Back to Journals » Clinical Ophthalmology » Volume 19
Retrospective Single-Center Outcomes After a First Bimatoprost Sustained-Release Implant
Authors Olevson CT, Mai AP ![]() , Schweitzer JA, Berdahl JP
, Schweitzer JA, Berdahl JP ![]() , Ferguson TJ
, Ferguson TJ
Received 13 September 2025
Accepted for publication 5 December 2025
Published 16 December 2025 Volume 2025:19 Pages 4775—4786
DOI https://doi.org/10.2147/OPTH.S563264
Checked for plagiarism Yes
Review by Single anonymous peer review
Peer reviewer comments 2
Editor who approved publication: Dr Scott Fraser
Collin T Olevson,1 Anthony P Mai,2 Justin A Schweitzer,3 John P Berdahl,1,3 Tanner J Ferguson1,3
1University of South Dakota, Sioux Falls, SD, USA; 2John A. Moran Eye Center, University of Utah, Salt Lake City, UT, USA; 3Vance Thompson Vision, Sioux Falls, SD, USA
Correspondence: Collin T Olevson, University of South Dakota Sanford School of Medicine, 1400 W 22 nd St, Sioux Falls, SD, 57105, USA, Email [email protected]
Purpose: To evaluate the long-term efficacy of the bimatoprost sustained-release (SR) implant focusing on time to additional intraocular pressure (IOP) lowering intervention and changes in medication burden and IOP, with subgroup analyses by lens status and prior trabecular meshwork (TM) procedures.
Patients and Methods: This retrospective study included patients who received a single bimatoprost SR implant between September 2020 and June 2022 at a single center. Data was obtained from electronic medical records. The primary outcomes were time to failure defined as addition of IOP-lowering medications, procedures, or surgery, changes in topical medication use, and IOP over time. Kaplan-Meier survival analysis and linear mixed-effects models were used to assess overall outcomes and within subgroups.
Results: The study included 223 eyes from 134 patients. At 6-, 12-, and 24-months post-implantation, 67.3%, 38.5%, and 20.5% of eyes, respectively, remained free of additional IOP-lowering treatment. The rates of survival were not statistically significant when stratified by lens status or history of TM procedures. The mean number of topical medications was 1.8 ± 1.3 at baseline and was significantly reduced beginning at 1 month and through 18 months (p < 0.001). There was not a significant IOP decrease post implantation. Subgroup analysis showed no significant differences in IOP and a borderline significant difference in medication use (p = 0.051) between phakic and pseudophakic eyes. Eyes with a history of TM procedures had higher IOP compared to those without prior intervention (p = 0.042), and medication use was not significantly different between groups.
Conclusion: In this retrospective, single-center study the bimatoprost SR implant provided significant reduction in topical medication burden for 18 months. The implant provided six months of freedom from additional IOP lowering interventions in more than half of the eyes with an expected decline. A small group continued to be free from additional IOP lowering intervention for up to 24 months.
Plain Language Summary: Glaucoma is an eye disease that can lead to vision loss if eye pressure is not controlled. The bimatoprost sustained-release implant is a small device placed in the eye that slowly releases medication and can reduce the need for daily eye drops. This study reviewed medical records of patients treated with the implant in routine clinical practice and followed them for up to two years. Outcomes included changes in eye pressure, number of glaucoma medications, and duration of treatment effect. The implant provided stable eye pressure and reduced medication use in many patients, but its effect often declined over time, and additional treatments were frequently required. These results provide real-world information on the performance of the implant outside of clinical trials.
Keywords: open-angle glaucoma, intracameral drug delivery, intraocular pressure reduction, medication reduction
Introduction
Glaucoma remains a leading cause of global blindness and estimates suggest more than 100 million people will suffer from the disease by 2040.1 All current treatment options target the reduction of intraocular pressure (IOP), the only clinically validated risk factor associated with development and progression of the disease.1 The treatment landscape has evolved considerably in recent years with introduction of new topical, laser, and surgical treatment options. These options include multiple classes of topical medications, wearable technologies, laser procedures and surgical devices.1–3
For topical medication use in the treatment of glaucoma, prostaglandin analogues are a common first-line treatment option given their proven efficacy and favorable side effect profile.1,4–6 Although the drops have proven efficacy when used appropriately, there are known challenges with topical medications. These challenges include drop adherence, complex medication regimens and difficulty with drop instillation.5,7 One study found the mean compliance across 12 months for prostaglandin analogues to be 37%.8 An additional study found that up to 50% of patients purposefully discontinue their drops within the first 6 months.9 This has stimulated interest in alternative forms of drug delivery. Recently, bimatoprost, a proven prostaglandin analogue agent effective as a topical medication, was reformulated into an intracameral sustained-release (SR) implant.4 In clinical trials leading to its approval, the bimatoprost SR implant was shown to have comparable efficacy to topical bimatoprost 0.03% and topical timolol 0.5%.4,10 In the clinical trials, the implant was studied in eyes diagnosed with ocular hypertension and open-angle glaucoma and notable exclusions included eyes with narrow angles or reduced central endothelial count.4,10
The bimatoprost SR implant helps reduce medication burden by reducing reliance on eye drops through an intracameral implant designed to elute the drug over the course of 90 days.4 Although nearly all medication was released by day 80 in the Phase I/II clinical trial, it was reported that 40% of eyes survived by 12 months and 28% of eyes survived by 24 months without additional IOP-lowering intervention.4 Given the sustained duration of effect, it is thought that a higher concentration of medication at target tissues produces trabecular meshwork (TM) remodeling which leads to long-term IOP lowering.4,11,12 Additionally, by eluting medication intracamerally, ocular surface and periorbital side effects are limited.10
In addition to clinical trials, several real-world studies have investigated outcomes of the bimatoprost SR implant. These include studies by Ali et al, Wong et al, Xu et al, Teymoorian et al, and Mann et al. These studies reported varying medication reduction from 0.5 to 1.2 drops and survival without IOP lowering treatment ranging from 32% to 77% at 12 to 18 months.13–17 This present study adds to and expands on the real-world time until failure, medication burden, and IOP by examining the implant up to 24 months, incorporating Kaplan-Meier survival curve through 24 months, and utilizing subgroup analyses based on lens status and previous trabecular meshwork procedures.
