Back to Journals » International Medical Case Reports Journal » Volume 17
Resuscitation from Respiratory Arrest Due to Life-Threatening Ventricular Arrhythmias in a Patient with Amitriptyline Intoxication: An Old Problem in a New Era
Authors Nguyen TT, Le LD, Vu TT ![]() , Nguyen AT, Doan DB, Pham DT, Pham TT, Vu CN, Nguyen Vo MH
, Nguyen AT, Doan DB, Pham DT, Pham TT, Vu CN, Nguyen Vo MH ![]()
Received 27 June 2024
Accepted for publication 24 October 2024
Published 11 November 2024 Volume 2024:17 Pages 949—957
DOI https://doi.org/10.2147/IMCRJ.S478761
Checked for plagiarism Yes
Review by Single anonymous peer review
Peer reviewer comments 2
Editor who approved publication: Dr Vinay Kumar
Tan Thanh Nguyen,1 Lac Duy Le,1 Thanh Tri Vu,2 Anh Thai Nguyen,1 Duc Binh Doan,1 Duyen Thi Pham,1 Tung Thanh Pham,1 Chuc Ngoc Vu,3 Minh Hoang Nguyen Vo4
1Cardiac Intensive Department, Thu Duc City Hospital, Ho Chi Minh City, Vietnam; 2Board of Directors, Thu Duc City Hospital, Ho Chi Minh City, Vietnam; 3Emergency Department, Thu Duc City Hospital, Ho Chi Minh City, Vietnam; 4Office of Science Management and International Affairs, Thu Duc City Hospital, Ho Chi Minh City, Vietnam
Correspondence: Minh Hoang Nguyen Vo, Office of Science Management and International Affairs, Thu Duc City Hospital, No. 29 Phu Chau Street, Tam Phu ward, Thu Duc, Ho Chi Minh City, 700000, Vietnam, Tel +84 389135014, Email [email protected]
Introduction: Tricyclic antidepressants (TCAs) were once commonly used to treat major depressive disorder (MDD), but are now considered second-line options after SSRIs and SNRIs. Additionally, TCAs are used to treat other conditions such as chronic pain and enuresis in children. Due to their numerous side effects and potential for drug interactions, cases of poisoning and death from TCA overdose, particularly amitriptyline, are on the rise. Therefore, this article revisits the overview and describes the clinical progression regarding blood gases, ECG, and electrolytes of the patient, as well as the use of 4.2% sodium bicarbonate and 2% lidocaine to treat cases of amitriptyline overdose poisoning.
Case Presentation: A 49-year-old female patient was admitted to the hospital due to cardiac and respiratory arrest. The patient had a past medical history of untreated cervical cancer and sleep disorders. Prior to admission, the patient had taken about 20 tablets of amitriptyline 25mg and was in a drowsy state with gasping breaths. During transportation to the hospital, the patient experienced cardiac arrest once and was successfully resuscitated, with a total arrest and resuscitation time of approximately 10 minutes.
Results: The use of 4.2% Sodium Bicarbonate and 2% Lidocaine, the patient was not used plasma exchange in this case, proved effective in this case. Continuous monitoring of blood gas levels, ECG, and electrolytes was maintained. The patient was able to walk independently and was discharged after 12 days of treatment.
Conclusion: The key factor was the healthcare staff’s quick recognition and timely management of TCA poisoning, in this case, amitriptyline.
Keywords: tricyclic antidepressants, amitriptyline, cardiac arrhythmia
Introduction
Tricyclic antidepressants (TCAs) were first introduced for the treatment of depression in the 1950s.1 Two years later, the first case involving TCAs side effects was reported.2 Among these medications, amitriptyline is still widely used, with 1,353,110 users in the United States in 20213 and 4654 cases of poisoning, including 5 deaths attributed to amitriptyline (the highest proportion among TCAs).4
The toxic dose of amitriptyline is over 5mg/kg. At toxic doses, this drug can inhibit central alpha-adrenergic, histamine, muscarinic, and serotonin receptors. Alpha-adrenergic receptor blockade causes hypotension. Muscarinic receptor blockade causes anticholinergic poisoning symptoms, while histamine receptor blockade causes mental status changes. TCAs can also be cardiotoxic, as evidenced by ECG QRS widening and QT prolongation, and bradycardia. TCAs have quinidine-like effects on the heart, causing decreased contractility and hypotension.5–7 According to statistics, up to 70% of amitriptyline poisoning deaths occur before reaching healthcare facilities, and only 2–3% of deaths occur after reaching medical facilities.8
Based on the above evidence, the role of management and prognosis of patients with amitriptyline poisoning is very important. On October 4, 2023, Thu Duc City Hospital admitted and successfully treated a case of amitriptyline poisoning.
