Checked for plagiarism Yes
Review by Single anonymous peer review
Peer reviewer comments 3
Editor who approved publication: Dr Vinay Kumar
Haixiang Xu, Jianfeng Qian, Wen Pan, Jianhua Fan
Department of Cardiology, Kunshan Hospital of Traditional Chinese Medicine Affiliated to Yangzhou University, Suzhou, People’s Republic of China
Correspondence: Jianhua Fan, Department of Cardiology, Kunshan Hospital of Traditional Chinese Medicine Affiliated to Yangzhou University, Suzhou, People’s Republic of China, Email [email protected]
Background: Leadless pacemakers offer a promising alternative to traditional transvenous pacemakers, especially in patients with complex vascular anatomy or a high risk of infection. Conventional access routes may be compromised in patients with significant venous stenosis or prior vascular interventions, requiring alternative strategies for device implantation.
Case Presentation: We report the case of a 74-year-old female with sick sinus syndrome, chronic kidney disease, type 2 diabetes, and severe bilateral iliac vein stenosis, who was deemed high-risk for conventional pacemaker implantation. After failed attempts through both femoral veins, the right internal jugular vein (RIJV) was successfully used as an alternative access route for Micra leadless pacemaker implantation. The procedure was performed under ultrasound and fluoroscopic guidance without complications. Post-procedure, the pacing threshold was 0.75 V, sensing was 8.5 mV, and impedance was 760 Ω, all within normal limits.
Conclusion: This case highlights the feasibility and safety of using the right internal jugular vein as an alternative access route for leadless pacemaker implantation in high-risk patients when femoral access is not possible. This approach provides a valuable option for patients with complex venous anatomy, contributing to the broader application of leadless pacing technology.
Keywords: micra leadless pacemaker, right internal jugular vein, iliac vein stenosis, high-risk patient, alternative access
Introduction
Cardiac pacing has long been considered a fundamental therapeutic approach for managing various bradyarrhythmias, with the conventional transvenous pacemaker serving as the standard treatment modality for numerous years.1 Nonetheless, in patients presenting with complex comorbidities and intricate venous anatomy—particularly those with end-stage renal disease, diabetes mellitus, or a history of vascular interventions—traditional transvenous pacemakers may precipitate considerable complications, including lead dislodgement, venous thrombosis, device pocket hematoma, pneumothorax, and device infection, which can ultimately lead to device malfunction, need for extraction, or systemic complications such as endocarditis.2–4
As the number of patients with complex vascular anatomy increases, especially those with severe stenosis or occlusion of major veins, there is an urgent need for alternative, safe, and effective methods of device implantation. Leadless pacemakers, developed by several manufacturers including Medtronic, Abbott, and Boston Scientific, represent a substantial advancement in the domain of cardiac pacing.5 By obviating the necessity for lead wires and a subcutaneous pocket, this innovative technology provides a less invasive alternative, thereby mitigating the risk of infections and complications commonly associated with conventional pacemaker systems.6 This approach is particularly advantageous for high-risk patients—such as those with end-stage renal disease on hemodialysis, low body mass index, diabetes mellitus, prior central venous catheterization, or immunosuppression—who are more susceptible to these complications due to impaired vascular integrity and compromised immune status. Despite the considerable benefits of leadless pacemakers, their implantation poses certain challenges. The femoral vein is generally the preferred access route for these devices; however, this option may be hindered by vascular stenosis or other anatomical constraints.7 In such instances, it becomes imperative to explore alternative venous pathways to ensure the safe and effective placement of the device.8,9
This case report presents a novel and rare application of the right internal jugular vein access for Micra implantation in a high-risk patient with severe bilateral iliac vein stenosis and a high susceptibility to infections. This procedure, performed successfully under ultrasound and fluoroscopic guidance, demonstrates the feasibility and safety of this approach when conventional access routes are not available. This report adds to the growing body of evidence that supports the expanding use of leadless pacing technology in patients with complex vascular anatomy and provides valuable insight into a previously underexplored access route.
Case Presentation
A 74-year-old female presented with recurrent episodes of chest tightness and palpitations for two months. She was diagnosed with SSS, warranting permanent pacing therapy. Notably, her medical history was significant for chronic kidney disease with a five-year history of dialysis, type 2 diabetes mellitus for 20 years, renal anemia, and coronary artery disease with prior coronary stenting. Given her frail physical condition, with a body weight of only 40 kg, along with prolonged antiplatelet therapy, she was at high risk for conventional leaded pacemaker complications, including infection and device-related adverse events. Hence, a Micra leadless pacemaker was chosen as the preferred treatment approach.
