Back to Journals » International Medical Case Reports Journal » Volume 9
Retropupilar positioning of foldable iris-claw intraocular lens for correction of aphakia with no capsular support
Authors Faria MY, Pinto Ferreira N, Gama I, Pinto JM, Canastro M, Monteiro Grillo M
Received 9 August 2016
Accepted for publication 4 October 2016
Published 31 October 2016 Volume 2016:9 Pages 337—340
DOI https://doi.org/10.2147/IMCRJ.S119347
Checked for plagiarism Yes
Review by Single anonymous peer review
Peer reviewer comments 3
Editor who approved publication: Dr Scott Fraser
Video abstract presented by Faria et al.
Views: 2887
Mun Yueh Faria,1-3 Nuno Pinto Ferreira,1-3 Ivo Gama,1-3 Joana Medeiros Pinto,1-4 Mario Canastro,1-3 Manuel Monteiro Grillo1-3
1Hospital Santa Maria, Ophthalmology Department, 2Vision Study Center, University of Lisbon, 3Faculty of Medicine, University of Lisbon, Lisbon, 4Hospital Divino Espirito Santo, Ponta Delgada, Portugal
Summary: Iris-claw intraocular lens (ICIOL) for aphakia needs a large 5.4 mm corneal incision for its implantation. The technique needs corneal suture, associated with some postoperative astigmatism. Foldable ICIOL is used in phakic patients undergoing refractive surgery and has the advantage of a sutureless small corneal incision. We report a case of a high myopic patient with dislocated intraocular lens (IOL) and no capsular support. Dislocated IOL with its capsular bag was released with three-port, 23-gauge vitrectomy; placed in the anterior chamber; sliced; and extruded through a 3.2-mm corneal incision, where a foldable ICIOL was introduced and placed retropupillary. This technique achieved a stable fixation of the IOL. Retropupillary implantation of a foldable ICIOL on aphakic patients has advantages over that of a polymethylmethacrylate (PMMA) ICIOL due to smaller corneal incision. The technique may be safe and easy to perform.
Purpose: The purpose of this report was to describe the technique of retropupillary implantation of a foldable iris-claw intraocular lens (ICIOL) in a patient with dislocated intraocular lens (IOL) in mid vitreous cavity.
Methods: Foldable ICIOL (Artiflex® Myopia Model 401) is used in phakic patients undergoing refractive surgery and has the advantage of a sutureless small corneal incision. We report a case of a high myopic patient with dislocated IOL and no capsular support. The calculation was a -5.0 D IOL for retropupilar position, and a foldable ICIOL was introduced through a 3.2-mm corneal incision and placed retropupillary.
Results: The technique was easy to achieve. IOL was properly positioned retropupillary and maintained stable. There was no ocular hypertension and no anterior chamber flare or iris atrophy.
Conclusion: Retropupillary implantation of a foldable ICIOL on aphakic patients has advantages over that of a PMMA ICIOL due to smaller corneal incision. The technique may be safe and easy to perform.
Keywords: aphakia, dislocated IOL, foldable iris-claw IOL, retro iris IOL
Introduction
High myopia, pseudoexfoliation, and longer span of life might be implicated in late in-the-bag intraocular lens (IOL) subluxations and dislocations. This late complication of phacoemulsification surgery is responsible for severe visual acuity (VA) impairment. The surgical management of aphakia without capsular support is often complex. To date, there is still no optimal surgical approach in these cases.1 The choices include anterior chamber (AC) IOLs, iris-sutured or scleral-sutured posterior chamber (PC) IOLs, and iris-claw intraocular lens (ICIOL).2
ICIOL implantation has been used more commonly over the last decade.3 Although originally designed for fixation on the anterior surface of the iris, some case series showed some advantages of fixating the ICIOL retropupillary, namely, by maintaining the AC depth and reducing the corneal endothelial cell loss.4,5
The ICIOL used for correction of aphakia is made of rigid polymethylmethacrylate (PMMA). Its implantation demands a 5.4-mm corneal or scleral incision. A foldable aphakia correction IOL, with a smaller corneal incision, would allow shorter surgical intervention and would reduce postoperative complications.
The Artiflex® Myopia Model 401 (Ophtec, Groningen, the Netherlands) is a three-piece IOL consisting of a flexible optic made from polysiloxane and rigid haptics made from compression-molded PMMA. The available dioptric powers range from -2 D to -14.5 D. It is currently used in myopic patients for refractive purposes. Its foldability allows implantation through a 3.2-mm clear corneal incision.