Case Report
A 49-year-old female, was admitted to the hospital due to cardiopulmonary arrest. The patient has a medical history that includes untreated cervical cancer and sleep disorders. Three hours before admission, the patient’s family members noticed that the patient was lethargic, yawning, and found that the patient had taken about 20 tablets of amitriptyline 25mg, prompting an emergency call. During transport to Thu Duc City Hospital, the patient experienced one cardiac arrest and was successfully resuscitated, with the arrest and resuscitation lasting about 10 minutes. Upon admission to the Emergency Department at Thu Duc City Hospital, the patient was unconscious/on mechanical ventilation, with a blood pressure of 105/70 mmHg on a background of Noradrenaline at a dose of 0.5 µg/kg/min and Adrenaline at a dose of 0.3 µg/kg/min. The extremities were warm, the pulse was clear, and the heart rate was regular and fast at 115 beats per minute. After admission to the Emergency Department, the patient experienced a second cardiac arrest and was resuscitated with basic and advanced cardiopulmonary resuscitation, achieving return of spontaneous circulation after 15 minutes.
The pH level is 6.902 and bicarbonate (HCO3) is 18.4, which is very low compared to normal levels, indicating severe acidosis. Blood oxygen (pO2) is 52 and lactate is 10.39 mmol/L, indicating the patient is experiencing hypoxia. The results in Table 1 show that the patient is suffering from severe acidosis, respiratory failure, and tissue hypoxia. (Table 1)
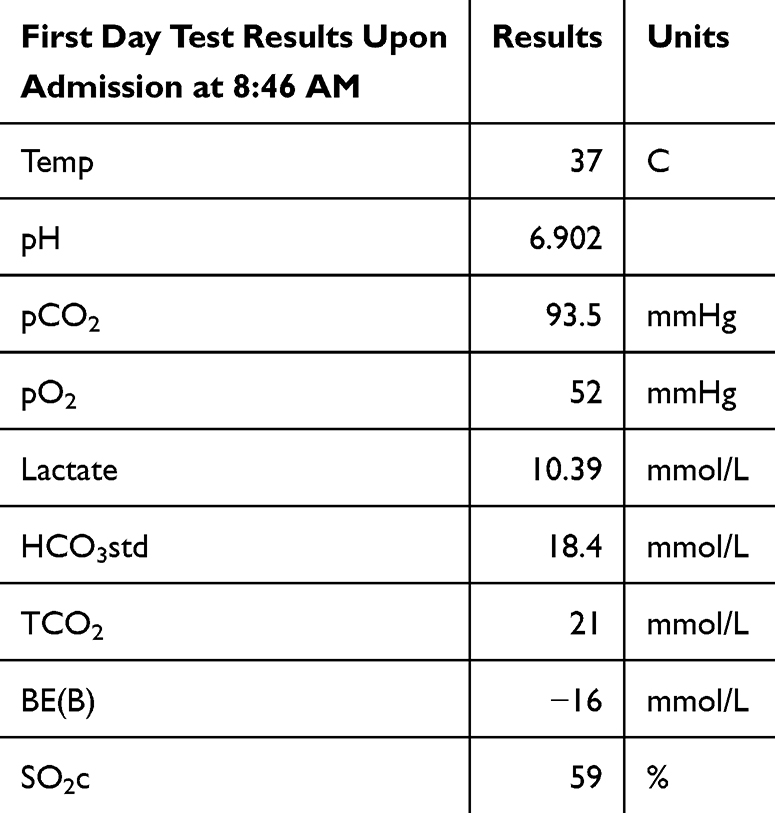 |
Table 1 Paraclinical Results Upon Admission |
The electrocardiogram (ECG) upon admission (Figure 1) shows the patient with a slow heart rate of 46 cycles per minute and a widened QRS complex of 240 ms. Several short episodes of ventricular tachycardia were recorded on the monitoring device. (Figure 1)
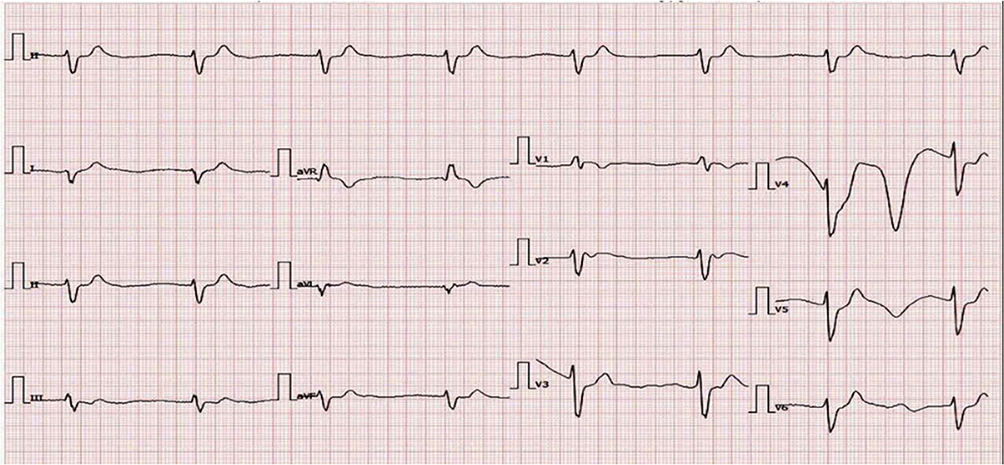 |
Figure 1 Photograph of ECG on admission. |
The patient was diagnosed with: Resuscitated cardiac arrest - Ventricular arrhythmias - QT prolongation - Seizures / Tricyclic antidepressant poisoning - Respiratory acidosis - Untreated cervical cancer - Sleep disorders.
