Back to Journals » International Medical Case Reports Journal » Volume 19
Rethinking the Kinetics of Extended WBC Differential Count and Inflammatory Index Marker in Secondary Dengue Infection: Case Report at University Hospital
Authors Sugianli AK ![]() , Aulia N, Sari YANA, Hamdan AR
, Aulia N, Sari YANA, Hamdan AR ![]() , Fauziah N
, Fauziah N ![]() , Logito V
, Logito V
Received 20 January 2026
Accepted for publication 1 April 2026
Published 22 April 2026 Volume 2026:19 594518
DOI https://doi.org/10.2147/IMCRJ.S594518
Checked for plagiarism Yes
Review by Single anonymous peer review
Peer reviewer comments 2
Editor who approved publication: Dr Tanvi Dhere
Adhi Kristianto Sugianli,1– 4 Namira Aulia,5 Yona Alvira Nur Aluna Sari,5 Angkasa Ramatuan Hamdan,6 Nisa Fauziah,2,4,7 Verina Logito1,2
1Department of Clinical Pathology, Faculty of Medicine Universitas Padjadjaran, Sumedang, West Java, Indonesia; 2Department of Pathology, RS Unpad University Hospital, Sumedang, West Java, Indonesia; 3Department of Supporting Medicine, Dr. Hasan Sadikin General Hospital, Bandung, West Java, Indonesia; 4Research Center for Care and Control of Infectious Disease, Universitas Padjadjaran, Bandung, West Java, Indonesia; 5Medical Professional Program, Faculty of Medicine Universitas Padjadjaran, Sumedang, West Java, Indonesia; 6Department of Internal Medicine, Faculty of Medicine Universitas Padjadjaran/RS Unpad University Hospital, Sumedang, West Java, Indonesia; 7Department of Biomedical Sciences, Faculty of Medicine, Universitas Padjadjaran, Sumedang, West Java, Indonesia
Correspondence: Adhi Kristianto Sugianli, Department of Clinical Pathology, Faculty of Medicine Universitas Padjadjaran, Jl. Ir. Soekarno KM 21, Jatinangor, Sumedang, West Java, 45363, Indonesia, Tel +62-22-84288888, Email [email protected]
Abstract: Dengue infection is an emerging disease that continues to present a serious global public health challenge, contributing substantially to morbidity and mortality. Clinical and diagnostic management remain challenging due to the rapid progression of dengue among patients. This case report presents a comprehensive approach integrating clinical assessment with laboratory findings for the evaluation and management of secondary dengue infection. Key points highlighted include: (1) the negative kinetics of dengue antigen and antibody detection; and (2) the dynamic changes observed in extended white blood cell differential counts and inflammatory marker functions in relation to clinical outcomes. In summary, monitoring the extended white blood cell differential count and inflammatory index markers offers substantial value in detecting rapid escalation of disease severity. Furthermore, these parameters are notable for their repeatability, feasibility, and cost-effectiveness, thereby enhancing patient management efficiency.
Keywords: dengue infection, extended WBC differential count, inflammatory index marker, kinetics marker
Introduction
Dengue infection is a prevalent viral disease that occurs in tropical countries and has become a major public health concern in recent decades. According to the WHO’s global situation report on dengue in 2024, over 7.6 million cases of dengue were reported, including 3.4 million confirmed cases, more than 16,000 severe cases, and over 3000 deaths. In Indonesia, dengue has subsequently emerged as a significant public health issue over the past 50 years, characterized by consistently high incidence rates.1,2
Key environmental factors such as rainfall, temperature, and humidity are critical to the development of Aedes aegypti mosquitoes, which serve as the primary vectors for dengue transmission and underpin the endemic nature of dengue virus infection in Indonesia.2 Clinically, dengue may present as a spectrum ranging from mild-to-severe illness ie. dengue without warning signs, dengue with warning signs and severe dengue. The detection of dengue virus non-structural 1 (NS1) antigen, along with dengue antibodies, is widely utilized for diagnosing acute dengue infections. However, access to these serological tests can be limited, particularly in remote healthcare facilities, and issues such as low sensitivity—dependent on the duration of fever and regional population differences—may impact diagnostic accuracy.3,4 Moreover, inflammatory markers like C-Reactive Protein (CRP) and Procalcitonin may be useful in assessing the severity of the disease;5 but, these parameters may have limited availability in certain healthcare facilities, ie. primary health care settings. Recently, the use of hematology analyzers to perform complete blood count (CBC) tests has been implemented in primary health care over the past decade as an initial screening tool for diseases such as dengue. However, effective utilization of these instruments continues to be a challenge.6 In addition, simple and cost-effective inflammatory index markers, ie. Neutrophil-to-Lymphocyte Ratio (NLR), Platelet-to-Lymphocyte Ratio (PLR), Monocyte-to-Lymphocyte Ratio (MLR) have demonstrated their utility in defining both diagnosis and prognosis of the disease.5 Furthermore, advancements in flow cytometry-based hematology analyzers have enhanced the white blood cell (WBC) differential count by providing additional parameters that may be utilised for monitoring immune responses.7–9 However, there is limited information regarding the application of these parameters in viral infections, particularly dengue.
