Back to Journals » Journal of Blood Medicine » Volume 12
Revisiting Autoimmunity in Chronic Lymphocytic Leukemia: Prognostic Value of Positive Direct Antiglobulin Test in a Retrospective Study and Literature Review
Authors Ahmed SA, Abdallah GEM, Aly MM, Abdelsalam EMN, Mohammed Saleh MF ![]()
Received 2 January 2021
Accepted for publication 16 March 2021
Published 13 April 2021 Volume 2021:12 Pages 225—234
DOI https://doi.org/10.2147/JBM.S296225
Checked for plagiarism Yes
Review by Single anonymous peer review
Peer reviewer comments 3
Editor who approved publication: Dr Martin H Bluth
Shimaa A Ahmed,1 Ghada EM Abdallah,2 Mai M Aly,2 Eman M Nagiub Abdelsalam,3 Mostafa F Mohammed Saleh2
1Department of Internal Medicine, Faculty of Medicine, South Valley University, Qena, Egypt; 2Clinical Hematology Unit, Department of Internal Medicine, Faculty of Medicine, Assiut University, Assiut, Egypt; 3Department of Clinical Pathology, Faculty of Medicine, Assiut University, Assiut, Egypt
Correspondence: Mostafa F Mohammed Saleh Tel +201013701057
Fax +2088-2332278-2080278
Email [email protected]
Introduction: A positive direct antiglobulin test (DAT) with or without autoimmune hemolytic anemia is a frequent finding in chronic lymphocytic leukemia (CLL). The heterogenic clinical course of CLL mainly depends on different pathogenetic mechanisms which appears in a form of variable biological and clinical features. These features allow stratification of patients into subsets with different outcomes.
Patients and Methods: We evaluated the DAT as a prognostic marker in 120 CLL patients treated with chemoimmunotherapy. Clinical and laboratory features, treatment response, and survival outcomes of CLL patients were assessed in relation to their DAT test status. Additionally, the English literature was extensively reviewed regarding the prognostic impact of a positive DAT in CLL.
Results: DAT positivity was detected in 36 patients (30%) and was associated advanced disease staging (P = 0.03). No correlations were found with other clinical, laboratory, or biological factors such as ZAP-70 or CD38. Both a positive DAT and an Eastern Cooperative Oncology Group performance status > 2 were predictors for non-response to first-line treatment in the multivariate analysis (OR = 0.3, 95% CI: 0.12– 0.8 and OR = 0.2, 95% CI: 0.08– 0.8, respectively). The five-year progression-free survival was significantly lower in the DAT-positive group (P = 0.004). No significant association was found with overall survival (P = 0.2). Sixteen reports analyzing more than 11,000 patients were identified in our review.
Conclusion: In conclusion, DAT positivity in CLL patients is associated with poor response to treatment and disease progression.
Keywords: autoimmunity, chronic lymphocytic leukemia, direct antiglobulin test, autoimmune hemolytic anemia
Introduction
Chronic lymphocytic leukemia (CLL) is the most common type of leukemia; it accounts for approximately 30% of all leukemias and primarily affects the elderly.1 The clinical course is usually indolent, but some patients experience more aggressive disease. CLL is frequently associated with immune disturbances. A positive direct antiglobulin test (DAT) with or without frank autoimmune hemolytic anemia (AIHA) is strongly associated with CLL. Associations with immune thrombocytopenia (ITP) and pure red cell aplasia (PRCA) have been reported as well. The incidence of immune cytopenia has been reported to range from less than 5% to 38%.2
The pathogenesis of autoimmunity in CLL is not well known. Different mechanisms have been proposed, including aberrant antigen presentation that induces IgG auto-antibodies coating erythrocytes and platelets with consequent antibody-dependent cellular cytotoxicity and complement-mediated destruction and the development of an autoreactive T-cell repertoire that produces inhibitory cytokines.3 The dysregulation of T regulatory cells in CLL with an imbalance of the T regulatory/T helper 17-cell ratio has also been noted.4,5
AIHA is primarily characterized by the presence of a positive DAT and the alteration of other hemolytic markers including the reticulocyte count, lactate dehydrogenase (LDH), and haptoglobin.6 The DAT is positive at some point during the course of CLL in up to 35% of cases.7 However, DAT positivity does not necessarily mean that AIHA is present, and only one-third of DAT-positive CLL cases develop clinically overt hemolysis.8
Regarding prognostic relevance, several reports have shown an association of AIHA in CLL patients with other clinical and biological prognostic factors.7,9–11 Moreover, DAT positivity at diagnosis may provide insights about survival in CLL; however, conflicting conclusions have been reported.12–14
In this study, we sought to determine the prognostic role of the DAT in CLL patients treated with chemoimmunotherapy by evaluating the response rate and survival outcomes. An extensive literature review was performed on this subject to verify this potential and provide a platform for possible use in future prognostic models of CLL.
