Back to Journals » International Journal of Women's Health » Volume 17
Revolutionizing Surgical Precision: A Case Report on the Articulating Endoscopic Linear Cutter for Laparoscopic Total Hysterectomy
Authors Liu FY, Guo Y, Chen QC, Hao S, Zhang CL, Ding DN, Liu SX, Zhang JX, Han FJ ![]()
Received 16 May 2025
Accepted for publication 11 October 2025
Published 27 October 2025 Volume 2025:17 Pages 3907—3912
DOI https://doi.org/10.2147/IJWH.S541001
Checked for plagiarism Yes
Review by Single anonymous peer review
Peer reviewer comments 2
Editor who approved publication: Dr Marleen van Gelder
Fang-Yuan Liu,1,2 Ying Guo,2 Qiao-Chu Chen,1 Songli Hao,2 Chun-Lan Zhang,2 Dan-Ni Ding,1 Shao-Xuan Liu,1 Jing-Xin Zhang,2 Feng-Juan Han2
1Graduate School, Heilongjiang University of Chinese Medicine, Harbin, Heilongjiang, People’s Republic of China; 2Third Department of Gynecology, The First Affiliated Hospital Heilongjiang University of Chinese Medicine, Harbin, Heilongjiang, People’s Republic of China
Correspondence: Feng-Juan Han, Third Department of Gynecology, The First Affiliated Hospital Heilongjiang University of Chinese Medicine, No. 26, Heping Road, Xiangfang District, Harbin, Heilongjiang, 150040, People’s Republic of China, Email [email protected]
Abstract: Uterine fibroids are a common benign gynecological condition, and laparoscopic total hysterectomy (LTH) remains a well-established treatment option. For patients with severe anemia or limited tolerance for prolonged anesthesia, reducing operative time, minimizing intraoperative blood loss, and preventing complications are key clinical challenges. We report the case of a 45-year-old Chinese woman with uterine fibroids presenting with dysmenorrhea and menorrhagia. During her laparoscopic total hysterectomy, bilateral fallopian tubes, round ligaments, broad ligaments, and proper ovarian ligaments were clearly exposed. An articulating endoscopic linear cutter was utilized to clamp and transect the uterine ligaments bilaterally. The procedure was completed in 115 minutes with an estimated intraoperative blood loss of 80 mL. The patient recovered fully without any postoperative complications. This case indicates that the use of an articulating endoscopic linear cutter in laparoscopic total hysterectomy may facilitate shorter operative times and reduced intraoperative blood loss, while maintaining surgical safety.
Keywords: articulating endoscopic linear cutter, laparoscopic total hysterectomy, uterine fibroid, case report
Introduction
Uterine fibroids are benign tumors. The global prevalence of uterine fibroids exceeds 75% among women.1,2 Heavy or prolonged menstrual bleeding, anemia, and adverse pregnancy outcomes are common manifestations that significantly impair quality of life.3,4 Treatment modalities for uterine fibroids include pharmacotherapy, interventional procedures, and surgical interventions. Laparoscopic total hysterectomy (LTH) is currently a widely adopted surgical approach for managing uterine fibroids.5 In anemic patients, rapid reduction of anesthesia time primarily depends on surgical expertise. Is there any other way to speed up the time of laparoscopic total hysterectomy of the uterine fibroid, reduce the risk of anesthesia, and promote the patient’s postoperative recovery?
This manuscript presents an innovative approach to optimizing uterine fibroids treatment via advanced instrument technology, advocating the application of an articulating endoscopic linear cutter in laparoscopic total hysterectomy. The device incorporates a blade-and-staple cartridge system that generates three staggered rows of staples on either side of the incision, enabling simultaneous cutting and stapling. With intelligent positioning and distal angle adjustment capabilities, it enhances surgical precision, shortens operative duration, and minimizes intraoperative bleeding through optimized hemostasis via staggered staple alignment.6 This design reduces procedural complexity, mitigates risks of tissue trauma and infection, and accelerates postoperative organ function recovery, consequently decreasing hospitalization duration.7,8 While literature on this technique remains sparse, we demonstrate its clinical feasibility through a case study of a 45-year-old patient with multiple uterine fibroids who successfully underwent surgery, providing empirical support for wider adoption of this technological advancement.