Due to its diverse clinical manifestations, rapid progression, and potential life-threatening, updated clinical-laboratory findings of dengue infection are crucial. This report presents an evaluation of dengue infection occurring in university hospital which serves as secondary healthcare settings, with comprehensive clinical-laboratory findings related to the disease’s pathophysiology, including inflammatory marker and extended WBC parameters from initial presentation until follow-up progression.
Case Synopsis and Laboratory Investigation
A 21-year-old male patient arrived at the university hospital emergency room (ER) with fever, rash, headache, and nausea. He had been experiencing continuous fever for three days, slightly improved with antipyretic drugs. He had recently stayed in a remote area identified as endemic for dengue infection. Vital sign revealed a high temperature of 39.1°C, heart rate of 102 beats per minute, respiratory rate of 102 per minute, and blood pressure of 137/81 mmHg. The physical examination was notable for epigastric tenderness and a rash on both upper extremities. Laboratory tests, including complete blood count and dengue antigen testing (shown in Table 1, days 3), indicated mild thrombocytopenia and leukopenia, with a negative result for dengue antigen. Despite this, the patient was diagnosed with dengue fever and discharged as an outpatient, as no significant warning signs were observed. The next day, he returned to the ER with a higher fever of 40.1°C and worsening symptoms, leading to hospitalization.
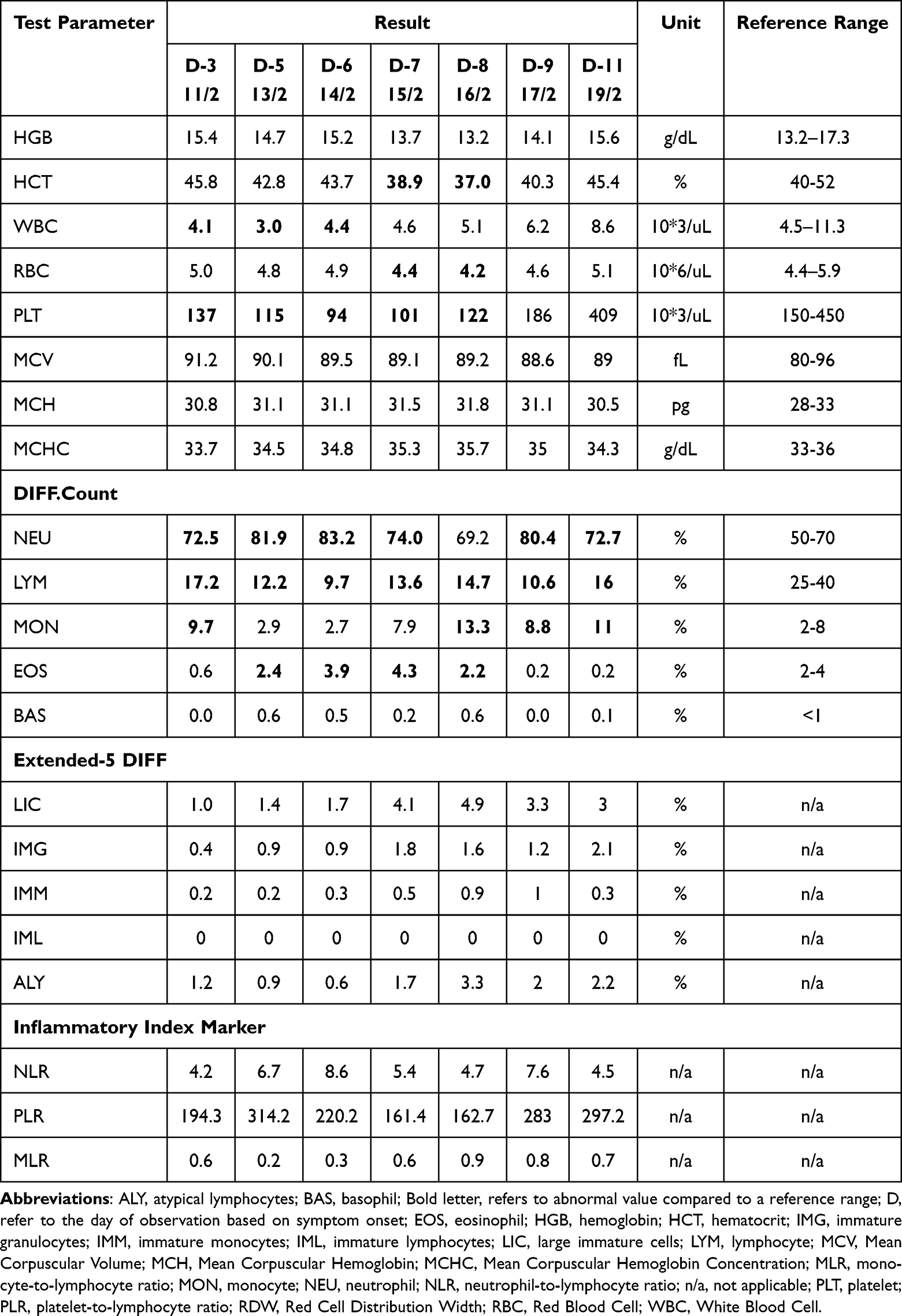 |
Table 1 Laboratory Finding of Complete Blood Count and Extended Differential Count |
In Table 1, a complete blood count with differential was required to identify the etiology based on the onset of clinical symptoms. Mild thrombocytopenia (100,000–150,000/uL) to moderate thrombocytopenia (50,000–100,000/uL) occurred between day 3 and day 8, ranging from 137,000/uL on day 3 to the lowest value of 94,000/uL on day 6. During this time, the patient experienced epistaxis and was treated with adrenaline nasal tampons. Leukopenia was also observed during the critical phase (days 3, 5, and 6). The differential count is a significant parameter in this case, reflecting the cellular immune response to pathogens. Between days 3 and 6, the percentage of lymphocytes decreased from 17.2% to 9.7%. Conversely, from days 7 to 11, the percentage of lymphocytes increased in response to clinical changes.
