Back to Journals » Clinical Ophthalmology » Volume 12
Retinal nerve fiber layer thickness after laser-assisted subepithelial keratomileusis and femtosecond LASIK: a prospective observational cohort study
Authors Katsanos A ![]() , Arranz-Marquez E
, Arranz-Marquez E ![]() , Cañones R, Lauzirika G
, Cañones R, Lauzirika G ![]() , Rodríguez-Perez I
, Rodríguez-Perez I ![]() , Teus MA
, Teus MA ![]()
Received 13 March 2018
Accepted for publication 23 April 2018
Published 4 July 2018 Volume 2018:12 Pages 1213—1218
DOI https://doi.org/10.2147/OPTH.S168033
Checked for plagiarism Yes
Review by Single anonymous peer review
Peer reviewer comments 3
Editor who approved publication: Dr Scott Fraser
Andreas Katsanos,1–3 Esther Arranz-Marquez,1,4 Rafael Cañones,2 Gorka Lauzirika,1 Isabel Rodríguez-Perez,1 Miguel A Teus1,2
1Clínica Novovisión, Madrid, Spain; 2Department of Ophthalmology, University of Alcala, Alcala de Henares, Spain; 3Department of Ophthalmology, University of Ioannina, Ioannina, Greece; 4Ophthalmology Clinic, Rey Juan Carlos Universitary Hospital, Móstoles, Madrid, Spain
Purpose: Based on the assumption that high levels of intraocular pressure (IOP) during femtosecond laser-assisted in situ keratomileusis (FS-LASIK) may compromise the retinal nerve fiber layer (RNFL), newer femtosecond platforms that operate without causing significant IOP elevation have been developed in recent years. However, this assumption has not been adequately tested. The aim of the current study was to evaluate possible changes in RFNL thickness in nonglaucomatous myopic patients undergoing FS-LASIK using the 60 KHz IntraLase® device that significantly elevates the IOP for an appreciable period of time vs an advanced surface ablation technique (laser-assisted subepithelial keratomileusis, LASEK) that does not induce any IOP elevation.
Methods: This was a prospective, observational, controlled cohort study. One randomly selected eye of 114 consecutive eligible patients was analyzed. Inclusion criteria were myopia up to -6.00 diopters and astigmatism up to -2.00 diopters. As clinically indicated, 50 patients underwent LASEK and 64 underwent FS-LASIK. The RNFL thickness was determined with a spectral-domain optical coherence tomography device preoperatively and 3 months postoperatively by the same masked observer.
Results: There was no significant difference in preoperative refractive error, age, or sex between the groups. Preoperatively, central corneal thickness was significantly lower in the LASEK group (529.1±36.1 vs 562.4±31.6 µm, P=0.001). For the LASEK group, there was no significant difference between preoperative and postoperative RNFL thickness in the studied sectors (superior-temporal, temporal, inferior-temporal, average). For the FS-LASIK group, compared to preoperative RNFL measures, statistically significant thicker postoperative values were found for the average RNFL (mean difference: 0.67 µm, 0.7% increase, P=0.008) and the inferior-temporal sector (mean difference: 0.92 µm, 0.6% increase, P=0.02).
Conclusion: LASIK with a femtosecond platform that induces high intraoperative IOP did not cause RNFL thinning. The observed differences between preoperative and postoperative values are below the axial resolution limit of optical coherence tomography devices.
Keywords: femtosecond laser, glaucoma, surface ablation, LASEK, photorefractive keratectomy, RNFL
Introduction
The advent of femtosecond lasers in the field of refractive surgery has improved the characteristics of corneal flaps created in laser-assisted in situ keratomileusis (LASIK).1–3 Femtosecond lasers use infrared light (1,053 nm) to accurately photodisrupt the corneal stroma, thus creating a predictable, homogeneously thick stromal cut.4 Similar to flap creation with a mechanical microkeratome, a suction ring is employed in femtosecond-assisted LASIK (FS-LASIK).
