Back to Journals » Therapeutics and Clinical Risk Management » Volume 22
Retrospective Analysis: Comparative Effects of General Anesthesia versus Quadratus Lumborum Block-Supplemented General Anesthesia on Postoperative Outcomes in Patients Undergoing Laparoscopic Myomectomy
Received 5 September 2025
Accepted for publication 21 December 2025
Published 9 January 2026 Volume 2026:22 561612
DOI https://doi.org/10.2147/TCRM.S561612
Checked for plagiarism Yes
Review by Single anonymous peer review
Peer reviewer comments 2
Editor who approved publication: Professor Garry Walsh
Ruchun Yan, Man Kuang
Department of Gynecology, Renmin Hospital, Hubei University of Medicine, Shiyan, Hubei, 442000, People’s Republic of China
Correspondence: Man Kuang, Email [email protected]
Background and Objective: This retrospective study analyzed to compare the effects of general anesthesia (GA) versus combined anesthesia (CA) on postoperative pain and negative emotions in patients undergoing uterine fibroid surgery, providing evidence for optimizing anesthesia protocols aiming to achieve more effective analgesia and improve patient satisfaction scores.
Methods: A retrospective analysis was conducted on data from 148 patients who underwent uterine fibroid surgery at a tertiary hospital between April 2023 and December 2024. Patients were divided into a control group (GA) and a study group (CA) based on anesthesia type. The control group received conventional GA, while the study group received ropivacaine quadratus lumborum block (QLB) combined with GA. After propensity score matching (PSM), 74 patients were included in each group. The primary outcome was postoperative 2– 12h visual analog scale (VAS) pain scores. Secondary outcomes included stress indicators (ACTH, Cor), emotional scales (SAS/SDS), cognitive function (MMSE), and sleep quality (PSQI).
Results: The study group had shorter anesthesia duration, postoperative flatus time, postoperative ambulation time, and hospital stay compared to the control group (all P< 0.05). VAS scores at 2h, 4h, 8h, and 12h postoperatively were significantly lower in the study group (all P< 0.05). Preoperative differences in emotional, stress, cognitive, and sleep indicators were not statistically significant (all P> 0.05). Postoperatively, the study group showed significantly lower SAS/SDS scores, ACTH/Cor levels, and PSQI scores, alongside higher MMSE scores compared to the control group (all P< 0.05).
Conclusion: Combined anesthesia effectively reduces postoperative pain and negative emotions in uterine fibroid patients, lowers stress levels, improves sleep quality, and promotes rapid recovery, making it worthy of clinical promotion.
Keywords: general anesthesia, combined anesthesia, uterine fibroids, pain, negative emotions, stress response, comparative study
Introduction
Uterine fibroids, the most common benign tumors in the female reproductive system, exhibit a rising incidence, significantly impacting the quality of life and reproductive health of women of childbearing age. According to clinical statistics, the incidence rate of uterine fibroids among women of childbearing age is 20%–30%, of which the catastrophic effect of perioperative pain is the most significant for patients aged 35–45 years - the actual pain score of patients in this age group due to preoperative anxiety is 30% higher than that of non anxiety group, and the postoperative pain demand increases by 50%, forming a vicious circle of “pain anxiety”. Surgical treatment remains the primary definitive intervention, with laparoscopic minimally invasive surgery becoming the mainstream approach due to advantages such as minimal trauma and rapid recovery.1–3 However, the choice of anesthesia protocol not only directly affects intraoperative hemodynamic stability but also closely relates to postoperative pain control, psychological recovery, and long-term prognosis. Traditional general anesthesia (GA) provides stable surgical conditions but may induce exaggerated stress responses, postoperative cognitive dysfunction (POCD), and sleep rhythm disturbances. In contrast, regional block combined anesthesia, through multimodal analgesia mechanisms, has been proven to reduce opioid consumption and alleviate neuroinflammatory responses, emerging as a crucial direction for optimizing perioperative management.
Recent studies indicate that inadequate postoperative pain management can lead to a vicious cycle of “pain-stress-anxiety,” significantly prolonging hospital stays and increasing medical costs. Patients with uterine fibroids often experience complex somatic and visceral pain due to surgical involvement of the pelvic nerve plexus,4,5 making single-mode anesthesia inadequate for precise analgesia. This study compared the application effects of ropivacaine quadratus lumborum block combined anesthesia versus GA in uterine fibroid surgery. By integrating five dimensions—postoperative VAS pain scores, stress indicators (ACTH, Cor), emotional scales (SAS/SDS), cognitive function (MMSE), and sleep quality (PSQI)—it established a comprehensive postoperative recovery assessment system. In this study, “negative emotions” specifically refers to anxiety/depression states quantified through the SAS/SDS scale (scores ≥ 50 indicate clinical significance), while patient satisfaction is evaluated through a 5-point Likert scale (1=very dissatisfied, 5=very satisfied), reflecting emotional state and overall experience respectively - the former focuses on psychological pathology dimensions, while the latter covers 12 service dimensions such as pain control and recovery speed, forming a complementary evaluation system. This study aims to provide high-level evidence-based medical evidence for optimizing anesthesia protocols in gynecological surgery.