We report a case and describe the technique for retropupillary implantation of a foldable ICIOL in a high myopic patient with aphakia and no capsular support.
Methods
A 72-year-old high myopic male patient complained of recent decrease in VA of left eye (OS). This patient had cataract surgery on OS 12 years ago (in-the-bag implanted IOL of -7 D) and had retinal detachment surgery on right eye (OD).
OD best-corrected visual acuity (BCVA) was no light perception, and OS BCVA was 20/200 (Snellen chart measurement). Slit lamp examination revealed bulbar atrophy of the OD and a subluxated in-the-bag IOL in mid vitreous cavity in OS.
A three-port, 23-gauge pars plana vitrectomy was performed, and after careful vitrectomy to release the dislocated IOL of his capsular bag, the IOL was placed in the AC, sliced, and explanted through a 3.2-mm corneal incision. A foldable ICOL (Artiflex Myopia Model 401) was inserted in the AC through the same corneal incision in a concave convex position. For IOL fixation, a technique used for retropupilar implantation of Artisan® Aphakia Model 205 (Ophtec) ICIOL was adapted. Two paracentesis at 3 and 9 o’clock were made for IOL enclavation. Owing to flexible consistency of this IOL body, the fixation forceps (DO2-70 Artisan Implantation Forceps) were positioned near the rigid haptics for better grasping. The haptics were inserted in the PC and lifted slightly forward toward the posterior surface of the iris so that the claw configuration of the haptic could be recognized on the iris anterior surface. A micro-cannula was used through lateral paracentesis at 3 o’clock position to clamp iris tissue inside the claw (Figure 1). The same process was repeated on 9 o’clock paracentesis (Figure 2). No iridectomy was made (Figure 3).
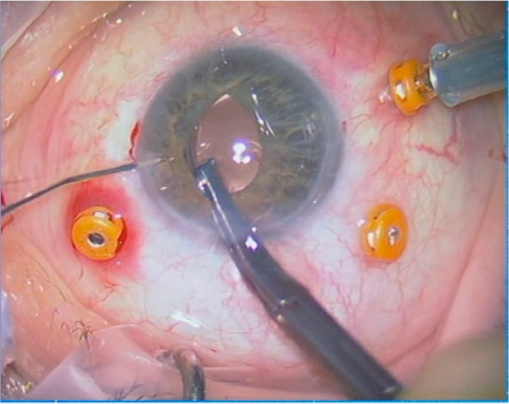 | Figure 1 Retropupilar enclavation at 3 o’clock position. |
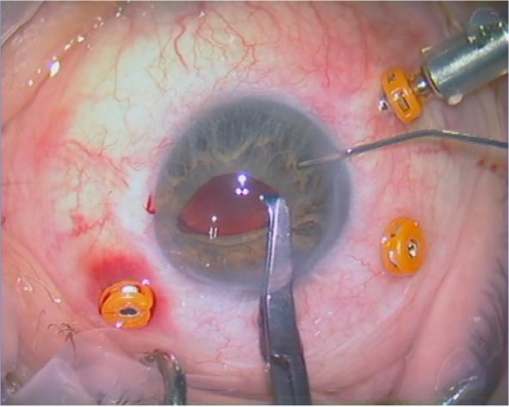 | Figure 2 Retropupilar enclavation at 9 o’clock position. |
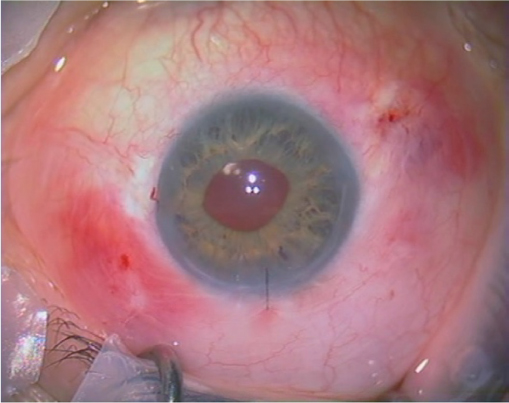 | Figure 3 Final result: retropupilar Artiflex® IOL. Abbreviation: IOL, intraocular lens. |
The IOL power was calculated using the SRK/T formula with the aim of achieving emmetropia. The manufacturer’s recommendation for A constant is 116.5 for retropupilar implantation of Artisan Aphakia AC250 ICIOL, and we used the same formula. The patient provided written informed consent to be included in this study and for the publication of the photographs.