Patients and Methods
Patients with newly diagnosed CLL between January 2011 and December 2019 who attended the Clinical Hematology Unit, Internal Medicine Department, Assiut University Hospital were recruited for this study. Patients were eligible if they had a confirmed diagnosis of CLL and the treatment was as per the International Workshop on Chronic Lymphocytic Leukemia (IWCLL).15 For diagnosis, peripheral blood smears and bone marrow morphology examinations with immunophenotyping by flowcytometry (strong expressions of CD5 and CD23, low or absent expressions of CD79b, sIgM, and FMC7) were performed. All patients were classified according to Rai staging.16 Any patient with a history of prior systemic autoimmune diseases and prior cancer or who had received previous chemotherapy and radiotherapy had been ruled out. Baseline data of different demographic and clinical parameters were collected, including age, sex, performance status, presence of B-symptoms, Rai stage, hepatitis status, and DAT test at diagnosis. The expressions of surface CD38 and cytoplasmic ZAP-70 were illustrated as the percentage of gated cells and were considered positive when ZAP-70 ≥ 20% and CD38 ≥ 30%. A flowcytometric analysis was performed by fluorescence-activated cell sorter Calibur flow cytometry, and data were obtained and analyzed using Cell Quest software (Becton Dickinson Biosciences).
The peripheral blood samples were obtained using K3EDTA vacutainers for the complete count (CBC), and DAT analyses. Another peripheral blood sample was collected without anticoagulants, and plain tubes were used for the assessments of serum LDH, urea, creatinine, and uric acid. Hematological parameters were determined by the automated CBC analyzer “Cell Dyne Ruby” (Abbott, Diagnostic ®). Biochemical markers were assessed using “Hitachi 912” (Japan) by photometric assay. The DAT was performed in all cases using microtube column agglutination Gel technique systems for antibody screening (Diamed). AIHA was diagnosed based on the presence of unexplained anemia; a positive DAT for IgG, C3d, or both; and/or an increased reticulocyte count and an increase in indirect bilirubin with no other cause for anemia identified prior to treatment or any blood product transfusion.
Treatment Course and Outcomes
Indications for treatment in the CLL patients followed the IWCLL guidelines.15 The following treatment regimens were administered:
- Thirty-five patients received an alkylating agent, chlorambucil, at a dose of 6–10 mg/d (0.1–0.2 mg/kg/d) PO for 7–14 days in 28-day cycles until the disease stabilized (usually 6–12 cycles).
- Twenty-one patients received a purine analog therapy, FCR (fludarabine (25 mg/m2/d intravenously (IV) × 5 days q28), cyclophosphamide (250 mg/m2 IV × 5 days), and rituximab (375 mg/m2 day 1 prior to each chemotherapy cycle by slow intravenous infusion)).
- Fifty-seven patients received CVP plus rituximab treatment on day 1 of a 21-day cycle with cyclophosphamide, 750 mg/m2 IV; vincristine, 1.4 mg/m2 (maximum of 2.0 mg); and prednisone, 100 mg by mouth daily for 5 days. Rituximab was administered as 375 mg/m2 one day prior to each chemotherapy cycle by slow intravenous infusion.
The response to treatment was classified as complete remission,16 which was defined by the disappearance of the disease in the clinical and imaging studies; partial response, which was defined by a >50% decrease of the involved site; progressive disease, which was defined by a >50% increase in the size of the involved lesions or the appearance of new lesions; or as relapse, which was defined by recurrence of the disease after CR. Stable disease was defined as a change of −45% to +45% in size of the involved lesions.17 The overall response included both CR and PR.
Overall survival (OS) was defined as the duration between the date of diagnosis and the last follow-up or date of death. Progression-free survival (PFS) is the period from the date of first-line therapy to the date of relapse, progression, the last follow-up, or death from any cause. The study was approved by our Institutional Review Board in accordance with the Declaration of Helsinki, and written informed consent was obtained from all recruited patients.