Nowadays, hematology analyzers have improved in their capability to determine the development process of blood cell, from immature cells to mature cells, particularly leukocyte differentiation. Utilizing flow cytometry methods, the expression of molecules such as trans-membrane proteins or RNA/DNA content enables differentiation of leukocytes into various lineages (eg, immature monocytes (IMM), immature lymphocytes (IML), immature granulocytes (IMG), atypical lymphocytes (ALY)), flagged with certain global parameters in the instrument (LIC, large immature cells).10 The presence of immature cells (IMG, IMM, and ALY) can be observed from day 5 to day 10/11 (Table 1). An increase in the percentage of IMG (from 0.9% to 2.1%) and IMM (from 0.2% to 1%) suggests an innate immune response to dengue viral infection. Additionally, an increase in atypical lymphocytes (ALY) may indicate the severity of the disease, particularly during the initial critical phase (day 3) (Figure 1).
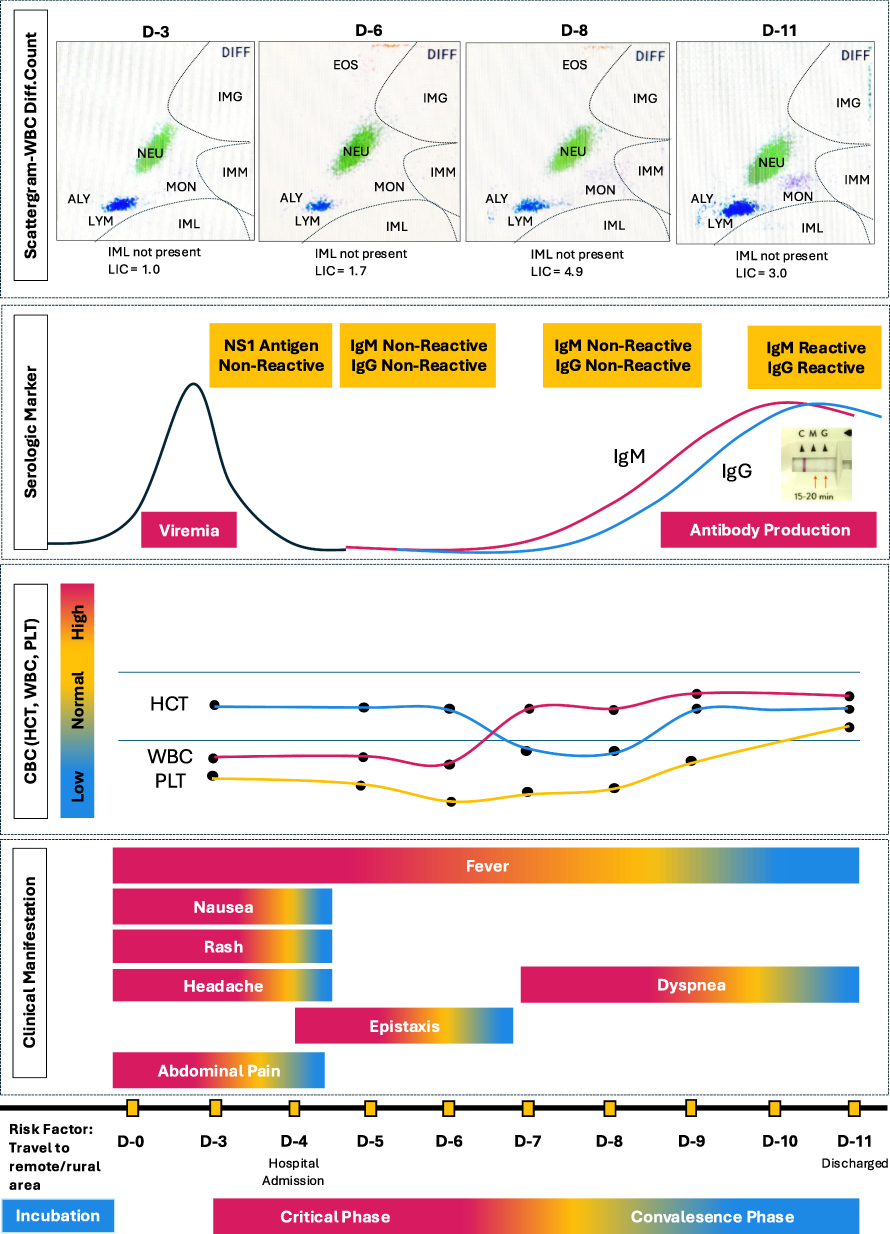 |
Figure 1 Color scale graph of clinical manifestation, complete blood count, serologic marker and scattergram-WBC Differential count. Abbreviations: ALY, atypical lymphocytes; D, refer to the day of observation based on symptom onset; EOS, eosinophil; HCT, hematocrit; IMG, immature granulocytes; IML, immature lymphocytes; IMM, immature monocytes; LIC, large immature cells; LYM, lymphocyte; MON, monocyte; NEU, neutrophil; PLT, platelet; WBC, White Blood Cell. |
On day 7, the patient’s fever and epistaxis improved; however, he experienced dyspnea with peripheral oxygen saturation levels between 91–93% (Figure 1). A chest X-ray revealed non-cardiogenic pulmonary edema, as the electrocardiogram showed a normal sinus rhythm. The dyspnea was managed with oxygenation using a non-rebreathing mask (NRM) at 10–12 liters per minute. The pulmonary edema