Back to Journals » Clinical Ophthalmology » Volume 16
Retrospective Study of a Sustained-Release Intracanalicular Dexamethasone Insert for Treatment of Ocular Inflammation After Cataract and Corneal Surgery
Authors Fram N ![]() , Alsetri H
, Alsetri H ![]() , Shiler O
, Shiler O ![]() , Paterno PJ, Cabang J
, Paterno PJ, Cabang J
Received 19 August 2022
Accepted for publication 6 December 2022
Published 10 December 2022 Volume 2022:16 Pages 4065—4074
DOI https://doi.org/10.2147/OPTH.S386702
Checked for plagiarism Yes
Review by Single anonymous peer review
Peer reviewer comments 2
Editor who approved publication: Dr Scott Fraser
Nicole Fram,1,2 Hasan Alsetri,1 Orly Shiler,1 Paul Jerick Paterno,1 Julieanne Cabang1
1Research Department, Advanced Vision Care, Los Angeles, CA, USA; 2Stein Eye Institute, David Geffen School of Medicine, UCLA, Los Angeles, CA, USA
Correspondence: Nicole Fram, Advanced Vision Care, 2080 Century Park East Suite #911, Los Angeles, CA, 90067, USA, Tel +1 310 625 8061, Fax +1 310 229 1222, Email [email protected]
Purpose: To evaluate the effectiveness and safety of a sustained-release intracanalicular dexamethasone insert (Dextenza, Ocular Therapeutix, Inc.) as an adjunctive therapy in patients undergoing cataract and corneal surgery.
Patients and Methods: This retrospective case series contains 18 patients undergoing cataract surgery and 6 patients undergoing corneal surgery. All patients received the Dextenza intracanalicular insert. 6/18 of the patients in the cataract surgery arm were on the standard of care post-surgery topical steroid drop regimen, whereas 11/18 of the patients were on a reduced regimen. 1/18 of the patients was on a drop regimen that deviated from the aforementioned regimens. 2/6 of the patients in the corneal surgery arm were on the standard of care post-surgery topical steroid drop regimen, whereas 3/6 of the patients were on a reduced regimen. 1/6 of the patients were on a drop regimen that deviated from the aforementioned regimens.
Results: The primary outcome measures are intraocular pressure (IOP) levels and anterior chamber inflammation levels across the post-operative recovery period. 1/18 of the patients in the cataract surgery arm and 1/6 of the patients in the corneal surgery arm experienced a clinically significant IOP spike greater than 10 millimeters of mercury (mmHg) above baseline IOP. No patient in either of the study groups had significant inflammation after 1 week post-surgery. 1/18 of the patients in the cataract surgery arm and 1/6 of the patients in the corneal surgery arm experienced a canalicular obstruction.
Conclusion: Dextenza with the lower drop protocol showed non-inferiority in terms of inflammation management and safety. As with any steroid delivery mechanism, monitoring IOP is paramount when using Dextenza. One of the patients with a canalicular obstruction had a history of punctal plug implantation, so care should be taken when choosing to implant Dextenza in such a patient.
Keywords: steroid drops, Dextenza, graft rejection, cystoid macular edema, intraocular pressure, Fuchs dystrophy
Introduction
Adherence to treatment regimens after ocular surgery can be complicated by patient compliance and difficulty administering topical drops.1 It is particularly important to address ocular inflammation after surgical procedures such as cataract surgery and corneal transplantation to decrease the likelihood of anterior chamber inflammation, macular edema, and corneal edema/rejection.2 Surgical technique and postoperative treatments are both geared towards minimizing postoperative inflammation. Minimally invasive surgical techniques and technological advances have led to smaller surgical incisions, resulting in reduced trauma to ocular structures.3,4 Despite the novel advances to cataract surgery, postoperative inflammation remains ever-present. Surgical trauma induced breakdown of the blood aqueous barrier leads to an increased incidence of observed cells and flare in the anterior chamber of the eye.5 The inflammatory cascade triggered by the surgical trauma can lead to the development of retinal cysts known as cystoid macular edema (CME) or Irvine-Gass syndrome, which can lead to reduced visual acuity post cataract surgery.6
The postoperative medication regimen is critical towards inhibiting the potentially destructive effects of the inflammatory cascade. Corticosteroids and non-steroidal anti-inflammatory drugs (NSAIDs) are the main tools in the ophthalmic surgeon’s arsenal to combat non-infectious ocular inflammation, CME, and corneal graft rejection.7,8 An ocular side effect of corticosteroid use, regardless of the delivery mechanism is increased intraocular pressure (IOP) which can lead to optic neuropathy and steroid-induced glaucoma. Moderate steroid responders (6 to 15-mmHg IOP baseline increase) constitute 33% of the non-glaucomatous population, whereas 4–6% are considered high responders with IOP increases above 15-mmHg.9 The most common methods for the local delivery of corticosteroids to ocular structures include: topical, subconjunctival, periocular, and intravitreal administration.10 Although the ophthalmic community is moving towards a dropless or “less drop” environment, topical therapy remains the standard of care in many cases.11
Topical administration of corticosteroids over a post-operative recovery period is the standard method for steroid delivery post cataract or corneal surgery,12 however long-term topical steroid use is not without its shortcomings. Topical steroids can reduce the immunological competence of the eye, as well as inhibit the corneal absorption of topical antibiotics, which can lead to opportunistic bacterial, viral, or fungal infections. Topical steroids have also been found to potentially delay corneal epithelial healing, particularly in the setting of a neurotrophic cornea. In addition, rebound ocular inflammation is always a risk following abrupt discontinuation or rapid tapering of topical steroids.13 The drawbacks of topical steroids extend beyond the realm of the eyeball itself; complex drop regimens give rise to increased costs and inconveniences to patients, leading to a reduction in patient drop compliance.14 The department of ophthalmology at McGill University found that 92.6% of the patients in their study showed an improper drop administration technique following cataract surgery. This included patients instilling an incorrect number of drops, missing their eye with the drops, contaminating the bottle tip, or failing to wash their hands before administering the drops.15
To help relieve patients of the burdens associated with the aforementioned corticosteroid delivery systems, we explored a sustained-release intracanalicular dexamethasone insert (Dextenza, Ocular Therapeutix, Inc.), which is placed in the punctum of the eye lid, and is designed to deliver preservative free dexamethasone to the ocular surface for up to thirty days.16 Dextenza has been shown to safely decrease ocular inflammation and pain post operatively3,17–19 and could provide a more consistent, reliable method for corticosteroid delivery to ocular structures. This strategy could simplify the complex drop regimens, potentially improving patient compliance, increasing both patient comfort and safety following surgery. Many surgeons may not feel comfortable abandoning the anti-inflammatory topical drop regimens without a safe and effective alternative. The purpose of our study was to evaluate the safety and effectiveness of Dextenza as a corticosteroid delivery mechanism in combination with a shortened topical drop regimen following cataract or corneal surgery.