A literature search for relevant studies was performed using PubMed, Scopus, and Google Scholar. The following key words were used: autoimmunity, DAT test, Coombs test, AHIA, and CLL. Relevant references in the cited studies were also included in the review process. Case reports or studies of other autoimmune cytopenias such as ITP or PRCA in CLL were excluded.
Statistical Analysis
Comparisons between DAT-positive and -negative groups were performed regarding CBC, LDH levels, staging, treatment outcomes, and survival analysis. Numeric variables were expressed as the mean ± standard deviation or the median (interquartile range) depending on tests of normality, and categorical variables were described as relative frequencies. The t-test, Wilcoxon Sum-Rank test, and the chi-square test were used for comparisons between groups. The differences were considered statistically significant at P < 0.05. The survival curves were determined by the Kaplan–Meier method and analyzed by a cox regression hazard ratio. The difference between groups was calculated by the Log Rank test. Data were analyzed using the Statistical Package for Social Science version 24 (IBM Corp., Armonk, NY).
Results
The baseline data of 120 patients were collected, and two patients had completed their treatment and follow-up in another center and thus only their baseline data were analyzed. The mean age of the cohort population was 60 ± 12.5 years, and 56 patients (46.7%) were females. DAT positivity was recorded at study entry in 36 patients (30%). The baseline clinical and laboratory parameters of the cohort according to the DAT test at diagnosis are illustrated in Table 1.
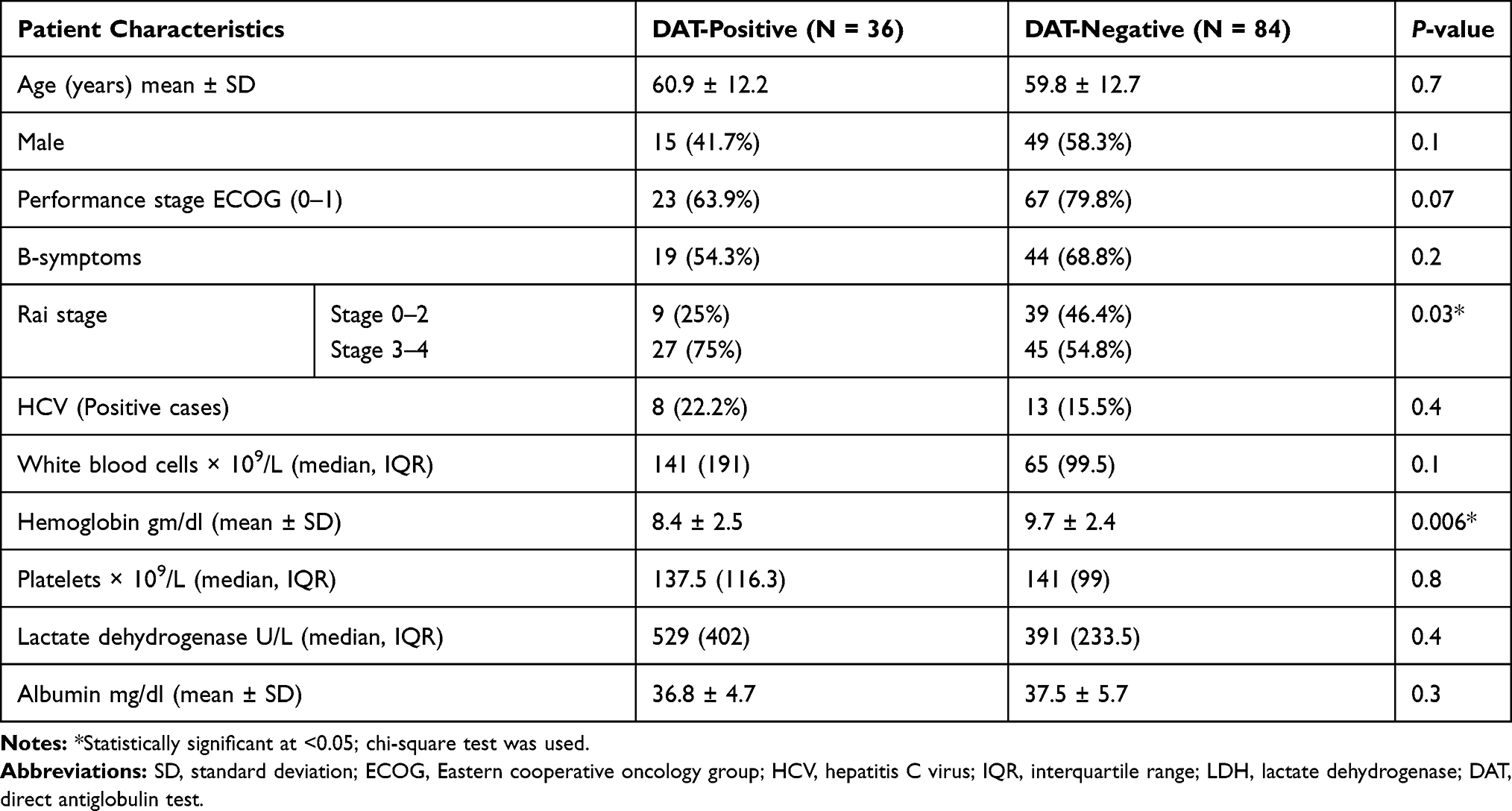 |