resulted from fluid leakage from the capillaries due to dengue-related inflammation and plasma leakage. This condition was substantiated by alterations in inflammatory index markers observed between day 8 and day 11, indicating both local tissue and systemic inflammatory responses. Inflammatory markers serve different purposes:5 (a) NLR indicates physiological stress in critically ill patients, regardless of the disease etiology; (b) MLR helps predict viral disease outcomes; (c) PLR signals inflammation and its prognostic value. In this case, the trend of the inflammatory index marker increases in correlation with the progression of clinical manifestation. Additionally, the patient’s metabolic status remained stable, as indicated by electrolyte parameters and blood gas analysis (Table 2).
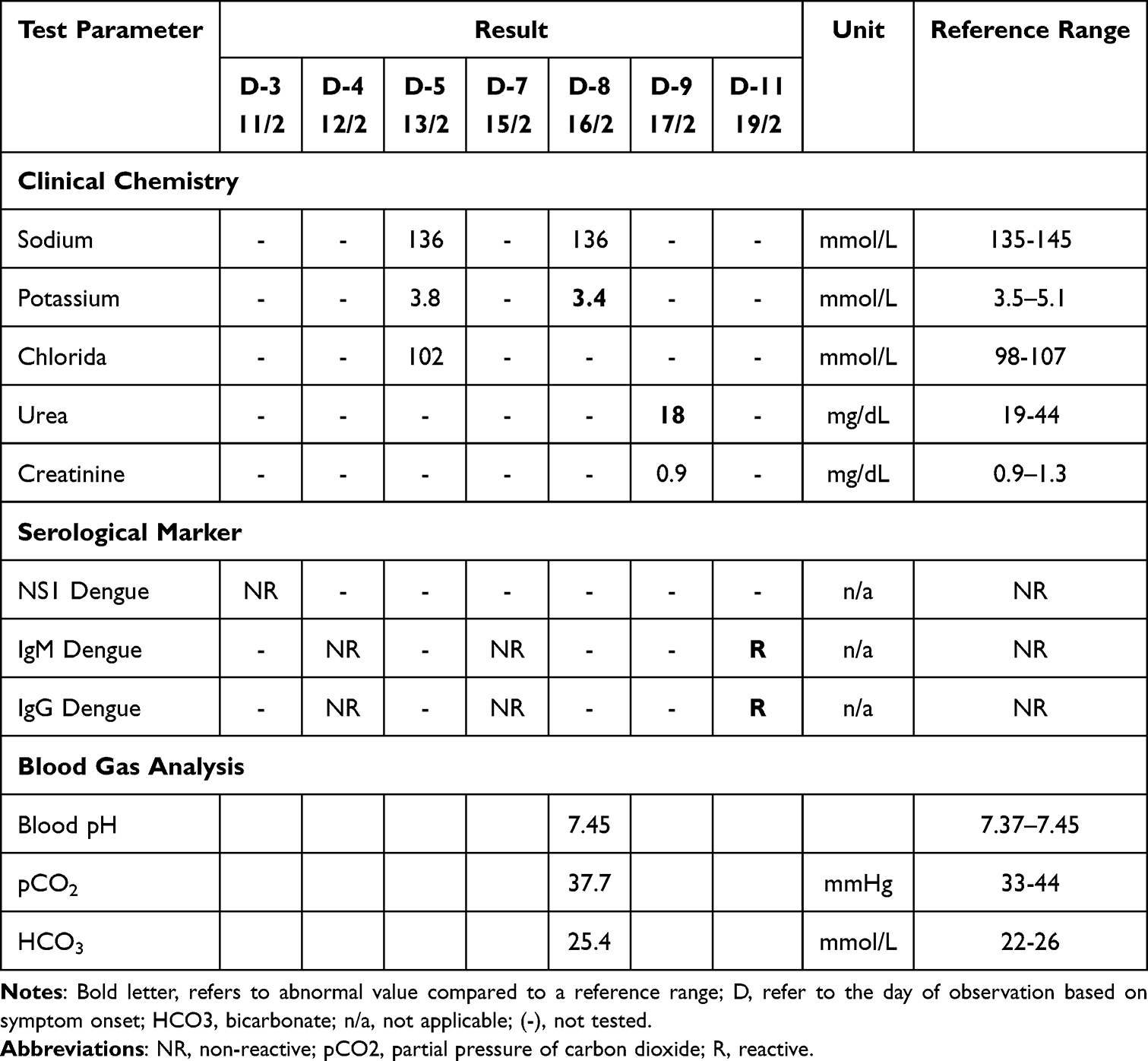 |
Table 2 Laboratory Finding of Clinical Chemistry and Serological Marker |
By day 11, all symptoms improved, and only abnormal lab result was a positive IgM and IgG dengue antibody test, with higher inflammatory markers (Table 1). Therefore, dengue antibody seroconversion occurred on days 11, aligning with clinical and hematological improvements. The patient was discharged from the hospital on day 11, and the follow-up visit a week later showed an unremarkable physical examination without any additional laboratory tests performed.
Discussion
Dengue infection remains a significant public health concern, primarily as a mosquito-borne acute febrile illness. Transmission occurs via dengue viruses (DENV), which comprise four major serotypes: DENV-1, DENV-2, DENV-3, and DENV-4. Humans become infected with DENV through the bites of female Aedes mosquitoes, notably Aedes albopictus and Aedes aegypti. Distinct DENV serotypes are associated with varying risks of severe complications.2,11–13 In this case, we highlighted several clinico-laboratory findings within the case, ie.1 the negative kinetics of antigen and antibody dengue in the first week of illness;2 the kinetics of extended-WBC differential count and inflammatory markers function related with dengue clinical outcome.