Materials and Methods
This non-randomized, retrospective study encompassed 18 patients who underwent cataract surgery and 6 patients who underwent corneal surgery with the Dextenza intracanalicular insert placed into the punctum of their operated eyes between February 2020 and August 2020. This study complied with the declaration of Helsinki and was determined to have exempt status by the WCG Institutional Review Board. Patient consent to review medical records was waived by the WCG Institutional Review Board due to the retrospective nature of the study, and as such the patients’ data was anonymized and their confidentiality was maintained.
The primary outcome measures for this study included incidence of IOP elevation > 10mmHg above baseline and prolonged anterior chamber (AC) inflammation. This retrospective study was performed in a private practice setting by N.F. Dextenza was inserted immediately before the cataract or corneal surgery, by first dilating the patient’s punctum with an ophthalmic dilator, drying the punctal area, and placing Dextenza into the patient’s canaliculus using blunt, non-toothed forceps. Baseline IOP measurements were recorded for each patient prior to their cataract or corneal surgery using a Goldmann applanation tonometer. The patients’ IOPs and AC inflammation levels were then monitored and recorded over a 3-month post-operative period for the cataract surgery patients, and a 6-month post-operative period for the corneal surgery patients. The presence of cell or flare in the AC, assessed using a slit-lamp, was used as a marker for AC inflammation. The severity of the AC inflammation was graded from 0 to 4+ using the standardization of uveitis nomenclature (SUN) working group grading scheme for anterior chamber cells and flare.20 Chronic inflammation was defined as the presence of at least 1+ cell or flare in the AC, requiring continued use of topical steroids 3 months post-surgery. Clinically significant IOP spikes were defined as a 10-mmHg increase in IOP from the baseline pre-surgery IOP measurements. Secondary outcome measures included best corrected visual acuity (BCVA), incidence of CME evaluated clinically, and a subjective, self-reported pain assessment. Adverse events were defined as any patient with chronic inflammation, clinically significant IOP spikes, self-reported pain or canalicular complications.
The post cataract surgery regimen for topical steroid administration was defined as two categories: cataract extraction standard of care (CESOC), and cataract extraction Dextenza protocol (CEDP). The topical steroid administered was prednisolone acetate 1%, and the topical NSAID administered was Bromfenac 0.07%, which was utilized in both regimens 1 time a day for the same duration as the topical steroid use. The CESOC regimen refers to the topical steroid plan created for patients before we utilized Dextenza and involves the administration of a topical steroid four times a day for 2 weeks, which subsequently gets tapered down to two times a day for 1 month, for a total of 6 weeks of topical steroid administration. The CEDP regimen refers to the topical steroid plan created for the purpose of testing the effectiveness and safety of the Dextenza insert in reducing the need for topical steroid administration. The CEDP regimen involves the administration of a topical steroid four times a day for 2 weeks, which subsequently gets tapered down to two times a day for 2 weeks, for a total of 4 weeks of topical steroid administration (Table 1).
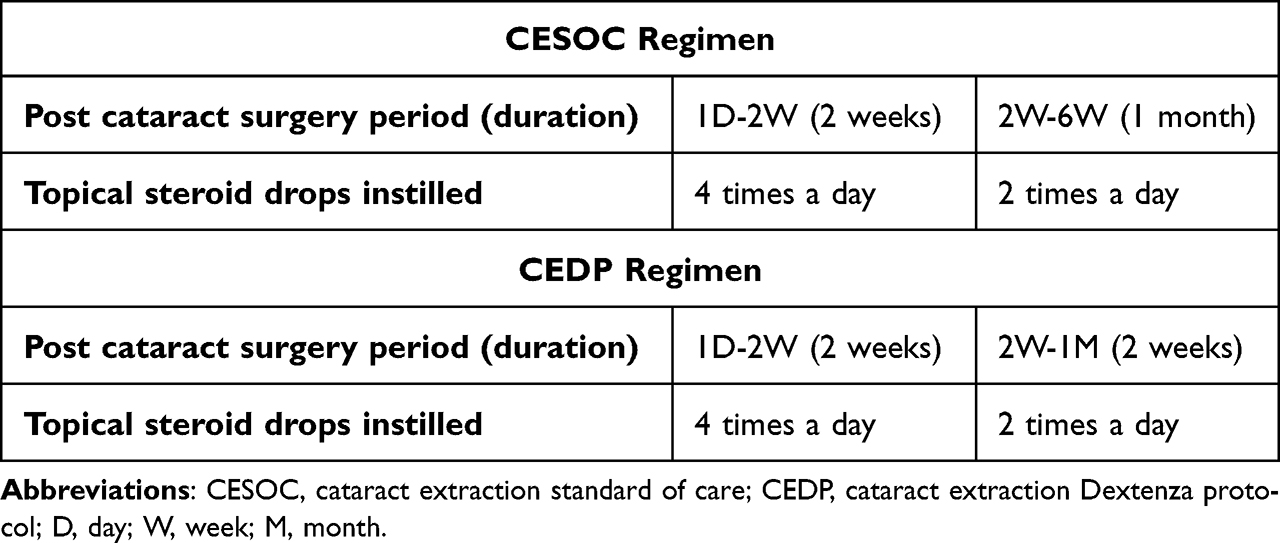 |
Table 1 The Two Post Cataract Surgery Topical Steroid Regimens Employed in the Study |
The post corneal transplant surgery regimen for topical steroid administration was defined as two categories: corneal transplant surgery standard of care (KSOC), and corneal transplant surgery Dextenza protocol (KDP). The topical steroid administered was prednisolone acetate 1%. The KSOC regimen refers to the topical steroid plan created for corneal transplant patients before we utilized Dextenza and involves the administration of a topical steroid eight times a day for 2 weeks, which subsequently gets tapered down to four times a day for 1 month, then three times a day for 1 month, then two times a day for 1 month, and then one time a day indefinitely. The KDP regimen refers to the topical steroid plan created for the purpose of testing the effectiveness and safety of the Dextenza insert in reducing the need for topical steroid administration. The KDP regimen involves the administration of a topical steroid four times a day for 1 month, which subsequently gets tapered down to three times a day for 1 month, then two times a day for 1 month, and then one time a day indefinitely (Table 2).