The patient was treated with mechanical ventilation, noradrenaline 0.5µg/kg/minute, sedation, and 750mL of 4.2% sodium bicarbonate in the emergency room.
On the first day in the Cardiovascular Intensive Care Unit, we continued to maintain vasopressors, sedatives, and muscle relaxants, and administered isotonic sodium chloride solution and 4.2% sodium bicarbonate, adjusting the patient’s blood sodium and potassium levels. During the treatment monitoring process, the monitor showed ventricular tachycardia (Figure 2) with a frequency of about 130 beats per minute, while the arterial blood gas results recorded a pH of 7.61, pO2 of 94, pCO2 of 40.4, and HCO3 of 40.6. Since the pH had reached the treatment threshold, the patient was administered an additional 1.5g of 15% magnesium sulfate intravenously over 15 minutes. The ECG results showed a narrowing QRS complex, but the monitor still recorded temporary episodes of ventricular tachycardia and frequent ventricular ectopic beats. The doctors decided to administer additional intravenous 2% lidocaine at a dose of 1.2mg/kg/h (Figure 2)(Table 2).
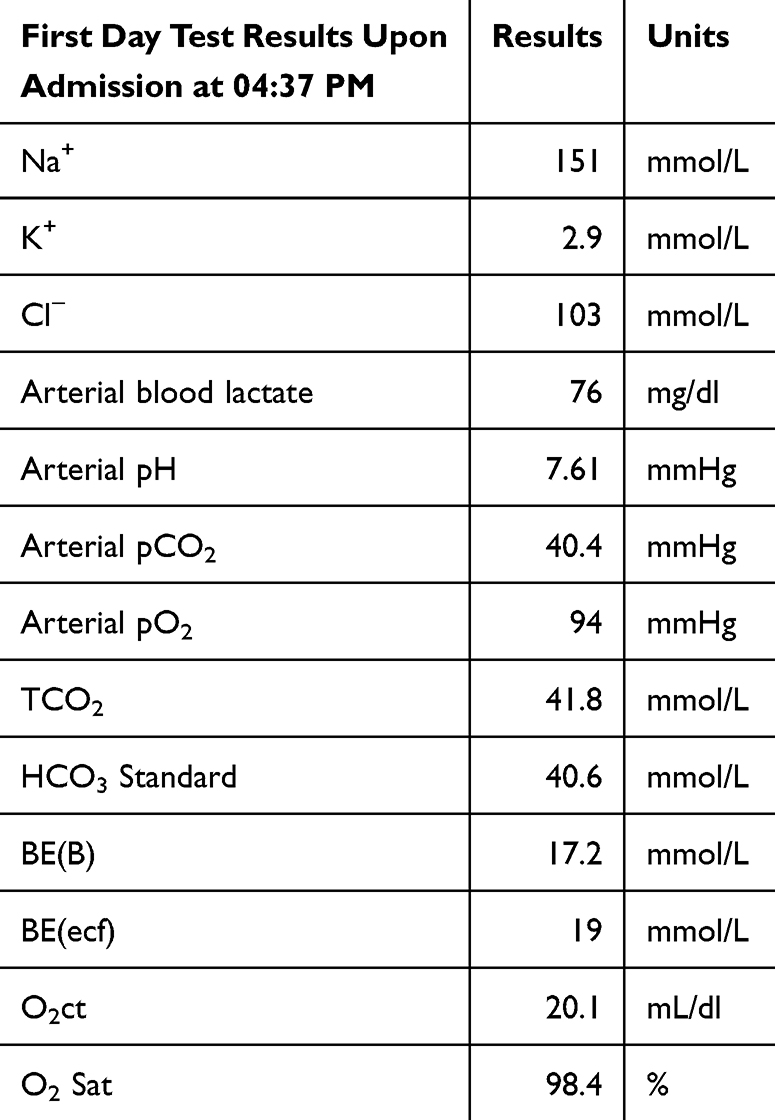 |
Table 2 Paraclinical Results in the Cardiovascular Intensive Care Unit |
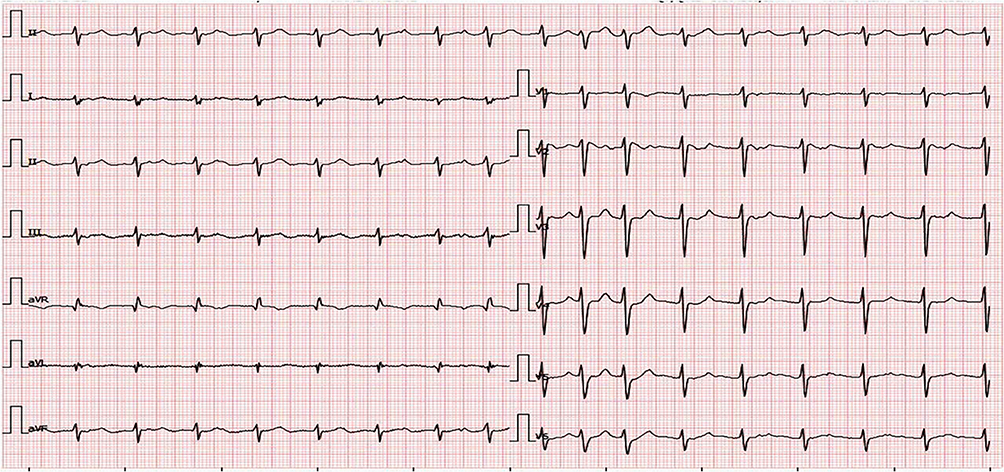 |
Figure 2 Photograph of ECG after treatment with 750mL of 4.2% sodium bicarbonate. |
On the 2nd day after hospitalization, arterial blood gas results recorded a pH of 7.52; pO2 of 146; pCO2 of 31.8; HCO3 of 26; and a magnesium level of 4.69 mmol/L. Although the patient’s QTc was prolonged (510ms), due to the high blood magnesium level (4.69 mmol/L) after using 4.5g of 15% magnesium sulfate, and the monitor only recorded short episodes of ventricular tachycardia, we discontinued the magnesium sulfate and continued to maintain lidocaine intravenously. On the same day, the patient suddenly developed a high fever twice at 39°C, cough with yellow sputum, and was supplemented with antibiotics for pneumonia treatment. At this point, the 4.2% Sodium bicarbonate and sedation were discontinued (Table 3).