Case Presentation
A 45-year-old Chinese woman was hospitalized for persistent heavy menstrual bleeding and dysmenorrhea unresponsive to ibuprofen, lasting over 4 years. These symptoms prompted multiple hospital visits. Over the preceding 2 months, she reported a marked increase in blood loss alongside fatigue, lumbosacral pain, and insomnia. Comprehensive medical history and clinical evaluations were conducted. Her past surgical history included breast fibroadenoma resection in 2021, with no other significant medical history. She denied adverse drug reactions, is a nonsmoker, abstains from alcohol, and reports no relevant family history.
On physical examination, the patient’s temperature was 36.5°C, heart rate 74 bpm, blood pressure 126/93 mmHg, and respiratory rate 18 breaths per minute. The abdomen was soft, without peritoneal irritation signs such as rigidity, rebound tenderness, fever, nausea, or vomiting. Gynecological examination revealed: normal external genital development, smooth vaginal mucosa without abnormal discharge, cervix exhibiting columnar enlargement, anterverted uterine position with uterine size enlarged to approximately two fists’ dimensions, uterine corpus demonstrating fair to moderate mobility and firm consistency, absence of tenderness, and bilateral adnexa without palpable abnormalities.
Blood analysis revealed a hemoglobin level of 76 g/L, indicating moderate anemia severity. To optimize postoperative recovery outcomes, iron supplementation therapy was implemented, followed by a subsequent complete blood count (CBC) evaluation demonstrating a hemoglobin level of 104 g/L. Urinalysis showed occult blood (2+). Given the association between abnormal uterine bleeding and thyroid dysfunction, thyroid function tests demonstrated elevated antithyroglobulin antibodies (54.51 IU/mL) and antithyroid peroxidase autoantibody (6.75 IU/mL), consistent with thyroid autoimmunity; thyroid ultrasonography confirmed diffuse parenchymal changes. Sex hormone profiling (luteinizing hormone 2.51 mIU/mL, follicle-stimulating hormone 6.41 mIU/mL, prolactin 22.28 pg/mL, estradiol 31.00 pg/mL, progesterone 0.40 ng/mL, testosterone 28.15 ng/dL) was performed to assess ovarian function and reserve, particularly for ovarian preservation considerations during hysterectomy. Additional investigations included tumor markers (ferritin 9.04 ng/mL), vaginal secretion analysis (Nugent score 3), electrocardiogram showing myocardial ischemia, and lung CT revealing multiple right lung nodules, a right lower lobe bullous cavity, bilateral lung infiltrates. Pelvic MRI confirmed multiple uterine fibroids with degenerative changes, heterogeneous endometrial signal, cervical nabothian cyst, and trace pelvic free fluid (Figure 1). These comprehensive evaluations were pivotal for individualized surgical planning and perioperative optimization.
 |
Figure 1 Different degrees of uterine fibroid in MRI. (A) Sagittal MRI images; (B) Horizontal MRI images. Note: The red circular outline indicates the patient’s uterine boundary. |
The final diagnosis in this case was multiple uterine fibroids accompanied by mild anemia, which is consistent with the clinical presentation and MRI findings. The treatment plan, including the diagnosis and recommended surgical procedure, was thoroughly explained to the patient. After discussing all available alternative management options, such as conservative treatment and High-Intensity Focused Ultrasound (HIFU), the patient strongly insisted on undergoing a total hysterectomy. Consequently, she was scheduled for and provided consent to a laparoscopic total hysterectomy with bilateral salpingectomy and bilateral ovarian exploration.