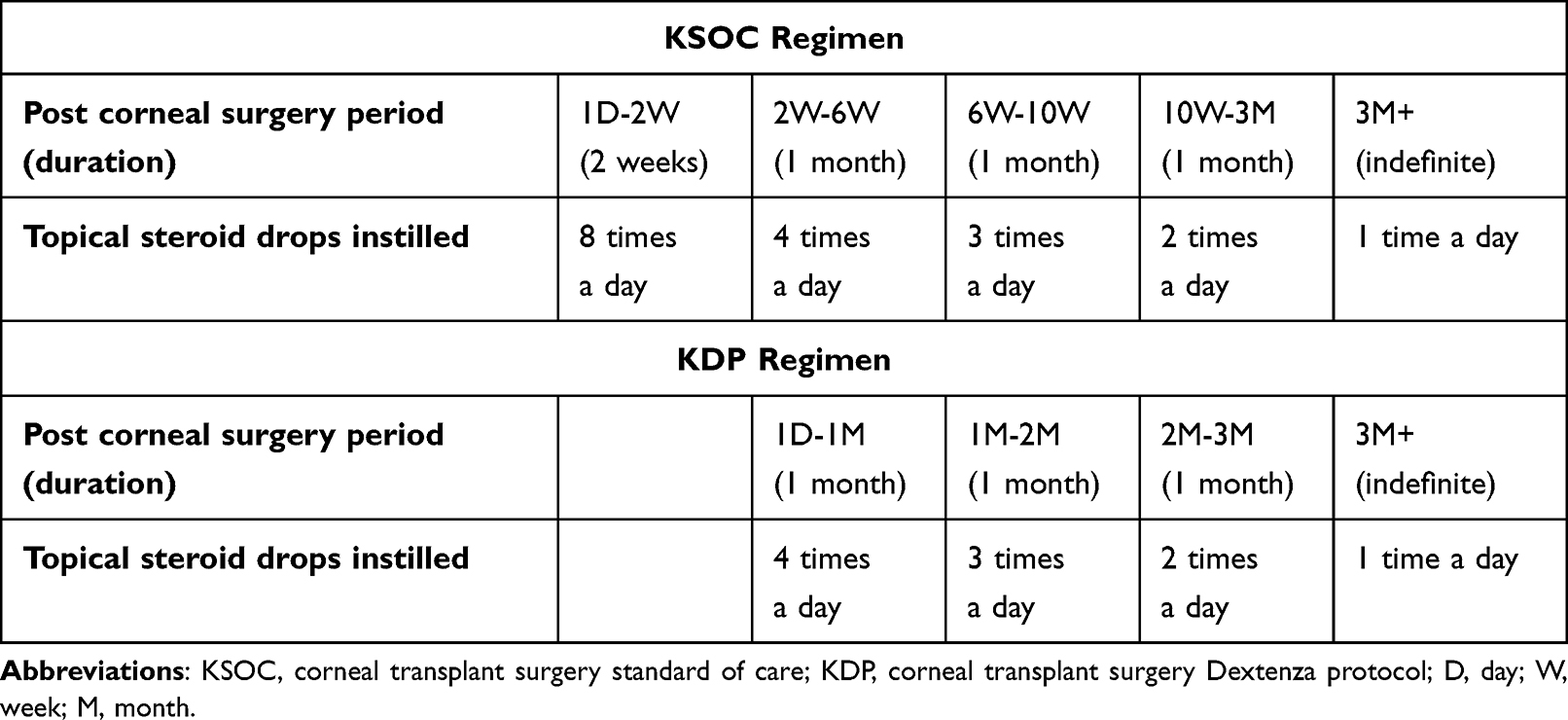 |
Table 2 The Two Post Corneal Surgery Topical Steroid Regimens Employed in the Study |
Results
Cataract Surgery Group
The cataract surgery arm contained 18 patients (15 female, 3 male) who had undergone cataract extraction with intraocular lens implantation in the posterior chamber (CE/PCIOL). Of the 18 patients in the cataract surgery arm, 6/18 (33.3%) were on the CSOC regimen, 11/18 (61%) were on the CDP regimen and 1 (5.6%) was on a regimen that did not fall into either category, designated as not standard (Figure 1).