Table 1 Clinical and Laboratory Characteristics of Patients with CLL Based on DAT Status |
CD38 and ZAP-70 were analyzed for 90 patients at diagnosis, and the results indicated that 32 (35.6%) patients were positive for ZAP-70 and 25 (27.8%) were positive for CD38. The frequencies of the positive CD38 and ZAP-70 cases within positive and negative DATs cases are shown in Table 2.
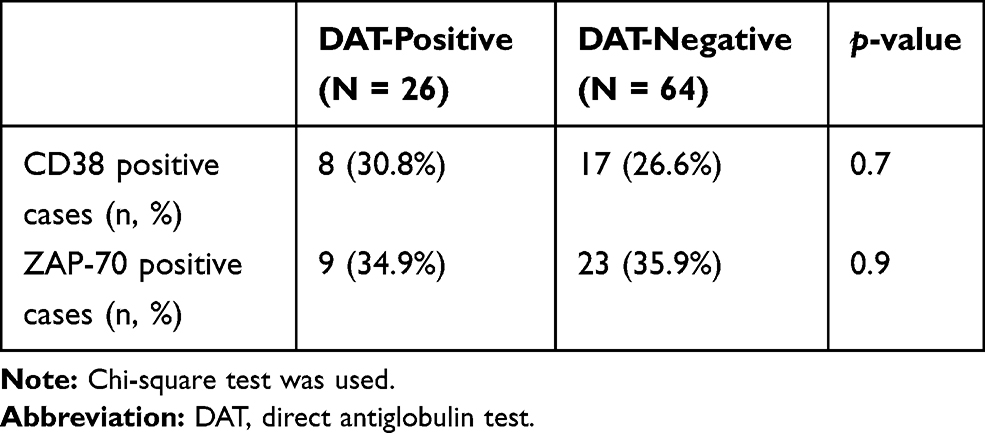 |
Table 2 Associations of CD38 and ZAP-70 with DAT |
A total of 113 patients in the cohort required treatment with either fludarabine-based chemotherapy or non-fludarabine-based chemotherapy (chlorambucil ± R or CVP ± R), five patients remained under a wait and see protocol throughout the entire recorded follow-up period, and there no data were available regarding the therapy response in two patients. The percentages of the patients treated by the different therapy lines in DAT-positive and DAT-negative cases are illustrated in Table 3. The details of the response are illustrated in Table 4. The univariate logistic regression analysis of the overall response of the patients who received first-line treatment was associated with a positive DAT at diagnosis (OR = 0.3, 95% CI: 0.12–0.65), an Eastern Cooperative Oncology Group (ECOG) performance score >2 (OR = 0.2, 95% CI: 0.08–0.5), and older age (OR = 0.96, CI: 0.93–0.99); conversely, there was no association with being positive for CD38 at diagnosis (OR = 0.5, 95% CI: 0.21–1.4), being positive for ZAP-70 (OR = 0.7, 95% CI: 0.3–1.9), or advanced Rai stage (OR = 1.2, 95% CI: 0.5–2.6). The multivariate model including performance status, age, and positive DAT is illustrated in Table 5.