Materials and Methods
Study Design and Population
This was a retrospective, consecutive case review that included all patients that received their first intracameral bimatoprost SR implant from October 1st, 2020, to May 31st, 2022, within a single practice (Sioux Falls, SD). Approval to access records was granted by the institution. Bilateral implants were included. Patients undergoing selective laser trabeculoplasty (SLT) the same day as the bimatoprost SR implant and repeat bimatoprost SR implants were excluded. All other eyes were included in this study. This study was conducted in adherence to the Declaration of Helsinki and approved by the University of South Dakota Institutional Review Board (IRB-22-70). Informed consent was waived by the Institutional Review Board due to the retrospective nature of this study. Patient confidentiality was maintained throughout the study and data was de-identified at the earliest opportunity.
Surgical Technique
The bimatoprost SR implant was administered using the standard technique described by Craven et al.4 Following implantation, patients were started on a topical antibiotic drop four times per day for four days in the operative eye.
Data Collection
All data were obtained from the electronic health record. Baseline data was collected for each eye from the most recent office visit prior to implantation and included sex, glaucoma type and severity, previous IOP-lowering treatments or procedures, current topical medications, and IOP. At post implantation visits, the IOP and the number of topical medications were collected. In the case of combination medications, each medication was counted separately. Follow up visits were based on days after implantation and collected at one month and every three months as follows: 7–60 days (1 month), 61–150 days (3 months), 151–240 days (6 months), 241–330 days (9 months), 331–420 days (12 months), 421–510 days (15 months), 511–600 days (18 months), 601–690 days (21 months), and 691+ days (24 months). The time to rescue, defined as additional IOP lowering therapies, including medications, lasers, or surgeries, was recorded. The IOPs after the rescue treatment was not censored from further collection. Goldmann applanation tonometry was used for IOP values when available; alternative methods were employed otherwise.
Outcome Measures and Safety Evaluation
The primary outcomes included duration until rescue, number of IOP-lowering medications, and IOP. The duration of efficacy was determined by the time from implantation until rescue, which was defined as addition of any additional IOP lowering therapies. Medication burden was evaluated by comparing the number of topical medications before and after receiving the bimatoprost SR implant. IOP was evaluated by comparing the IOP before implantation to after implantation without addition of other IOP lowering therapies. The secondary outcome included safety of the implant. This was determined by adverse ocular events or need for implant removal.
Analysis
All eyes with available data were used in the “all” group for medications, IOP, and duration of efficacy. Subgroup analyses were performed for eyes with history of minimally invasive glaucoma surgery (MIGS) or selective laser trabeculoplasty (SLT) (the “TM procedure” group) and pseudophakic eyes (the “pseudophakic” group). Survival time was assessed using a Kaplan-Meier survival curve. A p-value of < 0.05 was considered statistically significant. Means are presented with standard deviations. A linear mixed-effects model was used to evaluate changes in medication use and IOP over time, accounting for repeated measures within eyes and variable follow-up intervals. IOP data was censored after initiation of any IOP-lowering therapy and number of glaucoma medications were censored after addition of an IOP-lowering procedure. As this was a retrospective observational study designed to describe real-world outcomes rather than to test a prespecified hypothesis, a formal power calculation was not performed. All eligible eyes meeting inclusion criteria during the study period were included.
Results
Patient Characteristics
The study included 223 eyes from 134 patients who received a bimatoprost implant between September 2020 and June 2022. Baseline characteristics of the included patients are presented in Table 1, and baseline characteristics of the eyes included in the study are shown in Table 2. Of the 223 eyes, 159 were from female patients. The mean age was 77.7 ± 10.6 years. Disease severity ranged from mild to severe open-angle glaucoma, with severe disease being the most common (37.7%).