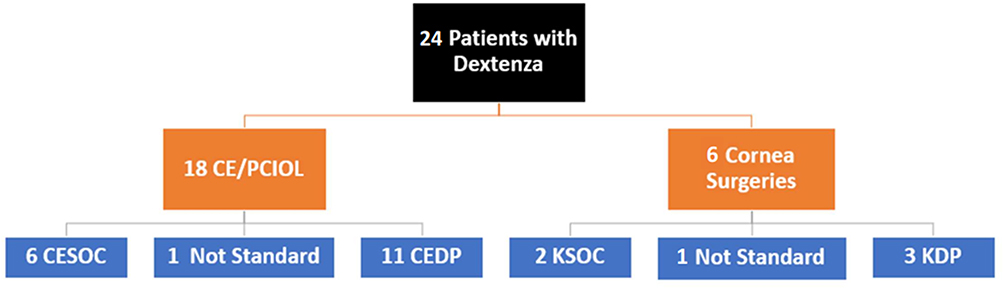 |
Figure 1 A breakdown of the patients in the study by drop regimen. There were 24 patients with the Dextenza insert, 18/24 underwent cataract extraction with intraocular lens implantation in the posterior chamber (CE/PCIOL) while 6/24 underwent corneal surgeries. Of the 18 patients that underwent CE/PCIOL, 6 were under the cataract extraction standard of care drop regimen (CESOC), 11 were under the cataract extraction Dextenza protocol regimen (CEDP) and 1 was on a regimen that was considered not standard. Of the 6 patients who underwent corneal surgeries, 2 were under the corneal transplant standard of care regimen, 3 were under the corneal transplant Dextenza protocol regimen (KDP), and 1 was on a regimen that was considered not standard. |
Corneal Surgery Group
The corneal surgery arm contained 6 patients (2 female, 4 male), 3/6 eyes underwent descemet’s stripping endothelial keratoplasty (DSEK), 1/6 underwent descemet’s stripping without endothelial keratoplasty (DWEK), 1/6 underwent penetrating keratoplasty (PKP), and 1/6 underwent a combined CE/PCIOL with a descemet’s membrane endothelial keratoplasty (DMEK). The indications for the corneal surgeries were: pseudophakic bullous keratopathy (PBK) (2/6), Fuchs endothelial corneal dystrophy (FECD) (2/6), and corneal graft failure (2/6) (Figure 2). Of the 6 patients in the corneal surgery arm, 2 (33.3%) were on the KSOC regimen, 3 (50%) were on the KDP regimen and 1 (28.6%) was on a regimen that did not fall into either category, designated as not standard (Figure 1).
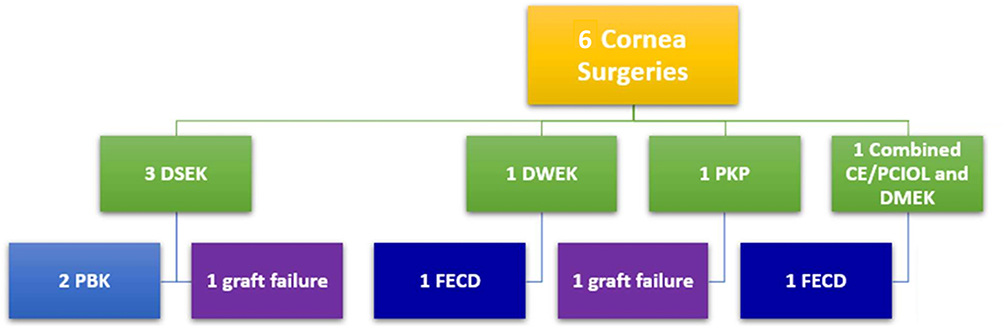 |
Figure 2 A breakdown of the corneal surgery procedures and their indications. Of the 3 patients who underwent descemet’s stripping endothelial keratoplasty (DSEK), 2/3 had pseudophakic bullous keratopathy (PBK) and 1/3 had a previous corneal graft failure. The patient who underwent penetrating keratoplasty (PKP) had a previous corneal graft failure. The patient who underwent descemet’s stripping without endothelial keratoplasty (DWEK) and the patient who underwent the combined cataract extraction with intraocular lens implantation in the posterior chamber (CE/PCIOL) with descemet’s membrane endothelial keratoplasty (DMEK) both had Fuchs endothelial corneal dystrophy (FECD). |
Table 3 depicts the demographics of the study population. The mean age in the cataract surgery arm was 73.2 years, ranging from 62–86 years, with 15/18 (83.3%) female and 3/18 (16.7%) male. The mean age in the corneal surgery arm was 70.7 years, ranging from 38–82 years, with 2/6 (33.3%) female and 4/6 (66.6%) male.
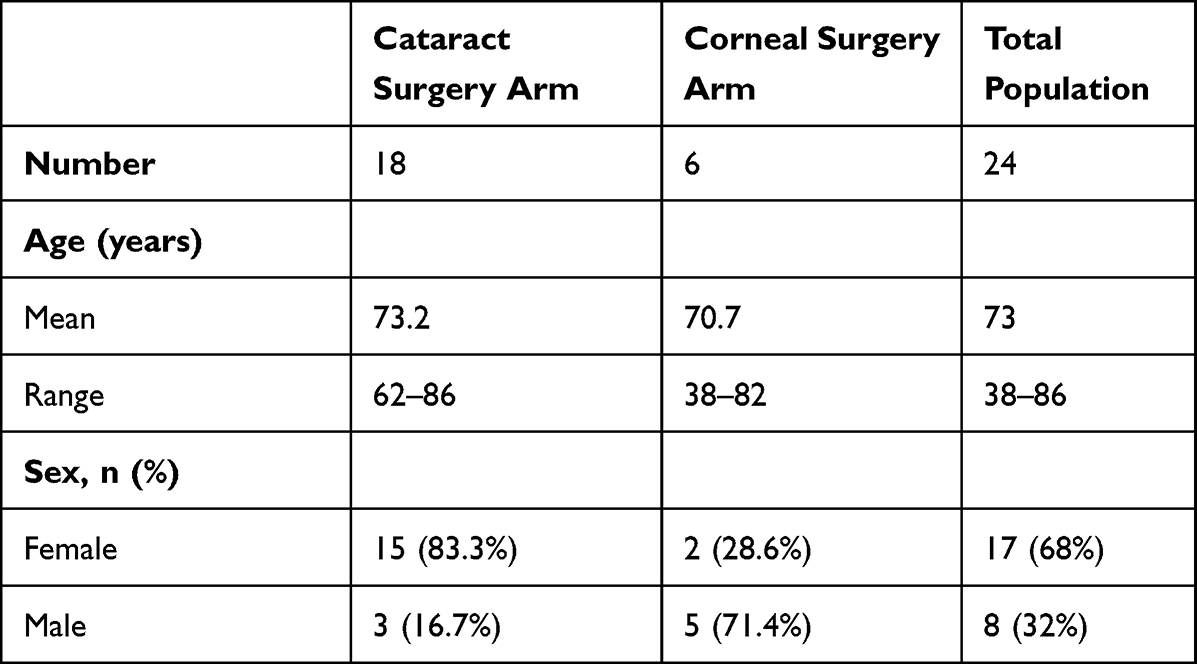 |
Table 3 Study Population Demographics |
The primary outcome measures for the study were IOP levels and AC inflammation levels across the post-operative recovery period for both the cataract surgery and the corneal surgery arms. The patients in the cataract surgery arm had their change in IOP across their post-surgery time period presented for the 1 day, 1 week, 2–6 week, and 2–3 month post-surgery time points. A clinically significant pressure spike of 10-mmHg above baseline levels was experienced by a patient 1-month post cataract surgery and represents the only such pressure spike experienced by any of the patients in the cataract surgery arm (Figure 3).