 |
Table 3 Proportions of the Therapy Lines in DAT-Positive and DAT-Negative Cases |
 |
Table 4 Response Assessment-Based DAT |
 |
Table 5 Multivariate Analysis of Overall Response to the First-Line Therapy |
The median follow-up was 35.5 months (range, 2–84 months). The median survival time of the patients with a negative DAT was 84 months, which did not differ significantly from the group with a positive Coombs test (60 months, P = 0.2) (Figure 1). The five-year PFS of patients with positive DATs was significantly lower than that of patients with negative Coombs tests (22% vs 60%, P = 0.004) (Figure 2).
 |
Figure 1 Kaplan–Meier estimates of overall survival in CLL patients according to DAT status (P = 0.2). |
 |
Figure 2 Kaplan–Meier estimates of PFS in CLL patients according to DAT status (P = 0.004). Median PFS of positive and negative cases: 40.9 and 84 months, respectively. |
We included parameters that were reported as predictors of PFS in the univariate cox regression hazards analysis (Table 6) and used them in the multivariate cox regression model. This model indicated that a positive DAT (HR = 2.3, 95% CI: 1.1–4.8) and being positive for CD38 (HR = 2.5, CI: 1.1–5.1) could serve as predictors.
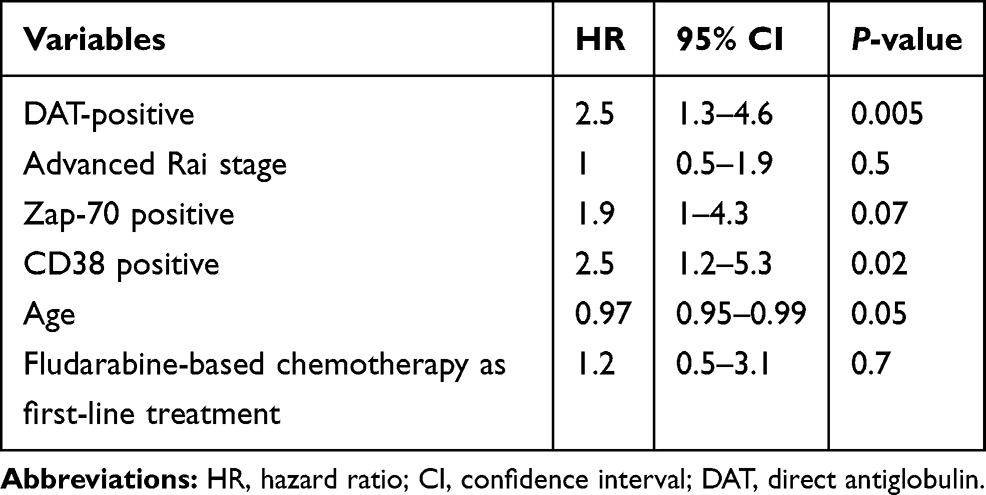 |
Table 6 Univariate Cox Regression Hazard Analysis of Possible Predictors of PFS |
Only 12 patients with a positive DAT had confirmed AHIA, and 24 patients had no obvious anemia. As shown in Figure 3, there was no difference in PFS between patients who developed AIHA and those who did not (median PFS of 36 and 42 months, respectively, P = 0.9).
 |
Figure 3 Kaplan–Meier estimates of PFS in DAT-positive CLL patients according to AIHA development (P = 0.9). |
We thoroughly searched for previous studies performed on CLL patients with AIHA or a positive DAT and identified 16 reports with more 11,000 total patients. Table 7 summarizes the impact of a positive DAT on CLL patient outcomes reported by those studies.
 |
Table 7 Studies About the Prognostic Impact of a Positive DAT on CLL Outcomes |
Discussion
A positive DAT with or without AIHA is a common finding in CLL. Although there are convincing data that the clinical outcome of CLL patients who have a positive DAT differs from that of patients with a negative result, the conclusions remain inconsistent.
In the present study, the frequency of a positive DAT was 30%. This is very similar to previous studies from Asia that were conducted in Chinese and Pakistani populations.13,18 Reports from western countries had lower prevalence.10,19–21 The higher incidence might be explained by ethnic background or late patient medical consultation resulting in a higher percentage (60%) of advanced disease stages at diagnosis, as noted in our cohort.