The trocar placement adhered to conventional gynecologic laparoscopic standards: a 10 mm umbilical port for a 30° laparoscope, a 10–12 mm supraumbilical port as the primary operating channel, and 5 mm ports at right McMaster’s point and left reverse McMaster’s point for auxiliary maneuvers. The articulating endoscopic linear cutter was introduced through the primary channel and advanced to the uterine cup via vaginal access. Considering the patient’s anemia, strategies focused on minimizing intraoperative bleeding, reducing surgical duration, and optimizing postoperative recovery. Ovarian preservation was prioritized as intraoperative evaluation confirmed bilateral ovarian integrity.
Initial steps involved exposing the tubal isthmus, round ligaments, broad ligaments, and proper ovarian ligaments. A dissecting articulating linear cutter was used to clamp and transect these structures bilaterally along the uterine corpus, with safe anatomical positioning away from the ureter ensuring no injury (Figure 2). The fallopian tubes were subsequently transected near the uterine corpus, followed by isolation of the uterine arteries using vascular clips and an ultrasonic scalpel. Cervical resection was completed in a single step. Intraoperative blood loss totaled 80 mL with an operative time of 115 minutes. The patient achieved uncomplicated postoperative recovery, validating the efficacy of this technical approach in balancing surgical efficiency with patient safety.
 |
Figure 2 Articulating endoscopic linear cutter using an endoscopic linear articulating cutter and postoperative incision status. The red arrows indicate the sites of bilateral incisions. Upper right image was created by Figdraw. |
Discussion
As a common clinical disease, laparoscopic total hysterectomy for uterine fibroid has been a recognized procedure.9 However, the necessity of salpingectomy merits attention. In patients without fertility requirements, concurrent bilateral salpingectomy following total hysterectomy is supported by multiple medical rationales. First, the fallopian tubes serve as the primary origin for high-grade serous ovarian carcinoma: the most lethal histological subtype, with over 70% of such malignancies arising from the tubal fimbriae. Salpingectomy has been associated with an ovarian cancer risk reduction of approximately 80%.10 Additionally, the procedure requires minimal additional operative time, does not elevate intraoperative bleeding or infection risk, and prevents complications like hydrosalpinx or inflammation, thereby minimizing subsequent surgical interventions.11 Meanwhile, parasitic fibroids following surgery should be prevented.12 Moreover, for patients with uterine fibroids accompanied by severe anemia, optimizing operative time reduction and minimizing intraoperative blood loss remain primary research challenges.
In this clinical case involving a patient with multiple leiomyomas and concomitant anemia, the primary objectives were to minimize operative duration and reduce intraoperative blood loss. To achieve these goals, we introduced the articulating endoscopic linear cutter: a novel surgical instrument, into gynecological procedures. The articulating endoscopic linear cutter is primarily employed in procedures such as gastric cancer,13 low rectal cancer,14 and splenectomy,15 demonstrating significant efficacy in reducing operative duration and minimizing intraoperative blood loss. This device offers advantages of rapidity, simplicity, and precision, enabling surgical mechanization while expanding operative scope. In traditional laparoscopic total hysterectomy, sequential dissection of individual ligaments: such as the round ligament, broad ligament, tubal isthmus, and proper ovarian ligament, is required. This study employed the articulating endoscopic linear cutter to synchronously clamp the round ligament, broad ligament, tubal isthmus, and proper ovarian ligament. Through optimized surgical pathway planning, this approach effectively reduced instrument movement frequency during deep lesion manipulation, thereby diminishing the probability of iatrogenic tissue trauma from repetitive maneuvers. Concurrently, it achieved a shortened operative duration while maintaining hemostatic efficacy through the device’s reliable cutting-edge sealing properties. This report specifically details the laparoscopic total hysterectomy performed using this device. Notably, for the first time in such a clinical context, the application of the articulating endoscopic linear cutter was systematically implemented to address both time efficiency and hemorrhagic risk in an anemic patient. The approach demonstrates innovative integration of mechanical precision with patient-specific risk mitigation, aligning with contemporary principles of minimally invasive surgery and blood conservation strategies. A study has found that totally laparoscopic Billroth I distal gastrectomy utilizing Tri-Staple is both feasible and safe, yielding favorable short-term surgical outcomes.7 Building upon this foundation, we further extended our exploration and clinical application by promoting and attempting the use of an Articulating Endoscopic Linear Cutter in total hysterectomy procedures. A total of five patients were enrolled in this preliminary study, with detailed patient information and surgical outcomes summarized in Table 1. The patient has demonstrated favorable long-term outcomes, with all current monitoring indicators showing excellent results.
