Back to Journals » ClinicoEconomics and Outcomes Research » Volume 16
Resources Utilization Assessment and Cost-Minimization Analysis of the 6-Monthly Formulation of Triptorelin in the Treatment of Prostate Cancer in China
Authors Chen Y ![]() , Pan J, Zhong Y, Wu B, Yan M, Zhang R
, Pan J, Zhong Y, Wu B, Yan M, Zhang R
Received 6 July 2024
Accepted for publication 5 November 2024
Published 13 December 2024 Volume 2024:16 Pages 869—875
DOI https://doi.org/10.2147/CEOR.S485856
Checked for plagiarism Yes
Review by Single anonymous peer review
Peer reviewer comments 2
Editor who approved publication: Dr Xing Lin Feng
Ying Chen,1 Jiahua Pan,2 Yan Zhong,3 Bin Wu,1 Mengxia Yan,4 Ruiyun Zhang2
1Clinical Research Institute, Renji Hospital, School of Medicine, Shanghai Jiaotong University, Shanghai, 200000, People’s Republic of China; 2Department of Urology, Renji Hospital, School of Medicine, Shanghai Jiaotong University, Shanghai, 200000, People’s Republic of China; 3China Association for Promotion of Health Science and Technology, Beijing, 100000, People’s Republic of China; 4Department of Pharmacy, Ningbo Hangzhou Bay Hospital, Ningbo, 315000, People’s Republic of China
Correspondence: Ruiyun Zhang, Email [email protected]
Objective: Prostate Cancer can be treated with various formulations of Gonadotropin-Releasing Hormone Agonists (GnRHa), but cost analyses of these treatments in China are lacking. This study aims to evaluate the differences in cost and resource utilization between various formulations of GnRHa for Prostate Cancer by conducting a resource utilization assessment and cost minimization analysis.
Methods: From the perspective of society and medical healthcare, this study used the cost minimization model to generate cost and resource estimates for GnRHa drug acquisition and administration for “Current practice” and for a “Base case” scenario. In the “Base case” scenario, all of the patients who were receiving 1-monthly or 3-monthly GnRHa therapy in “Current practice” switched to a 6-monthly formulation triptorelin. Cost/Resource estimates were calculated per patient per administration and scaled to annualized population levels. Deterministic sensitivity analysis was conducted to explore the uncertainty of the model variables and applied assumptions.
Results: From a societal perspective, if all 1-monthly and 3-monthly formulations of GnRHa were switched to a 6-monthly formulation triptorelin, it is conservatively estimated that the annual societal cost could be reduced by ¥ 13,382,951.13, with an average annual cost savings of ¥ 46.53 per patient. Additionally, the 6-monthly formulation could save 3,608,973.91 hours annually, translating to an average time savings of 12.55 hours per patient, reducing treatment time by 78%. From a healthcare system perspective, if the introduction of the 6-monthly formulation of GnRHa is delayed, it would lead to an annual increase of ¥ 94 million in medical costs, and require an additional 64,445.96 working days for doctors and nurses. Deterministic sensitivity analysis demonstrated the model’s robustness, showing the 6-monthly GnRHa remains cost-effective across various parameter changes, with drug price being the most influential factor.
Conclusion: Compared to current 1-monthly and 3-monthly formulations, the 6-monthly GnRHa can reduce the total burden associated with prostate cancer treatment.
Keywords: triptorelin, prostate cancer, cost-minimization, budget impact
Introduction
Prostate cancer is one of the most important malignant tumors threatening the health of men in China. The incidence rate among Chinese men is 10.79 per 100,000, with a mortality rate of 3.82 per 100,000, placing it among the leading causes of male cancer-related deaths.1 The most common treatment involves the use of Gonadotropin-Releasing Hormone Agonists (GnRHa).2,3
Currently, the commonly used GnRHa in clinical practice includes leuprorelin, goserelin, and triptorelin. These drugs include a variety of dosage forms, and the dosage forms that have been marketed in China include 1-month dosage form GnRHa (1M GnRHa) and 3-month dosage form GnRHa (3M GnRHa). 22.5 mg triptorelin (called 6M GnRHa below) is the first 6-monthly GnRHa introduced into China in 2023 and was included in the medical insurance catalog. This formulation is primarily used for patients with locally advanced or metastatic prostate cancer. Studies indicate that the efficacy and safety of the 6M GnRHa are comparable to the 1M and 3M formulations.4,5 In addition, fewer injections result in a lower incidence of adverse reactions,5 reduced pain and anxiety,6 and improved patient compliance,7 ultimately enhancing the quality of life (QoL) for patients.8 In regions where long-acting GnRHa is available, patients prefer the 6M formulation.9–12 Research from the UK also demonstrates that the 6M GnRHa significantly reduces both costs and time.5,13
Despite these advantages, there is considerable uncertainty regarding the costs of transitioning from 1M and 3M to 6M GnRHa in China. Model-based analysis can inform better decisions by providing tools to assess the costs and benefits of these strategies. This study aims to comprehensively assess the time and cost associated with medical treatment and compare the resource utilization of the 6M GnRHa with the 1M/3M formulations through a cost-minimization analysis.