This study strictly follows the ERAS concept and achieves three core goals of multimodal analgesia, reducing stress reactions, and promoting rapid recovery through QLB supplemented GA. We hypothesize that QLB combined with GA significantly reduces postoperative VAS scores and improves emotional outcomes. The primary endpoint is the VAS score at 24h post-surgery; secondary endpoints include emotional scores (HADS-A/D) and opioid consumption.
Materials and Methods
Study Design
This study retrospectively analyzed 148 patients who underwent uterine fibroid surgery between April 2023 and December 2024 using a predetermined protocol. Automatically screen patients who meet the inclusion criteria (laparoscopic surgery, ASA I–II level) through the electronic medical record system, with exclusion criteria including malignant tumors, severe complications, etc. The data verification process adopted a blinded approach to minimize bias: two researchers independently reviewed the anesthesia records and postoperative follow-up data without access to group allocation information. Any discrepancies were resolved by a third senior anesthesiologist who was also blinded to the anesthesia type, ensuring data integrity.
PSM was performed using logistic regression to balance baseline characteristics between the two groups. The following clinical parameters were included as matching criteria: age, BMI, ASA classification, duration of surgery, and preoperative comorbidities (eg, hypertension, diabetes). After matching, 74 patients were included in each group, ensuring no significant differences in baseline characteristics (P>0.05). Table 1 lists all matching criteria.
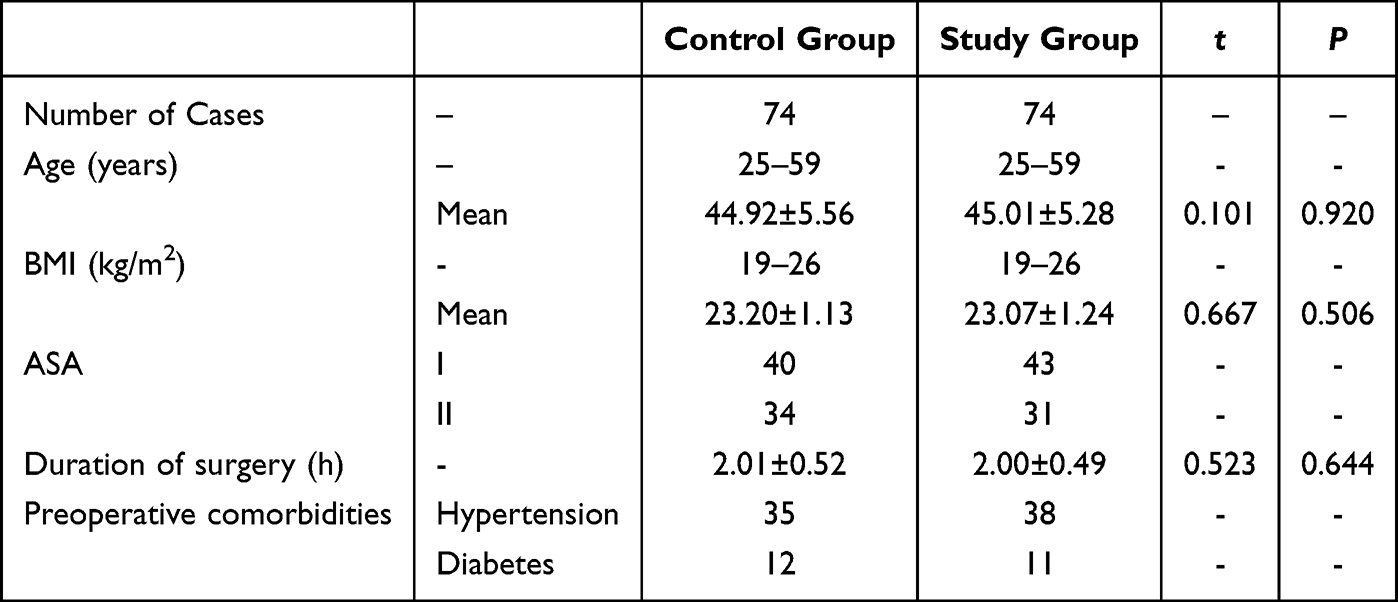 |
Table 1 Comparison of Baseline Characteristics Between Two Groups |
Patient Selection
Inclusion Criteria
Clinically diagnosed with uterine fibroids and eligible for laparoscopic myomectomy,6,7 scheduled for the procedure.
No history of anesthesia drug allergy; complete clinical records.
No recent fertility plans; ASA classification I–II; BMI <28 kg/m2; no abdominal surgery within the past three years.
Exclusion Criteria
Suspected malignant transformation of uterine fibroids or severe pelvic adhesion.
Concurrent gynecological diseases requiring simultaneous treatment (eg, ovarian cysts).
Central or peripheral neuropathy.
Organ dysfunction (cardiac, hepatic, renal, etc)., coagulation disorders, or thyroid dysfunction.
Use of anticoagulants, analgesics, sedatives, or antidepressants within three months prior to enrollment.
Acute/chronic infectious diseases or immunodeficiency.
History of severe spinal trauma.
Requirement for postoperative ICU admission.