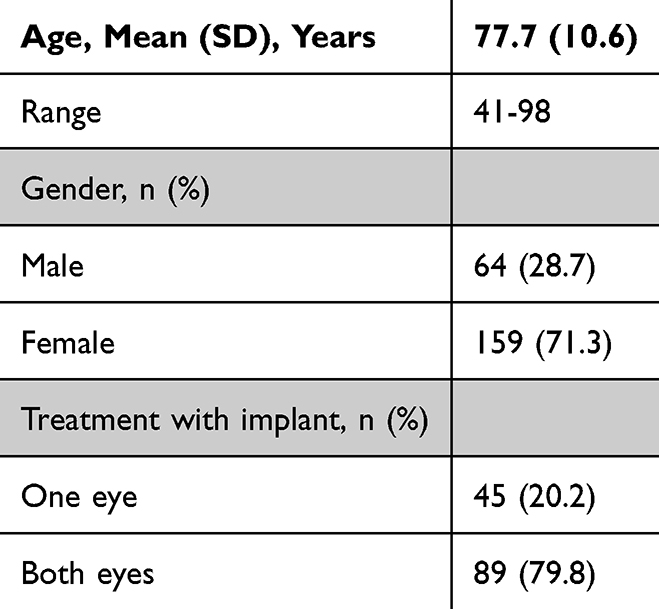 |
Table 1 Patient Demographics |
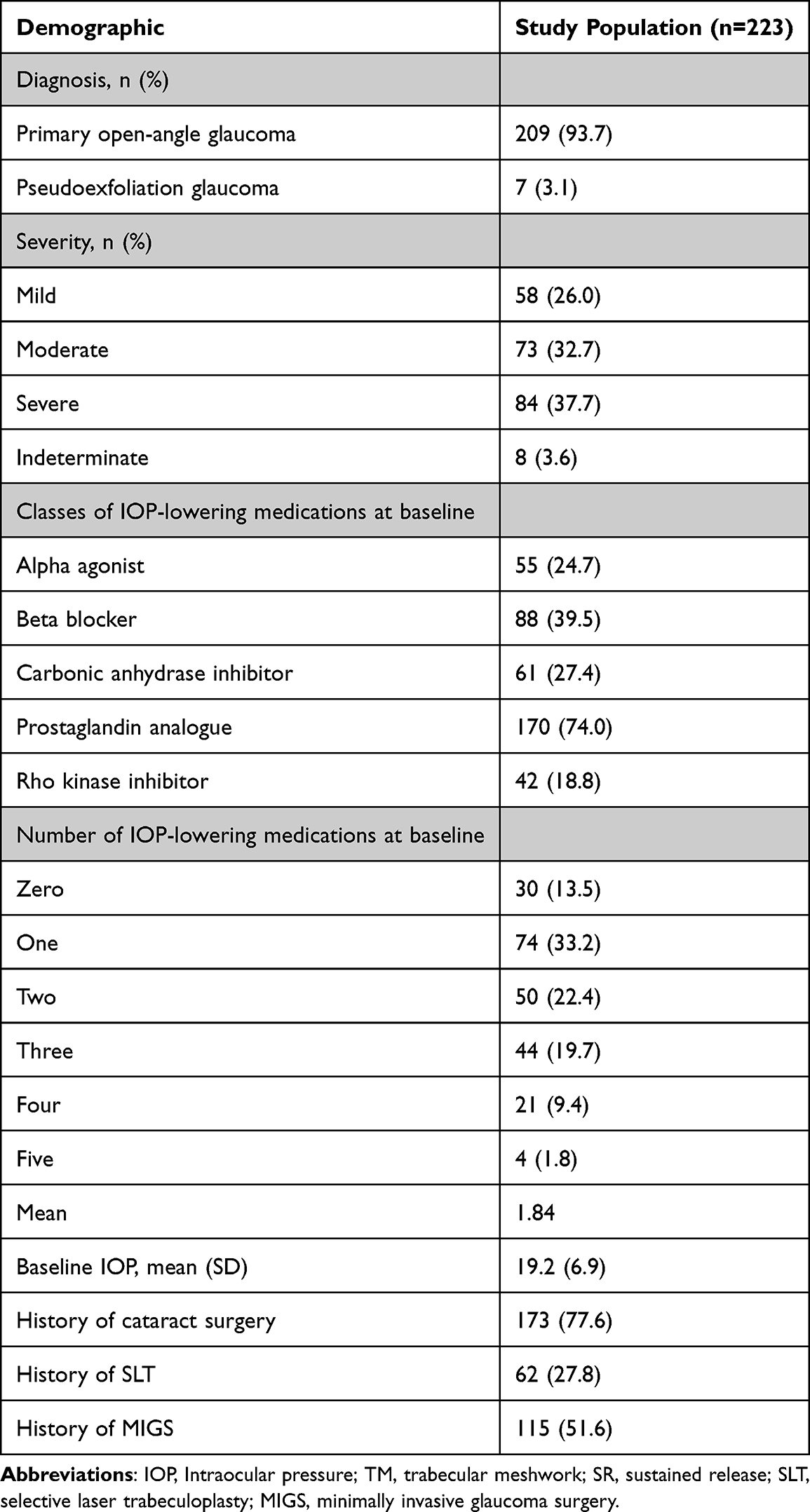 |
Table 2 Individual Eye Demographics |
Duration of Efficacy
A Kaplan–Meier survival curve for all eyes is shown in Figure 1. At 6 months, 67.3% of eyes did not require any additional IOP-lowering treatment; this decreased to 38.5% at 12 months and 20.5% at 24 months.
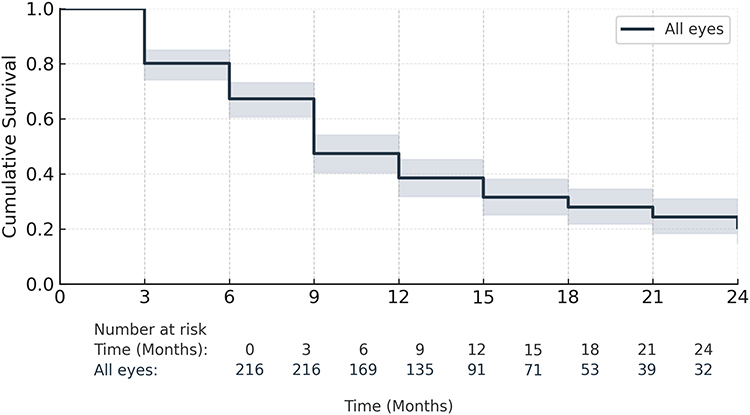 |
Figure 1 Kaplan-Meier survival analysis for all eyes included in the study. |
Subgroup analysis by lens status is shown in Figure 2. Although pseudophakic eyes seemed to have a slightly higher survival compared to phakic eyes, the difference was not statistically significant (p = 0.486). At 6 months, survival was 66.5% in pseudophakic eyes and 68.2% in phakic eyes. By 12 months, survival declined to 40.0% and 31.7%, respectively, and at 24 months, survival was 21.8% and 16.2%, respectively.