Among the different baseline clinical and biological factors of CLL, DAT positivity was associated with advanced stage CLL. This association between either a positive DAT10 or AIHA and advanced disease has been consistently reported in several studies.12,19 Other studies have reported that autoimmune diseases or positive DATs in CLL were associated with older age,13,20 male gender,20 higher lymphocytic count at presentation,10,20 high serum LDH,18,22 and high β2-microglobulin levels.10,14,23
AIHA occurred in 33.3% of the patients with a positive DAT, and this accounted for approximately 10% of the entire cohort, which is in agreement with other studies.8,12 This could indicate that a positive DAT without anemia in CLL might serve as an early unique prognostication of the disease.
In the present study, the subgroup comparison based on DAT positivity revealed no differences regarding the presence of other biologic prognostic parameters such as ZAP-70 or CD38, and this was partially agreed by Xu et al who found no correlation with CD38 despite the presence of a correlation with ZAP-70.18 Others reported that a positive DAT was associated with ZAP-70 and CD38.10 Nevertheless, because such assessments did not account for all patients in this study, this finding should be interpreted with caution.
Unfortunately, baseline cytogenetic and molecular data of our cohort were not recorded and were not included in our analysis to verify our assumption; however, several reports have shown that DAT positivity was associated with poor risk cytogenetics22 and unmutated IgVH status.8,18,22
In the response assessment, a positive DAT and worse ECOG performance status seemed to be the only independent predictors for an unfavorable response to the different chemo-immunotherapies. Dearden et al reported lower overall response rates for positive DATs that reflected poor PFS,12 which is quite similar to our findings. The outcomes of the DAT-positive patients treated with a fludarabine-based regimen were not any better, which is consistent with the results of Barcellini et al.9 However, the combination of cyclophosphamide with fludarabine may have a protective effect against the development of AIHA with a better response and PFS compared with fludarabine alone. Interestingly, positive DATs have been reported to have shorter treatment-free survival in untreated CLL.8
Previous reports have shown that anemia caused by autoimmune mechanisms results in better survival compared with anemia secondary to bone marrow infiltration with advanced disease stages.24 Herein, the PFS did not differ between the patients who developed AIHA and those who did not among the DAT-positive cohort. An interesting finding by Dearden et al was that PFS and OS were better for DAT-negative patients, even after excluding those who developed AHA.12 This strongly indicates that a positive DAT represents a risk factor independently from developing anemia for the survival of CLL patients.
A positive DAT was not associated with OS in our cohort. This finding is in accordance with previous reports;1,10,13,25 however, Quinquenel et al reported that a positive DAT was an independent adverse prognostic factor for OS.8 In our study, PFS may not be a surrogate for OS because this association became weaker in diseases with longer survival post progression, and it may require a longer follow-up duration to detect it.26
This study has some limitations. It is a retrospective cohort study with a relatively short follow-up duration. The unavailability of data about cytogenetic parameters and other molecular variables such as IgVH status or del 17 prevented us from conducting further analyses to prove our hypothesis. Another limitation was that patients receiving novel agents such as Bruton tyrosine kinase inhibitors like ibrutinib or BCL2 inhibitors like Venetoclax were not included in our study; thus, our conclusions might not extend to this population.
Conclusion
When assessing CLL, anemia is a cornerstone of Rai and Binet staging systems;16,27 however, whether it is immune-related has not yet been incorporated in those models, which might limit better disease evaluation and prognostication. DAT positivity can be considered a surrogate marker for advanced clinical stage and progression of the disease course in patients with CLL, and we suggest incorporating it with other developing molecular stratifying parameters currently being investigated to develop a novel risk stratification system for CLL.
Abbreviations
CLL, Chronic lymphocytic leukemia; CR, Complete remission; DAT, Direct antiglobulin test; ECOG, Eastern Cooperative Oncology Group; IWCLL, International Workshop on Chronic Lymphocytic Leukemia; OR, Or advanced Rai; OS, Overall survival; PFS, Progression-free survival; PR, Partial response; PRCA, Pure red cell aplasia.
Author Contributions
All authors made substantial contributions to conception and design, acquisition of data, or analysis and interpretation of data; took part in drafting the article or revising it critically for important intellectual content; agreed to submit to the current journal; gave final approval of the version to be published; and agree to be accountable for all aspects of the work.
Disclosure
The authors report no conflicts of interest in this work.