Materials and Methods
Overview of the Model
We adapted a previously developed cost minimization model introduced by Cornford.13 The time horizon is one year. Input data were sourced from published Chinese literature, and in the absence of data, expert opinions or conservative assumptions were used. A detailed summary of model parameters is provided in Table 1. To maintain consistency in the analysis, we assumed that patient compliance with different GnRHa dosage forms remained constant.
 |
Table 1 Model Parameters |
Patient Population Assumptions
Estimating the total number of patients treated with GnRHa involved three key factors: (1) the total number of patients with prostate cancer,14 (2) the distribution of patients across different disease stages, as this may influence treatment choices,15 and (3) the proportion of patients opting for GnRHa treatment at each disease stage based on treatment indications.16 Patients diagnosed with stage I or unknown stage were excluded, as they may not meet the indications for GnRHa treatment.29
Resource Inputs
The study comprehensively considered the resource consumption during the medical treatment process, mainly including time and cost. Time-related factors included round-trip transportation, registration waiting for,26–28 and injection. Since the round-trip transportation and injection time for each medical visit were unavailable, expert surveys provided estimated values. Costs were categorized into medical and social costs. Medical costs included drug acquisition, injection, and registration fees. Drug costs were calculated based on the market share of various formulations and the drug prices listed in the China Drug Catalog.17,18 Injection fees were derived from the median in documents across 31 provinces, while registration fees accounted for both specialist and general consultations.20–22 Social costs covered transportation25 and productivity losses, with the latter referring to labor costs for individuals aged 15–65, who make up 11.96% of the population14 and missed work for medical treatment.24 For those outside this age group, including 88.03% over 65 and 0.01% under 15,14 costs were estimated based on the need for accompanying care.30 The relevant inputs are detailed in Table 1.
Sensitivity Analysis
To ensure the robustness of the model, we conducted a univariate sensitivity analysis for medical prices, allowing prices to fluctuate by 20%. Parameters were adjusted one by one to assess their impact on the total cost. If parameter changes resulted in values exceeding 100%, we capped them at 100% to maintain the rationality of the outcomes.
Result
Base Case Analysis
Model estimates suggest that if all prostate cancer patients switch from 1/ 3M to 6M GnRHa treatment, the overall cost would decrease despite an increase in medical costs (Table 2). The most significant savings come from reduced productivity costs, while other expenses, such as injection, registration, transportation, and productivity losses, also decrease. In terms of time-saving, patients are expected to save a total of 3,608,973.96hours annually, with each patient saving an average of 12.55hours per year (representing a 78% reduction in time spent on diagnosis and treatment). For healthcare workers, this change could save approximately 515,567.71hours annually, equivalent to about 64,445.96 working days (based on an 8-hour workday). Detailed data are provided in Figure 1.