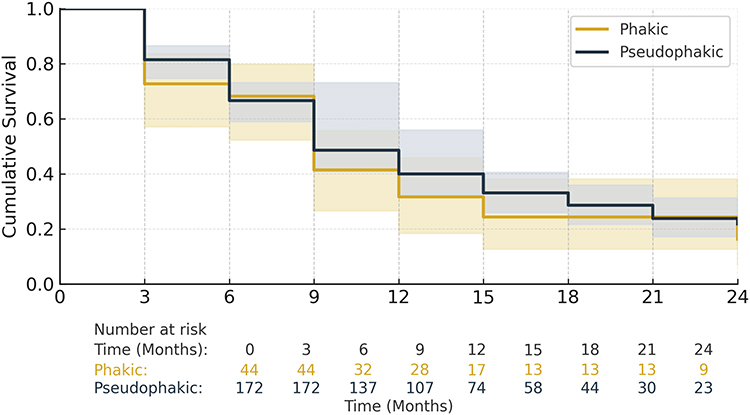 |
Figure 2 Kaplan-Meier survival analysis comparing phakic and pseudophakic eyes. |
Subgroup analysis by TM procedure (MIGS or SLT) is shown in Figure 3. Eyes without prior TM procedures demonstrated higher survival than those with prior TM procedures; however, this difference was not statistically significant (p = 0.097). At 6 months, survival was 75.0% in eyes without prior TM procedures and 60.4% in eyes with prior TM procedures. By 12 months, survival was 47.7% and 30.2%, respectively. At 24 months, survival was similar between groups (20.6% vs 20.5%).
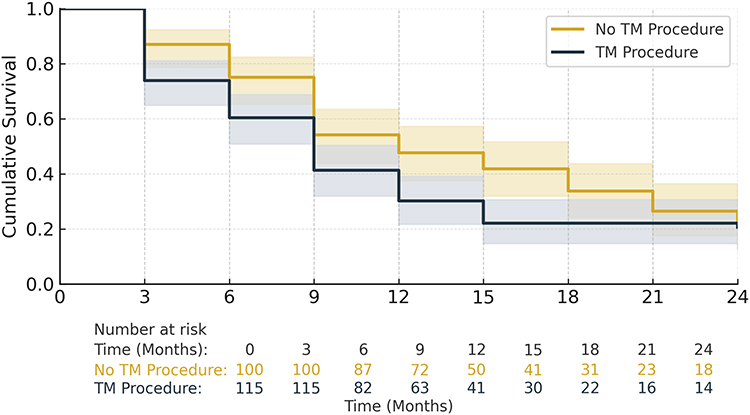 |
Figure 3 Kaplan-Meier survival analysis comparing eyes with history of a TM procedure and those without history of any procedures. |
Of the 162 eyes that experienced treatment failure, 70.4% resumed topical medications, 18.5% underwent glaucoma surgery, 11.7% received SLT, and 1.2% underwent repeat bimatoprost SR implantation.
Medications
At baseline, the mean number of topical medications was 1.8 ± 1.3. The most used agents were prostaglandin analogues (74.0%), followed by beta-blockers (39.5%). Overall, 86.5% of eyes were on one or more topical medications at baseline. At one month following bimatoprost SR implantation, 53.4% of eyes were medication-free. The distribution at that time was: 0 (53.4%), 1 (13.9%), 2 (21.1%), 3 (8.5%), and 4 (3.1%) medications.
Medication use over time is shown in Figure 4. There was a statistically significant reduction in medication use beginning at 1 month (p < 0.001), which persisted through 18 months. At 21 and 24 months, the reduction was no longer statistically significant (p > 0.09). Eyes with severe glaucoma required significantly more medications over time (+1.95 medications, p = 0.01).
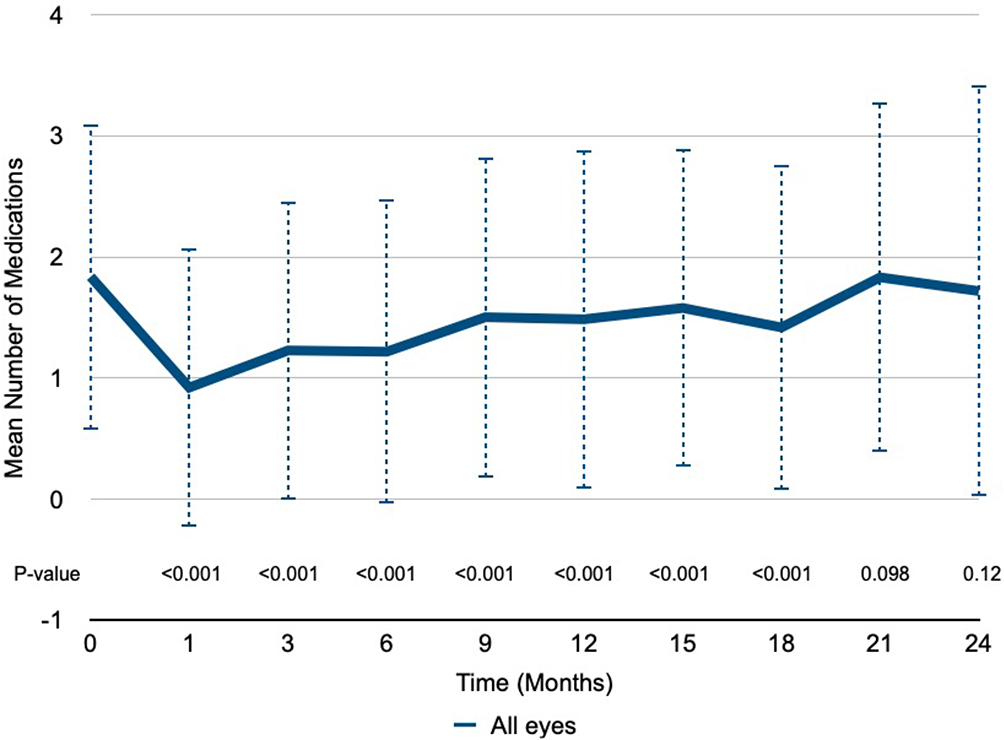 |
Figure 4 Mean number of topical IOP-lowering medications used at baseline and during follow-up in all eyes with p-values. Data are presented as mean ± standard deviation. |
Subgroup analysis by lens status (Figure 5) showed that pseudophakic eyes trended toward higher average medication use (+0.34 medications), although this was borderline significant (p = 0.051). Subgroup analysis by TM procedure history (Figure 6) showed no statistically significant difference in medication use (p = 0.136).