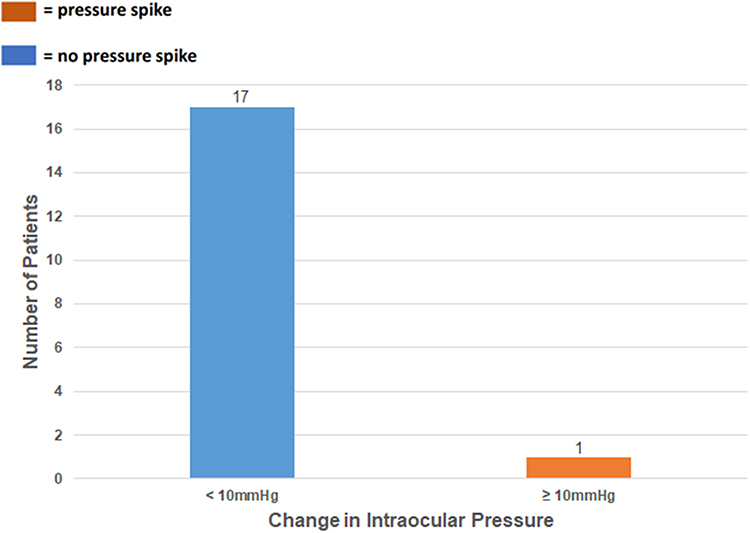 |
Figure 3 Change in intraocular pressure (IOP) relative to each patient’s baseline IOP measurement 2–6 weeks post-cataract surgery (n=18). One of the patients experienced a clinically significant pressure increase of 10-mmHg 1 month post cataract-surgery. |
The patients in the corneal surgery arm had their change in IOP across their post-surgery time period presented for the 1 day, 1 week, 2–6 week, 3 month, and 6 month post-surgery time points. A clinically significant pressure spike of 14-mmHg above baseline levels was experienced by a patient 3-months post corneal surgery and represents the only such pressure spike experienced by any of the patients in the corneal surgery arm (Figure 4).
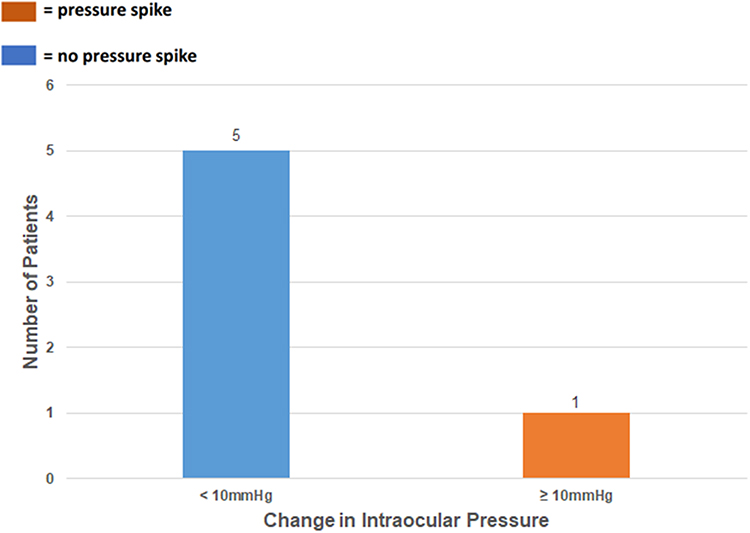 |
Figure 4 Change in intraocular pressure (IOP) relative to each patient’s baseline IOP measurement 3 months post-corneal surgery (n=6). One of the patients experienced a clinically significant pressure increase of 14-mmHg 3 months post corneal surgery. |
The patients in the cataract surgery arm had their AC inflammation levels presented for the 1 day, 1 week, 2–6 week and 2–3 month post-surgery time periods. By the 1 week post-cataract surgery time point, all examined patients had AC cell grades lower or equal to 0.5+ (trace cell) (Figure 5). All of the patients had flare grades of 0 at all post-cataract surgery time points.