It is generally agreed that the intraocular pressure (IOP) elevation that is induced during LASIK with a mechanical microkeratome does not affect the retinal nerve fiber layer (RNFL) of healthy individuals in a measurable way.5–8 Nonetheless, experimental evidence shows that acute elevations in IOP may result in morphological changes of the optic nerve head that could compromise retinal nerve axon homeostasis.9 Even more, IOP elevations induced by flap creation during microkeratome-assisted LASIK have been reported to cause acute ischemic insults of the optic nerve in healthy eyes.10,11
In human eyes undergoing LASIK, the level of IOP reached during the stages of suction and flap creation cannot be accurately determined in vivo. In a previous experimental study of our group, an anterior chamber cannulation set-up was used for the comparison of IOP characteristics during LASIK with a mechanical microkeratome (M2; Moria, Antony, France) and a femtosecond laser (Abbott Medical Optics Inc, Santa Ana, CA, USA) in freshly enucleated porcine eyes.12 In that study, the phases of suction and lamellar cut using the mechanical microkeratome lasted for a mean 21.4 and 15.0 seconds, respectively, and the mean IOP reached 122.5 and 160.5 mmHg, respectively. Using the femtosecond laser, these phases lasted longer, but the IOP increased less (suction: 40.0 seconds, 89.2 mmHg; cutting: 52.8 seconds, 119.3 mmHg). It is currently unknown if lower IOP levels that are maintained for longer (such as those observed with some FS-LASIK systems) pose a smaller risk for a patient’s RNFL compared to higher IOP levels maintained for shorter periods (such as those observed with microkeratome-assisted LASIK). Based on the assumption that the IOP increase during LASIK procedures may be harmful for the optic nerve, newer femtosecond lasers use lower pressures during the suction and flap cutting phases.13–16 The purported safety advantage of lower pressures during FS-LASIK with newer lasers compared to the classic high-pressure femtosecond platforms remains to be determined.
On the other hand, laser-assisted subepithelial keratomileusis (LASEK) is an advanced corneal surface ablation technique in which the dissection of a corneal epithelial flap up to the level of Bowman’s membrane does not necessitate the application of a suction ring. Consequently, the IOP elevation observed with LASIK is avoided, although the change in the anterior corneal shape and thus the refractive correction is similar in both techniques.17 At least in principle then, LASEK should not induce any refractive surgery-related impact on a patient’s RNFL thickness.18
The aim of the current study was to evaluate possible changes in RFNL thickness of myopic patients undergoing LASIK using a femtosecond laser that significantly elevates IOP for an appreciable period of time vs an advanced surface ablation technique (LASEK) that does not induce any IOP elevation.
Methods
This was a prospective, observational, comparative, assessor-masked study that recruited eligible consecutive patients who underwent refractive surgery for the correction of myopia at the Novovisión Eye Institute, Madrid, Spain. The study adhered to the tenets of the Helsinki Declaration of 1975 as revised in 1983, and the investigation review board of the Novovisión Eye Institute approved the protocol. The nature and purpose of the study were explained in detail to all participants, and written informed consent was obtained. All participants met the following inclusion criteria: myopia lower than −6.00 diopters (D) and astigmatism lower than −2.00 D. Exclusion criteria were acquired corneal irregularities, previous corneal disease, signs or history of ocular trauma or inflammation, previous ocular surgery, signs or history of glaucoma or ocular hypertension, and neurodegenerative diseases that could affect the RNFL.
If both eyes of the same patient met the inclusion criteria, 1 eye was randomly chosen. Eyes were allocated to the FS-LASIK group or the LASEK group depending on the surgical technique deemed more appropriate for the patient. The included eyes were matched for refractive error.