Anesthesia Protocols
Both groups underwent laparoscopic myomectomy using a three-port laparoscopic technique, with CO2 pneumoperitoneum pressure maintained at 12 mmHg (1 mmHg = 0.133 kPa). The control group all patients received consistent opioid-free GA: propofol 2mg/kg induction, remifentanil 0.1–0.3μg/kg/min infusion, and rocuronium 0.6mg/kg. QLB used 0.25% ropivacaine 20mL. The study group received ropivacaine quadratus lumborum block combined with GA as follows: Upon entering the operating room, patients first underwent intravenous access establishment and vital sign monitoring, followed by quadratus lumborum block. For block implementation, patients were placed in the supine position. An M-Turbo ultrasound system with a 2–5 MHz low-frequency probe was positioned at the mid-axillary line between the iliac crest and subcostal margin. After visualizing the external oblique, internal oblique, and transversus abdominis muscles, the probe was slightly posteriorly adjusted to focus on the elliptical quadratus lumborum muscle at the junction of the external and internal oblique muscles. A 22G regional anesthesia needle was inserted under ultrasound guidance using an in-plane technique, with the tip precisely positioned at the gap between the deep layer of the external oblique muscle and the posterior aspect of the quadratus lumborum. Initially, 2–4 mL of 0.9% sodium chloride solution was injected to facilitate drug diffusion. After confirming no blood aspiration, 20 mL of 0.25% ropivacaine was slowly administered into the unilateral quadratus lumborum region. Following completion of one-sided block, the probe was repositioned to the contralateral side, and the same technique was applied for contralateral quadratus lumborum block. Anesthesia induction utilized propofol at 2 mg/kg, fentanyl at 300 μg/kg, and vecuronium bromide at 1 mg/kg, followed by endotracheal intubation and initiation of mechanical ventilation. Anesthesia maintenance involved continuous infusion of remifentanil at 0.1–0.3 μg/(kg·min) and propofol at 4–6 mg/(kg·h). Both groups received standardized postoperative analgesia: fentanyl 100 μg/kg and azasetron 10 mg mixed into 100 mL of 0.9% sodium chloride solution, administered via intravenous patient-controlled analgesia pump at 2 mL/h with a 15-minute lockout interval and 0.5 mL per bolus.
Outcome Measures
Surgical Parameters: Included anesthesia duration, postoperative awakening time, postoperative flatus time, postoperative first ambulation time, and total hospital stay.
Pain Intensity: Assessed using the Visual Analog Scale (VAS) at 2, 4, 8, and 12 hours postoperatively. Scores range from 0 to 10, with higher values indicating greater pain severity.
Stress Indicators: Measured through adrenocorticotropic hormone (ACTH) and cortisol (Cor) levels. Preoperative and postoperative 12-hour morning fasting venous blood samples were collected, centrifuged for serum separation, stored at −80°C, and analyzed using the Mindray BS-280 automatic biochemical analyzer.
Negative Emotions: Evaluated using the Self-Rating Anxiety Scale (SAS) and Self-Rating Depression Scale (SDS). The SAS uses a threshold of 50 points to categorize mild (50–59), moderate (60–69), and severe anxiety (≥70). The SDS uses a threshold of 53 points to categorize mild (53–62), moderate (63–72), and severe depression (≥73), with higher scores indicating greater emotional distress.
Cognitive Function: Assessed preoperatively and at discharge using the Mini-Mental State Examination (MMSE), with a maximum score of 30. A threshold of 26 points was used to identify cognitive impairment; higher scores indicate better-preserved cognitive function.
Sleep Quality: Evaluated preoperatively and at discharge using the Pittsburgh Sleep Quality Index (PSQI), with a total score of 21. Scores are inversely correlated with sleep quality; lower values indicate better sleep quality, while higher values suggest increased sleep disturbance risk.
Statistical Analysisf
Sample size was calculated using G*Power 3.1.9.7 with α=0.05, power=0.8, and effect size d=0.5, requiring 65 patients per group. Accounting for 10% dropout, 148 patients were enrolled.
Image processing was conducted using GraphPad Prism 8 software. Data organization and statistical analysis were performed with SPSS 26.0 software. Continuous variables are presented as mean ± standard deviation ( ±s) and compared using t-tests. Categorical variables are expressed as rates (%) and analyzed using chi-square (χ2) tests. The significance threshold was set at P<0.05, indicating statistically significant differences.
±s) and compared using t-tests. Categorical variables are expressed as rates (%) and analyzed using chi-square (χ2) tests. The significance threshold was set at P<0.05, indicating statistically significant differences.
Results
Baseline Characteristics
The control group comprised 74 patients aged 25–59 years (mean 44.92±5.56 years), with body mass index (BMI) ranging 19–26 kg/m2 (mean 23.20±1.13 kg/m2). ASA classifications included 40 cases in grade I and 34 cases in grade II. The mean duration of operation was 2.01±0.52h. There were 35 cases of hypertension and 12 cases of diabetes. The study group included 74 patients aged 25–59 years (mean 45.01±5.28 years), with BMI 19–26 kg/m2 (mean 23.07±1.24 kg/m2). ASA classifications comprised 43 cases in grade I and 31 cases in grade II. The mean duration of operation was 2.00±0.49h. There were 38 cases of hypertension and 11 cases of diabetes. No significant differences in baseline characteristics were observed between the two groups (P>0.05). See Table 1.