Procedural Details
Under ultrasound guidance, we initially attempted right femoral vein access. Angiography, however, revealed significant stenosis of the right iliac vein (Figure 1). Subsequently, left femoral vein access was attempted, with similar findings of severe stenosis in the left iliac vein (Figure 2). Due to the bilateral iliac vein stenosis, access via the internal jugular vein was considered. Under ultrasound guidance, the right internal jugular vein was accessed, Angiography was performed post-puncture to assess the venous anatomy and to identify any potential obstructions before proceeding. Upon confirming adequate right internal jugular vein patency, a flexible introducer sheath over a guide wire was placed (Figure 3). Using fluoroscopic guidance, the Micra device was advanced through the sheath until reaching optimal positioning within the right ventricle, with the patient tolerating the procedure well (Figure 4). Post-implantation parameters were within the desired range, including a pacing threshold of 0.75 V, sensing of 8.5 mV, and impedance of 760 Ω. Once satisfied with performance, the sheath was removed, and hemostasis achieved with “8” figure suture.
 |
Figure 1 Angiography via the right femoral vein revealed severe stenosis of the right iliac vein. |
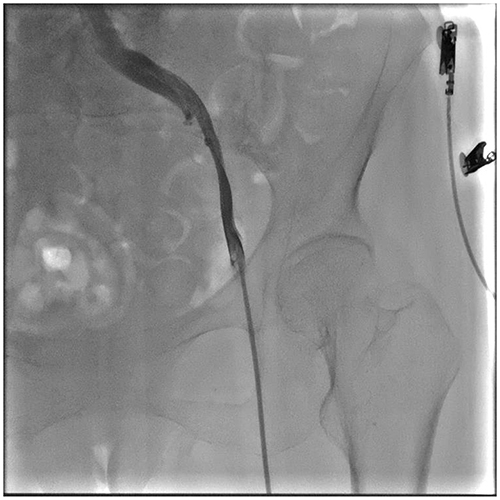 |
Figure 2 Angiography via the left femoral vein revealed severe stenosis of the left iliac vein, which is estimated to be impassable for a 23F sheath. |
 |
Figure 3 The Micra delivery catheter is advanced over the guidewire through the right jugular vein into the right atrium. |
 |
Figure 4 Under right anterior oblique view, the Micra was successfully implanted in the low septal position of the right ventricle. |
Throughout the procedure, vital signs including blood pressure, heart rate, and oxygen saturation were continuously monitored (Table 1). Intraprocedural electrocardiographic and fluoroscopic monitoring ensured accurate leadless pacemaker deployment and real-time evaluation of cardiac rhythm and device stability. Procedural success was defined as:(1) Successful vascular access and sheath delivery;(2) Optimal device deployment in the right ventricular septum without dislodgement or repositioning;(3) Acceptable electrical parameters, including pacing threshold <1.0 V at 0.24 ms, R-wave amplitude >5 mV, and impedance between 500–1500 Ω;(4) Absence of complications such as pericardial effusion, significant bleeding, or arrhythmia; and (5) Hemodynamic stability and absence of procedural-related adverse events during recovery.
 |
Table 1 Procedural Monitoring and Device Parameters |
The patient returned for her 1-month and 3-month follow-up appointments. At the 1-month visit, the pacing threshold remained stable at 0.75 V, and the R-wave amplitude and impedance were consistent with the post-implantation values. The patient reported no symptoms such as dizziness, syncope, or discomfort at the implantation site. At 3 months, the device function remained optimal, and no complications were observed. The patient continued to show normal device parameters, confirming the long-term efficacy and stability of the leadless pacemaker.
Discussion
Leadless pacemakers, exemplified by the Micra device, have emerged as a valuable alternative to traditional transvenous systems, particularly for patients at elevated risk of infection, vascular complications, or complex anatomical challenges.5 In scenarios such as the present case, where the patient presents with sick sinus syndrome (SSS) alongside a medical history that includes chronic kidney disease necessitating dialysis, longstanding diabetes, renal anemia, and prior coronary interventions, the use of a traditional pacemaker would entail substantial risks. Conversely, leadless pacemakers confer several advantages, notably the elimination of the need for a subcutaneous pocket, thereby reducing the risk of infection. This attribute is especially advantageous for patients with low body weight or those who are immunocompromised due to conditions such as diabetes and kidney disease.