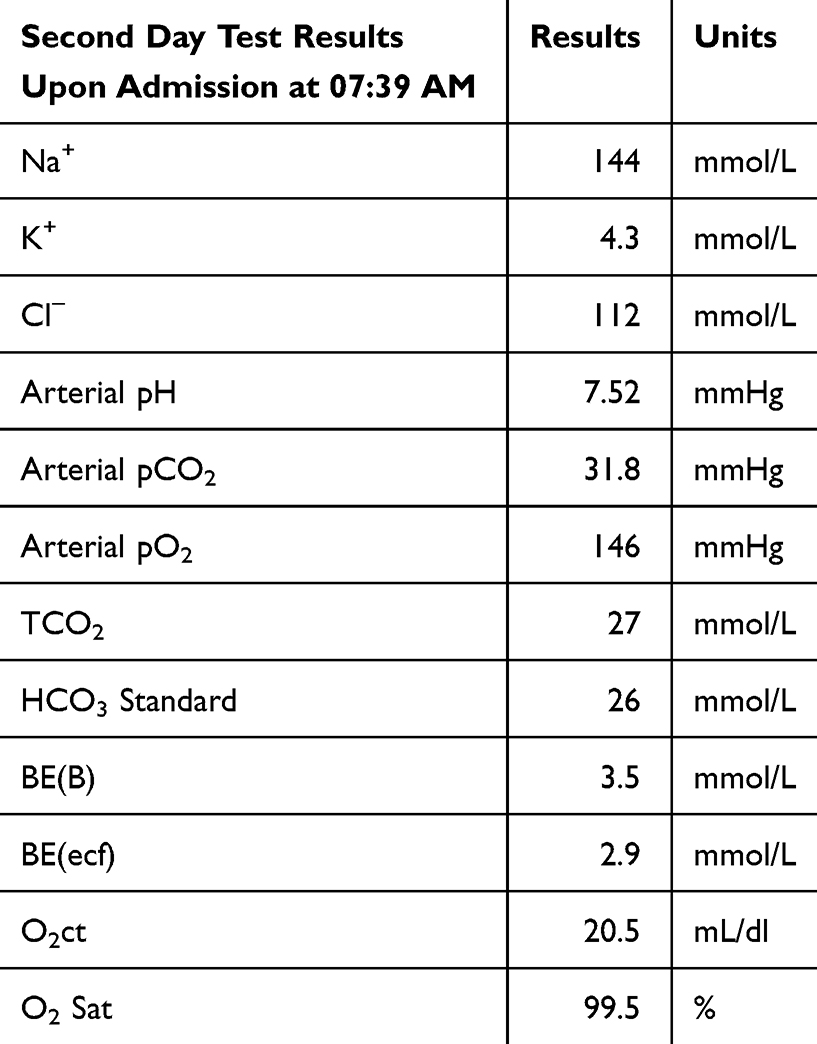 |
Table 3 Test Results on the Second Day After Hospital Admission |
At the end of the 3rd day of hospitalization, 2% lidocaine was discontinued for the patient. After discontinuing the use of 4.3% sodium bicarbonate and 2% lidocaine, the ECG showed a stable sinus rhythm of 95 cycles per minute, a narrowed QRS complex of 88 ms, and a QTc of 440 ms (Figure 3)(Table 4).