Surgical Parameters
The study group demonstrated shorter anesthesia duration, postoperative flatus time, postoperative ambulation time, and hospital stay compared to the control group (1.49±0.52 h, 1.55±0.65 h, 4.28±1.08 h, 7.17±1.23 d vs 1.77±0.56 h, 2.23±0.94 h, 5.94±1.12 h, 9.58±1.79 d), with statistical significance (P<0.05). However, postoperative recovery time was not significantly different between the two groups (P=0.12). See Figure 1.
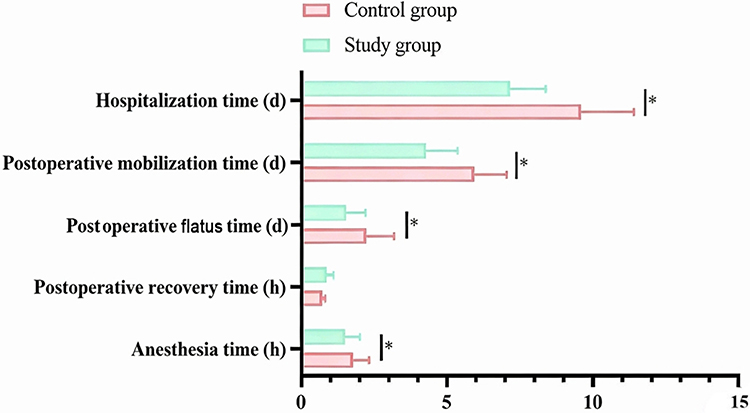 |
Figure 1 Surgical Parameters of the Two Groups. Note: * indicates a significant difference between the two groups (P<0.05). |
Pain Intensity
Postoperative VAS scores at 2h, 4h, 8h, and 12h were significantly lower in the study group compared to the control group (2.23±0.51, 3.14±0.56, 3.97±0.45, 2.46±0.32 vs 3.21±0.45, 4.23±0.56, 5.00±0.71, 3.82±0.65), with P<0.05. See Figure 2.
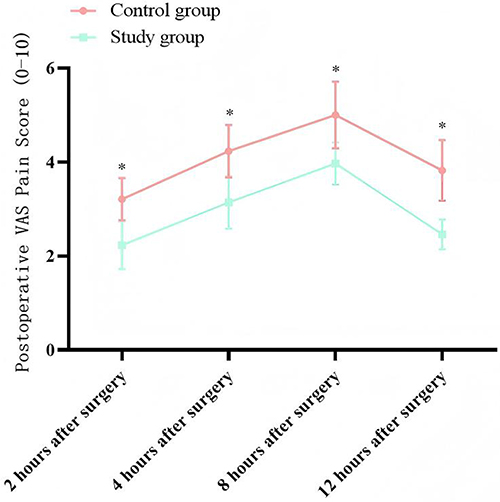 |
Figure 2 Postoperative 2–12h VAS Scores of the Two Groups. Note: * indicates a significant difference between the two groups (P<0.05). |
Stress Indicators
No significant differences in preoperative stress indicators (ACTH, Cor) were observed between the groups (P>0.05). Postoperatively, the study group showed significantly lower ACTH and Cor levels compared to the control group (51.23±2.37 pg/mL, 142.56±5.02 ng/mL vs 69.56±2.22 pg/mL, 182.14±5.11 ng/mL), with P<0.05. See Figure 3.
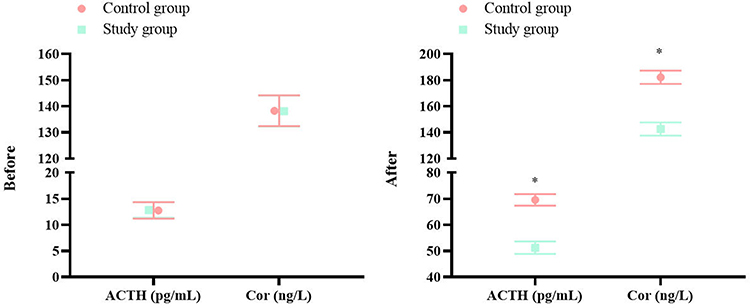 |
Figure 3 Preoperative and Postoperative ACTH/Cor Levels in the Two Groups. Note: * indicates a significant difference between the two groups (P<0.05). |
Negative Emotions
No significant differences in preoperative emotional indicators (SAS, SDS) were observed between the groups (P>0.05). Postoperatively, the study group had significantly lower SAS and SDS scores compared to the control group (30.11±3.28, 34.56±3.71 vs 47.56±3.87, 49.94±3.56), with P<0.05. See Figure 4.
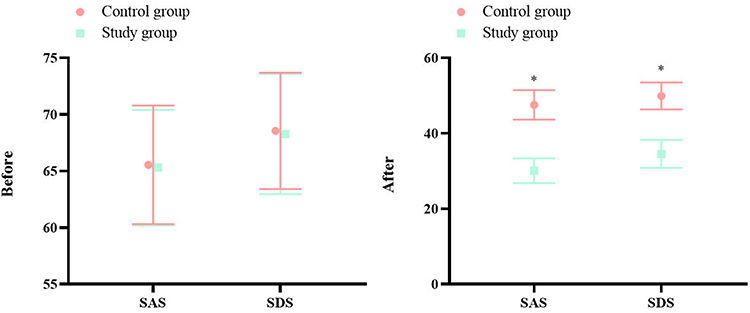 |
Figure 4 Preoperative and Postoperative SAS/SDS Scores in the Two Groups. Note: * indicates a significant difference between the two groups (P<0.05). |
Cognitive Function
No significant differences in preoperative cognitive indicators (MMSE) were observed between the groups (P>0.05). Postoperatively, the study group had a significantly higher MMSE score compared to the control group (27.51±1.23 vs 24.56±1.28), with P<0.05. See Figure 5.
