Back to Journals » Clinical, Cosmetic and Investigational Dermatology » Volume 19
Restorative Challenges: Reconstruction of Large Axillary Defects Following Surgery for Extramammary Paget’s Disease
Authors Wang T, Li H, Chen Z, Sun L
Received 29 December 2025
Accepted for publication 1 March 2026
Published 11 July 2026 Volume 2026:19 590107
DOI https://doi.org/10.2147/CCID.S590107
Checked for plagiarism Yes
Review by Single anonymous peer review
Peer reviewer comments 2
Editor who approved publication: Dr Monica K. Li
Tian Wang, Han Li, Zhaochao Chen, Lan Sun
Department of Dermatology, Nanjing Medical University Affiliated Suzhou Hospital, Suzhou, People’s Republic of China
*These authors contributed equally to this work
Correspondence: Zhaochao Chen, Department of Dermatology, Nanjing Medical University Affiliated Suzhou Hospital, Suzhou, People’s Republic of China, Email [email protected] Lan Sun, Department of Dermatology, Nanjing Medical University Affiliated Suzhou Hospital, Suzhou, People’s Republic of China, Email [email protected]
Abstract: Extramammary Paget’s disease (EMPD) is a rare malignant neoplasm arising from apocrine gland–bearing skin, with involvement of the axilla being particularly uncommon. Surgical excision remains the first-line treatment. However, management can be challenging because wide excision to achieve tumor-free margins may result in a large axillary defect in a high mobility region where scar contracture can compromise shoulder function. Here, we report a single case of axillary EMPD managed with surgical excision and reconstruction using a pedicled thoracodorsal artery perforator (TDAP) flap. This case highlights the pedicled TDAP flap as a reliable, muscle-sparing reconstructive option for managing large axillary defects after EMPD excision, offering favorable functional and aesthetic outcomes with minimal donor-site morbidity.
Keywords: extramammary Paget’s disease, axilla, thoracodorsal artery perforator flap, pedicled flap, reconstruction
Introduction
EMPD is a rare malignant cutaneous neoplasm arising in apocrine gland–bearing skin. It most commonly involves the vulva, genital region, and perianal area, while axillary involvement is exceedingly rare.1 Because its clinical manifestations often resemble benign inflammatory dermatoses such as eczema or dermatitis, EMPD is frequently overlooked in the early stage and is therefore often diagnosed only after the lesion has progressed to an extensive size.2
Surgical excision remains the first-line treatment for EMPD. To achieve histologically confirmed tumor-free margins, wide local excision is generally recommended.3 As a consequence, substantial skin and soft-tissue defects are often unavoidable. Given the unique anatomical and functional characteristics of the axilla, effective reconstruction of large defects while preserving adequate perfusion, shoulder mobility, and acceptable cosmetic appearance continues to represent a significant clinical challenge.
The TDAP flap is a flap that offers reliable vascularity, reduced donor-site morbidity, and favorable aesthetic outcomes. Although the TDAP flap has been widely used in breast and trunk reconstruction, its application in axillary defect reconstruction following EMPD excision has rarely been reported.4 In this report, we present a rare case of axillary EMPD successfully managed with wide local excision followed by immediate reconstruction using a pedicled TDAP flap, highlighting its feasibility and potential advantages in addressing challenging axillary defects.
Case Presentation
A 78-year-old man presented in May 2024 with a 1-year history of a gradually enlarging pruritic lesion in the left axilla. The lesion developed insidiously without an identifiable trigger and progressively increased in size. He denied fever, weight loss, or other systemic symptoms. No prior treatment had been administered.
Physical examination revealed no abnormalities on general or systemic evaluation, and no palpable superficial lymphadenopathy was detected. Dermatological examination showed a well-demarcated, infiltrative erythematous plaque in the left axilla, measuring approximately 8.0×7.0 cm. The lesion exhibited a dark-red coloration without erosion or ulceration. A diagnostic skin biopsy demonstrated intraepidermal nests of atypical Paget cells involving the epidermis and extending into the hair follicles (Figure 1a and b). Immunohistochemical staining revealed positivity for cytokeratin 7 (CK7), carcinoembryonic antigen (CEA), epithelial membrane antigen (EMA), and gross cystic disease fluid protein 15 (GCDFP-15), while cytokeratin 20 (CK20), cytokeratin 5/6 (CK5/6), S-100, and SOX10 were negative. The Ki-67 proliferation index was approximately 40%, and HER2 showed equivocal positivity (2+). These findings were consistent with EMPD.