References
1. Rebecca S, Siegel M, Kimberly D, Miller M, Ahmedin Jemal D. Cancer statistics. CA Cancer J Clin. 2017;67(27):7–30.
2. Hodgson K, Ferrer G, Montserrat E, Moreno C. Chronic lymphocytic leukemia and autoimmunity: a systematic review. Haematologica. 2011;96(5):752–761. doi:10.3324/haematol.2010.036152
3. Fattizzo B, Barcellini W. Autoimmune cytopenias in chronic lymphocytic leukemia: focus on molecular aspects. Front Oncol. 2020;9:1435. doi:10.3389/fonc.2019.01435
4. D’Arena G, Simeon V, D’Auria F, et al. Regulatory T-cells in chronic lymphocytic leukemia: actor or innocent bystander? Am J Blood Res. 2013;3(1):52–57.
5. Lad DP, Varma S, Varma N, Sachdeva MUS, Bose P, Malhotra P. Regulatory T-cell and T-helper 17 balance in chronic lymphocytic leukemia progression and autoimmune cytopenias. Leuk Lymphoma. 2015;56(8):2424–2428. doi:10.3109/10428194.2014.986479
6. Zent CS, Kay NE. Autoimmune complications in chronic lymphocytic leukaemia (CLL). Best Pract Res Clin Haematol. 2010;23(1):47–59. doi:10.1016/j.beha.2010.01.004
7. Borthakur G, O’Brien S, Wierda WG, et al. Immune anaemias in patients with chronic lymphocytic leukaemia treated with fludarabine, cyclophosphamide and rituximab–incidence and predictors. Br J Haematol. 2007;136(6):800–805. doi:10.1111/j.1365-2141.2007.06513.x
8. Quinquenel A, Al Nawakil C, Baran‐Marszak F, et al. Old DAT and new data: positive direct antiglobulin test identifies a subgroup with poor outcome among chronic lymphocytic leukemia stage A patients. Am J Hematol. 2015;90(1):E5–E8. doi:10.1002/ajh.23861
9. Barcellini W, Capalbo S, Agostinelli RM, et al. Relationship between autoimmune phenomena and disease stage and therapy in B-cell chronic lymphocytic leukemia. Haematologica. 2006;91(12):1689–1692.
10. Moreno C, Hodgson K, Ferrer G, et al. Autoimmune cytopenia in chronic lymphocytic leukemia: prevalence, clinical associations, and prognostic significance. Blood. 2010;116(23):4771–4776.
11. Zanotti R, Frattini F, Ghia P, et al. ZAP-70 expression is associated with increased risk of autoimmune cytopenias in CLL patients. Am J Hematol. 2010;85(7):494–498. doi:10.1002/ajh.21737
12. Dearden C, Wade R, Else M, et al. The prognostic significance of a positive direct antiglobulin test in chronic lymphocytic leukemia: a beneficial effect of the combination of fludarabine and cyclophosphamide on the incidence of hemolytic anemia. Blood. 2008;111(4):1820–1826.
13. Abbas SA, Zeeshan R, Sultan S, Irfan S. Direct Coombs test positivity in B-chronic lymphoid leukemia: a marker of advanced clinical disease. Asian Pac J Cancer Prev. 2015;16(14):6007–6010. doi:10.7314/apjcp.2015.16.14.6007
14. Ricci F, Tedeschi A, Vismara E, et al. Should a positive direct antiglobulin test be considered a prognostic predictor in chronic lymphocytic leukemia? Clin Lymphoma Myeloma Leuk. 2013;13(4):441–446. doi:10.1016/j.clml.2013.02.024
15. Hallek M, Cheson BD, Catovsky D, et al. Guidelines for the diagnosis and treatment of chronic lymphocytic leukemia: a report from the International Workshop on Chronic Lymphocytic Leukemia updating the National Cancer Institute-Working Group 1996 guidelines. Blood. 2008;111(12):5446–5456. doi:10.1182/blood-2007-06-093906
16. Rai KR, Sawitsky A, Cronkite EP, Chanana AD, Levy RN, Pasternack BS. Clinical staging of chronic lymphocytic leukemia. Blood. 1975;46(2):219–234. doi:10.1182/blood.V46.2.219.219
17. Hallek M, Cheson BD, Catovsky D, et al. iwCLL guidelines for diagnosis, indications for treatment, response assessment, and supportive management of CLL. Blood. 2018;131(25):2745–2760. doi:10.1182/blood-2017-09-806398
18. Xu W, Li J-Y, Miao K-R, et al. The negative prognostic significance of positive direct antiglobulin test in Chinese patients with chronic lymphocytic leukemia. Leuk Lymphoma. 2009;50(9):1482–1487. doi:10.1080/10428190903111930
19. Hamblin TJ, Oscier DG, Young BJ. Autoimmunity in chronic lymphocytic leukaemia. J Clin Pathol. 1986;39(7):713–716. doi:10.1136/jcp.39.7.713
20. Mauro FR, Foa R, Cerretti R, et al. Autoimmune hemolytic anemia in chronic lymphocytic leukemia: clinical, therapeutic, and prognostic features. Blood. 2000;95(9):2786–2792. doi:10.1182/blood.V95.9.2786.009k30_2786_2792
21. Kyasa MJ, Parrish RS, Schichman SA, Zent CS. Autoimmune cytopenia does not predict poor prognosis in chronic lymphocytic leukemia/small lymphocytic lymphoma. Am J Hematol. 2003;74(1):1–8. doi:10.1002/ajh.10369
22. Ricci F, Tedeschi A, Vismara E, et al. Positive Direct Antiglobulin Test (DAT) in Chronic Lymphocytic Leukemia (CLL) Patients: Correlation with Prognostic Factors. American Society of Hematology; 2009.