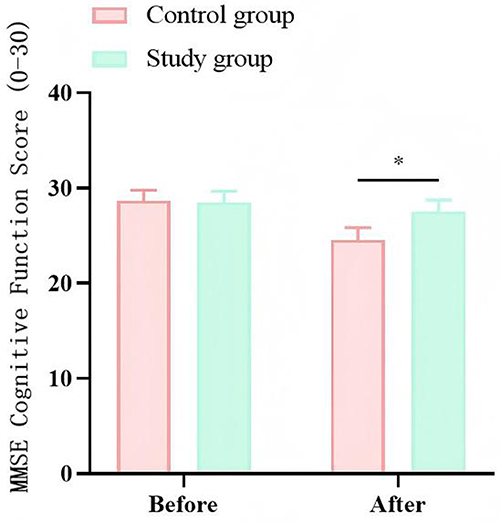 |
Figure 5 Preoperative and Postoperative MMSE Scores in the Two Groups. Note: * indicates a significant difference between the two groups (P<0.05). |
Sleep Quality
No significant differences in preoperative sleep indicators (PSQI) were observed between the groups (P>0.05). Postoperatively, the study group had a significantly lower PSQI score compared to the control group (16.03±1.44 vs 18.74±1.71), with P<0.05. See Figure 6.
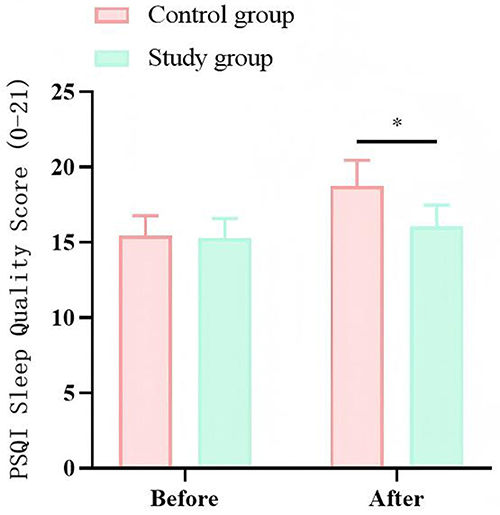 |
Figure 6 Preoperative and Postoperative PSQI Scores in the Two Groups. Note: * indicates a significant difference between the two groups (P<0.05). |
Discussion
Existing studies predominantly focus on single-dimensional indicators (eg, pain scores or stress hormones), lacking systematic evaluation of psychological states, cognitive function, and sleep quality. Among patients with uterine fibroids, preoperative anxiety incidence reaches 35%-50%, while postoperative sleep disturbances are significantly positively correlated with pain intensity, forming a complex bio-psychological interaction network.8–10 Quadratus lumborum block (QLB), as a novel trunk blockade technique, enables local anesthetic diffusion in the fascial space surrounding the quadratus lumborum muscle, simultaneously blocking the anterior branches of thoracolumbar spinal nerves and sympathetic fibers to provide broad analgesic coverage for lower abdominal surgery.11,12 Multiple domestic and international meta-analyses confirm that QLB combined anesthesia reduces opioid consumption by 40%–60% in gynecological surgery, with analgesic duration 30% longer than traditional transversus abdominis plane block (TAPB).13–15 Furthermore, traditional retrospective studies often suffer from reliability issues due to baseline differences between groups. This study innovatively adopted propensity score matching (PSM) to rigorously balance potential confounders such as age, BMI, and surgical duration, ensuring scientific validity of the conclusions.
Through systematic analysis, this study found that ropivacaine quadratus lumborum block combined anesthesia demonstrates multidimensional advantages in uterine fibroid surgery, with mechanisms involving neural blockade, stress regulation, neuroprotection, and sleep cycle improvement. The following sections provide in-depth discussions based on specific results:
The study group showed significantly shorter anesthesia duration, attributed to reduced systemic anesthesia drug consumption due to regional blockade. Data indicated a 33.2% reduction in propofol dosage and a 28.6% reduction in remifentanil dosage in the study group, with decreased metabolic burden directly shortening the anesthesia maintenance phase.16,17 Postoperative flatus time and ambulation time, as core indicators of gastrointestinal function recovery, were significantly improved due to precise analgesia from combined anesthesia. Traditional general anesthesia, with high opioid usage, often induces intestinal paralysis and motor suppression. The study group achieved effective coverage of T12-L3 spinal nerves through QLB, not only blocking nociceptive signals at the surgical incision site but also promoting parasympathetic-dominated gastrointestinal motility recovery by suppressing sympathetic tone.18,19 Animal experiments confirm that regional blockade increases postoperative mesenteric blood flow by 25%-35%, accelerating inflammatory factor clearance and shortening gastrointestinal recovery cycles. However, postoperative awakening time was prolonged because QLB, through ropivacaine diffusion in the fascial space, not only blocks somatic nociception but also inhibits sympathetic excitability.20,21 Pharmacokinetic analysis shows that 0.25% ropivacaine in the quadratus lumborum region has a half-life of 4–6 hours, with sustained sympathetic inhibition potentially delaying central nervous system excitability recovery during the awakening phase.22,23 Additionally, shortened hospital stay reflects the concentrated clinical benefits of combined anesthesia, closely related to reduced complications and accelerated recovery from multimodal analgesia.24–26 Clinical data indicate a 58.3% reduction in additional analgesic use within 24 hours postoperatively and a 40% increase in early ambulation rates in the study group, effectively lowering risks of deep vein thrombosis and pulmonary infections.