 |
Figure 5 Mean number of topical IOP-lowering medications used at baseline and during follow-up in pseudophakic and phakic eyes. Data are presented as mean ± standard deviation. |
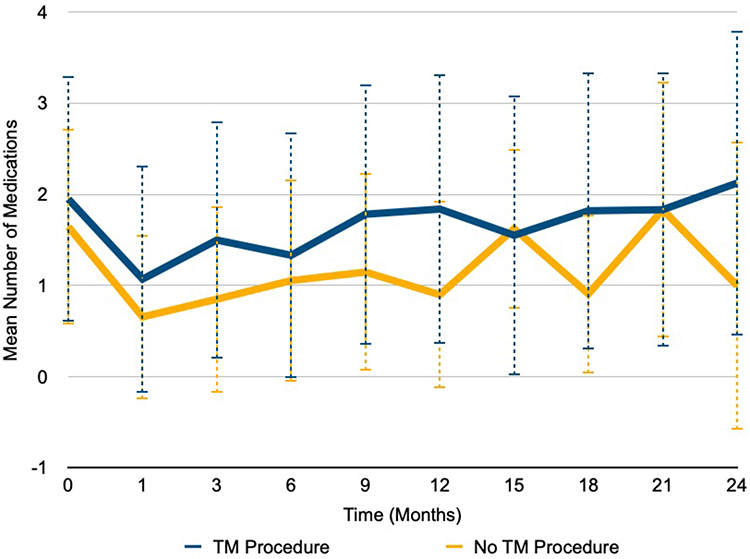 |
Figure 6 Mean number of topical IOP-lowering medications used at baseline and during follow-up in eyes with a history of TM procedure and those without. Data are presented as mean ± standard deviation. |
IOP
Average IOP at baseline and across follow-up is shown in Figure 7. No significant change in IOP was observed through 21 months. At 24 months, however, there was a statistically significant mean reduction of 4.92 mmHg compared to baseline (p < 0.001). Glaucoma severity did not significantly affect IOP (all p-values > 0.25).
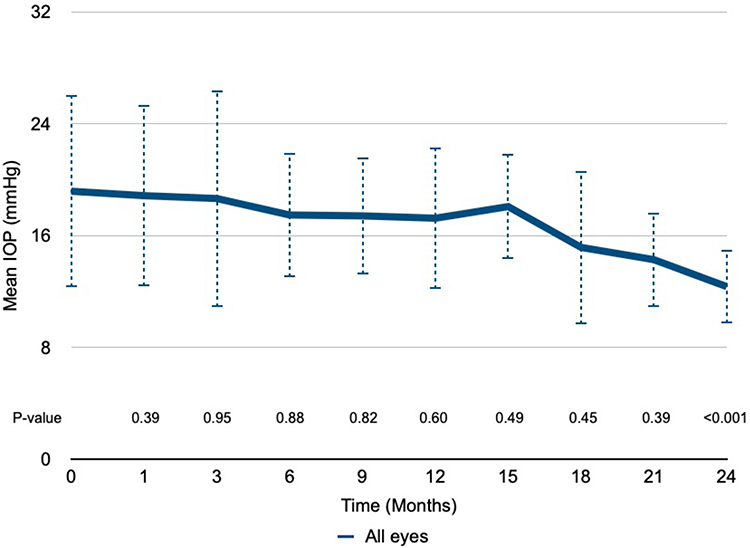 |
Figure 7 Mean intraocular pressure (IOP) measured at baseline and subsequent time points in all eyes with p-values. Data are presented as mean ± standard deviation. |
Subgroup analysis by lens status (Figure 8) showed no significant difference in IOP between phakic and pseudophakic eyes (p = 0.955). In contrast, subgroup analysis by TM procedure history (Figure 9) revealed a significant difference. Eyes with a history of TM procedures had 1.65 mmHg higher IOP on average compared to those without prior TM procedures (p = 0.042).