23. Shvidel L, Tadmor T, Braester A, et al. Pathogenesis, prevalence, and prognostic significance of cytopenias in chronic lymphocytic leukemia (CLL): a retrospective comparative study of 213 patients from a national CLL database of 1518 cases. Ann Hematol. 2013;92(5):661–667. doi:10.1007/s00277-012-1663-3
24. Zent CS, Ding W, Schwager SM, et al. The prognostic significance of cytopenia in chronic lymphocytic leukaemia/small lymphocytic lymphoma. Br J Haematol. 2008;141(5):615–621. doi:10.1111/j.1365-2141.2008.07086.x
25. Atef B, Azmy E, Aladle D, Mabed M. The prevalence and prognostic significance of autoimmune cytopenias in a cohort of Egyptian patients with chronic lymphocytic leukemia. Hematol Oncol Stem Cell Ther. 2019;12(2):97–104. doi:10.1016/j.hemonc.2019.01.004
26. Amir E, Seruga B, Kwong R, Tannock IF, Ocaña A. Poor correlation between progression-free and overall survival in modern clinical trials: are composite endpoints the answer? Eur J Cancer. 2012;48(3):385–388. doi:10.1016/j.ejca.2011.10.028
27. Binet JL, Leporrier M, Dighiero G, et al. A clinical staging system for chronic lymphocytic leukemia: prognostic significance. Cancer. 1977;40(2):855–864. doi:10.1002/1097-0142(197708)40:2<855::AID-CNCR2820400239>3.0.CO;2-1
28. Demir C, Ekinci Ö. Clinical and serological autoimmune complications in chronic lymphocytic leukemia. Wien Klin Wochenschr. 2017;129(15–16):552–557. doi:10.1007/s00508-017-1208-9
29. Visentin A, Imbergamo S, Gurrieri C, et al. Major infections, secondary cancers and autoimmune diseases occur in different clinical subsets of chronic lymphocytic leukaemia patients. Eur J Cancer. 2017;72:103–111. doi:10.1016/j.ejca.2016.11.020
30. Duek A, Shvidel L, Braester A, Berrebi A. Clinical and immunologic aspects of B chronic lymphocytic leukemia associated with autoimmune disorders. Isr Med Assoc J. 2006;8(12):828–831.
 © 2021 The Author(s). This work is published and licensed by Dove Medical Press Limited. The
full terms of this license are available at https://www.dovepress.com/terms
and incorporate the Creative Commons Attribution
- Non Commercial (unported, 3.0) License.
By accessing the work you hereby accept the Terms. Non-commercial uses of the work are permitted
without any further permission from Dove Medical Press Limited, provided the work is properly
attributed. For permission for commercial use of this work, please see paragraphs 4.2 and 5 of our Terms.
© 2021 The Author(s). This work is published and licensed by Dove Medical Press Limited. The
full terms of this license are available at https://www.dovepress.com/terms
and incorporate the Creative Commons Attribution
- Non Commercial (unported, 3.0) License.
By accessing the work you hereby accept the Terms. Non-commercial uses of the work are permitted
without any further permission from Dove Medical Press Limited, provided the work is properly
attributed. For permission for commercial use of this work, please see paragraphs 4.2 and 5 of our Terms.