All surgeries were performed by the same experienced surgeon (MAT) under topical anesthesia (lidocaine 2% eyedrops). For FS-LASIK procedures, the IntraLase® 60 kHz device (Abbott Medical Optics Inc) was used for flap cutting with intended flap thickness of 110 μm. For LASEK procedures, a 20% alcohol solution was instilled inside a 7 mm corneal semi-sharp marker and the epithelial flap was peeled back with a crescent blade leaving a hinge at the 12 o’clock position. The ablation was performed with the WaveLight® Allegretto excimer laser (Alcon, Fort Worth, TX, USA) in all cases. For patients who underwent FS-LASIK, the postoperative treatment regimen consisted of topical fluorometholone 1 mg/mL and ciprofloxacin 3 mg/mL, each instilled 4 times daily for 7 days. Patients who underwent LASEK were prescribed topical fluorometholone 1 mg/mL 4 times daily for 1 month and topical tobramycin 3 mg/mL 4 times daily for 1 week.
Preoperatively as well as postoperatively, all patients underwent a full ophthalmic examination that included the measurement of uncorrected and best-corrected distance visual acuity, central corneal thickness determination with ultrasound, slit-lamp biomicroscopy, and funduscopy. In addition, the same experienced operator measured the peripapillary RNFL thickness using a spectral-domain optical coherence tomography (OCT) device (Spectralis®, Heidelberg Engineering, Heidelberg, Germany, Software version 5.0) before and 3 months after the refractive surgery. The OCT operator was masked to the patient’s treatment group at all visits. A scan circle with a diameter of 12° was centered at the optic disc. Peripapillary RNFL measurements were obtained with the pRNFL protocol using automatic real-time scanning for speckle noise reduction. Additionally, the eye-tracking algorithm of the instrument (TruTrack Technology™, Heidelberg Noise Reduction™, Heidelberg Engineering) was employed to obtain high-quality images without motion artifacts. RNFL thickness values of the temporal-superior, temporal, and temporal-inferior sectors as well as average peripapillary thickness were considered for analysis. At the 3-month postoperative visit, the peripapillary RNFL thickness was obtained using the real-time gaze tracking algorithm of the device (AutoRescan™, Heidelberg Engineering) that ensures scanning at the same location for each eye (ie, at the exact location of the baseline scan obtained before the operation). According to the manufacturer, this OCT device captures infrared fundus and spectral-domain OCT images at 40,000 A-scans per second with an axial resolution of 4 microns.
Statistical analysis was performed using the Statview SE + Graphics platform (Abacus Concepts Inc., Berkeley, CA, USA) for Macintosh. Data are reported as mean ± SD. The Student’s t-test for paired data was used for the comparison between average RNFL thickness obtained before and 3 months after the refractive surgery. The Student’s t-test for unpaired data was used for between-group comparisons. Differences were considered statistically significant when the P-value was <0.05. Sample size was calculated before the study commenced and indicated that 50 eyes per group would be needed so that a difference of 5 microns could be detected in within-group comparisons (α=0.05, β=0.20).
Results
A total of 114 myopic eyes of 114 patients fulfilled the inclusion criteria. Fifty cases underwent LASEK and 64 cases underwent FS-LASIK. There were 30 women in the LASEK group and 32 women in the FS-LASIK group. The demographic characteristics of the participants are summarized in Table 1.
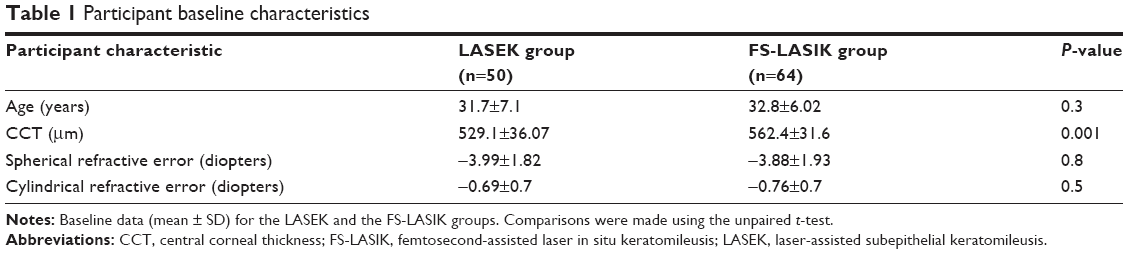 | Table 1 Participant baseline characteristics |
There were no significant differences between the groups in terms of preoperative refractive error, age, or sex. Eyes in the LASEK group had a significantly thinner preoperative central corneal thickness compared to those in the FS-LASIK group (529.1±36.1 vs 562.4±31.6 μm, respectively, P=0.001).