Results
In the first postoperative day, the patient referred a subjective increase in VA. BCVA was 20/100 and intraocular pressure (IOP) was 12 mm using applanation tonometry. The patient has now 12 months of follow-up. There was no complication so far: the lens was in a stable position with no IOP variations, deep AC, no AC flare, and no iris atrophy.
Ocular fundus revealed myopic choroidal atrophy and maculopathy.
BCVA was no better than 20/100.
Discussion
ICIOL is nowadays an alternative technique for correction of aphakia in patients with no capsular support. Several case series have demonstrated its safety and good visual results.4,6–8 The technique is simple, less time consuming, and has a lower postoperative complication rate than other techniques.9–11 It has been associated with some peri- and postoperative complications, such as pupillary distortion, anterior uveitis, hyphema, iris depigmentation, spontaneous lens dislocation, ocular hypertension, cystoid macular edema, and retinal detachment.12 Nevertheless, most of the complications are rare, and some are clinically insignificant or easily controlled.
More recently, a new issue has been added to the debate regarding the best choice of IOL for correcting aphakia: where to position the ICIOL. Some studies recommend fixating the ICIOL on the anterior surface of the iris in cases of aphakia,4 while others recommend a retropupillary position.13,14 The retropupillary approach for ICIOL implantation does not need iridectomy and has recently gained popularity. Rijneveld et al7 reported in 1994 clinical results in 19 patients with ICIOL and penetrating keratoplasty and concluded that retropupilar ICIOL implantation combined with penetrating keratoplasty is a safe alternative to achieve pseudophakia in eyes with corneal edema and inadequate posterior capsular support. Mohr et al in 200215 reported retropupilar ICIOL in 47 eyes and concluded that “the retropupillary fixation of an ICIOL seems to have the advantages of a true PC implantation with a low intra and postoperative risk profile”. More recently, in 2015, Forlini et al3 published retrospective analysis of long-term follow-up of retropupillary implantation of the ICIOL in 320 patients and concluded that complications related to retropupillary implantation of the ICIOL were minimal compared with its benefits. Therefore, using retropupillary implantation of the ICIOL for secondary implantations is a valid alternative strategy for aphakia without capsular support. Hara et al9 compared retropupillary implantation of the ICIOL with transscleral suturing fixation of IOL and verified that the first technique had a lower rate of complications (namely, IOP rise), a faster postoperative VA recovery, and was less time consuming.
Artisan Aphakia AC250 (Ophtec) is the most commonly used ICIOL for aphakia correction. This ICIOL is rigid and has an overall diameter of 8.5 mm and a body of 5.4 mm. Hence, a corneal incision of 5.4 mm is needed for its introduction in the AC, which implies a larger corneal incision for ICIOL implantation and the possibility of greater surgically induced astigmatism. The available dioptric powers are +2.0 D–+30.0 D.
The ideal ICIOL should be flexible to avoid the wound enlargement. Artiflex Myopia Model 401 (Ophtec) is a three-piece ICIOL with a foldable optic, which allows implantation through a 3.2-mm clear corneal incision. Its characteristics and structure seem eligible for aphakia correction, except for its available dioptric power of -2.0 D to -14.0 D. There is a previously described case of aphakia treated with a foldable ICIOL implanted in the AC.16 To our knowledge, this is the first case of retropupillary implantation of a foldable ICIOL for aphakia correction with no capsular support.
The implantation technique is similar to the rigid ICIOL. Attention should be taken when grasping the ICIOL, since the forceps should not grasp the flexible body but near the harder PMMA base of the claw haptics, for secure grasping and to avoid damage to the optic component of the IOL. The major limitation for foldable ICIOL in cases of aphakia is the absence of commercially available positive sphere powers.
In our case, being a high myope with estimated IOL calculation of -5 D, we managed to introduce this foldable ICIOL and obtained a final spherical equivalent of -1.0 D.
Conclusion
Implantation of a retropupillary foldable ICIOL may be an effective and safe technique for the correction of myopic aphakic eye without capsular support, avoiding large corneal incisions and further postoperative complications.
To our knowledge, this is the first description of retropupillary implantation of a foldable ICIOL for correction of aphakia.
Disclosure
The authors report no conflicts of interest in this work.