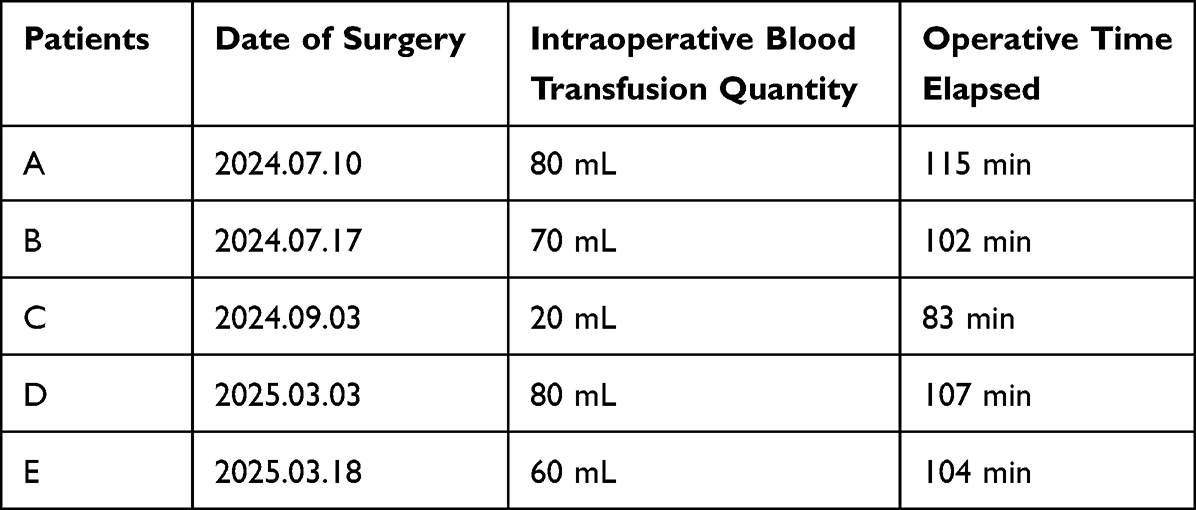 |
Table 1 Patient Demographics and Surgical Outcomes Following Laparoscopic Total Hysterectomy Using an Articulating Endoscopic Linear Cutter |
However, there are some concerning issues. Since the articulating endoscopic linear cutter is employed to simultaneously transect multiple ligaments, adequate exposure is imperative to prevent damage to surrounding organs. In females, the surgical site is often situated deep within the pelvic cavity, an area characterized by complex anatomical structures, a constrained working space, and close proximity to vital organs such as the bladder, rectum, and ureters. These factors collectively contribute to challenging tissue exposure, limited intraoperative visualization, and increased procedural complexity and risks. Consequently, preoperative assessment of pelvic anatomy holds utmost significance. Prior to intrauterine surgeries, magnetic resonance imaging (MRI) and B-ultrasound evaluations, as pivotal imaging modalities, can significantly enhance the accuracy of preoperative diagnosis and surgical safety.16 Studies have shown that MRI, with its exceptional soft-tissue resolution, can precisely define the location, size, and adjacent relationships with surrounding organs (eg, the bladder, rectum, and ureters) of lesions including uterine fibroids, adenomyosis, and endometrial cancer.17 Additionally, we have refrained from using the articulating endoscopic linear cutter to simultaneously interrupt the blood supply of the uterine arteries. Notably, in existing reports, this device is predominantly employed for gastrointestinal anastomosis, which implies that its application in the context of uterine artery manipulation is relatively novel and less explored. Given the abundant and robust blood flow within the uterine arteries, along with the intricate and delicate task of dissecting the connective tissues that encase them, we have made a deliberate decision not to ligate these arteries. This choice is rooted in a steadfast commitment to upholding the highest standards of surgical safety, as any misstep in this high - stakes procedure could lead to severe complications such as excessive bleeding and subsequent organ damage. Therefore, although this technology undeniably holds significant potential for broader application in gynecological surgeries, its implementation must be preceded by a comprehensive and individualized anatomical assessment. Such an assessment will enable surgeons to tailor the surgical approach to each patient’s unique anatomical characteristics, thereby achieving a delicate balance between enhancing surgical efficiency and effectively managing associated risks.