In the LASEK group, no statistically significant difference between preoperative and postoperative RNFL thickness values was detected for any of the examined sectors and the average peripapillary area (Table 2). In the FS-LASIK group, compared to preoperative values, postoperative values were statistically higher for the average RNFL thickness (P=0.008) and the RNFL thickness in the temporal-inferior sector (P=0.02). On the other hand, there was no statistically significant difference between preoperative and postoperative values for the temporal and temporal-superior sectors in the FS-LASIK group (Table 2).
 | Table 2 RNFL thickness results for the study groups |
Discussion
In our study, we found that neither LASEK nor LASIK with a high-pressure femtosecond system induce thinning of the RNFL, as evaluated with spectral-domain OCT, in otherwise healthy myopic eyes. Scant literature exists on the effect of femtosecond platforms that either do not cause marked IOP elevations by virtue of a curved corneal interface,19 or cause significant IOP elevations due to a flat corneal interface for a relatively short period of time.20,21 On the other hand, to the best of our knowledge, the potential effect of the high-pressure femtosecond platform that we used on the RNFL thickness has not been investigated so far. This particular device uses a flat patient interface and maintains relatively high pressures for a comparatively extended period of time.15,16,21
The available literature indicates that the IOP elevation induced in microkeratome-assisted LASIK does not cause any measurable thinning of the RNFL in healthy eyes.5–8,18 Despite this consensus, there are few case reports suggesting that the procedure may in fact damage the optic nerve.10,11
FS-LASIK procedures have become very popular over the last several years. Although large numbers of patients have undergone the procedure, it is difficult to ascertain that microkeratome-assisted LASIK shares the same safety profile in terms of optic nerve and RNFL impact with FS-LASIK, because the differences in the induced IOP and its temporal characteristics between the 2 procedures are significant.12,15,22,23 For example, in an in vivo experimental study using the M2 microkeratome and the VisuMax 200 kHz femtosecond laser (Carl Zeiss Meditec, Jena, Germany), Chaurasia et al22 found that the IOP was significantly lower and the fluctuation was much smaller during all phases of the procedure with the VisuMax laser. On the other hand, flap creation with this femtosecond laser was twice as long.22 Similar results were reported by other investigators using the femtosecond device of the current study.23
In our study, the RNFL thickness of patients who underwent LASEK was not affected by the procedure. These results are in accord with data from a small contralateral eye study with 20 participants who were randomized to microkeratome-assisted LASIK and LASEK.18 Using time-domain OCT, these authors did not find any statistically significant differences between preoperative and postoperative RNFL thickness values determined 1 month after any of the 2 procedures.18 A subsequent, larger study by the same group confirmed that LASEK does not significantly affect the RNFL thickness of nonglaucomatous myopic eyes.24
In our FS-LASIK group, postoperative values for the average thickness and the temporal-inferior sectors were statistically higher than the preoperative ones (P=0.008 and P=0.02, respectively). In the case of average thickness, this change represents a 0.7% increase, while in the case of the temporal-inferior thickness the change represents a 0.6% increase. No other statistically significant difference was detected between preoperative and postoperative values for the rest of the parameters in the group. The reason for the statistical difference between preoperative and postoperative values in average and temporal-inferior RNFL thickness observed in the FS-LASIK group is unclear. One potential explanation could be that LASIK-induced corneal changes may have affected image acquisition in the postoperative visit. In a study by Feng et al,25 the authors used time-domain OCT to investigate the effect of myopic microkeratome-assisted LASIK on retinal structures. Compared to preoperative values, total macular volume was significantly larger 3 months after surgery (P=0.003). No statistically significant differences between