Back to Journals » International Medical Case Reports Journal » Volume 13
Resolution of Long-Standing Diabetes Mellitus Two Years After Surgery for Growth Hormone Producing Pituitary Tumor
Authors Sreeramaneni PGA ![]() , Ghanta RK
, Ghanta RK
Received 2 November 2019
Accepted for publication 18 December 2019
Published 28 February 2020 Volume 2020:13 Pages 71—75
DOI https://doi.org/10.2147/IMCRJ.S236972
Checked for plagiarism Yes
Review by Single anonymous peer review
Peer reviewer comments 2
Editor who approved publication: Professor Ronald Prineas
Video abstract presented by Poorna Gopal Azad Sreeramaneni.
Views: 6777
Poorna Gopal Azad Sreeramaneni,1 Rajesh K Ghanta2
1Department of Endocrinology, Sreeramaneni Sumanth Krishna Endocrinology, Diabetes and Thyroid Hospitals, Vijayawada, India; 2Department of Neurosurgery, Suraksha Hospitals, Vijayawada, India
Correspondence: Poorna Gopal Azad Sreeramaneni
Department of Endocrinology, Sreeramaneni Sumanth Krishna Endocrinology, Diabetes and Thyroid Hospitals, Vijayawada 520002, India
Tel +91 8662436156
Email [email protected]
Abstract: Excess serum growth hormone (GH) induces insulin resistance leading to reduced uptake of glucose in peripheral tissues, gluconeogenesis in the liver and lipolysis and finally an increase in the blood glucose levels. We report a case where a 54-year-old woman presented with uncontrolled blood glucose levels since 5 years. On examination, she had signs and symptoms consistent with acromegaly including recurrent headaches, sleep apnea, soft tissue swelling, enlargements of the feet, hands, ears and lips, mandibular overgrowth, forehead protrusio and teeth spacing. She was on oral hypoglycemic agents (OHAs) for 12 years before she visited our hospital, but the blood glucose levels have been uncontrolled for the past 5 years with recurrent hyperglycaemic and occasional hypoglycaemic events. She underwent pituitary surgery for GH producing tumor and 2 years post surgery, we had to stop all the medications for the diabetes mellitus. This indicates that even long-standing diabetes mellitus can resolve in some patients with acromegaly.
Keywords: diabetes control in growth hormone pituitary tumor, surgery for growth hormone producing pituitary tumor
Learning Points
Once the diagnosis of acromegaly is made, it is recommended to increase the dose of insulin sensitizers like metformin and reduce the dose of sulfonylureas like glimepiride to preserve the pancreatic beta cell mass to make it possible in future to stop the medications directed towards controlling blood glucose levels completely.1
Even for patients with long-standing diabetes mellitus in acromegaly, it is possible to stop the anti-diabetic medications within few years after the removal of GH producing tumor.
In patients with very high GH levels at the time of diagnosis (>40 ng/mL), second pituitary surgery might be required even after a successful surgery to meet the required results.
Dopamine agonists like cabergoline might be required to reduce the IGF-1 levels along with pituitary surgery.
Background
In this patient, the acromegaly was undiagnosed for several years. The patient informed that the changes in the face, suggestive of acromegaly, started around 10 years before she was finally diagnosed of the condition. At the time of diagnosis, the serum GH levels were more than 40 ng/mL. The GH testing was done through chemiluminescence method.
Case Presentation
A 54-year-old woman presented with uncontrolled blood glucose levels with history of diabetes mellitus since 12 years. Her blood glucose levels have been uncontrolled since 5 years with HbA1C at the time of the diagnosis of acromegaly at around 12%. Her facial features like mandibular overgrowth, unusually thick lips (see Figure 1), forehead protrusion, and other signs like enlarged hands and feet raised the suspicion of acromegaly2,3 in which the pituitary produces an excess of growth hormone. High serum growth hormone levels cause insulin resistance, gluconeogenesis in the liver and lipolysis leading to uncontrolled blood glucose levels.4,5 As the serum growth hormones levels increase so do the blood glucose levels.