For this patient, both femoral veins were unsuitable for access due to severe bilateral iliac vein stenosis, an uncommon but critical anatomical limitation that made the insertion of the pacemaker sheath difficult. While iliac vein stenosis is rare in the general population, it is more frequently seen in patients with end-stage renal disease undergoing long-term dialysis, likely due to vascular calcification. Given these challenges, the team opted to use the right internal jugular vein for access, a route not often utilized for Micra implantation.10
Although the literature on utilizing the internal jugular vein for Micra leadless pacemaker implantation is limited, as femoral access is typically preferred, recent case reports indicate that jugular access may serve as a viable alternative. This approach provides stable access to the right ventricle while circumventing compromised venous pathways in the lower extremities.11–13 Successful implantation via the jugular vein necessitates meticulous management of technical challenges, such as the angulation and maneuverability of the Micra delivery catheter, to ensure accurate device placement without dislodgement or excessive manipulation. Continuous monitoring of critical parameters, including blood pressure, heart rate, and oxygen saturation, demonstrated hemodynamic stability throughout the procedure. The post-implant electrical measurements—pacing threshold of 0.75 V at 0.24 ms, R-wave amplitude of 8.5 mV, and impedance of 760 Ω—met the widely accepted standards for effective Micra leadless pacemaker performance. The 3-month follow-up data show that the patient experienced no complications and that the device function remained optimal. These objective findings confirm the procedural success and appropriate device function. The absence of complications such as arrhythmia, hematoma, or pericardial effusion, combined with the patient’s stable postoperative course, further validates the safety and feasibility of this approach in high-risk anatomical contexts.
From a procedural standpoint, the utilization of ultrasound guidance was crucial for the safe cannulation of the right internal jugular vein, especially in patients presenting with complex anatomical variations and multiple comorbidities. Furthermore, pre-procedural imaging modalities, such as venography, were instrumental in diagnosing iliac vein stenosis, thereby emphasizing the critical importance of comprehensive vascular assessment in patients with a history of dialysis and previous vascular interventions. This case underscores the significance of multidisciplinary collaboration in managing complex cardiovascular procedures. Through close cooperation with vascular and imaging specialists, we were able to identify and adapt to the patient’s unique anatomical challenges, highlighting the necessity for flexible and personalized treatment strategies in patients with multiple comorbidities.
Leadless pacemakers, particularly the Micra device, have gained attention as a viable alternative to traditional transvenous pacemaker systems, especially for patients with complex vascular anatomy and high risks of infection. Our case presents the successful use of the right internal jugular vein for Micra implantation in a high-risk patient with severe bilateral iliac vein stenosis, a technique rarely explored in the current literature. Compared to previous studies,14,15 such as those by Malagù et al and Bencardino et al, which highlight femoral access as the primary route for leadless pacemaker implantation, our case emphasizes the feasibility of utilizing the right internal jugular vein when femoral access is not possible. While the right internal jugular vein has been documented for other procedures, its use for Micra implantation is less common, especially in patients with complex venous anatomy. This case contributes to the growing body of evidence that supports the viability of the right internal jugular vein as an alternative access route, with no adverse events observed during or after the procedure.
Despite the successful outcome in this case, there are limitations to be considered. First, this is a single-center case report with only one patient, and the findings may not be generalizable to larger populations. Second, while the procedure was successful, the long-term follow-up data is limited to three months, and further monitoring would be needed to assess the durability and potential complications of the Micra leadless pacemaker via the right internal jugular vein in similar high-risk patients. Lastly, while this case highlights the benefits of an alternative access route, it is crucial to consider patient-specific factors and anatomical variations before determining the best approach for pacemaker implantation.
In conclusion, although femoral access remains the standard for leadless pacemaker implantation, this case contributes to the growing evidence supporting the right internal jugular vein as a viable alternative. For patients with bilateral iliac vein stenosis or similar complex venous anatomy, jugular access offers a safe, effective solution, broadening the use of leadless pacing technology in high-risk patient populations.
This alternative technique provides a significant clinical implication for high-risk patients, particularly those with compromised vascular access due to chronic conditions such as end-stage renal disease, diabetes, and prior vascular interventions. By enabling successful pacemaker implantation in these patients, this approach reduces the risks associated with traditional transvenous procedures and enhances patient outcomes in cases where conventional access routes are not feasible.
Data Sharing Statement
The datasets used are available from the corresponding author on request.
Ethical Approval
Our institution does not require ethical approval for reporting case reports.
Informed Consent
The patient provided written informed consent for the publication of her clinical information and any accompanying images in this case report.
Acknowledgments
We thank the patient for allowing the publication of this report.
Funding
There is no funding to report.
Disclosure
The authors report no conflicts of interest in this work.