preoperative and postoperative disc area, rim area, cup/disk ratio, or average foveal thickness were detected. Of note, the change in total macular volume showed a significant correlation with the treatment-induced change in spherical equivalent, maximal and minimal corneal curvature, and corneal ablation depth.25 Although these authors did not offer a specific explanation for their findings, the observed correlation between corneal changes and apparent macular volume increase may point toward a LASIK-induced optical artifact, rather than true macular edema. In our study, the possibility that the increased postoperative RNFL thickness may represent axonal edema cannot be excluded. At least in principle, IOP elevations such as those observed during LASIK could impede ocular blood flow and axoplasmic transport, thus causing retinal edema in the postoperative period.26,27 However, we believe that this mechanism cannot explain our results. There are no accounts of clinically observable retinal edema occurring even in the immediate post-LASIK period in uncomplicated cases. Subclinical edema of the RNFL, on the other hand, has been suggested in 1 paper, but only within minutes following LASIK.28 In the paper by Zhang and Zhou,28 the authors used Fourier-domain OCT to assess macular, ganglion cell complex and RNFL thickness in 102 eyes treated with the Ziemer LDV femtosecond laser (Ziemer Group, Port, Switzerland) and 102 eyes treated with the M2 microkeratome. Although average foveal and parafoveal thickness values were increased compared to the preoperative values in both groups 30 minutes following the procedures, these differences disappeared already in the first postoperative day and consequently remained statistically similar to the preoperative values up to the 1 year follow-up visit.28
Unfortunately, any explanation for our results is inevitably hypothetical and cannot be adequately supported by the existing literature. It is important, however to note that the observed differences between our preoperative and postoperative RNFL values are particularly small: the mean change in average thickness was 0.67 μm (0.7% increase) and the mean change in the inferior-temporal sector was 0.92 μm (0.6% increase). These values are well below the axial resolution limits (~5 μm) of most currently available OCT devices.29
As the femtosecond laser we used in the current study was the first to become commercially available, the majority of the published evidence that has been produced about FS-LASIK over the last several years refers to this particular device, and corroborates its efficacy and safety profile in corneal refractive surgery.30 Based on the assumption that lower pressures during LASIK may offer a better safety profile in terms of RNFL thinning, several newer femtosecond platforms that do not increase the IOP significantly have been developed. To the best of our knowledge, evidence supporting this assumption is lacking. Consequently, at the current state of knowledge, it may be preferable to take into account factors such as predictability of flap size and thickness obtained, the degree of corneal inflammation induced, the speed of visual recovery, etc., when different femtosecond platforms are considered.
Conclusion
The current study shows that LASEK has no effect on RNFL thickness in otherwise healthy myopic eyes. It further shows that the FS-LASIK platform that we used does not cause any detectable RNFL thinning in otherwise healthy eyes despite the fact that fairly high intraoperative IOP levels are reached over a relatively long period.
Author contributions
AK helped in analysis and interpretation of data and drafting of the manuscript; EA-M was involved in analysis and interpretation of data and drafting of the manuscript; RC assisted with the data analysis and drafting of the manuscript; GL played a role in data acquisition and drafting of the manuscript; IR-P was involved in data acquisition and analysis and critical revision of the manuscript; MAT made substantial contributions to conception and design, analysis, and interpretation of data and also in critical revision of the manuscript for important intellectual content. All authors contributed toward data analysis, drafting and critically revising the paper and agree to be accountable for all aspects of the work.
Disclosure
The authors report no conflicts of interest in this work.