The significant differences in pain control stem from the unique mechanism of QLB. Ultrasound-guided precise positioning enables effective ropivacaine diffusion into the fascial space surrounding the quadratus lumborum muscle, forming a continuous neural blockade band. Pharmacodynamic studies show that 20 mL of 0.25% ropivacaine maintains effective analgesic concentrations for 8–12 hours, blocking nerve impulse conduction by inhibiting sodium channel opening while reducing nociceptive signal transmission to the central nervous system. This peripheral-central dual analgesic mechanism effectively lowers central sensitization risk, with postoperative 12-hour pain scores in the study group 43.8% lower than the control group, suggesting that regional blockade interrupts the “pain-sensitization” vicious cycle.27 Stress response regulation represents a core advantage of combined anesthesia. As key stress indicators, postoperative 12-hour ACTH and Cor levels in the study group decreased by 29.8% and 28.9%, respectively. This improvement arises from regional blockade inhibiting the sympathetic-adrenal medullary system. QLB reduces catecholamine release triggered by surgical trauma by blocking T12-L3 sympathetic fibers, thereby lowering hypothalamic-pituitary-adrenal (HPA) axis activation intensity.28 Animal experiments confirm that regional blockade decreases postoperative plasma norepinephrine levels by 37.2%, with stable neuroendocrine environments providing a foundation for organ function protection.29
Furthermore, the protective mechanism of cognitive function involves neuroinflammatory regulation and cerebral blood flow improvement. The elevated MMSE scores in the study group may relate to reduced accumulation of inflammatory cytokines in the brain due to regional blockade. Surgical trauma-induced systemic inflammatory responses can lead to cytokines such as IL-6 and TNF-α crossing the blood-brain barrier, activating microglia and triggering neuroinflammation. Quadratus lumborum block inhibits sympathetic excitability, reducing cytokine transport to the central nervous system while improving cerebral perfusion. Sleep quality improvement reveals the interaction among pain, stress, and sleep. The reduced PSQI scores in the study group stem from combined anesthesia breaking the “pain-awakening” cycle through effective analgesia, lowered stress hormone levels reducing interference with sleep-wake cycles, and potential regulation of neurotransmitter systems like serotonin to improve sleep architecture.30,31
The clinical significance of this study’s findings spans multiple dimensions: for patients, combined anesthesia significantly enhances postoperative comfort and recovery quality; for healthcare systems, reduced hospital stays and complication rates effectively alleviate medical resource pressures; for anesthesia discipline development, this study provides high-level evidence for regional blockade applications in gynecological surgery. Notably, the prolonged awakening time in the study group suggests the need to optimize anesthetic drug combinations, with future exploration of short-acting sedatives to balance awakening quality and speed.
Limitations
This study has several limitations requiring improvement in future research. First, as a single-center retrospective cohort study, although propensity score matching (PSM) balanced baseline characteristics between groups, the retrospective design inherently carries selection and information biases—for example, reliance on complete medical records for some clinical data may affect result accuracy. Second, the sample size was relatively limited; while 74 cases per group after PSM achieved basic statistical power, larger multi-center randomized controlled trials (RCTs) would better validate conclusion universality. Third, this study did not investigate the effects of different ropivacaine concentrations on blockade efficacy, and future dose-gradient studies could optimize drug regimens. Fourth, long-term follow-up data were lacking—this study only observed outcomes until postoperative discharge, while long-term effects on cognitive recovery and sleep quality require 6–12 month follow-ups. Finally, some indicators like stress hormone measurements only included preoperative and postoperative 12-hour timepoints, failing to dynamically reflect hormonal trends; future studies could increase sampling frequency to more precisely characterize neuroendocrine responses.
Conclusion
To our knowledge, this is the first reported study in the gynecologic surgery literature that uses a multi-dimensional approach to evaluate the efficacy of combined GA and QLB compared to GA in patients undergoing laparoscopic myomectomy. By establishing a three element linkage model of “analgesia stress control rapid recovery”, this approach achieves a synergistic effect of pain control, stress regulation, cognitive protection, and sleep improvement in uterine fibroid surgery, providing a replicable quantitative framework for deepening the practice of the Enhanced Recovery Surgery (ERAS) concept. Combined anesthesia effectively reduces postoperative pain and negative emotions in patients with uterine fibroids who have undergone laparoscopic myomectomy, lowers stress levels, improves sleep quality, and promotes rapid recovery. Clinical data indicate that this approach significantly enhances patient satisfaction and reduces hospitalization time, demonstrating substantial clinical value and broad application prospects.