References
1. Coppola M, Yealy DM. Transvenous pacemakers. Emerg Med Clin North Am. 1994;12(3):633–643. doi:10.1016/S0733-8627(20)30405-3
2. Christie S, McGregor M, Krahn AD. Cardiac implantable electronic device infection. Trends Cardiovasc Med. 2025;35(5):310–316. doi:10.1016/j.tcm.2025.02.001
3. Watanabe T, Iwai-Takano M. The pacemaker lead dislocation. Clin Case Rep. 2022;10(4):e05776. doi:10.1002/ccr3.5776
4. Ng P, Paul V, Shetty S, Lambert J. Percutaneous extraction of a malpositioned subclavian arterial pacing lead using the retained wire technique and a vascular closure device: a case report. Eur Heart J Case Rep. 2022;6(6):ytac234. doi:10.1093/ehjcr/ytac234
5. Xu F, Meng L, Lin H, Xu W, Guo H, Peng F. Systematic review of leadless pacemaker. Acta Cardiol. 2024;79(3):284–294. doi:10.1080/00015385.2023.2276537
6. Lancellotti P, Gach O, Marechal P, Robinet S. Micra® leadless pacemaker. Rev Med Liege. 2019;74(S1):S104–S108.
7. Bednarczyk D, Kuliczkowski W, Letachowicz K, et al. Simultaneous placement of leadless pacemaker and dialysis catheter in patient with exhausted vasculature. J Vasc Access. 2021;22(1):147–150. doi:10.1177/1129729819894085
8. Suresh SP, Buchanan EB, Yoo D. First reports of dual-chamber leadless pacemaker implantation via intrajugular access. J Cardiovasc Electrophysiol. 2025;36(4):895–899. doi:10.1111/jce.16572
9. Jelisejevas J, Breitenstein A, Hofer D, Winnik S, Steffel J, Saguner AM. Left femoral venous access for leadless pacemaker implantation: patient characteristics and outcomes. Europace. 2021;23(9):1456–1461. doi:10.1093/europace/euab083
10. Saleem-Talib S, van Driel VJ, Nikolic T, et al. The jugular approach for leadless pacing: a novel and safe alternative. Pacing Clin Electrophysiol. 2022;45(10):1248–1254. doi:10.1111/pace.14587
11. Molitor N, Saleem-Talib S, Ramanna H, Hofer D, Breitenstein A, Steffel J. Leadless pacemaker implantation via the internal jugular vein. Europace. 2024;26(8):euae199. doi:10.1093/europace/euae199
12. El-Bokl A, Siddeek H, Hou C, Leslie A, Jimenez E, Cortez D. Pediatric micra leadless pacemaker implantation via internal jugular and femoral veins: experience with 11 patients. Future Cardiol. 2022;18(9):679–686. doi:10.2217/fca-2021-0139
13. Siddeek H, Jimenez E, Ambrose M, et al. Pediatric micra leadless pacemaker implantation via the internal jugular and femoral vein: a single-center, US experience. Future Cardiol. 2021;17(6):1116–1122. doi:10.2217/fca-2020-0169
14. Malagù M, D’Aniello E, Vitali F, Balla C, Gasbarro V, Bertini M. Leadless pacemaker implantation in superobese patient. Rev Cardiovasc Med. 2022;23(4):125. doi:10.31083/j.rcm2304125
15. Bencardino G, Scacciavillani R, Narducci ML. Leadless pacemaker technology: clinical evidence of new paradigm of pacing. Rev Cardiovasc Med. 2022;23(2):43. doi:10.31083/j.rcm2302043
 © 2025 The Author(s). This work is published and licensed by Dove Medical Press Limited. The
full terms of this license are available at https://www.dovepress.com/terms
and incorporate the Creative Commons Attribution
- Non Commercial (unported, 4.0) License.
By accessing the work you hereby accept the Terms. Non-commercial uses of the work are permitted
without any further permission from Dove Medical Press Limited, provided the work is properly
attributed. For permission for commercial use of this work, please see paragraphs 4.2 and 5 of our Terms.
© 2025 The Author(s). This work is published and licensed by Dove Medical Press Limited. The
full terms of this license are available at https://www.dovepress.com/terms
and incorporate the Creative Commons Attribution
- Non Commercial (unported, 4.0) License.
By accessing the work you hereby accept the Terms. Non-commercial uses of the work are permitted
without any further permission from Dove Medical Press Limited, provided the work is properly
attributed. For permission for commercial use of this work, please see paragraphs 4.2 and 5 of our Terms.