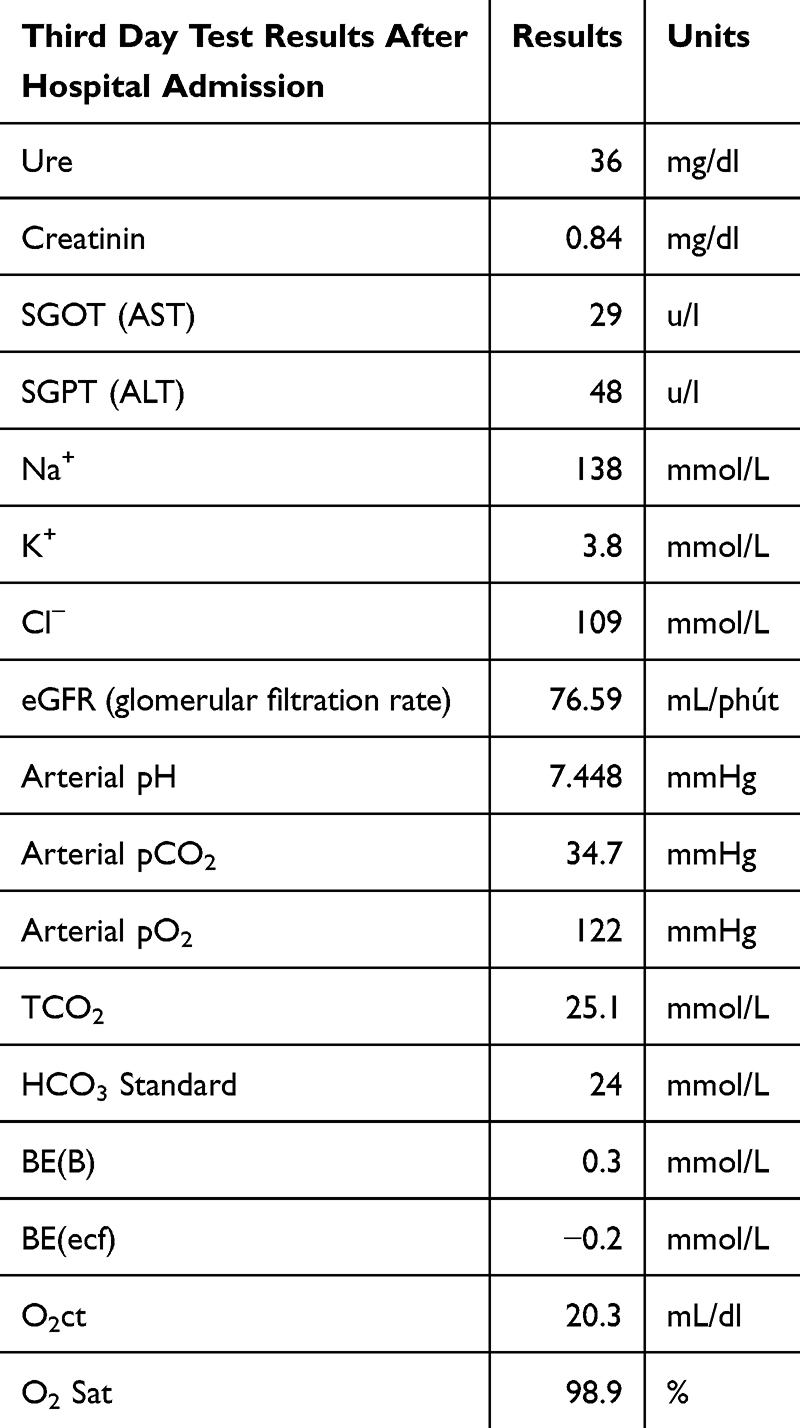 |
Table 4 Test Results on the Third Day After Hospital Admission |
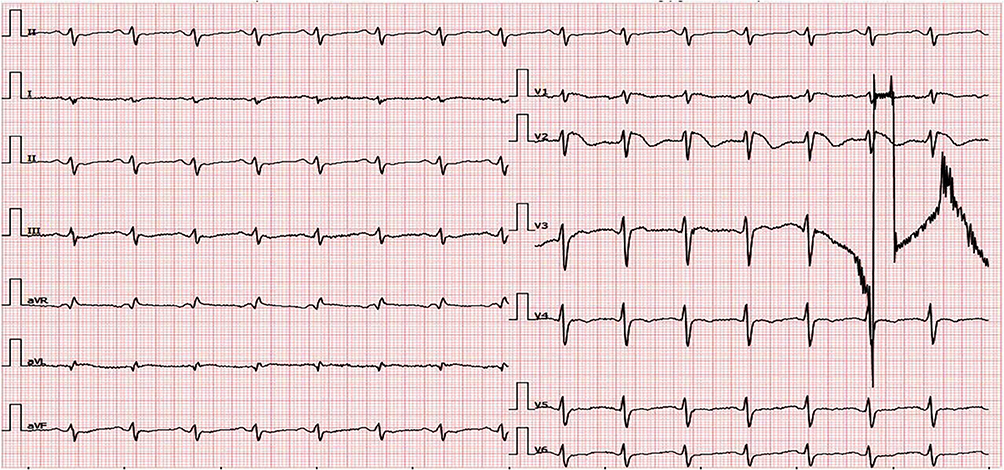 |
Figure 3 Photograph of ECG upon discontinuation of Sodium Bicarbonate 4.2% and Lidocaine 2%. |
The patient was successfully weaned off mechanical ventilation and extubated after 48 hours of sedation discontinuation, able to understand and follow commands. The patient recovered well, with no fever after 1 day of antibiotic treatment, and antibiotics were discontinued after 10 days. After 12 days of treatment, the patient was able to walk independently. After 15 days of treatment, the patient was discharged from the hospital in good recovery. The entire treatment process is summarized in Table 5.