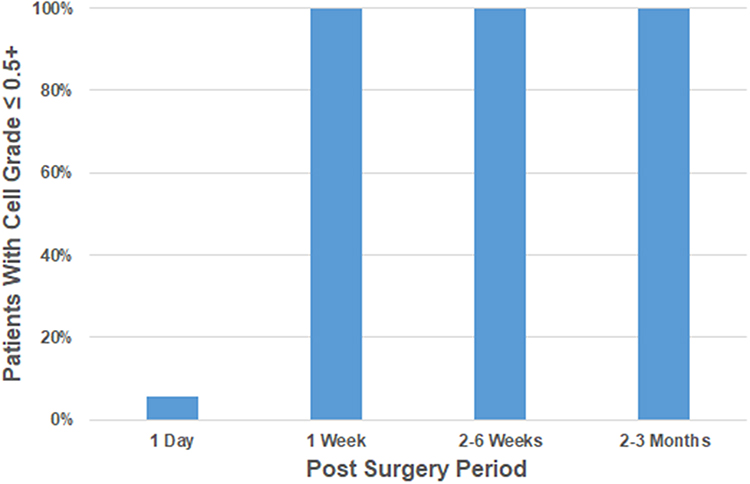 |
Figure 5 Patients with anterior chamber (AC) cell grades less than or equal to 0.5+ for 1 day, 1 week, 2–6 weeks, and 2–3 months post-cataract surgery. By the 1 week post-cataract surgery time point, all examined patients had AC cell grades lower or equal to 0.5+ (trace cell). |
The patients in the corneal surgery arm had their AC inflammation levels presented for the 1 day, 1 week, 2–6-week, 3 month, and 6 month post-surgery time periods. From the 1-week time point to the 6-month time point, all examined patients in the corneal surgery arm had AC cell grades equal to 0 (Figure 6). All of the patients had flare grades of 0 at all post-corneal surgery time points. Table 4 highlights the adverse events experienced by the patients in the study. Both the cataract surgery arm as well as the corneal surgery arm experienced two adverse events each: one pressure spike and one canalicular obstruction in each arm. No chronic inflammation, loss of BCVA, CME, or self-reported pain was experienced by any patient throughout the study.
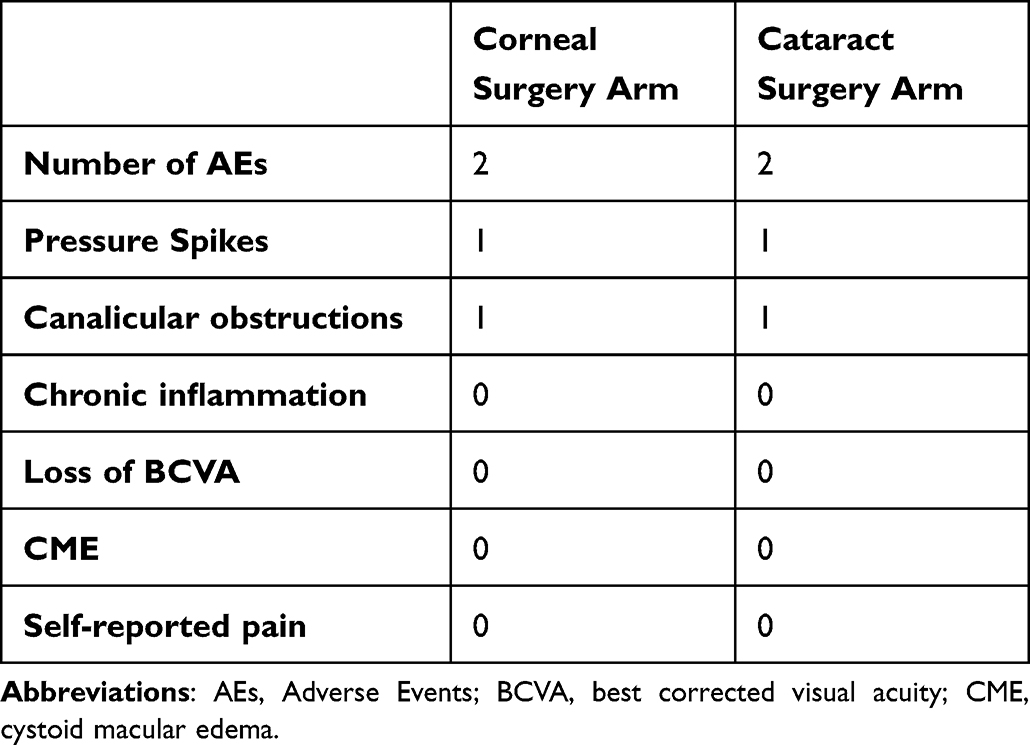 |
Table 4 Adverse Events Experienced by Study Patients |
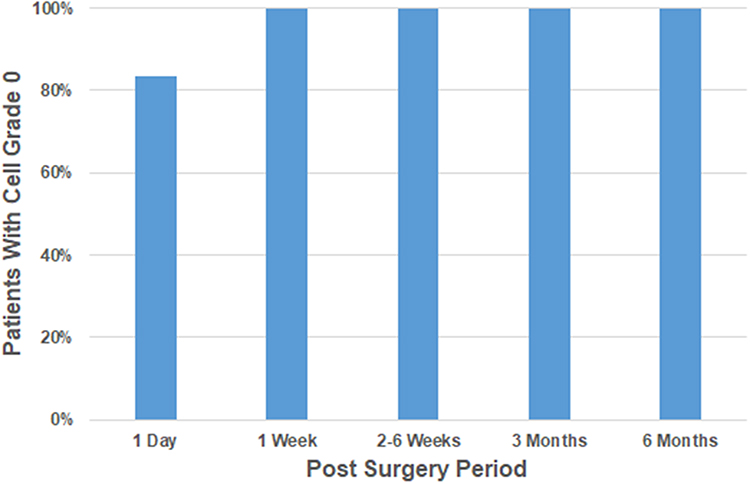 |
Figure 6 Patients with anterior chamber (AC) cell grades of 0 for 1 day, 1 week, 2–6 weeks, 3 months and 6 months post-corneal surgery. From the 1-week time point to the 6-month time point, all examined patients had AC cell grades lower or equal to 0. |
Discussion
Inflammation management is a vital part of an eye surgeon’s post-surgery recovery plan for patients undergoing cataract or corneal surgeries. Topical administration of corticosteroids has long been the standard method for combating inflammation following eye surgery;12 however, it is not without its drawbacks. Topical steroid administration has been found to potentially delay corneal epithelial healing, as well as reduce the immunological competence of the eye.13 In addition, many patients struggle to adhere to the complex topical steroid regimens, preventing them from realizing the full recovery potential that the regimens were designed to deliver.14,15 Dextenza is an alternative method for corticosteroid delivery to ocular tissues post cataract or corneal surgery. This intracanalicular insert is designed to deliver preservative free dexamethasone to the ocular surface for up to thirty days, mitigating the effects of volatile patient compliance.16 Previous studies exploring the safety and efficacy of Dextenza, by monitoring adverse events, ocular pain and inflammation found significant reductions in inflammation and ocular pain in study groups that received Dextenza.3,17–19 This study differs from the previous studies exploring Dextenza, by assessing its safety and effectiveness in patients who have undergone corneal transplantation surgeries.