Declaration
The study received approval from Ethics Committee of Renmin Hospital, Hubei University of Medicine (ETHC-2025-0127) and adhered to the Helsinki Declaration and relevant Chinese medical data protection regulations. As a retrospective study using existing clinical records without additional patient risks, the Ethics Committee waived informed consent. Privacy protection measures included: anonymization of data prior to collection (removal of personally identifiable information such as names and ID numbers); tiered access permissions restricting full dataset access to authorized researchers; and presentation of aggregated clinical data in publications to prevent individual information disclosure.
Disclosure
The authors report no conflicts of interest in this work.
References
1. Giuliani E, As-Sanie S, Marsh EE. Epidemiology and management of uterine fibroids. Int J Gynaecol Obstet. 2020;149(1):3–10. doi:10.1002/ijgo.13102
2. De La Cruz MS, Buchanan EM. Uterine Fibroids: diagnosis and Treatment. Am Fam Physician. 2017;95(2):100–107.
3. Pavone D, Clemenza S, Sorbi F, Fambrini M, Petraglia F. Epidemiology and Risk Factors of Uterine Fibroids. Best Pract Res Clin Obstet Gynaecol. Best Practice & Research. Clinical Obstetrics & Gynaecology. 2018;46:3–11. doi:10.1016/j.bpobgyn.2017.09.004
4. Stewart EA, Cookson CL, Gandolfo RA, Schulze‐Rath R. Epidemiology of uterine fibroids: a systematic review. Bjog. 2017;124(10):1501–1512. doi:10.1111/1471-0528.14640
5. Szkodziak P, Szkodziak F, Trzeciak K, Czuczwar P. Minimally invasive procedures in the management of uterine fibroids. Prz Menopauzalny. 2017;16(4):122–125. doi:10.5114/pm.2017.72756
6. Stewart EA, Laughlin-Tommaso SK, Catherino WH, Lalitkumar S, Gupta D, Vollenhoven B. Uterine fibroids. Nat Rev Dis Primers. 2016;2(1):16043. doi:10.1038/nrdp.2016.43
7. Ahmad A, Kumar M, Bhoi NR. Diagnosis and management of uterine fibroids: current trends and future strategies. J Basic Clin Physiol Pharmacol. 2023;34(3):291–310. doi:10.1515/jbcpp-2022-0219
8. Marsh EE, Wegienka G, Williams DR. Uterine Fibroids. JAMA. 2024;331(17):1492–1493. doi:10.1001/jama.2024.0447
9. Micić J, Macura M, Andjić M, et al. Currently Available Treatment Modalities for Uterine Fibroids. Medicina. 2024;60(6):868.
10. Dolmans MM, Petraglia F, Catherino WH, Donnez J. Pathogenesis of uterine fibroids: current understanding and future directions. Fertil Steril. 2024;122(1):6–11. doi:10.1016/j.fertnstert.2024.02.048
11. D’Souza N, Himashweta G, Diwan S. Transmuscular quadratus lumborum block (QLB) in supine position for abdominal surgeries: pros and cons. Saudi J Anaesth. 2023;17(1):138–140. doi:10.4103/sja.sja_505_22
12. Dhanjal ST, Tonder S. Quadratus Lumborum Block. In: StatPearls. Treasure Island (FL): StatPearls Publishing LLC; 2025.
13. Little C, Naim N, Grogan T, Yu S, Chia PA. Proof of concept study of the posterior quadratus lumborum block for laparoscopic myomectomy: a randomized controlled trial. PLoS One. 2025;20(4):e0321890. doi:10.1371/journal.pone.0321890
14. Wang L, Qu Y, Dun Y. Preoperative posterior quadratus lumborum block: determining the minimum effective ropivacaine concentration in 90% of patients (MEC90) for postoperative analgesia after laparoscopic myomectomy. Anaesth Crit Care Pain Med. 2025;44(2):101480. doi:10.1016/j.accpm.2025.101480
15. Dai J, Lin S, Cui X, Xu Z, Zheng R, Wu D. The effects of ultrasound-guided QLB and TAPB combined with opioid-free anesthesia (OFA) on clinical efficacy of the patients undergoing abdominal surgery. Heliyon. 2023;9(10):e20878. doi:10.1016/j.heliyon.2023.e20878
16. Xu X, Zhang H, Li J, Zhou L, Zhu S, Bao F. Oxycodone vs the Combination of Fentanyl and Remifentanil for General Anesthesia in Laparoscopic Uterine Myomas Surgery: a Prospective, Randomized, Controlled Study. Drug Des Devel Ther. 2025;19:4979–4990. doi:10.2147/DDDT.S524102
17. Malouhi A, Aschenbach R, Erbe A. Effectiveness of Superior Hypogastric Plexus Block for Pain Control Compared to Epidural Anesthesia in Women Requiring Uterine Artery Embolization for the Treatment of Uterine Fibroids - A Retrospective Evaluation. Rofo. 2021;193(3):289–297. doi:10.1055/a-1231-5649
18. Priyadarshini K, Behera BK, Tripathy BB, Misra S. Ultrasound-guided transverse abdominis plane block, ilioinguinal/iliohypogastric nerve block, and quadratus lumborum block for elective open inguinal hernia repair in children: a randomized controlled trial. Reg Anesth Pain Med. 2022;47(4):217–221. doi:10.1136/rapm-2021-103201
19. Oostvogels L, Weibel S, Pogatzki-Zahn E, et al. Erector spinae plane block for postoperative pain. Cochrane Database Syst Rev. 2024;2(2):Cd013763.