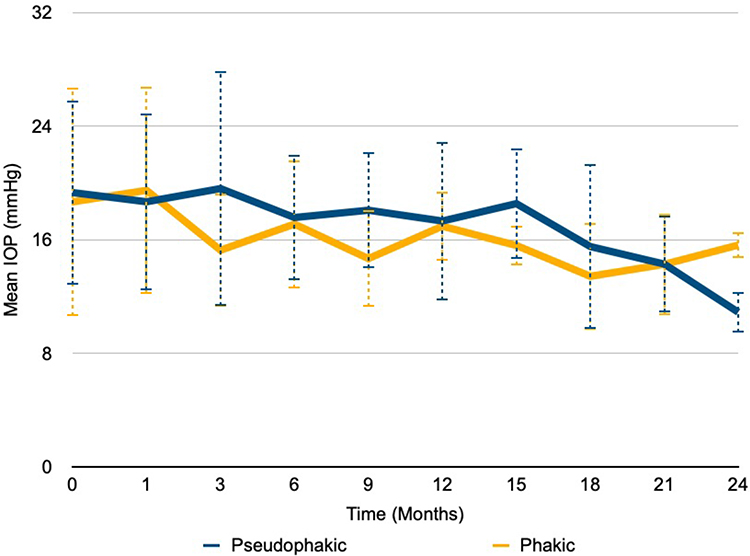 |
Figure 8 Mean intraocular pressure (IOP) measured at baseline and subsequent time points in pseudophakic and phakic eyes. Data are presented as mean ± standard deviation. |
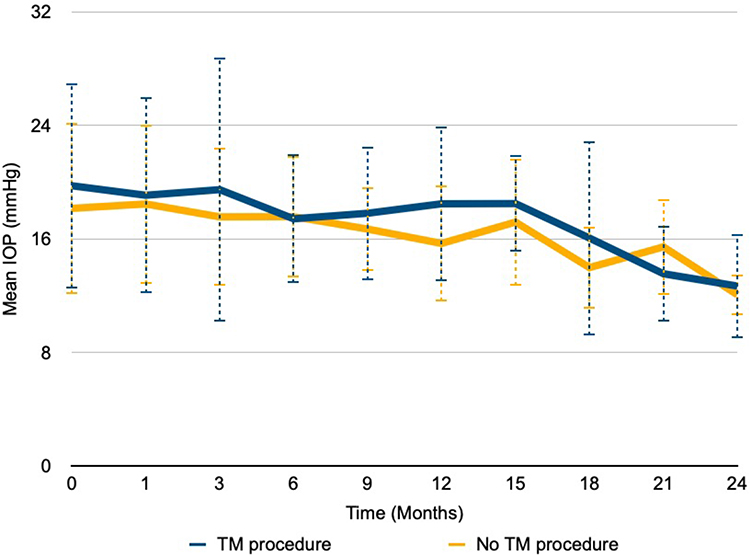 |
Figure 9 Mean intraocular pressure (IOP) measured at baseline and subsequent time points eyes with a history of TM procedure and those without. Data are presented as mean ± standard deviation. |
Safety
The overall safety profile of the bimatoprost SR implant was favorable. Five adverse events were reported, including transient blurred vision, pain, and mild irritation, all of which resolved without lasting effects. One case of disc hemorrhage and one case of macular edema were reported following implantation, both of which resolved.
Discussion
Although topical IOP-lowering drops are among the first-line treatments for glaucoma, patients may experience challenges with their use. These challenges include adherence issues, complex regimens, and difficulty with drop instillation.5,7 Bimatoprost was reformulated as an intracameral SR implant to help address these challenges.
The rates of survival without additional treatment in this study were 67.3% at 6 months, 38.5% at 12 months, and 20.5% at 24 months. These are similar to the phase I/II trial, which reported 68%, 40%, and 28% at the same time points.4 In real-world studies, Ali et al reported survival rates of 69.2% at 3 months, 55.0% at 6 months, and 40.5% at 12 months.12 Xu et al reported a 67.4% survival rate at an average of 260 ± 122 days.14 The ARGOS study by Mann et al showed even higher rates: 88.6% at 6 months, 83.7% at 12 months, and 77.7% at 18 months.17 Differences in study design, rescue definitions, and patient selection likely explain the variability in reported survival. Several eyes in our study were rescued within 80 days, a period in which the implant is still expected to be eluting medication.4,11 In these cases, early rescue may reflect inadequate response due to disease severity or the need for further IOP lowering, rather than early loss of implant efficacy. Baseline IOP in our cohort was higher than in several prior real-world studies, including Teymoorian et al (+2.6mmHg), Ali et al (+3.2 mmHg), Wong et al (+0.7mmHg), and Xu et al (+2.7mmHg). Similarly, our cohort had a higher proportion of eyes with severe glaucoma at baseline than Teymoorian et al (17.8%) and Wong et al (26.3%).
In this retrospective study, bimatoprost SR demonstrated a significant reduction in the mean number of topical medications over 18 months. At 3 months, the mean reduction in topical medications was 0.61 medications and 0.36 at 12 months. A decrease in IOP-lowering medications was also observed in four other retrospective studies of bimatoprost SR, with reported mean reductions of 0.60 to 1.2 topical medications at 3 months and 0.51 to 1.2 topical medications at 12 months.13–16 Although the effect of bimatoprost SR was similar to what has been reported in previous studies soon after implantation, the effect tapered off more quickly in our study. As mentioned above, baseline IOP and glaucoma severity were higher in our cohort. Additionally, our study censored data after IOP-lowering procedures. These differences may partly account for the smaller reduction in topical medications compared to prior reports. Differences in clinical practice, such as thresholds for reintroducing medications, may also contribute to variability between studies.
In both phakic and pseudophakic eyes, a reduction in the mean number of topical medications was sustained through 18 months. However, pseudophakic eyes required more medications on average with a borderline significant difference (p = 0.051). One possible explanation for this finding is that pseudophakic eyes, which may already have enhanced aqueous outflow following cataract surgery, may respond less to the implant, leading to additional topical therapy despite similar baseline IOPs.18 There was no significant difference in mean number of topical medications in eyes with and without a history of TM procedures (p = 0.136). This is similar to what has been reported in a retrospective study by Wonget al, which found that SLT history did not affect medication burden following implantation.14 These findings suggest that lens status may influence medication burden following implantation, while TM procedures do not appear to have a significant effect.
Although there was a significant decrease in mean IOP at 24 months, no significant change in IOP was observed at any earlier time point compared to baseline. This late IOP decrease likely reflects censoring of rescued eyes and a survivor bias, rather than a late sustained or peak treatment effect. Greater absolute reductions in IOP have been reported in previous retrospective studies, with decreases between 0.93 to 3.3 mmHg in all eyes between 6 and 12 months, compared to a 0.07 mmHg decrease and 0.38 mmHg increase at 6 and 12 months in this study.14–16 In our study, IOP was censored after any form of rescue with the goal to remove confounding IOP reduction by eye drops or surgery. Additionally, in our clinical practice, the bimatoprost SR implant is often used to replace an existing medication. The goal in these cases is not necessarily further IOP reduction, but rather to reduce eye drop burden while preserving current IOP. This therapeutic goal may partially explain why our cohort showed minimal changes in mean IOP compared to prior studies that reported greater reductions.