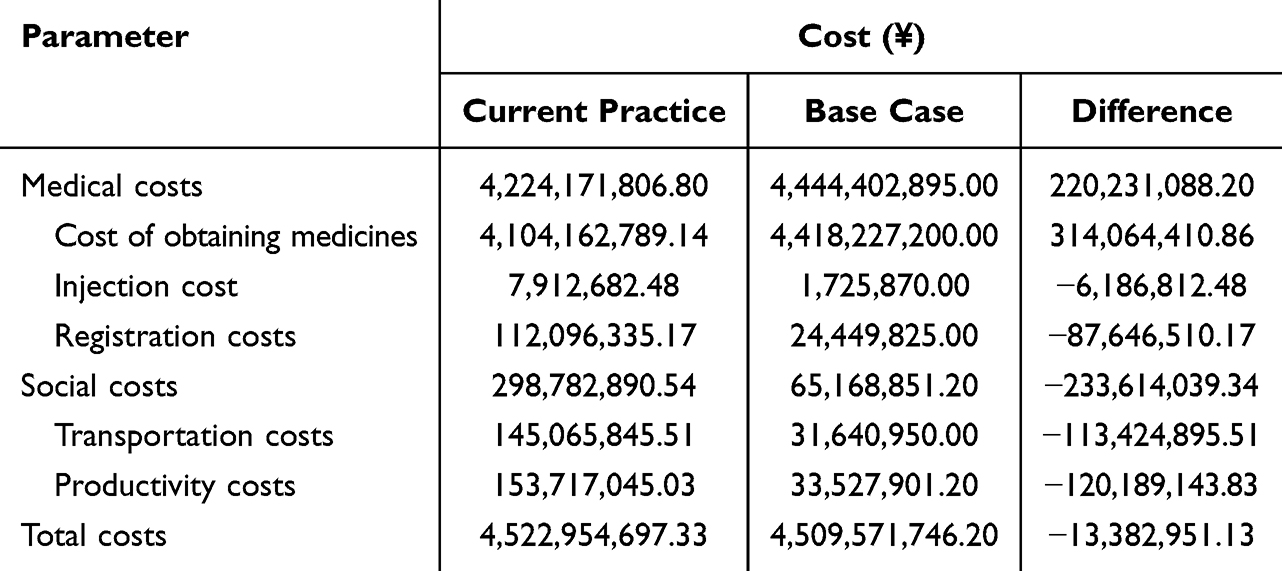 |
Table 2 Cost Changes in the “Base Case” Scenario Compared to “Current Practice” |
 |
Figure 1 Time savings in the ”base case” scenario compared to the ”current practice”. |
Sensitivity Analysis
As depicted in Figure 2, the 6M GnRHa remains economically advantageous under a wide range of parameter fluctuations. The factor with the most significant impact on the results was the price of the drug, which varied from -¥2,130,450,151.13 to ¥170,709,848.87.
 |
Figure 2 Tornado diagram of one-way sensitivity analysis. |
Discussion
This study is the first to conduct a cost-minimization analysis comparing the resource and cost utilization of 1M, 3M, and 6M GnRH for prostate cancer treatment in China from both social and medical perspectives. The results showed that compared with the 1M/3M GnRH, 6M GnRH increases medical costs from a medical perspective, but reduces social costs from a social perspective. The results of the sensitivity analysis showed that it saves money in many cases, but the impact on drug prices is significant.
Our findings are consistent with previous studies, which also found 6M triptorelin to be cost-effective.31 A real-world study in the UK and another modeling study also support this view.5,13 In addition, a discrete choice trial in Japan also considered the savings of intangible costs, and its results were similar to ours.32 Since the calculation of intangible costs is difficult and controversial, our study did not calculate this part of the cost. However, whether or not this part of the cost is included does not affect our research conclusions.
Differences in the availability of dosage forms exist globally. According to a 2021 survey, approximately 2/3 of prostate cancer patients in China use 1M GnRHa, while 2/3 of prostate cancer patients in Sweden use a 3M GnRHa.7,16 As of 2023, the 6M GnRHa has been introduced in China and is now included in the medical insurance catalog. The findings of this study offer valuable insights into the impact of this dosage form on society, the healthcare system, and patient outcomes. Future studies based on real-world data can further validate these conclusions.
Several limitations should be noted: 1) The proportion of expert consultation, time of round-trip transportation, and injection, these data are derived from expert interviews, and conservative assumptions are used, which may introduce some uncertainty. Future studies need to expand the data set to improve the availability of the parameters; 2) The data on parameters such as registration cost and transportation cost are extracted from documents or literature in some regions, which may not fully reflect the actual situation across the country. However, sensitivity analysis tested the uncertainty of these parameters, showing they had minimal impact on the overall results; 3) The number of experts interviewed is relatively limited, and they are all from tertiary hospitals, which may lead to overestimating the treatment costs of patients. 4) The study does not include all possible medical and social costs, such as patient examination fees. However, existing research indicates that the majority of cost savings result from fewer medical visits, making it unlikely that including additional cost types would alter the overall conclusions; in fact, it could potentially reinforce them. Finally, as the efficacy and safety of different GnRHa formulations are comparable, these factors were not considered in this study.