References
Fernández-Buenaga R, Alio JL, Pérez-Ardoy AL, et al. Late in-the-bag intraocular lens dislocation requiring explantation: risk factors and outcomes. Eye (Lond). 2013;27(7):795–801. | ||
Dick HB, Augustin AJ. Lens implant selection with absence of capsular support. Curr Opin Ophthalmol. 2001;12(1):47–57. | ||
Forlini M, Soliman W, Bratu A, Rossini P, Cavallini GM, Forlini C. Long-term follow-up of retropupillary iris-claw intraocular lens implantation: a retrospective analysis. BMC Ophthalmol. 2015;15:143. | ||
Acar N, Kapran Z, Altan T, Kucuksumer Y, Unver YB, Polat E. Secondary iris claw intraocular lens implantation for the correction of aphakia after pars plana vitrectomy. Retina. 2010;30(1):131–139. | ||
Gicquel J-J, Guigou S, Bejjani RA, Briat B, Ellies P, Dighiero P. Ultrasound biomicroscopy study of the Verisyse aphakic intraocular lens combined with penetrating keratoplasty in pseudophakic bullous keratopathy. J Cataract Refract Surg. 2007;33(3):455–464. | ||
Güell JL, Velasco F, Malecaze F, Vázquez M, Gris O, Manero F. Secondary Artisan-Verysise aphakic lens implantation. J Cataract Refract Surg. 2005;31(12):2266–2271. | ||
Rijneveld WJ, Beekhuis WH, Hassman EF, Dellaert MM, Geerards AJ. Iris claw lens: anterior and posterior iris surface fixation in the absence of capsular support during penetrating keratoplasty. J Refract Corneal Surg. 1994;10(1):14–19. | ||
Gonnermann J, Torun N, Klamann MKJ, et al. Visual outcomes and complications following posterior iris-claw aphakic intraocular lens implantation combined with penetrating keratoplasty. Graefes Arch Clin Exp Ophthalmol. 2013;251(4):1151–1156. | ||
Hara S, Borkenstein AFM, Ehmer A, Auffarth GU. Retropupillary fixation of iris-claw intraocular lens versus transscleral suturing fixation for aphakic eyes without capsular support. J Refract Surg. 2011;27(10):729–735. | ||
Cellini M, Strobbe E, Toschi PG, Campos EC. Secondary IOL implantation without capsular support: a laser flare cell meter study. ISRN Ophthalmol. 2012;2011:653246. | ||
Teng H, Zhang H. Comparison of Artisan iris-claw intraocular lens implantation and posterior chamber intraocular lens sulcus fixation for aphakic eyes. Int J Ophthalmol. 2014;7(2):283–287. | ||
De Silva SR, Arun K, Anandan M, Glover N, Patel CK, Rosen P. Iris-claw intraocular lenses to correct aphakia in the absence of capsule support. J Cataract Refract Surg. 2011;37(9):1667–1672. | ||
Wolter-Roessler M, Küchle M. [Correction of aphakia with retroiridally fixated IOL]. Klin Monatsblätter für Augenheilkd. 2008;225(12):1041–1044. | ||
Rüfer F, Saeger M, Nölle B, Roider J. Implantation of retropupillar iris claw lenses with and without combined penetrating keratoplasty. Graefes Arch Clin Exp Ophthalmol. 2009;247(4):457–462. | ||
Mohr A, Hengerer F, Eckardt C. [Retropupillary fixation of the iris claw lens in aphakia. 1 year outcome of a new implantation techniques]. Ophthalmologe. 2002;99(7):580–583. | ||
Güell JL, Manero F. Artiflex (foldable iris claw IOL) secondary implantation for correction of aphakia after penetrating ocular injury. J Refract Surg. 2004;20(3):282–283. |
 © 2016 The Author(s). This work is published and licensed by Dove Medical Press Limited. The
full terms of this license are available at https://www.dovepress.com/terms
and incorporate the Creative Commons Attribution
- Non Commercial (unported, 3.0) License.
By accessing the work you hereby accept the Terms. Non-commercial uses of the work are permitted
without any further permission from Dove Medical Press Limited, provided the work is properly
attributed. For permission for commercial use of this work, please see paragraphs 4.2 and 5 of our Terms.
© 2016 The Author(s). This work is published and licensed by Dove Medical Press Limited. The
full terms of this license are available at https://www.dovepress.com/terms
and incorporate the Creative Commons Attribution
- Non Commercial (unported, 3.0) License.
By accessing the work you hereby accept the Terms. Non-commercial uses of the work are permitted
without any further permission from Dove Medical Press Limited, provided the work is properly
attributed. For permission for commercial use of this work, please see paragraphs 4.2 and 5 of our Terms.