First, in this case, the NS1 and IgM/IgG dengue tests were negative during the first week of illness (days 3–7); however, by day 11, IgM/IgG reactivity was detected. NS1 is present in both primary and secondary dengue infections during the acute phase, beginning from the first day of illness. In primary infections, NS1 detection persists for at least nine days after symptom onset, whereas in secondary infections, levels tend to decrease by days 6–7. The highest detection rates for both types of infection occur on days 3–4. Lower NS1 concentrations may be observed in primary dengue compared to secondary infection due to a reduced viral load. Conversely, higher NS1 levels in secondary cases may result from antibody-dependent enhanced infection and could serve as a predictive marker for progression to more severe disease. The presence of NS1, as an endothelial toxin during dengue infection, is contributed to the development of vascular leakage.14–17 Subsequently, elevated levels of anti-NS1 IgG may result in the rapid clearance or reduction of circulating NS1, leading to the formation of immune complexes. These complexes can deposit on the surface of endothelial cells, thereby playing a role in the pathogenesis of vascular leak.18 This finding accounts for the negative NS1 result observed on day 3 of the acute phase. During this period, there is an overlap between the declining phase of NS1 and the increasing levels of IgG/IgM antibodies. The use of anti-NS1 IgG against NS1 leads to low IgG levels on days 4 and 7, resulting in non-reactive test outcomes.19 Another possible explanation for a negative NS1 result is that amino acid variations in the NS1 protein may decrease assay sensitivity by affecting monoclonal antibody binding in commercial kits, as previously reported.3 These amino acid differences in NS1 have also been linked to the DENV-2 serotype. Although specific serotype data were not available in this case study, recent epidemiological research from Yogyakarta shows that DENV-2 is currently the most prevalent serotype in Aedes aegypti (25%), followed by DENV-1 (22.3%) and DENV-3 (17%).11 Based on these findings, this case is consistent with a secondary dengue infection attributable to the DENV-2 serotype.