The Dextenza insert was evaluated for both its effectiveness and safety as a corticosteroid delivery system in the post-operative recovery regimens of 18 patients who underwent cataract extraction, and 6 patients who underwent corneal surgeries. The goal was to evaluate this therapy as adjunctive to topical therapy in order to decrease the total drop burden experienced by patients. Dextenza was found to be effective in reducing AC inflammation following cataract or corneal surgery. In the cataract surgery arm, 17 of the 18 patients who underwent cataract extraction had AC cell grades equal to 0 between 2 and 6 weeks post-cataract surgery, indicating that no AC cells were visualized in those patients. One of the patients had an AC cell grade of 0.5+ (less than five cells visualized in the AC),20 3-months post-cataract surgery. In the corneal surgery arm, all examined patients had AC cell grades equal to 0 at the 1 week post-corneal surgery time point. None of the patients in the cataract or corneal surgery arms showed evidence of AC flare from the first post-surgery day, and none of the patients experienced rebound inflammation.
The safety aspect of the Dextenza insert was evaluated by monitoring the IOPs of the patients with the Dextenza insert over their post-surgery recovery periods, and by evaluating each patient for canalicular complications. Of the 18 patients in the cataract surgery arm, 1/18 (5.5%) experienced a pressure spike of 10-mmHg above baseline IOP at the 1 month post-cataract surgery time point. This incidence is consistent with many topical corticosteroid regiments.21 Of the 6 patients in the corneal surgery arm, one pressure spike of 14-mmHg above baseline IOP was recorded at the 3 month post-corneal surgery time point. It is likely that the 3 month pressure spike can be attributed to the topical prednisolone acetate 1% use, as the Dextenza insert dissolves 30 days after it is implanted. Although 92% of the patients in the study did not suffer any IOP complications, as is the case with most methods of corticosteroid delivery to ocular structures, an increase in IOP is always a concern, and patient IOP should be monitored carefully.
In the cataract surgery arm one canalicular obstruction was observed at the 2 month post-cataract surgery time point, and in the corneal surgery arm, one canalicular obstruction was observed at the 6-month post-corneal surgery time point. The patient with the canalicular obstruction in the corneal surgery arm had a canalicular obstruction in their other eye as well, which was not operated on, nor was it implanted with the Dextenza insert. The epiphora that manifested in both eyes due to the canalicular obstructions was worse in the eye that did not have the Dextenza insert, leading us to believe that the Dextenza insert was not responsible for the canalicular obstruction or the epiphora that the patient experienced. The patient with the canalicular obstruction in the cataract surgery arm experienced mucous discharge from the lower left punctum and required a nasolacrimal irrigation procedure to alleviate the obstruction. The patient had a history of intracanalicular 4mm dissolvable collagen punctal plugs for their dry eye syndrome approximately 4 weeks prior to the placement of the Dextenza insert, which is hypothesized to be a contributing factor to the canalicular obstruction that the patient experienced. A recent study found that 3 eyes in their study experienced canaliculitis and subsequent epiphora after Dextenza implantation.22 Attentiveness is paramount when considering Dextenza for a patient with a history of punctal plug insertions.23
Conclusion
In summary, the Dextenza intracanalicular insert is a safe and effective method for delivering corticosteroids to the ocular structures for inflammation management following cataract or corneal surgery, despite shortened treatment regimens in the immediate postoperative period. Limitations of the study include its small sample size, as well as its retrospective nature. Although our sample size was small, the Dextenza insert was demonstrated to be safe, as long as IOPs are carefully monitored, and patients are carefully screened for past histories of punctal plug insertions before being selected as candidates. Future considerations that can be explored could involve the use of Dextenza without a topical steroid regimen, to elucidate if topical steroid use can be safely eliminated from a post-surgery treatment regimen instead of just reduced. The Dextenza insert ensures corticosteroid delivery to the ocular structures regardless of patient drop compliance and could bridge the gap between a surgeon’s desired post-operative regimen, and the expectations of patients for a comfortable and safe regimen, in order to achieve the mutually desired outcome of a successful and uneventful surgery.
Funding
This study was funded with a grant from Ocular Therapeutix, Inc.
Disclosure
The authors report no conflicts of interest in this work.