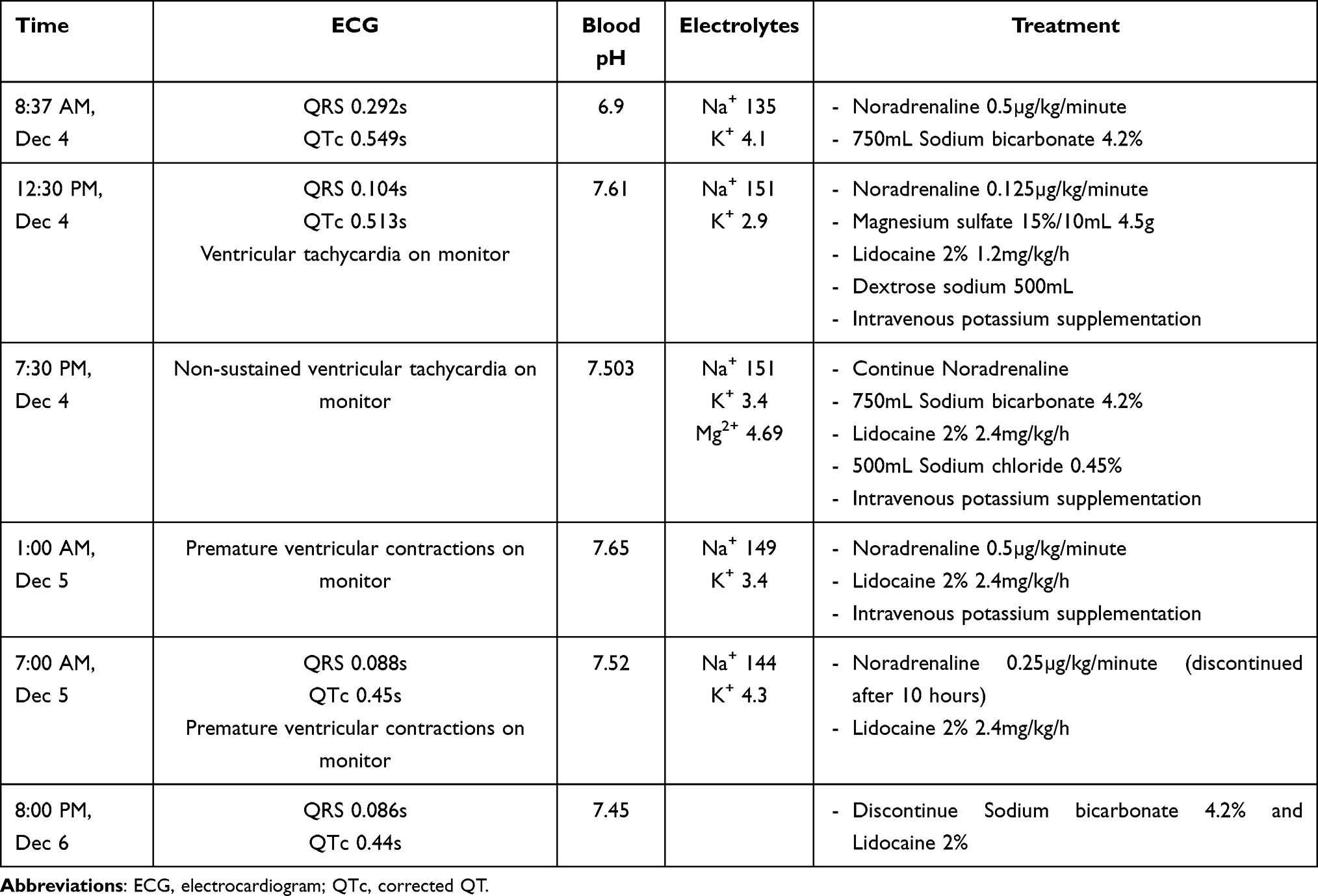 |
Table 5 Summary of ECG, Arterial Blood Gas pH, and Electrolyte Chart Progression During Treatment |
Discussion
As previously mentioned, the use of TCAs remains relatively high, and this is associated with a high rate of intentional poisoning and deaths related to this group of drugs. TCAs are rapidly absorbed through the gastrointestinal tract. Notably, these drugs have an anti-cholinergic effect which can reduce gastrointestinal motility, leading to decreased absorption and toxicity. Once absorbed into the bloodstream, TCAs have a long half-life due to their high protein binding and lipid solubility. Amitriptyline is metabolized in the liver through the CYP2C19, CYP3A4, and CYP2D6 systems into Nortriptyline, which is excreted by the kidneys. It is important that both Amitriptyline and its metabolite have the potential to cause poisoning. Symptoms of poisoning can last 24–48 hours, but some cases have been reported to last up to 5 days.5,8
Our patient presented with almost all the signs of amitriptyline poisoning. With regard to alpha-adrenergic receptor blockade, the patient required blood pressure support with Noradrenaline, as well as coma due to histamine receptor blockade and anticholinergic effects. We also observed brief seizures in the patient, as TCAs have agonist effects on GABA-A receptors.8,9 In addition, on the ECG, signs suggestive of TCA overdose included QRS>100ms, QTc>430ms, and R/S ratio >0.7 in aVR, all of which were present in this patient. The ECG is a factor that helps stratify risk in patients, guides treatment, and also plays an important role in the prognosis of cardiovascular and neurological complications (such as seizures, arrhythmias, torsades de pointes) more than the drug concentration in the blood.9
Determining the time the patient started taking the drug is crucial.9 In this patient, the duration of drug use was more than 6 hours, so general measures in drug poisoning management, such as gastric lavage, were nearly ineffective. Although the clinical evidence for the use of Sodium bicarbonate is still limited, it remains the standard treatment9 for TCAs poisoning through three mechanisms. Firstly, sodium bicarbonate increases the sodium concentration gradient across affected sodium channels, counteracting the effects of TCAs. Secondly, it raises the pH, leading to the dissociation of TCAs from sodium channels in the heart – the main cause of TCAs-related arrhythmias.10 Finally, at high pH, TCAs are more likely to bind to proteins, reducing the concentration of active TCAs in the blood.11 However, a pH greater than 7.6 can predispose the patient to arrhythmias.9 When we discovered that the patient’s blood pH was higher than 7.6, we promptly discontinued sodium bicarbonate infusion to avoid the risk of arrhythmias in the patient.