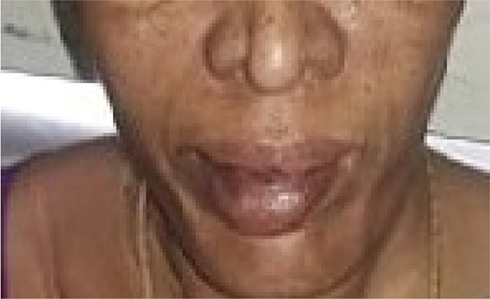 |
Figure 1 Unusually thick lips and mandibular overgrowth. |
Investigation
Growth Hormone levels were high at >40 ng/mL at the initial visit. OGTT suppression test was done and the fasting GH levels were >40 ng/mL, 38.6 ng/mL at 1 hrs and 38.7 ng/mL at 2 hrs after the administration of 100 g of glucose.
IGF1 levels were elevated at 783 ng/mL (normal value: 94–252 ng/mL)
Prolactin was 3.98 ng/mL and LH was 12.3 mIU/mL. ACTH (45 pg/mL) and cortisol (9.94 mcg/dl) levels were also within the normal ranges. HbA1c level was 12%. Fasting blood glucose level was 248 mg/dl and postprandial blood glucose level was 322 mg/dl.
MRI of pituitary revealed asymmetrical enlargement of the anterior pituitary gland on the left side with the involvement of the left cavernous sinus (see Figures 2 and 3).
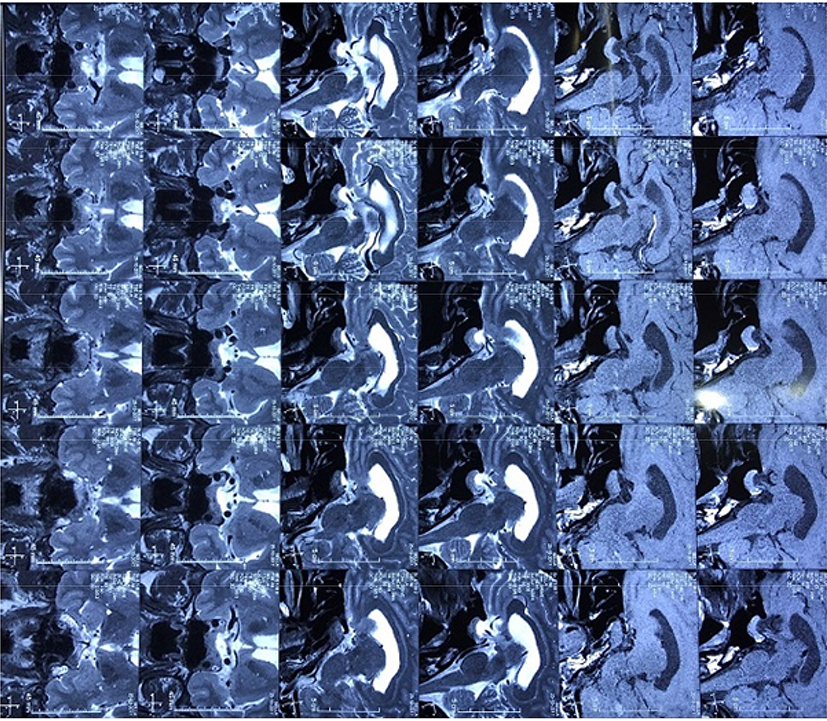 |
Figure 2 MRI of the pituitary and the brain. Film number one. |
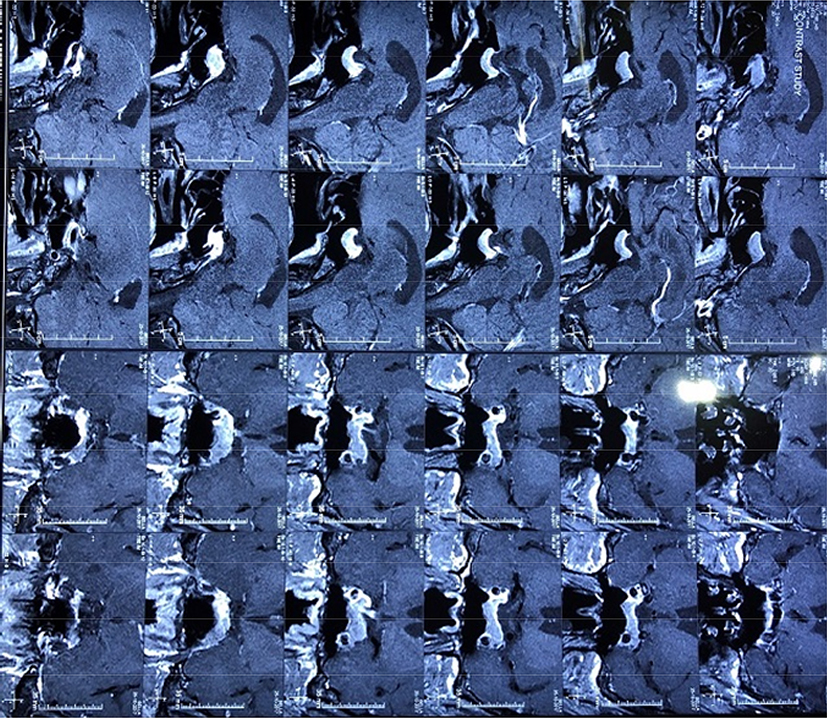 |
Figure 3 MRI of the pituitary and the brain. Film number two. |
Treatment and Outcome
Pituitary surgery was performed in November 2017 by Endoscopic Endonasal approach with excision of the pituitary macroadenoma. Three months post-surgery, the GH levels reduced from >40 ng/mL to 21.8 ng/mL. MRI pituitary, which was repeated 3 months post-surgery, showed a residual mass towards left side of the sella abutting the left ICA and showing homogenous enlargement. Second pituitary surgery was performed 4 months after the first surgery. After the second surgery on the pituitary, cabergoline was initiated at 0.5 mg once weekly to aid in reducing the GH levels which was later decreased to 0.5 mg once weekly and was completely stopped after 1 year. Dopamine agonists like cabergoline are effective and well tolerated treatment in acromegaly in lowering the serum GH levels.12
During the time of surgery, the blood glucose levels have been controlled with insulin therapy and metformin. Blood glucose levels were maintained below 180 mg/dl. Serum growth hormone levels were tested every 3 months for 2 years.