In both phakic and pseudophakic eyes, no significant difference in IOP was observed overall (p = 0.955), although pseudophakic eyes trended toward a slightly higher IOP. Similarly, while IOP decreased in eyes with and without a history of TM procedures, the reduction was smaller in eyes with prior TM procedures (p = 0.042). This suggests that eyes with prior TM procedures may be less responsive to the bimatoprost SR implant. These findings are different than those reported by Wong et al, which found no association between SLT history and IOP reduction.14 Potential reasons for this discrepancy include the shorter follow up time (27.8 weeks) in Wong et al, which may not capture long-term trends. Additionally, Wong et al did not censor IOP after additional topical medications or surgical intervention, potentially underestimating differences between the two groups. Finally, combining MIGS and SLT into a single category in our study may have introduced confounding, and the response may be attributable to prior MIGS rather than SLT. Overall, the subgroup trends support the idea that patient-specific factors such as prior surgical history may help predict response to the implant and should be considered in treatment planning.
Safety outcomes in this study were favorable. Five adverse events were reported: transient blurred vision, pain, and mild irritation (each resolving spontaneously), as well as one case each of disc hemorrhage and macular edema. No implant removals were required. As follow-up typically occurred more than one week after implantation, transient adverse effects may have resolved prior to follow-up visits. However, endothelial counts were not routinely performed, and adverse events were not systematically captured, limiting interpretation of safety. Safety outcomes for the bimatoprost SR implant have been favorable in previous studies. The most reported adverse effects are transient and likely related to the procedure itself.4,14,16 In the Phase III study, corneal and inflammatory adverse events were reported with corneal endothelial cell loss being the most common.10
This study’s strengths include its real-world applicability, as patients were not preselected, representing everyday clinical practice. The implant was evaluated in the context of various ocular histories and ongoing treatments. The inclusion of varied ranges of disease severity, surgical history, and lens status allowed for subgroup analysis. This study incorporated Kaplan-Meier survival analysis to characterize treatment duration. The use of a linear mixed effects model was another methodological strength. This model allows analysis of longitudinal IOP and medication use while accounting for repeat measurements from the same eye and missing data points. Overall, this allowed for a more accurate estimate of effects over time in a retrospective study such as this.
However, the study also has limitations. These include the lack of a randomized control trial design and the gaps in data due to its retrospective nature. Without a formal study protocol, follow-up was not standardized, leading to missing data at certain time points and potential IOP variability between visits. Additionally, bilaterality was not modeled at the patient level, and power was not formally calculated. Although a linear-mixed effects model was used to account for repeated measures and variable follow-up, more complex patient-level approaches could be considered in future analyses. The lack of a control group prevents definitive conclusions about treatment efficacy relative to other interventions. In addition, the absence of a washout period before implant administration makes it difficult to isolate the true effect of the implant on IOP. Baseline IOP and medication use were likely influenced by concurrent therapies at the time of implantation, which may confound results of treatment-related changes.
Overall, this study supports the bimatoprost SR implant as a tool for reducing topical medication burden and improving adherence in appropriately selected patients, particularly in the short to medium term. However, its IOP-lowering effects appear modest and inconsistent, and freedom from additional treatment declines substantially by 12 to 24 months. These results should be generalized cautiously to similar single-center, real-world settings, and future work should focus on standardized data collection, patient-level modeling, and formal safety evaluation.
Conclusion
In this retrospective, single-center study the bimatoprost SR implant provided significant reduction in topical medication burden for 18 months. The implant provided six months of freedom from additional IOP lowering interventions in more than half of the eyes with an expected decline. A small group continued to be free from additional IOP lowering intervention for up to 24 months.
Data Sharing Statement
The data set collected and analyzed for this present study is available from the corresponding author per reasonable request.
Disclosure
JAS reports consulting fees from Alcon, Aldeyra, Allergan, Bausch and Lomb, Bruder, Sight Sciences, Dompe, Zeiss, Visus, Science Based Health, Tarsus, Santen, Sun, Reichert, Glaukos, MediPrint, LKC, Viatris, Thea, Heru, Lenz, and Harrow. JPB reports consulting fees from AbbVie, Aerpio, ALJ Health, Alcon, Aldeyra, Aquea Health, Aurion Biotech, Avelino, Balance Ophthalmics, Bausch and Lomb, Belkin, CorneaGen, Dakota Lions Eye Bank, Elios Vision Inc., Expert Opinion, Glaukos, Gore, Greenman, Horizon Surgical, Iacta Pharmaceuticals, Imprimis, iRenix, IVERIC bio, Johnson and Johnson, Kala, Layer Bio, MELT Pharmaceuticals, MicroOptx, New World Medical, Ocular Surgical Data, Ocular Therapeutix, Omega Ophthalmic, Orasis, Oyster Point, RxSight, Santen, Sight Sciences, Tarsus, TavoBio, Tear Clear, Tissue Gen, Verana Health, Versea Biologics, Vertex Ventures, and ViaLase. He also reports ownership interest in Aquea Health, Aurion Biotech, Balance Ophthalmics, CorneaGen, Elios Vision Inc., Expert Opinion, Glaukos, Greenman, Iacta Pharmaceuticals, Layer Bio, MELT Pharmaceuticals, Ocular Surgical Data, Omega Ophthalmic, Orasis, Oyster Point, TavoBio, Tear Clear, True North CRO, Vance Thompson Vision, Verana Health, and ViaLase, as well as patents with Balance Ophthalmics, Glaukos, Imprimis, and MELT Pharmaceuticals. TJF reports research support from Alcon and RxSight, consulting fees from Balance Ophthalmics, Glaukos, Johnson & Johnson, and RxSight, and ownership in True North CRO and Greenman. The authors report no other conflicts of interest in this work.