In addition to pH, electrolytes are also important considerations. The concentration of Magnesium sulfate should be maintained at 0.7–1.05 mmol/L to stabilize the myocardial cell membrane, and the potassium levels are recommended at 4.5–5.0 mmol/L to shorten the QT interval.12
In cases of hypotension that does not respond to fluid resuscitation, vasopressors should be considered. Due to the mechanism of action of TCAs, which is to block the reuptake of neurotransmitters, Noradrenaline (direct effect) is believed to be more beneficial than Dopamine (indirect effect).13 Indeed, the patient was treated with Noradrenaline and showed a good response.
Our patient was treated with Lidocaine to manage arrhythmias after careful consideration of the risks and benefits. Antiarrhythmic drugs should only be used after Sodium bicarbonate has been used and the patient’s condition has not stabilized. Class Ia (quinidine, procainamide, etc) or Class Ic (flecainide) drugs should not be used in the setting of acute TCAs poisoning due to their similar sodium channel blocking effects, which can lead to decreased conduction velocity and decreased myocardial contractility. On the other hand, Class II drugs should also be avoided due to the risk of hypotension that may lead to cardiac arrest, while Class III drugs (amiodarone) can further prolong the QT interval, increasing the risk of arrhythmias.14 Although Class Ib drugs (phenytoin, lidocaine) also have effects on sodium channels in the heart, they have a shorter duration of action than Class Ia, Ic drugs, and when competing with TCAs, they can help to restore more sodium channels to their normal state earlier, leading to increased myocardial conduction velocity.15
Plasma exchange is considered when other basic treatment methods are ineffective.16 This is due to the lipid-soluble and protein-binding properties of TCAs. Plasma exchange helps remove unbound drug. There have been several successful case reports. In 2013, Karaci reported a case of a 15-year-old female patient in Turkey who overdosed on Amitriptyline at a dose of 22mg/kg. The patient’s Glasgow Coma Scale (GCS) improved from 5 to 13 points after initial treatment with endotracheal intubation, gastric lavage, and sodium bicarbonate, followed by plasma exchange for 4 hours.17
In the United States, in 2012, a case was reported by Levine of a 12-year-old girl with amitriptyline overdose of unknown quantity who presented with cardiac arrest, seizures, prolonged QRS and QTc.18 The patient received similar initial treatment to our patient, including endotracheal intubation, vasopressors, sodium bicarbonate, and followed by 20% intravenous lipid emulsion, resulting in stabilization of blood pressure and gradual narrowing of the QRS. In 2014, Agarwala reported a case of a 44-year-old male patient who presented with somnolence, hypotension, wide QRS, seizures, and asystole. The patient was treated similarly with good results and a good recovery.19
The treatment with Sodium bicarbonate 4.2% and Lidocaine 2% yielded a positive response in our patient, leading us not to use plasma exchange. Upon returning for a follow-up five days post-discharge, the patient demonstrated satisfactory recovery. However, long-term monitoring is essential to evaluate any potential adverse effects of Amitriptyline on the patient’s current health and mental well-being.
Conclusion
TCAs poisoning is not uncommon in clinical practice. Advances in diagnosis and treatment have helped to risk stratify patients and provide effective treatment. Sodium bicarbonate, lidocaine, and plasma exchange have all been shown to be effective in clinical reports. The successful treatment of this case was due to the accurate identification and classification of the severity of the condition, timely intervention to maintain pH and electrolytes, and early correction of ventricular arrhythmias, which resulted in positive outcomes in the emergency management of the patient.
Ethics Approval and Written Consent from the Patient
This study was approved by the Institutional Review Board of Thu Duc City hospital. The privacy and personal identity information of all participants were protected in accordance with the Declaration of Helsinki. Written informed consent has been obtained from all participants.
Consent for Publication
Written informed consent was obtained from the patient for the publication of this case report and any accompanying images. A copy of the written consent is available for review by the Editor-in-Chief of this journal. We believe that the information presented in the manuscript is sufficient, and institutional approval is not required for the publication of this manuscript.
Funding
There is no funding to report.
Disclosure
The authors declare no conflicts of interest in this work.