References
1. An JA, Kasner O, Samek DA, Lévesque V. Evaluation of eyedrop administration by inexperienced patients after cataract surgery. J Cataract Refract Surg. 2014;40(11):1857–1861. doi:10.1016/j.jcrs.2014.02.037
2. McColgin AZ, Heier JS. Control of intraocular inflammation associated with cataract surgery. Curr Opin Ophthalmol. 2000;11(1):3–6. doi:10.1097/00055735-200002000-00002
3. Walters T, Endl M, Elmer TR, Levenson J, Majmudar P, Masket S. Sustained-release dexamethasone for the treatment of ocular inflammation and pain after cataract surgery. J Cataract Refract Surg. 2015;41(10):2049–2059. doi:10.1016/j.jcrs.2015.11.005
4. Monnet D, Tépenier L, Brézin AP. Objective assessment of inflammation after cataract surgery: comparison of 3 similar intraocular lens models. J Cataract Refract Surg. 2009;35(4):677–681. doi:10.1016/j.jcrs.2008.12.021
5. Pande MV, Spalton DJ, Kerr-Muir MG, Marshall J. Postoperative inflammatory response to phacoemulsification and extracapsular cataract surgery: aqueous flare and cells. J Cataract Refract Surg. 1996;22(Suppl 1):770–774. doi:10.1016/s0886-3350(96)80160-x
6. Bélair ML, Kim SJ, Thorne JE, et al. Incidence of cystoid macular edema after cataract surgery in patients with and without uveitis using optical coherence tomography. Am J Ophthalmol. 2009;148(1):128–35.e2. doi:10.1016/j.ajo.2009.02.029
7. Quintana NE, Allocco AR, Ponce JA, Magurno MG. Non steroidal anti-inflammatory drugs in the prevention of cystoid macular edema after uneventful cataract surgery. Clin Ophthalmol. 2014;8:1209–1212. doi:10.2147/OPTH.S61604
8. Costa DC, de Castro RS, Kara-Jose N. Case-control study of subconjunctival triamcinolone acetonide injection vs intravenous methylprednisolone pulse in the treatment of endothelial corneal allograft rejection. Eye. 2009;23(3):708–714. doi:10.1038/eye.2008.289
9. Armaly MF, Becker B. Intraocular pressure response to topical corticosteroids. Fed Proc. 1965;24(6):1274–1278.
10. Fung AT, Tran T, Lim LL, et al. Local delivery of corticosteroids in clinical ophthalmology: a review. Clin Experiment Ophthalmol. 2020;48(3):366–401. doi:10.1111/ceo.13702
11. Loden JC. Dropless cataract surgery: better for the patient, better for the surgeon. Ophthalmol Manage. 2014;18:20–22.
12. Patel A, Cholkar K, Agrahari V, Mitra AK. Ocular drug delivery systems: an overview. World J Pharmacol. 2013;2(2):47–64. doi:10.5497/wjp.v2.i2.47
13. Renfro L, Snow JS. Ocular effects of topical and systemic steroids. Dermatol Clin. 1992;10(3):505–512. doi:10.1016/s0733-8635(18)30318-8
14. Kholdebarin R, Campbell RJ, Jin YP, Buys YM. Multicenter study of compliance and drop administration in glaucoma. Can J Ophthalmol. 2008;43(4):454–461. doi:10.3129/i08-076
15. An JA, Kasner O, Samek DA, Levesque V. Evaluation of eyedrop administration by inexperienced patients after cataract surgery. J Cataract Refract Surg. 2014;40(11):1857–1861. doi:10.1016/j.jcrs.2014.02.037
16. Ocular therapeutix; 2021. Available from: https://www.ocutx.com/products/dextenza/.
17. Walters TBS, Vold S, Bafna S, et al. Efficacy and safety of sustained release dexamethasone for the treatment of ocular pain and inflammation after cataract surgery: results from two Phase 3 studies. J Clin Exp Ophthalmol. 2016;7. doi:10.4172/2155-9570
18. Tyson SL, Bafna S, Gira JP, et al. Multicenter randomized phase 3 study of a sustained-release intracanalicular dexamethasone insert for treatment of ocular inflammation and pain after cataract surgery. J Cataract Refract Surg. 2019;45(2):204–212. doi:10.1016/j.jcrs.2018.09.023
19. Torkildsen G, Abelson MB, Gomes PJ, McLaurin E, Potts SL, Mah FS. Vehicle-controlled, Phase 2 clinical trial of a sustained-release dexamethasone intracanalicular insert in a chronic allergen challenge model. J Ocul Pharmacol Ther. 2017;33(2):79–90. doi:10.1089/jop.2016.0154
20. Jabs DA, Nussenblatt RB, Rosenbaum JT; Standardization of Uveitis Nomenclature (SUN) Working Group. Standardization of uveitis nomenclature for reporting clinical data. Results of the First International Workshop. Am J Ophthalmol. 2005;140(3):509–516. doi:10.1016/j.ajo.2005.03.057
21. Kusne Y, Kang P, Fintelmann RE. A retrospective analysis of intraocular pressure changes after cataract surgery with the use of prednisolone acetate 1% versus difluprednate 0.05%. Clin Ophthalmol. 2016;10:2329–2336. doi:10.2147/OPTH.S121849
22. Williams KJ, Blieden LS, Koch DD, Yen MT. Intractable epiphora with the dexamethasone ophthalmic insert. J Cataract Refract Surg. 2021;47(7):963–964. doi:10.1097/j.jcrs.0000000000000665
23. Tost FHW, Geerling G. Plugs for occlusion of the lacrimal drainage system. Dev Ophthalmol. 2008;41:193–212.
 © 2022 The Author(s). This work is published and licensed by Dove Medical Press Limited. The
full terms of this license are available at https://www.dovepress.com/terms
and incorporate the Creative Commons Attribution
- Non Commercial (unported, 3.0) License.
By accessing the work you hereby accept the Terms. Non-commercial uses of the work are permitted
without any further permission from Dove Medical Press Limited, provided the work is properly
attributed. For permission for commercial use of this work, please see paragraphs 4.2 and 5 of our Terms.
© 2022 The Author(s). This work is published and licensed by Dove Medical Press Limited. The
full terms of this license are available at https://www.dovepress.com/terms
and incorporate the Creative Commons Attribution
- Non Commercial (unported, 3.0) License.
By accessing the work you hereby accept the Terms. Non-commercial uses of the work are permitted
without any further permission from Dove Medical Press Limited, provided the work is properly
attributed. For permission for commercial use of this work, please see paragraphs 4.2 and 5 of our Terms.