Second, in this study, we evaluate the kinetics of differential WBC count and their extended parameters as immune response of dengue infection. As reported in previous studies,4 clinical features and complete blood count (CBC) parameters may facilitate the dengue infection from other causes. As summary, the changes of CBC in first week of dengue case show lowest WBC count on day 5, lowest platelet count on day 6, meanwhile the differential WBC count shows highest monocytes and eosinophil on day 8 and 7, respectively. Higher atypical lymphocytes were shown on day 8. This finding was in agreement with observational study in Thailand which observed over 154 patient confirmed serologically dengue. The occurrence of leukopenia was caused by the destruction or inhibition of myeloid progenitor cells. Increase of monocytes in the first few days of the fever related with hypothesis that monocytes and macrophages are the part of the primary immune which carry out phagocytosis of microorganisms and present the resulting carried antigen to T helper cells. Monocytosis is also considered as the parameter to predict the severity of dengue infection. Meanwhile, eosinopenia in acute phase of dengue infection due to the response to the inflammatory process. The higher atypical lymphocytes are more likely found in dengue hemorrhagic fever and useful in the prediction of the severity of dengue infection. Lastly, the occurrence of cytopenia is the major finding of CBC can help to distinguish dengue infection from other diseases. Cytopenia is considered as protective mechanism to limit the injury to the marrow stem cells during subsequent process of the eradication of infected cells. Moreover, the dengue-infected endothelial cells are potentially bound to WBC, neutrophils, lymphocytes, platelets, and large lymphocytes in vitro but not with monocytes, basophils, and eosinophils. The increased binding of neutrophils and platelets to infected endothelial cells may explain the occurrence of neutropenia and thrombocytopenia in dengue case.4,20
Third, this study evaluates the utility of extended white blood cell (WBC) differential count and inflammatory index markers in dengue cases. Advancements in flow cytometry-based hematology analyzers have enabled more comprehensive assessment of leukocyte differentiation and counts related to hematopoiesis. While the use of extended WBC differential counts remains limited and variable, several studies have demonstrated their benefit in patient management. For instance, research involving sepsis populations has shown that extended WBC differential counts can aid in infection prediction, patient outcomes, and hospital sepsis management.9,21,22 Comparable approaches and findings have been reported in systemic viral infections, such as in moderate and severe COVID-19 cases,23,24 as well as in differentiating the etiologic agents responsible for acute febrile illness.20
Regarding inflammatory index markers, such as neutrophil-to-lymphocyte ratio (NLR), monocyte-to-lymphocyte ratio (MLR), and platelet-to-lymphocyte ratio (PLR), literature suggests each marker serves a specific function—for example, NLR reflects physiological stress in critically ill patients, whereas MLR and PLR are associated with prognostic or predictive value for clinical outcomes in infection.5 In this case study, the dynamic changes of these markers corresponded with the observed clinical presentations. It is notable, however, that some fluctuations in marker values may not correlate directly with disease progression, which can be attributed to the phenomenon of WBC heterogeneity. For example, neutrophils act as primary responders during pathogen invasion and play vital roles in inflammation and clearance. Distinct neutrophil subpopulations may exhibit varied activation levels and functions over time, contributing to overall heterogeneity. This complexity complicates the interpretation of neutrophil-based markers, as they do not necessarily represent the entirety of the neutrophil response during infection. Similar variabilities also occur in other WBC populations, influenced by inflammatory responses, immune exhaustion, and cell apoptosis.8
In summary, this case illustrates a thorough clinical diagnostic approach for secondary dengue infection, as outlined in Figure 2. Early differentiation of dengue is crucial, along with selecting the most suitable diagnostic methods. It is also important to monitor diagnostic findings while starting resuscitation procedures, administering appropriate treatments, and implementing specific interventions throughout hospitalization. Due to the rapid progression of dengue, it is important to use diagnostic tools that can be repeated and are practical, affordable, and cost-effective. Additional routine parameters—such as an extended white blood cell differential count and inflammatory index markers obtained from a complete blood count—play key roles in determining disease progression.