Three months after the second surgery, the serum GH level further lowered to around 14 ng/mL. Blood glucose levels were controlled with insulin therapy thrice daily which was reduced to twice daily later on along with metformin 1 g twice daily. At much later stage the blood glucose levels were controlled with metformin, sitagliptin and insulin once daily instead of twice daily. The HbA1c levels reduced from 12% at the initial diagnosis of acromegaly to 6.4% (Table 1) two years post surgery. It took almost 2 years since the first surgery on the pituitary for the serum GH levels to reduce to 7 ng/mL (Table 2). At this stage, all the medications directed towards the control of blood glucose levels including insulin and oral medications were stopped due to repeated incidents of hypoglycemia. Even after stopping all the medications for diabetes mellitus, the blood glucose levels have been well controlled with fasting blood glucose at around 130 mg/dl and postprandial blood glucose around 160 mg/dl and HbA1C of around 6.4%.
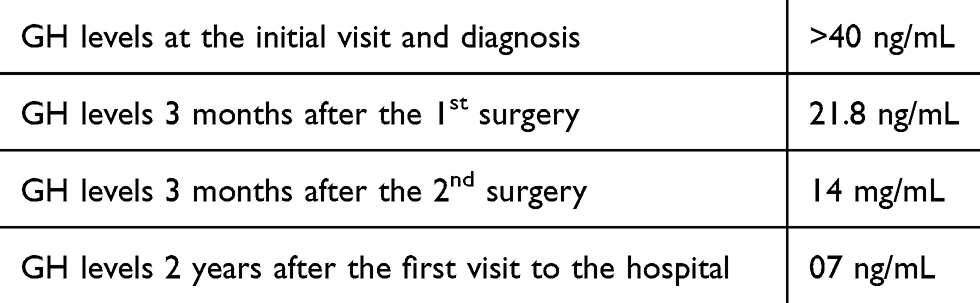 |
Table 1 Growth Hormone Levels Timeline |
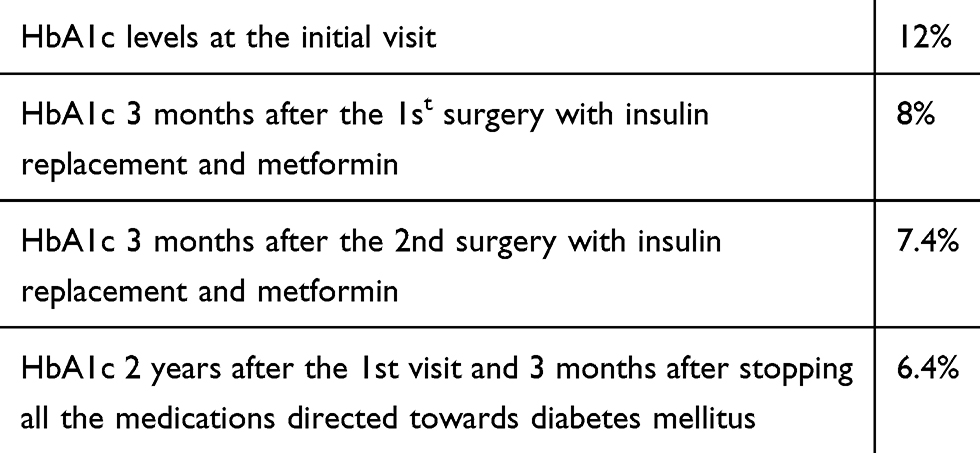 |
Table 2 HbA1c Levels Timeline |
Discussion
Acromegaly is rare and occurs in around 2.8 to 13.7 per 100,0000 people.6 Diabetes mellitus is present in around 12–37% of patients with acromegaly.7 High serum growth hormone levels lead to high blood glucose state because of high insulin resistance, gluconeogenesis and also lipolysis. Patients with acromegaly can also develop ketoacidosis. In fact in some patients with acromegaly, diabetic ketoacidosis can be the presenting complaint before the diagnosis of acromegaly is made.10 Hormones like glucagon, adrenaline, cortisol and growth hormone antagonize the insulin effect on blood glucose levels and thereby increasing the blood glucose levels.8,9 Also, growth hormone increases the blood glucose levels through gluconeogenesis.11 As the patients GH levels kept increasing over the years, blood glucose levels in this patient also kept fluctuating with high HbA1c levels for 5 years before the acromegaly was diagnosed. Once the GH levels reduced to around 7 ng/mL, the medications directed towards diabetes mellitus had to be completely stopped, This indicates in some cases of acromegaly where there is very high production of GH, even long-standing diabetes mellitus might resolve in some cases after drastic reduction in the GH levels. It took more than 2 years for the medications directed towards diabetes mellitus to be stopped in this patient.