References
1. López-Muñoz F, Alamo C. Monoaminergic neurotransmission: the history of the discovery of antidepressants from 1950s until today. Curr Pharm Des. 2009;15(14):1563–1586. doi:10.2174/138161209788168001
2. Liebelt EL. Cyclic Antidepressants. In: Hoffman RS, Howland MA, Lewin NA, Nelson LS, Goldfrank LR, editors. Goldfrank’s Toxicologic Emergencies, 10e. New York, NY: McGraw-Hill Education; 2015.
3. Kane SP. Amitriptyline, clincalc drugstats database. 2024. Available from: https://clincalc.com/DrugStats/Drugs/Amitriptyline.
4. Gummin DD, Mowry JB, Beuhler MC, et al. 2021 annual report of the national poison data system© (NPDS) from America’s poison centers: 39th annual report. Clin Toxicol. 2022;60(12):1381–1643. doi:10.1080/15563650.2022.2132768
5. Dempsey SK, Poklis JL, Sweat K, Cumpston K, Wolf CE. Acute toxicity from intravenous use of the tricyclic antidepressant tianeptine. J Anal Toxicol. 2017;41(6):547–550. doi:10.1093/jat/bkx034
6. Lubna NJ, Wada T, Nakamura Y, et al. Amitriptyline may have possibility to induce Brugada syndrome rather than long QT syndrome. Cardiovasc Toxicol. 2018;18(1):91–98. doi:10.1007/s12012-017-9417-z
7. Giwa A, Oey E. The return of an old nemesis: survival after severe tricyclic antidepressant toxicity, a case report. Toxicol Rep. 2018;5:357–362. doi:10.1016/j.toxrep.2018.03.009
8. Khalid MM, Waseem M. Tricyclic Antidepressant Toxicity. Treasure Island (FL): StatPearls Publishing; 2023.
9. Verbree F, Reijnen T, Mitrov-Winkelmolen L, Overdiek J, Dennesen PJNJCC. Tricyclic antidepressant poisoning: cardiovascular and neurological toxicity. Neth J Crit Care. 2016;24(2):16–20.
10. Blackman K, Brown SGA, Wilkes GJ. Plasma alkalinization for tricyclic antidepressant toxicity: a systematic review. Emergency Med. 2001;13(2):204–210. doi:10.1046/j.1442-2026.2001.00213.x
11. Body R, Bartram T, Azam F, Mackway-Jones K. Guidelines in emergency medicine network (GEMNet): guideline for the management of tricyclic antidepressant overdose. Emer Med J. 2011;28(4):347. doi:10.1136/emj.2010.091553
12. Kan A, de Lange D, Donker D, Meulenbelt J. Management of prolonged QT interval and torsades de pointes in the intoxicated patient. Netherlands J Med. 2014;72(3):119–126.
13. Zuidema X, Dünser MW, Wenzel V, Rozendaal FW, de Jager CPC. Terlipressin as an adjunct vasopressor in refractory hypotension after tricyclic antidepressant intoxication. Resuscitation. 2007;72(2):319–323. doi:10.1016/j.resuscitation.2006.07.005
14. Kerr GW, McGuffie AC, Wilkie S. Tricyclic antidepressant overdose: a review. Emer Med J. 2001;18(4):236–241. doi:10.1136/emj.18.4.236
15. Foianini A, Joseph Wiegand T, Benowitz N. What is the role of lidocaine or phenytoin in tricyclic antidepressant-induced cardiotoxicity? Clin Toxicol. 2010;48(4):325–330. doi:10.3109/15563650.2010.487050
16. Dönmez O, Cetinkaya M, Canbek R. Hemoperfusion in a child with amitriptyline intoxication. Pediatr Nephrol. 2005;20(1):105–107. doi:10.1007/s00467-004-1654-2
17. Karacı M, Özçetin M, Dilsiz G, Güçlü-Songür YG. Severe childhood amitriptyline intoxication and plasmapheresis: a case report. Turk J Pediatr. 2013;55(6):645–647.
18. Levine M, Brooks DE, Franken A, Graham R. Delayed-onset seizure and cardiac arrest after amitriptyline overdose, treated with intravenous lipid emulsion therapy. Pediatrics. 2012;130(2):e432–e438. doi:10.1542/peds.2011-2511
19. Agarwala R, Ahmed SZ, Wiegand TJ. Prolonged use of intravenous lipid emulsion in a severe tricyclic antidepressant overdose. J Med Toxicol. 2014;10(2):210–214. doi:10.1007/s13181-013-0353-4
 © 2024 The Author(s). This work is published and licensed by Dove Medical Press Limited. The
full terms of this license are available at https://www.dovepress.com/terms
and incorporate the Creative Commons Attribution
- Non Commercial (unported, 3.0) License.
By accessing the work you hereby accept the Terms. Non-commercial uses of the work are permitted
without any further permission from Dove Medical Press Limited, provided the work is properly
attributed. For permission for commercial use of this work, please see paragraphs 4.2 and 5 of our Terms.
© 2024 The Author(s). This work is published and licensed by Dove Medical Press Limited. The
full terms of this license are available at https://www.dovepress.com/terms
and incorporate the Creative Commons Attribution
- Non Commercial (unported, 3.0) License.
By accessing the work you hereby accept the Terms. Non-commercial uses of the work are permitted
without any further permission from Dove Medical Press Limited, provided the work is properly
attributed. For permission for commercial use of this work, please see paragraphs 4.2 and 5 of our Terms.