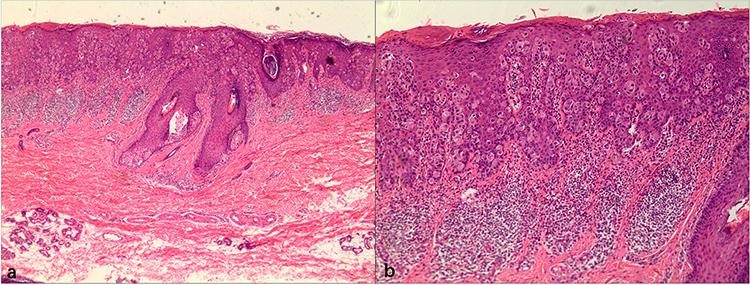 |
Figure 1 Histopathological findings of the lesion. (a) Epidermal acanthosis with scattered pale-staining atypical cells (H&E, ×40). (b) Paget cells with abundant pale cytoplasm and enlarged nuclei confined to the epidermis, with superficial dermal inflammatory infiltration (H&E, ×100). |
To exclude associated internal malignancy or distant metastasis, whole-body positron emission tomography–computed tomography (PET-CT) was performed and revealed no additional suspicious lesions, supporting a diagnosis of primary EMPD. Based on the diagnosis and tumor extent, surgical excision was planned. To assist in margin delineation, topical 20% 5-aminolevulinic acid (5-ALA) was applied prior to surgery. After incubation, lesion borders were assessed under red-light illumination according to fluorescence patterns, which guided surgical mapping.
Wide local excision was performed under general anesthesia on August 26, 2024. The lesion was excised with a 2-cm margin beyond the clinically and fluorescence-defined borders, resulting in a surgical defect measuring approximately 10.0×9.0 cm. The excised specimen was submitted in five labeled sections, including the central lesion and the 3, 6, 9, and 12 o’clock peripheral margins for intraoperative frozen-section analysis, which confirmed tumor-free margins. Given the size of the defect and the functional and aesthetic requirements of the axillary region, immediate reconstruction was performed using a pedicled TDAP flap. A skin paddle measuring approximately 11.0×6.0 cm was designed on the lateral thoracic region based on anatomical landmarks and ultrasound-assisted localization, and the flap was elevated with preservation of the dominant perforator (Figure 2a and b). The flap was subsequently rotated to cover the axillary defect, and layered closure was achieved (Figure 2c).
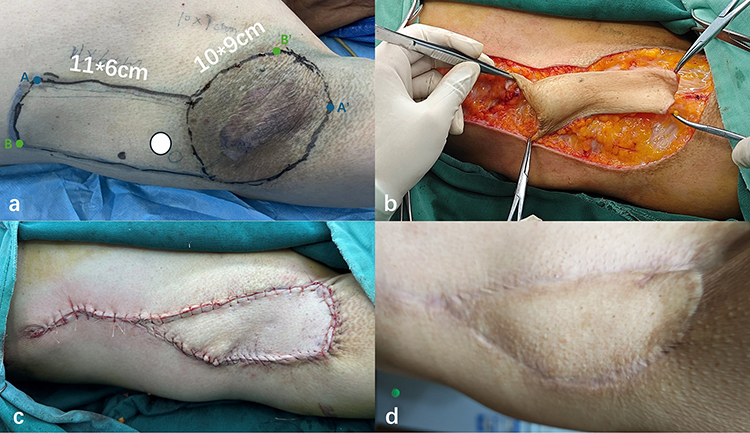 |
Figure 2 Reconstructive procedure and outcomes following axillary tumor excision. (a) Preoperative flap design. After excision of a 10×9 cm lesion, the vascular pedicle (white circle) was preserved, and the remaining flap was elevated and rotated (A to A′, B to B′) to cover the defect, followed by layered closure. (b) Intraoperative view showing flap elevation and transposition. (c) Immediate postoperative appearance after wound closure. (d) Clinical outcome at 12-month follow-up, demonstrating satisfactory healing and contour. |
Postoperative recovery was uneventful. Adjunctive red-light therapy and routine wound care were provided as part of postoperative management. Sutures were removed 10 days postoperatively. At the 12-month follow-up, the flap demonstrated complete survival with satisfactory contour and color match (Figure 2d). No evidence of local recurrence was observed, and shoulder mobility was fully preserved without functional limitation.
Discussion
Axillary EMPD is rare and typically requires wide surgical excision to achieve tumor-free margins. In the axilla, oncologic resection frequently results in large soft-tissue defects in a region characterized by constant motion and a high risk of postoperative contracture. Therefore, the key challenge in this case was the selection of an appropriate reconstructive strategy that could provide durable coverage while preserving shoulder mobility and achieving an acceptable cosmetic contour.
Reconstruction of axillary defects is uniquely demanding because even limited scar formation may translate into clinically significant restriction of shoulder abduction.5 In addition, the axilla is prone to friction, moisture, and repetitive stretching, which increases the risk of wound breakdown and hypertrophic scarring. An optimal reconstructive approach should therefore balance stable resurfacing, preservation of upper-limb function, and satisfactory aesthetic outcomes, particularly in elderly patients.
Several reconstructive options have been described following axillary tumor excision. Split-thickness skin grafting is technically straightforward but may be less durable in this highly mobile region and is associated with color and texture mismatch as well as a higher risk of secondary contracture.6 Pedicled musculocutaneous flaps, such as the latissimus dorsi flap, provide reliable vascularity and robust tissue coverage. However, they are associated with greater surgical trauma and potential donor-site functional impairment.7 These considerations underscore the need for a muscle-sparing reconstructive option that can reliably address large axillary defects without compromising shoulder function.