At present, China’s medical system faces the challenge of imbalance between the supply and demand of resources, especially in the allocation of high-quality medical resources, shortage of medical professionals, and supply of efficient drugs. The introduction of the 6M triptorelin formulation, the first long-acting sustained-release option approved for prostate cancer treatment in China, offers a promising solution to help alleviate these resource constraints.
Ethics
This study used publicly available population-level data that do not involve human participants, and therefore, did not require IRB or local ethics review board approval.
Funding
This publication was funded by Ipsen (China) International Trading Co.
Disclosure
The authors report no conflicts of interest in this work.
References
1. GBD Results. Institute for health metrics and evaluation. Available from: https://vizhub.healthdata.org/gbd-results.
2. Chinese expert consensus on testosterone management in prostate cancer (2021 edition). Available from: https://rs.yiigle.com/CN2021/1317833.htm0.
3. Prostate cancer diagnosis and treatment guidelines (2018 edition). Available from: https://guide.medlive.cn/guideline/17123.
4. Ploussard G, Mongiat-Artus P. Triptorelin in the management of prostate cancer. Future Oncol. 2013;9(1):93–102. doi:10.2217/fon.12.158
5. Cornford P, Jefferson K, Cole O, Gilbody J. Effects of initiating or switching to a six-monthly triptorelin formulation on prostate cancer patient-healthcare interactions and hospital resource use: a real-world, retrospective, non-interventional study. Oncol Ther. 2018;6(2):173–187. doi:10.1007/s40487-018-0087-1
6. Shore ND, Sieber P, Schimke L, Perzin A, Olsen S. Comparison of tolerability and adverse events following treatment with two GnRH agonists in patients with advanced prostate cancer. Urol Nurs. 2013;33(5):236–244,248. doi:10.7257/1053-816X.2013.33.5.236
7. George G, Garmo H, Rudman S, et al. Long-term adherence to GnRH agonists in men with prostate cancer. A nation-wide population-based study in prostate cancer data base Sweden. Scand J Urol. 2020;54(1):20–26. doi:10.1080/21681805.2019.1702093
8. Eisenhardt A, Schneider T, Scheithe K, Colling C, Heidenreich A. Quality of life of patients with prostate cancer under androgen deprivation with GnRH analogues: results of the noninterventional study TRIPTOSIX]. Urologe A. 2016;55(2):176–183. doi:10.1007/s00120-015-3989-7
9. Fode M, Nielsen TK, Al-Hamadani M, Andersen JR, Jakobsen H, Sønksen J. Preferred treatment frequency in patients receiving androgen deprivation therapy for advanced prostate cancer. Scand J Urol. 2014;48(2):183–188. doi:10.3109/21681805.2013.820789
10. Schulman C. Assessing the attitudes to prostate cancer treatment among European male patients. BJU Int. 2007;100 Suppl 1:6–11. doi:10.1111/j.1464-410X.2007.6976.x
11. Chung E, Watt H, Glasgow A, Skyring T. Patient rationale in selecting androgen deprivation (PRISAD): do we give patients what they want? Med Oncol. 2009;26(4):420–423. doi:10.1007/s12032-008-9139-y
12. Lebret T, Davin JL, Hennequin C, et al. Selection criteria for initiation and renewal of luteinizing hormone-releasing hormone agonist therapy in patients with prostate cancer: a French prospective observational study. Ther Adv Urol. 2014;6(6):205–214. doi:10.1177/1756287214542418
13. Cornford P, Halpin C, Sassmann J, Frankcom I, Braybrook S. Increased use of 6-monthly gonadotropin-releasing hormone agonist therapy for prostate cancer: a capacity and cost-minimization analysis for England. J Med Econ. 2023;26(1):208–218. doi:10.1080/13696998.2023.2172281
14. CancerMPact® - Cerner Enviza. Available from: https://www.cernerenviza.com/syndicated-insights-and-reports-for-life-sciences/cancermpact.