Conclusion
In general, we believe that the innovative application of this instrument in this particular case represents a significant advancement for laparoscopic total hysterectomy. By introducing the articulating endoscopic linear cutter, we have opened up new possibilities for optimizing the surgical procedure. This innovative use has the potential to bring about remarkable improvements, such as a reduction in operative time, a decrease in blood loss, and minimized tissue damage during the surgery. These potential benefits not only enhance the overall surgical experience for patients but also contribute to faster postoperative recovery and a lower risk of complications. Given its promising prospects, this approach holds substantial research value and warrants further exploration. However, it is essential to note that while the initial results are encouraging, more well - designed and comprehensive studies are urgently needed to conclusively confirm the advantages of the articulating endoscopic linear cutter in the context of laparoscopic total hysterectomy, thereby providing a solid evidence base for its widespread clinical adoption.
Data Sharing Statement
Data used in this case report are available upon request from the corresponding author.
Human Ethics
Written informed consent was obtained from the patient for publication of this case report and accompanying images. Institutional approval was not required for the publication.
Acknowledgments
The authors would like to express their sincere gratitude to the editors and reviewers for their meticulous efforts and insightful comments during the peer-review process. Additionally, we acknowledge the use of Figdraw (https://www.figdraw.com/) for creating Figure 2 in this manuscript.
Funding
This study was supported in part by the Heilongjiang Provincial Clinical Collaboration Program for Major and Refractory Diseases (Integrated Traditional Chinese and Western Medicine), and Heilongjiang Provincial Administration of Chinese Medicine Research Project (Grant no. ZHY2024-223 & ZHY2024-234).
Disclosure
The authors report no conflicts of interest in this work.
References
1. Marsh EE, Wegienka G, Williams DR. Uterine fibroids. JAMA. 2024;331(17):1492–1493. doi:10.1001/jama.2024.0447
2. Stewart EA, Nowak RA. Uterine fibroids: hiding in plain sight. Physiology. 2022;37(1):16–27. doi:10.1152/physiol.00013.2021
3. Dolmans MM, Petraglia F, Catherino WH, Donnez J. Pathogenesis of uterine fibroids: current understanding and future directions. Fertil Steril. 2024;122(1):6–11. doi:10.1016/j.fertnstert.2024.02.048
4. Harris HR, Petrick JL, Rosenberg L. The epidemiology of uterine fibroids: where do we go from here? Fertil Steril. 2022;117(4):841–842. doi:10.1016/j.fertnstert.2022.01.037
5. Micić J, Macura M, Andjić M, et al. Currently available treatment modalities for uterine fibroids. Medicina. 2024;60(6):868. doi:10.3390/medicina60060868
6. Sun BF. Research and industrialization of joint type disposable minimally invasive endoscopic cutting stapler. Jiangsu: Jiangsu Fenghe Medical Equipment Co. Ltd.; 2015.