In the present case, a pedicled TDAP flap was selected to meet these competing reconstructive demands. By preserving the latissimus dorsi muscle, this technique minimizes functional donor-site morbidity while providing well-vascularized, pliable tissue suitable for axillary resurfacing. The use of adjacent skin facilitates a closer match in color and texture compared with skin grafting, which may contribute to a more acceptable cosmetic outcome. Importantly, the donor site was closed primarily without hematoma formation or delayed wound healing. Clinically, the flap survived completely, shoulder mobility was preserved, and the postoperative contour was satisfactory at 12 months, supporting the feasibility of this muscle-sparing pedicled option for large axillary defects following oncologic resection.
Despite these encouraging results, this report is limited by its single-case design and lack of direct comparison with alternative reconstructive strategies. A longer follow-up is needed because EMPD may recur after apparently complete excision. Future studies with standardized range of motion assessment and patient-reported outcomes are warranted to better define long-term functional benefit and generalizability.
Conclusion
In conclusion, complete surgical excision with histologically confirmed tumor-free margins remains essential in the management of extramammary Paget’s disease. In cases involving large axillary defects, reconstruction should be tailored to defect size, anatomical location, and patient-specific factors. Although limited by its single-case design, this report demonstrates that, with a 12-month follow-up showing no evidence of local recurrence, the pedicled thoracodorsal artery perforator flap may represent a reliable and function-preserving reconstructive option for managing complex axillary defects after tumor excision.
Abbreviations
EMPD, Extramammary Paget’s disease; TDAP, thoracodorsal artery perforator; CK7, cytokeratin 7; CEA, carcinoembryonic antigen; EMA, epithelial membrane antigen; GCDFP-15, gross cystic disease fluid protein 15; CK20, cytokeratin 20; CK5/6, cytokeratin 5/6; PET-CT, positron emission tomography–computed tomography; 5-ALA, 5-aminolevulinic acid.
Ethics Approval
Ethics approval was not required for the publication of this single case report according to institutional policy.
Consent for Publication
Informed consent was obtained for the publication of the case. This article adheres to the applicable CAse REport (CARE) guidelines.
Funding
There is no funding to report.
Disclosure
The authors report no conflicts of interest in this work.
References
1. Shah RR, Shah K, Wilson BN, et al. Extramammary Paget disease. Part I. epidemiology, pathogenesis, clinical features, and diagnosis. J Am Acad Dermatol. 2024;91(3):409–4. doi:10.1016/j.jaad.2023.07.1051
2. Weng S, Zhu N, Li D, et al. Clinical characteristics, treatment, and prognostic factors of patients with primary Extramammary Paget’s Disease (EMPD): a retrospective analysis of 44 patients from a single center and an analysis of data from the surveillance, epidemiology, and end results (SEER) database. Front Oncol. 2020;10:1114. doi:10.3389/fonc.2020.01114
3. Shah RR, Shah K, Wilson BN, et al. Extramammary Paget disease. Part II. Evidence-based approach to management. J Am Acad Dermatol. 2024;91(3):421–430. doi:10.1016/j.jaad.2023.07.1052
4. Hamdi M, Dias LPN. The thoracodorsal artery perforator (TDAP) flap. In: Hamdi M, Vidya R, Agrawal A, editors. Pedicled Flaps in Partial Breast Reconstruction. Springer International Publishing; 2023:37–45.
5. Sanz Aranda E, Yuste Bevanvente V, Reola Ramírez E, Perales Enguita A, Martí Ayats JM, Sobrino Casorrán A. Axillary reconstruction: proposal of a therapeutic algorithm based on systematic review of the literature. Eur J Plast Surg. 2023;46(1):9–14. doi:10.1007/s00238-022-01977-8
6. Chen K, Henn D, Januszyk M, et al. Disrupting mechanotransduction decreases fibrosis and contracture in split-thickness skin grafting. Sci Transl Med. 2022;14(645):eabj9152. doi:10.1126/scitranslmed.abj9152
7. Lee KT, Mun GH. A systematic review of functional donor-site morbidity after latissimus dorsi muscle transfer. Plast Reconstr Surg. 2014;134(2):303–314. doi:10.1097/PRS.0000000000000365
 © 2026 The Author(s). This work is published and licensed by Dove Medical Press Limited. The
full terms of this license are available at https://www.dovepress.com/terms
and incorporate the Creative Commons Attribution
- Non Commercial (unported, 4.0) License.
By accessing the work you hereby accept the Terms. Non-commercial uses of the work are permitted
without any further permission from Dove Medical Press Limited, provided the work is properly
attributed. For permission for commercial use of this work, please see paragraphs 4.2 and 5 of our Terms.
© 2026 The Author(s). This work is published and licensed by Dove Medical Press Limited. The
full terms of this license are available at https://www.dovepress.com/terms
and incorporate the Creative Commons Attribution
- Non Commercial (unported, 4.0) License.
By accessing the work you hereby accept the Terms. Non-commercial uses of the work are permitted
without any further permission from Dove Medical Press Limited, provided the work is properly
attributed. For permission for commercial use of this work, please see paragraphs 4.2 and 5 of our Terms.