Also, some signs and symptoms which were present at the time of diagnosis of acromegaly like sleep apnea, hypertension, recurrent headaches and soft tissue swelling have subsided. However, skull deformities like cranial thickening did not show much improvement which is usually seen in many patients of acromegaly even if their GH levels have drastically reduced.14
Though most cases of Acromegaly are benign and non-aggressive, some can behave aggressively compromising local surrounding structures. These tumors tend to recur after the pituitary surgery and respond poorly to the somatostatin analogs.13 Treatment with somatostatin analogs bound with 90Y-DOTATATE maybe an option for aggressive tumors not responding to other methods.15
Patient Consent
Oral consent has been obtained from the patient and written informed consent has been provided by the patient’s family to have the case details and any accompanying images published.
Ethics Approval
Institutional review board approval is not required at our institution. Name of the patient has not been mentioned in the paper. The patient received treatment according to the current standard of care.
Acknowledgments
We would like to extend special thanks to Dr Benjamin Glaser and Dr Dresner Rivka Polak of Department of Endocrinology and Metabolism, Hadassah Medical Centre, Ein Kerem, Jerusalem, Israel. We also thank Dr Navya Sriramaneni, Ms Aishwarya Sreeramaneni and Mrs Gandharva Rani Sreeramaneni, MA who helped us in preparing this article.
Author Contributions in the Treatment
Dr Poorna Gopal Azad Sreeramaneni, Endocrinologist, first diagnosed the acromegaly in the patient and followed the blood glucose levels and growth hormone levels. Dr Rajesk K Ghanta, senior Neurosurgeon, performed the two surgeries on the pituitary and also followed up the growth hormone levels along with Dr Poorna.
Funding
This research did not receive any specific grant from any funding agency in the public, commercial or not-for-profit sector.
Disclosure
There is no conflict of interest that could be perceived as prejudicing the impartiality of the research reported.