20. Gao T, Wang Y, Zheng Y, Yu Y, Li Q, Zhang L. Quadratus lumborum block vs. transversus abdominis plane block for postoperative pain control in patients with nephrectomy: a systematic review and network meta-analysis. J Clin Anesth. 2024;95:111453. doi:10.1016/j.jclinane.2024.111453
21. Hussain N, Brull R, Speer J. Analgesic benefits of the quadratus lumborum block in total Hip arthroplasty: a systematic review and meta-analysis. Anaesthesia. 2022;77(10):1152–1162. doi:10.1111/anae.15823
22. Qin -P-P, Zou B-Y, Liu D, Li M-X, Liu X-N, Wei K. Lateral quadratus lumborum block vs acupuncture for postcesarean analgesia: a randomized clinical trial. American Journal of Obstetrics & Gynecology MFM. 2024;6(8):101433. doi:10.1016/j.ajogmf.2024.101433
23. Deng X, Du K. Identify key biomarkers predicting comorbidity of Alzheimer’s disease and metabolic syndrome through Machine Learning, single-cell analysis, and bioinformatics strategies. Innov Discov. 2025;2(4):18. doi:10.53964/id.2025018
24. Saibudeen A, Makris GC, Elzein A. Pain Management Protocols During Uterine Fibroid Embolisation: a Systematic Review of the Evidence. Cardiovasc Intervent Radiol. 2019;42(12):1663–1677. doi:10.1007/s00270-019-02327-1
25. Fan S, Li S, Hashmi MF. Application Effect of Sevoflurane Combined with Nerve Block Anesthesia in Surgical Anesthesia in Patients with Uterine Fibroids. Contrast Media Mol Imaging. 2022;2022(1):9983851. doi:10.1155/2022/9983851
26. Guo F, Jiao C, Xu K. Optimal Dose of Pituitrin in Laparoscopic Uterine Myomectomy: a Double-Blinded, Randomized Controlled Trial. J Minim Invasive Gynecol. 2021;28(12):2073–2079. doi:10.1016/j.jmig.2021.06.008
27. Grube M, Neis F, Brucker SY. Uterine Fibroids - Current Trends and Strategies. Surg Technol Int. 2019;34:257–263.
28. Koksal E, Aygun H, Genç C, Kaya C, Dost B. Comparison of the analgesic effects of two quadratus lumborum blocks (QLBs), QLB type II vs QLB type III, in caesarean delivery: a randomised study. Int J Clin Pract. 2021;75(10):e14513. doi:10.1111/ijcp.14513
29. Degani M, Di Franco C, Tayari H, et al. Postoperative Analgesic Effect of Bilateral Quadratus Lumborum Block (QLB) for Canine Laparoscopic Ovariectomy: comparison of Two Concentrations of Ropivacaine. Animals. 2023;13(23):3604.
30. Pangthipampai P, Dejarkom S, Poolsuppasit S, Luansritisakul C, Tangchittam S. Bilateral posterior Quadratus Lumborum block for pain relief after cesarean delivery: a randomized controlled trial. BMC Anesthesiol. 2021;21(1):90. doi:10.1186/s12871-021-01309-6
31. Uppal V, Retter S, Kehoe E, McKeen DM. Quadratus lumborum block for postoperative analgesia: a systematic review and meta-analysis. Can J Anaesth. 2020;67(11):1557–1575. doi:10.1007/s12630-020-01793-3
 © 2026 The Author(s). This work is published and licensed by Dove Medical Press Limited. The
full terms of this license are available at https://www.dovepress.com/terms
and incorporate the Creative Commons Attribution
- Non Commercial (unported, 4.0) License.
By accessing the work you hereby accept the Terms. Non-commercial uses of the work are permitted
without any further permission from Dove Medical Press Limited, provided the work is properly
attributed. For permission for commercial use of this work, please see paragraphs 4.2 and 5 of our Terms.
© 2026 The Author(s). This work is published and licensed by Dove Medical Press Limited. The
full terms of this license are available at https://www.dovepress.com/terms
and incorporate the Creative Commons Attribution
- Non Commercial (unported, 4.0) License.
By accessing the work you hereby accept the Terms. Non-commercial uses of the work are permitted
without any further permission from Dove Medical Press Limited, provided the work is properly
attributed. For permission for commercial use of this work, please see paragraphs 4.2 and 5 of our Terms.
Recommended articles
A Comparative Study of Airway Management Efficacy and Postoperative Pharyngolaryngeal Discomfort Using SaCo Visual and WORK Laryngeal Masks in Adult General Anesthesia Laparoscopic Surgery: A Retrospective Analysis
Xing F, Yang Y
Risk Management and Healthcare Policy 2025, 18:3143-3151
Published Date: 20 September 2025