References
Alió JL, Pinero DP. Very high-frequency digital ultrasound measurement of the LASIK flap thickness profile using the IntraLase femtosecond laser and M2 and Carriazo-Pendular microkeratomes. J Refract Surg. 2008;24(1):12–23. | ||
Von Jagow B, Kohnen T. Corneal architecture of femtosecond laser and microkeratome flaps imaged by anterior optical coherence tomography. J Cataract Refract Surg. 2009;35(1):35–41. | ||
Gil-Cazorla R, Teus MA, de Benito-Llopis L, Mikropoulos DG. Femtosecond laser vs mechanical microkeratome for hyperopic laser in situ keratomileusis. Am J Ophthalmol. 2011;152(1):16.e2–21.e2. | ||
Kymionis GD, Kankariya VP, Plaka AD, Reinstein DZ. Femtosecond laser technology in corneal refractive surgery: a review. J Refract Surg. 2012;28(12):912–920. | ||
Holló G, Katsanos A, Kóthy P, Kerek A, Süveges I. Influence of LASIK on scanning laser polarimetric measurement of the retinal nerve fibre layer with fixed angle and customised corneal polarisation compensation. Br J Ophthalmol. 2003;87(10):1241–1246. | ||
Dementyev DD, Kourenkov VV, Rodin AS, Fadeykina TL, Diaz Martines TE. Retinal nerve fiber layer changes after LASIK evaluated with optical coherence tomography. J Refract Surg. 2005;21(Suppl 5):S623–S627. | ||
Whitson JT, McCulley JP, Cavanagh HD, Song J, Bowman RW, Hertzog L. Effect of laser in situ keratomileusis on optic nerve head topography and retinal nerve fiber layer thickness. J Cataract Refract Surg. 2003;29(12):2302–2305. | ||
Aristeidou AP, Labiris G, Paschalis EI, Foudoulakis NC, Koukoula SC, Kozobolis VP. Evaluation of the retinal nerve fiber layer measurements, after photorefractive keratectomy and laser in situ keratomileusis, using scanning laser polarimetry (GDX VCC). Graefes Arch Clin Exp Ophthalmol. 2010;248(5):731–736. | ||
Fatehee N, Yu PK, Morgan WH, Cringle SJ, Yu DY. The impact of acutely elevated intraocular pressure on the porcine optic nerve head. Invest Ophthalmol Vis Sci. 2011;52(9):6192–6198. | ||
Bushley DM, Parmley VC, Paglen P. Visual field defect associated with laser in situ keratomileusis. Am J Ophthalmol. 2000;129(5):668–671. | ||
Lee AG, Kohnen T, Ebner R, et al. Optic neuropathy associated with laser in situ keratomileusis. J Cataract Refract Surg. 2000;26(11):1581–1584. | ||
Hernandez-Verdejo JL, Teus MA, Roman JM, Bolivar G. Porcine model to compare real-time intraocular pressure during LASIK with a mechanical microkeratome and femtosecond laser. Invest Ophthalmol Vis Sci. 2007;48(1):68–72. | ||
Williams GP, Ang HP, George BL, et al. Comparison of intra-ocular pressure changes with liquid or flat applanation interfaces in a femtosecond laser platform. Sci Rep. 2015;5:14742. | ||
Strohmaier C, Runge C, Seyeddain O, et al. Profiles of intraocular pressure in human donor eyes during femtosecond laser procedures – a comparative study. Invest Ophthalmol Vis Sci. 2013;54(1):522–528. | ||
Vetter JM, Faust M, Gericke A, Pfeiffer N, Weingärtner WE, Sekundo W. Intraocular pressure measurements during flap preparation using 2 femtosecond lasers and 1 microkeratome in human donor eyes. J Cataract Refract Surg. 2012;38(11):2011–2018. | ||
Vetter JM, Holzer MP, Teping C, et al. Intraocular pressure during corneal flap preparation: comparison among four femtosecond lasers in porcine eyes. J Refract Surg. 2011;27(6):427–433. | ||
Teus MA, De Benito-Llopis L, Sanchez-Pina JM. LASEK versus LASIK for the correction of moderate myopia. Optom Vis Sci. 2007;84(7):605–610. | ||
Sharma N, Sony P, Gupta A, Vajpayee RB. Effect of laser in situ keratomileusis and laser-assisted subepithelial keratectomy on retinal nerve fiber layer thickness. J Cataract Refract Surg. 2006;32(3):446–450. | ||