References
1. Weinreb RN, Aung T, Medeiros FA. The pathophysiology and treatment of glaucoma: a review. JAMA. 2014;311(18):1901–1911. doi:10.1001/jama.2014.3192
2. Birnbaum FA, Neeson C, Valle DSD. Microinvasive glaucoma surgery: an evidence-based review. Semin Ophthalmol. 2021;36(8):772–786. doi:10.1080/08820538.2021.1903513
3. Garg A, Gazzard G. Selective laser trabeculoplasty: past, present, future. Eye. 2018;32(5):863–876. doi:10.1038/eye.2017.273
4. Craven ER, Walters T, Christie WC, et al. 24‐month phase i/ii clinical trial of bimatoprost sustained‐release implant (bimatoprost sr) in glaucoma patients. Drugs. 2019;80(2):167–179. doi:10.1007/s40265-019-01248-0
5. Vandebroeck S, Geest SD, Dobbels F, Fieuws S, Stalmans I, Zeyen T. Prevalence and correlates of self-reported nonadherence with eye drop treatment: the Belgian Compliance Study in Ophthalmology (BCSO. J Glaucoma. 2011;20(7):414–421. doi:10.1097/IJG.0b013e3181f7b10e
6. Li F, Huang W, Zhang X. Efficacy and safety of different regimens for primary open-angle glaucoma or ocular hypertension: a systematic review and network meta-analysis. Acta Ophthalmol. 2018;96(3):277–284. doi:10.1111/aos.13568
7. Sleath B, Blalock S, Covert D, et al. The relationship between glaucoma medication adherence, eye drop technique, and visual field defect severity. Ophthalmology. 2011;118(12):2398–2402. doi:10.1016/j.ophtha.2011.05.013
8. Yeaw J, Benner JS, Walt JG, Sian S, Smith DB. Comparing adherence and persistence across 6 chronic medication classes. J Manag Care Pharm. 2009;15(9):728–740. doi:10.18553/jmcp.2009.15.9.728
9. Nordstrom BL, Friedman DS, Mozaffari E, Quigley HA, Walker AM. Persistence and adherence with topical glaucoma therapy. Am J Ophthalmol. 2005;140(4):598–606. doi:10.1016/j.ajo.2005.04.051
10. Medeiros FA, Walters TR, Kolko M, et al. Phase 3, randomized, 20-month study of bimatoprost implant in open-angle glaucoma and ocular hypertension (ARTEMIS 1). Ophthalmology. 2020;127(12):1627–1641. doi:10.1016/j.ophtha.2020.06.018
11. Seal JR, Robinson MR, Burke J, et al. Intracameral sustained-release bimatoprost implant delivers bimatoprost to target tissues with reduced drug exposure to off-target tissues. J Ocul Pharmacol Ther. 2019;35(1):50–57. doi:10.1089/jop.2018.0067
12. Stamer WD, Perkumas KM, Kang MH, et al. Proposed mechanism of long-term intraocular pressure lowering with the bimatoprost implant. Invest Ophthalmol Vis Sci. 2023;64(3):15. doi:10.1167/iovs.64.3.15
13. Ali AA, Elescano DA, Grover DS. Bimatoprost SR for glaucoma therapy implanted at the slit-lamp in a real-world setting. Clin Ophthalmol. 2024;18:1371–1377. doi:10.2147/OPTH.S450220
14. Wong MK, Bowers ME, Ventimiglia J, et al. Short-term outcomes of bimatoprost sustained-release intracameral implant in glaucoma. J Glaucoma. 2023;32(9):738–743. doi:10.1097/IJG.0000000000002271
15. Xu W, Zhou P, Kansara ND, et al. Intraocular pressure and eyedrop usage reduction with intracameral bimatoprost implant. J Ocul Pharmacol and Ther. 2023;39(6):398–403. doi:10.1089/jop.2023.0013
16. Teymoorian S, Craven ER, Nguyen L, et al. Real-world study of the effectiveness and safety of intracameral bimatoprost implant in a clinical setting in the United States. Clin Ophthalmol. 2024;18:187–199. doi:10.2147/OPTH.S445005
17. Mann E, Kammer JA, Sawhney G, et al. Prospective 18‐month study of bimatoprost intracameral implant in patients with open‐angle glaucoma or ocular hypertension in US clinical practice. Drugs. 2025;85(3):397–414. doi:10.1007/s40265-025-02157-1
18. Alaghband P, Beltran-Agulló L, Galvis EA, et al. Effect of phacoemulsification on facility of outflow. Br J Ophthalmol. 2018;102(11):1520–1526. doi:10.1136/bjophthalmol-2017-311548
 © 2025 The Author(s). This work is published and licensed by Dove Medical Press Limited. The
full terms of this license are available at https://www.dovepress.com/terms
and incorporate the Creative Commons Attribution
- Non Commercial (unported, 4.0) License.
By accessing the work you hereby accept the Terms. Non-commercial uses of the work are permitted
without any further permission from Dove Medical Press Limited, provided the work is properly
attributed. For permission for commercial use of this work, please see paragraphs 4.2 and 5 of our Terms.
© 2025 The Author(s). This work is published and licensed by Dove Medical Press Limited. The
full terms of this license are available at https://www.dovepress.com/terms
and incorporate the Creative Commons Attribution
- Non Commercial (unported, 4.0) License.
By accessing the work you hereby accept the Terms. Non-commercial uses of the work are permitted
without any further permission from Dove Medical Press Limited, provided the work is properly
attributed. For permission for commercial use of this work, please see paragraphs 4.2 and 5 of our Terms.