References
1. Page KA, Reisman T. Interventions to preserve beta-cell function in the management and prevention of type 2 diabetes. Curr Diab Rep. 2013;13(2):252–260. doi:10.1007/s11892-013-0363-2
2. Acromegaly. Available from: https://www.niddk.nih.gov/health-information/endocrine-diseases/acromegaly.
3. Dineen R, Stewart PM, Sherlock M. Acromegaly. QJM Int J Med. 2017;110(7):411–420. doi:10.1093/qjmed/hcw004
4. Takano A, Haruta T, Iwata M, et al. Growth hormone induces cellular insulin resistance by uncoupling phosphatidylinositol 3-kinase and its downstream signals in 3t3-l1 adipocytes. Diabetes. 2001;50:1891–1900. doi:10.2337/diabetes.50.8.1891
5. Vila G, Jørgensen JO, Luger A, Stalla GK. Insulin resistance in patients with acromegaly. Frontiers in Endocrinology. 2019;10. doi:10.3389/fendo.2019.00509
6. Lavrentaki A, Paluzzi A, JA W, Karavitaki N. Epidemiology of acromegaly: review of population studies. Pituitary. 2017;20(1):4–9. doi:10.1007/s11102-016-0754-x
7. Hannon AM, Thompson CJ, Sherlock M. Diabetes in Patients With Acromegaly. Curr Diab Rep. 2017;17(2):8. doi:10.1007/s11892-017-0838-7
8. Møller N, Jørgensen JO. Effects of growth hormone on glucose, lipid, and protein metabolism in human subjects. Endocr Rev. 2009;30(2):152–177. doi:10.1210/er.2008-0027
9. Smith U, Attvall S, Eriksson J, Fowelin J, Lönnroth P, Wesslau C. The insulin-antagonistic effect of the counterregulatory hormones — clinical and mechanistic aspects. In: Östenson CG, Efendić S, Vranic M, editors. New Concepts in the Pathogenesis of NIDDM. Boston, MA: Springer; 1993. doi:10.1007/978-1-4615-2910-1_12
10. Simmons LR, Hughes K, Markovic TP, Elizabeth L. Patients with acromegaly also develop ketoacidosis. Chua Clin Diabetes. 2012;30(4):170–172. doi:10.2337/diaclin.30.4.170
11. Vijayakumar A, Yakar S, LeRoith D. The intricate role of growth hormone in metabolism. Front Endocrinol. 2011;2. doi:10.3389/fendo.2011.00032.
12. Abs R, Verhelst J, Maiter D, et al. Cabergoline in the treatment of acromegaly: a study in 64 patients. J Clin Endocrinol Metab. 1998;83(2):374–378. doi:10.1210/jcem.83.2.4556
13. Carrasco CA, Gadelha M, Manavela M, et al. Aggressive tumors and difficult choices in acromegaly. Pituitary. 2014;17 Suppl 1(Suppl 1):S24–S29. doi:10.1007/s11102-013-0538-5
14. Rick JW, Jahangiri A, Flanigan PM, Aghi MK. Patients cured of acromegaly do not experience improvement of their skull deformities. Pituitary. 2017;20:292–294. doi:10.1007/s11102-016-0741-2
15. Waligórska-Stachura J, Gut P, Sawicka-Gutaj N, et al. Growth hormone–secreting macroadenoma of the pituitary gland successfully treated with the radiolabeled somatostatin analog 90Y-DOTATATE: case report. J Neurosurg. 2016;125:346–349. doi:10.3171/2015.6.JNS15363
 © 2020 The Author(s). This work is published and licensed by Dove Medical Press Limited. The
full terms of this license are available at https://www.dovepress.com/terms
and incorporate the Creative Commons Attribution
- Non Commercial (unported, 3.0) License.
By accessing the work you hereby accept the Terms. Non-commercial uses of the work are permitted
without any further permission from Dove Medical Press Limited, provided the work is properly
attributed. For permission for commercial use of this work, please see paragraphs 4.2 and 5 of our Terms.
© 2020 The Author(s). This work is published and licensed by Dove Medical Press Limited. The
full terms of this license are available at https://www.dovepress.com/terms
and incorporate the Creative Commons Attribution
- Non Commercial (unported, 3.0) License.
By accessing the work you hereby accept the Terms. Non-commercial uses of the work are permitted
without any further permission from Dove Medical Press Limited, provided the work is properly
attributed. For permission for commercial use of this work, please see paragraphs 4.2 and 5 of our Terms.