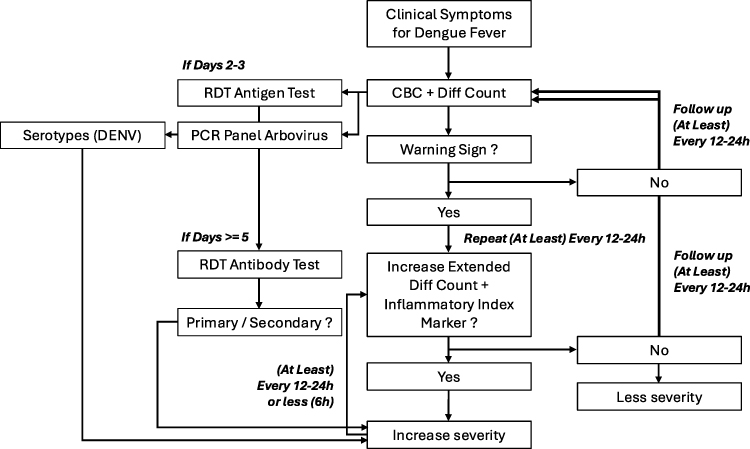 |
Figure 2 Case-flow-analysis of clinical manifestation, complete blood count, serologic marker and WBC differential count. Abbreviations: CBD, complete blood count; DENV, dengue virus; h, hours; PCR, polymerase chain reactions; RDT, rapid diagnostic test. |
Conclusion
The case illustrated a comprehensive approach that integrates clinical assessment with laboratory parameters for the management of secondary dengue infection. Monitoring the extended white blood cell differential count and inflammatory index markers, as part of a complete blood count, demonstrates potential value in identifying rapid progression of disease severity. These parameters are notable for being repeatable, feasible, and cost-effective, contributing to improved and efficient patient management. However, further evaluation and investigation are necessary, especially regarding reference ranges and the kinetics of these parameters at various stages of disease severity.
Ethics Statement
No ethical or institutional approval was required. The authors obtained written informed consent, ensured patient anonymity, and followed the Declaration of Helsinki and institutional guidelines for case reports.
Consent for Publication
Written informed consent for publication of their details was obtained from the patient in this case report.
Acknowledgments
We would like to express our gratitude to PT HORIBA Indonesia and PT Dexa Arfindo Pratama for technical and scientific support during writing the case report.
Funding
The study did not receive external funding.
Disclosure
The authors report no conflicts of interest in this work.
References
1. Indonesian Ministry of Health. Pedoman Nasional Pelayanan Kedokteran Tata Laksana Infeksi Dengue pada Dewasa. Indonesian Ministry of Health. 2020.
2. Masyeni S, Wardhana IMW, Permatananda PAN, Prebawa AG, Dewi SL, Nelwan EJ. Elevated levels of platelet-activating factor and syndecan-1 in severe dengue infections. J Clin Virol Plus. 2025;5(2):100213. doi:10.1016/j.jcvp.2025.100213
3. Felix AC, Romano CM, Centrone CDC, et al. Low sensitivity of NS1 protein tests evidenced during a dengue type 2 virus outbreak in Santos, Brazil, in 2010. Clin Vaccine Immunol. 2012;19(12):1972–9. doi:10.1128/CVI.00535-12
4. Chaloemwong J, Tantiworawit A, Rattanathammethee T, et al. Useful clinical features and hematological parameters for the diagnosis of dengue infection in patients with acute febrile illness: a retrospective study. BMC Hematol. 2018;18(1):20 doi:10.1186/s12878-018-0116-1.
5. Ng WW, Lam SM, Yan WW, Shum HP. NLR, MLR, PLR and RDW to predict outcome and differentiate between viral and bacterial pneumonia in the intensive care unit. Sci Rep. 2022;12(1):15974. doi:10.1038/s41598-022-20385-3
6. Anh DD, Sani LM, Riyanti R, et al. Diagnostic challenges of arboviral infections and dengue virus serotype distribution in febrile patients in East Java, Indonesia. IJID Reg. 2025;14:100512. doi:10.1016/j.ijregi.2024.100512
7. Dharap P, Raimbault S. Performance evaluation of machine learning-based infectious screening flags on the HORIBA Medical Yumizen H550 Haematology Analyzer for vivax malaria and dengue fever. Malar J. 2020;19(1):429. doi:10.1186/s12936-020-03502-3
8. M CDA, Brumpt C, Sala T, Oueidat N, Larsen M, Hausfater P. Cell population data for early detection of sepsis in patients with suspected infection in the emergency department. Clin Chem Lab Med CCLM. 2025;63(8):1654–1662. doi:10.1515/cclm-2025-0180
9. Herawati S, Somia IKA, Kosasih S, Wande IN, Felim J, Payana IMD. Integrating routine hematological and extended inflammatory parameters as a novel approach for timely diagnosis and prognosis in sepsis management. Diagnostics. 2024;14(9):956. doi:10.3390/diagnostics14090956
10. Nerin P. HORIBA medical in Europe: evolution of technologies for white blood cell differential at HORIBA medical. Readout Engl Ed. 2012;39:12–33.