Zhang J, Zhou Y, Zheng Y, Liu Q, Zhai C, Wang Y. Effect of suction on macular and retinal nerve fiber layer thickness during femtosecond lenticule extraction and femtosecond laser-assisted laser in situ keratomileusis. J Cataract Refract Surg. 2014;40(12):1994–2001. | ||
Hosny M, Zaki RM, Ahmed RA, Khalil N, Mostafa HM. Changes in retinal nerve fiber layer thickness following mechanical microkeratome-assisted versus femtosecond laser-assisted LASIK. Clin Ophthalmol. 2013;7:1919–1922. | ||
Yu CQ, Manche EE. Comparison of 2 femtosecond lasers for flap creation in myopic laser in situ keratomileusis: one-year results. J Cataract Refract Surg. 2015;41(4):740–748. | ||
Chaurasia SS, Luengo Gimeno F, Tan K, et al. In vivo real-time intraocular pressure variations during LASIK flap creation. Invest Ophthalmol Vis Sci. 2010;51(9):4641–4645. | ||
Vetter JM, Schirra A, Garcia-Bardon D, Lorenz K, Weingärtner WE, Sekundo W. Comparison of intraocular pressure during corneal flap preparation between a femtosecond laser and a mechanical microkeratome in porcine eyes. Cornea. 2011;30(10):1150–1154. | ||
Sharma N, Sony P, Prakash G, et al. Influence of epi-LASIK and alcohol-assisted LASEK on retinal nerve fiber layer thickness. J Refract Surg. 2007;23(5):431–432. | ||
Feng L, Burns SA, Shao L, Yang Y. Retinal measurements using time domain OCT imaging before and after myopic Lasik. Ophthalmic Physiol Opt. 2012;32(3):222–227. | ||
Dastiridou AI, Ginis HS, De Brouwere D, Tsilimbaris MK, Pallikaris IG. Ocular rigidity, ocular pulse amplitude, and pulsatile ocular blood flow: the effect of intraocular pressure. Invest Ophthalmol Vis Sci. 2009;50(12):5718–5722. | ||
Nuschke AC, Farrell SR, Levesque JM, Chauhan BC. Assessment of retinal ganglion cell damage in glaucomatous optic neuropathy: axon transport, injury and soma loss. Exp Eye Res. 2015;141:111–124. | ||
Zhang J, Zhou YH. Effect of suction on macular thickness and retinal nerve fiber layer thickness during LASIK used femtosecond laser and Moria M2 microkeratome. Int J Ophthalmol. 2015;8(4):777–783. | ||
Dong ZM, Wollstein G, Schuman JS. Clinical utility of optical coherence tomography in glaucoma. Invest Ophthalmol Vis Sci. 2016;57(9):OCT556–OCT567. | ||
Farjo AA, Sugar A, Schallhorn SC, et al. Femtosecond lasers for LASIK flap creation: a report by the American Academy of Ophthalmology. Ophthalmology. 2013;120(3):e5–e20. |
 © 2018 The Author(s). This work is published and licensed by Dove Medical Press Limited. The
full terms of this license are available at https://www.dovepress.com/terms
and incorporate the Creative Commons Attribution
- Non Commercial (unported, 3.0) License.
By accessing the work you hereby accept the Terms. Non-commercial uses of the work are permitted
without any further permission from Dove Medical Press Limited, provided the work is properly
attributed. For permission for commercial use of this work, please see paragraphs 4.2 and 5 of our Terms.
© 2018 The Author(s). This work is published and licensed by Dove Medical Press Limited. The
full terms of this license are available at https://www.dovepress.com/terms
and incorporate the Creative Commons Attribution
- Non Commercial (unported, 3.0) License.
By accessing the work you hereby accept the Terms. Non-commercial uses of the work are permitted
without any further permission from Dove Medical Press Limited, provided the work is properly
attributed. For permission for commercial use of this work, please see paragraphs 4.2 and 5 of our Terms.