7. Man-I M, Suda K, Kikuchi K, et al. Totally intracorporeal delta-shaped B-I anastomosis following laparoscopic distal gastrectomy using the Tri-Staple™ reloads on the manual Ultra handle: a prospective cohort study with historical controls. Surg Endosc. 2015;29(11):3304–3312. doi:10.1007/s00464-015-4085-1
8. Riga A, Karanjia N. Dangers in the use of staplers in liver surgery. Ann R Coll Surg Engl. 2007;89(8):810–811. doi:10.1308/003588407X232189
9. Sonkusare A, Dixit P. Comparative analysis of total laparoscopic hysterectomy versus non-descent vaginal hysterectomy for benign uterine pathologies in women: a systematic review. Cureus. 2024;16(6):e62846. doi:10.7759/cureus.62846
10. Kahn RM, Gordhandas S, Godwin K, et al. Salpingectomy for the primary prevention of ovarian cancer: a systematic review. JAMA Surg. 2023;158(11):1204–1211. doi:10.1001/jamasurg.2023.4164
11. Lai JM, Masten M, Markese A. Development of hydrosalpinx after prior vaginal hysterectomy and bilateral salpingectomy. Cureus. 2024;16(1):e52573. doi:10.7759/cureus.52573
12. Pham TH, Nguyen PN. Abdominal parasitic fibroids after laparoscopic surgery using a power morcellation: a novel insight from vietnam and a narrative revew of the literature. J Med Ultrasound. 2024. doi:10.4103/jmu.jmu_30_24
13. Ao CB. Application of linear cutting stapler and tube stapler in gastric cancer patients. Med Equip. 2019;32(07):93–94.
14. Cheng JZ. The role of cutting and closing devices in anal preservation surgery for low rectal cancer. China Med Device Inf. 2016;22(20):12–13. doi:10.15971/j.cnki.cmdi.2016.200.006
15. Wang YW, Wu W, Xu ZG. Application of linear cutting stapler in splenectomy of patients with portal hypertension (report of 27 cases). Chin J Mod Surg. 2011;15(05):350–351. doi:10.16260/j.cnki.1009-2188.2011.05.10
16. Nguyen XL, Huynh QH, Nguyen PN. Assessing the clinical characteristics and the role of imaging modalities in uterine sarcoma: a single-center retrospective study from Vietnam. J Clin Ultrasound. 2025. Epub ahead of print. doi:10.1002/jcu.24046
17. Nguyen PN, Nguyen VT. Additional value of Doppler ultrasound to B-mode ultrasound in assessing for uterine intracavitary pathologies among perimenopausal and postmenopausal bleeding women: a multicentre prospective observational study in Vietnam. J Ultrasound. 2023;26(2):459–469. doi:10.1007/s40477-022-00732-w
 © 2025 The Author(s). This work is published and licensed by Dove Medical Press Limited. The
full terms of this license are available at https://www.dovepress.com/terms
and incorporate the Creative Commons Attribution
- Non Commercial (unported, 4.0) License.
By accessing the work you hereby accept the Terms. Non-commercial uses of the work are permitted
without any further permission from Dove Medical Press Limited, provided the work is properly
attributed. For permission for commercial use of this work, please see paragraphs 4.2 and 5 of our Terms.
© 2025 The Author(s). This work is published and licensed by Dove Medical Press Limited. The
full terms of this license are available at https://www.dovepress.com/terms
and incorporate the Creative Commons Attribution
- Non Commercial (unported, 4.0) License.
By accessing the work you hereby accept the Terms. Non-commercial uses of the work are permitted
without any further permission from Dove Medical Press Limited, provided the work is properly
attributed. For permission for commercial use of this work, please see paragraphs 4.2 and 5 of our Terms.