15. Xu L, Wang J, Guo B, et al. Comparison of clinical and survival characteristics between prostate cancer patients of PSA-based screening and clinical diagnosis in China. Oncotarget. 2018;9(1):428–441. doi:10.18632/oncotarget.20787
16. Gu W, Ye D. Current status of gonadotropin-releasing hormone agonists in the treatment of prostate cancer. Chin J Urol. 2021;42(10):747–751. doi:10.3760/cma.j.cn112330-20210408-00177
17. Available IQVIA Data - IQVIA. Available from: https://www.iqvia.com/insights/the-iqvia-institute/available-iqvia-data.
18. Chinese list prices. Available from: https://www.udesk.cn/.
19. Prescribing Information. Available from: https://db.yaozh.com/instruct?comprehensivesearchcontent.
20. Shenzhen medical service price item catalog. Available from: http://hsa.sz.gov.cn/zwgk/zcfgjzcjd/zcfg/jggl/content/post_9040682.html.
21. Shanghai medical service price item catalog. Available from: https://wsjkw.sh.gov.cn/ylsfbz/index.html.
22. Fujian medical service price item catalog. Available from: http://ybj.fujian.gov.cn/zfxxgkzl/zc/xzgfxwj/xxyxgfxwjdyp/202306/t20230616_6188091.htm.
23. China Census Yearbook-2020. Available from: http://www.stats.gov.cn/sj/pcsj/rkpc/7rp/indexch.htm.
24. Minimum wage standards in each region of China. Available from: http://www.mohrss.gov.cn/SYrlzyhshbzb/laodongguanxi_/fwyd/202301/t20230102_492654.html.
25. Li Y, Qian D, Zhou S, Mao Z, Hu D, Lu J. Comparative study of direct economic burden of inpatients with lung cancer between urban and rural areas in a certain region. Chongqing Med Sci. 2016;45(5):661–663.
26. Shi Y. Quantitative statistics and analysis of out-patient waiting time in general hospital. Chin Hosp Stat. 2008;3:261–263.
27. Liu H, liu Z, Shi Y, Tan M, He C. Quantitative analysis and research on waiting time of outpatients in West China Hospital. 中国医院. 2012;16(11 vo 16):36–37.
28. Liang Y, Bao Y. Investigation and analysis of waiting time for medical treatment in Shanghai. J Shanghai Jiao Tong Univ. 2012;10 vo 32:1368–1372.
29. Decapeptyl SR 22 5.g - Summary of Product Characteristics (SmPC) - (emc). Available from: https://www.medicines.org.uk/emc/product/5906/smpc.
30. How can large general hospitals adapt outpatient spaces for an aging population of over 260 million seniors? Available from: http://www.360doc.com/content/12/0121/07/4310958_978633285.shtml.
31. Tang X, Zhang T, Li J, et al. Pharmacoeconomic evaluation of Triptorelin in the treatment of locally advanced or metastatic prostate cancer in China. Chin J Hospital Pharm. 2022;42(16):1725–1729. doi:10.13286/j.1001-5213.2022.16.18
32. Goto R, Uda A, Hiroi S, Iwasaki K, Takashima K, Oya M. Cost analysis of leuprorelin acetate in Japanese prostate cancer patients: comparison between 6-month and 3-month depot formulations. J Med Econ. 2017;20(11):1155–1162. doi:10.1080/13696998.2017.1362410
 © 2024 The Author(s). This work is published and licensed by Dove Medical Press Limited. The
full terms of this license are available at https://www.dovepress.com/terms
and incorporate the Creative Commons Attribution
- Non Commercial (unported, 3.0) License.
By accessing the work you hereby accept the Terms. Non-commercial uses of the work are permitted
without any further permission from Dove Medical Press Limited, provided the work is properly
attributed. For permission for commercial use of this work, please see paragraphs 4.2 and 5 of our Terms.
© 2024 The Author(s). This work is published and licensed by Dove Medical Press Limited. The
full terms of this license are available at https://www.dovepress.com/terms
and incorporate the Creative Commons Attribution
- Non Commercial (unported, 3.0) License.
By accessing the work you hereby accept the Terms. Non-commercial uses of the work are permitted
without any further permission from Dove Medical Press Limited, provided the work is properly
attributed. For permission for commercial use of this work, please see paragraphs 4.2 and 5 of our Terms.