11. Rahayu A, Saraswati U, Supriyati E, et al. Prevalence and distribution of dengue virus in Aedes Aegypti in Yogyakarta city before deployment of Wolbachia infected Aedes aegypti. Int J Environ Res Public Health. 2019;16(10):1742. doi:10.3390/ijerph16101742
12. Mamenun, Koesmaryono Y, Sopaheluwakan A, Hidayati R, Dasanto BD, Aryati R. Spatiotemporal characterization of dengue incidence and its correlation to climate parameters in Indonesia. Insects. 2024;15(5):366 doi:10.3390/insects15050366.
13. Wang WH, Urbina AN, Chang MR, et al. Dengue hemorrhagic fever – a systemic literature review of current perspectives on pathogenesis, prevention and control. J Microbiol Immunol Infect. 2020;53(6):963–978. doi:10.1016/j.jmii.2020.03.007
14. Glasner DR, Ratnasiri K, Puerta-Guardo H, Espinosa DA, Beatty PR, Harris E. Dengue virus NS1 cytokine-independent vascular leak is dependent on endothelial glycocalyx components. PLOS Pathog. 2017;13(11):e1006673. doi:10.1371/journal.ppat.1006673
15. Puerta-Guardo H, Glasner DR, Harris E. Dengue virus NS1 disrupts the endothelial glycocalyx, leading to hyperpermeability. PLOS Pathog. 2016;12(7):e1005738. doi:10.1371/journal.ppat.1005738
16. Beatty PR, Puerta-Guardo H, Killingbeck SS, Glasner DR, Hopkins K, Harris E. Dengue virus NS1 triggers endothelial permeability and vascular leak that is prevented by NS1 vaccination. Sci Transl Med. 2015;7(304). doi:10.1126/scitranslmed.aaa3787
17. Glasner DR, Puerta-Guardo H, Beatty PR, Harris E. The good, the bad, and the shocking: the multiple roles of dengue virus nonstructural protein 1 in protection and pathogenesis. Annu Rev Virol. 2018;5(1):227–253. doi:10.1146/annurev-virology-101416-041848
18. Muller DA, Choo JJY, McElnea C, Duyen HTL, Wills B, Young PR. Kinetics of NS1 and anti-NS1 IgG following dengue infection reveals likely early formation of immune complexes in secondary infected patients. Sci Rep. 2025;15(1):6684. doi:10.1038/s41598-025-91099-5
19. Ganesan M, Sudha R, Amudhan M, Thangam G. Lesson learned: retrospective analysis of ‘missed out’ dengue NS1 positives among IgM negative population. Asian Pac J Trop Med. 2020;13(5):221. doi:10.4103/1995-7645.283518
20. Prodjosoewojo S, Riswari SF, Djauhari H, et al. A novel diagnostic algorithm equipped on an automated hematology analyzer to differentiate between common causes of febrile illness in Southeast Asia. PLoS Negl Trop Dis. 2019;13(3):e0007183. doi:10.1371/journal.pntd.0007183
21. van der Geest PJ, Mohseni M, Linssen J, Duran S, de Jonge R, Groeneveld ABJ. The intensive care infection score – a novel marker for the prediction of infection and its severity. Crit Care. 2016;20(1):180. doi:10.1186/s13054-016-1366-6
22. Weimann K, Zimmermann M, Spies CD, et al. Intensive Care Infection Score – a new approach to distinguish between infectious and noninfectious processes in intensive care and medicosurgical patients. J Int Med Res. 2015;43(3):435–451. doi:10.1177/0300060514557711
23. Vrbacky F, Fatorova I, Blazek M, Smahel P, Zak P. Intensive Care Infection Score (ICIS) is elevated in patients with moderate and severe COVID-19 in the early stages of disease. J Infect Public Health. 2022;15(5):533–538. doi:10.1016/j.jiph.2022.03.018
24. Rutkowska E, Kwiecień I, Kulik K, et al. Usefulness of the new hematological parameter: reactive lymphocytes RE-LYMP with flow cytometry markers of inflammation in COVID-19. Cells. 2021;10(1):82. doi:10.3390/cells10010082
 © 2026 The Author(s). This work is published and licensed by Dove Medical Press Limited. The
full terms of this license are available at https://www.dovepress.com/terms
and incorporate the Creative Commons Attribution
- Non Commercial (unported, 4.0) License.
By accessing the work you hereby accept the Terms. Non-commercial uses of the work are permitted
without any further permission from Dove Medical Press Limited, provided the work is properly
attributed. For permission for commercial use of this work, please see paragraphs 4.2 and 5 of our Terms.
© 2026 The Author(s). This work is published and licensed by Dove Medical Press Limited. The
full terms of this license are available at https://www.dovepress.com/terms
and incorporate the Creative Commons Attribution
- Non Commercial (unported, 4.0) License.
By accessing the work you hereby accept the Terms. Non-commercial uses of the work are permitted
without any further permission from Dove Medical Press Limited, provided the work is properly
attributed. For permission for commercial use of this work, please see paragraphs 4.2 and 5 of our Terms.