Back to Archived Journals » Integrated Blood Pressure Control » Volume 13
Resistant Hypertension: Where are We Now and Where Do We Go from Here?
Received 17 April 2020
Accepted for publication 21 June 2020
Published 5 August 2020 Volume 2020:13 Pages 83—93
DOI https://doi.org/10.2147/IBPC.S223334
Checked for plagiarism Yes
Review by Single anonymous peer review
Peer reviewer comments 2
Editor who approved publication: Professor Turgay Celik
Mansur K Pathan, Debbie L Cohen
Perelman School of Medicine at the University of Pennsylvania, Renal, Electrolyte and Hypertension Division, Philadelphia, PA 19104, USA
Correspondence: Debbie L Cohen; Mansur K Pathan
Perelman School of Medicine at the University of Pennsylvania, Renal, Electrolyte and Hypertension Division, 1 Founders Building, 3400 Spruce Street, Philadelphia, PA 19104, USA
Tel + 1 215-615-0794
Email [email protected]; [email protected]
Abstract: Resistant hypertension is an important subtype of hypertension that leads to an increased risk of cerebrovascular, cardiovascular, and kidney disease. The revised guidelines from the American College of Cardiology and American Heart Association now define resistant hypertension as blood pressure that remains above goal despite use of three maximally titrated anti-hypertensive medications including a diuretic or as a hypertensive patient who requires 4 or more agents for adequate BP control. These agents typically include a calcium-channel blocker, a renin-angiotensin system inhibitor, and a diuretic at maximal or maximally tolerated doses. As recognition of resistant hypertension increases, it is important to distinguish pseudo-resistant or apparent hypertension from true resistant hypertension. Etiologies of apparent resistant hypertension include measurement error and medication non-adherence. The prevalence of true resistant hypertension is likely much lower than reported in the literature when accounting for patients with apparent resistant hypertension. Evaluation of patients with true resistant hypertension includes screening for causes of secondary hypertension and interfering medications. Successful management of resistant hypertension includes lifestyle modification and optimization of medical therapy, often including the use of mineralocorticoid receptor antagonists. Looking ahead at developments in hypertension management, a slew of new device-based therapies are under active development. Of these, renal denervation is the closest to routine clinical application. Further study is needed before these devices can be recommended in the routine treatment of resistant hypertension.
Keywords: resistant hypertension, pseudo-resistant hypertension, apparent resistant hypertension, masked hypertension
Introduction
Hypertension is a growing global health concern. As the worldwide prevalence of hypertension increases, so too does the burden of excess disease attributable to hypertension including coronary artery and cerebrovascular disease.1 Within this category of patients is a subgroup identified as having resistant hypertension. They face a disproportionate burden of associated complications and pose distinct challenges in treatment.2 Recent efforts have sought to optimize establishing the diagnosis of true resistant hypertension, improve existing management methods, and attempt to develop novel technologies in the treatment of resistant hypertension.
Definition
Resistant hypertension is defined by the American College of Cardiology and American Heart Association as blood pressure (BP) that remains above goal despite use of three maximally titrated anti-hypertensive medications including a diuretic.2 As a corollary, it also includes those hypertensive patients who require 4 or more agents for adequate BP control. These agents typically include a calcium-channel blocker, a renin-angiotensin system inhibitor, and a diuretic at maximal or maximally tolerated doses. Apparent resistant or pseudo-resistant hypertension refers to hypertension that meets the above criteria but is the result of inadequate medication adherence or inaccurate blood pressure measurement.
Epidemiology
Estimates of the prevalence of resistant hypertension have varied widely, with reported figures ranging from 2% to 40%.1,3 Efforts to quantify the burden of resistant hypertension are hampered by variations in the definition of resistant hypertension. Additionally, simple measures of prevalence fail to account for errors in blood pressure measurement or apparent resistant hypertension as a result of medication non-adherence. Unsurprisingly, the prevalence of resistant hypertension rises when more stringent blood pressure targets are applied, such as the 2017 American College of Cardiology/American Heart Association guidelines.4
Resistant hypertension is associated with multiple adverse long-term consequences. Data from the ALLHAT trial showed that apparent resistant hypertension was associated with an adjusted hazard ratio of 1.44 for coronary artery disease, 1.57 for stroke, 1.88 for heart failure, 1.95 for end-stage kidney disease (ESKD), and 1.30 for all-cause mortality.5 Similarly, a large meta-analysis also found significant increases in the rate of resistant hypertension in patients with coronary artery disease and chronic kidney disease compared with the general population.6 Over a period of 5 years, de Beus and colleagues found that in patients with chronic kidney disease-resistant hypertension is linked to a 1.5-fold greater risk of adverse cardiovascular outcomes and 2.3-fold increase in progression to ESKD.7
Pathophysiology
Hypertension arises from dysfunction of various mechanisms which maintain blood pressure homeostasis. This includes disproportionate renal activation of the sympathetic nervous system leading to an increase in renin release from the juxtaglomerular apparatus in the kidney which increases both sympathetic and renin-angiotensin aldosterone system activation resulting in inappropriate intravascular volume retention, vasoconstriction and increased cardiac contractility resulting in an increase in blood pressure.8 Excessive dietary sodium intake plays an important role in hypertension and causes an increase in BP due to salt sensitivity particularly in black, elderly and diabetic patients. There may also be inadequate natriuresis in patients who are not particularly salt sensitive or do not have excessive sodium intake. The role of excess aldosterone is key in exacerbating hypertension particularly in patients with resistant hypertension who have been shown to have excess levels of aldosterone when compared to controls with normotension or hypertension controlled with ≤2 anti-hypertensive agents.9,10 A recent study found that elevated aldosterone levels, independent of renin levels, corresponded to worsening hypertension across all stages of hypertension severity11. These findings suggest that excess aldosterone contributes to the pathophysiology of hypertension even in patients with “essential” hypertension who do not meet the criteria for primary hyperaldosteronism. These factors can be further compounded by intrinsic renal dysfunction in the presence of chronic kidney disease.
Diagnosis
Once the initial diagnosis of resistant hypertension has been made based on the above definition, it is vital to distinguish patients who have apparent resistant hypertension. A diagnosis of resistant hypertension cannot be made without accurate measurement of blood pressure. Errors can arise both from measurement techniques and discordance between in-office and out-of-office blood pressure readings. Patients with apparent resistant hypertension must also be evaluated for medication non-adherence.
While measurement of in-office blood pressure is a ubiquitous feature of outpatient clinical medicine, accuracy is far from assured. Inadequate technique is an important source of error, but even accurately obtained in-office blood pressure may be misleading in the presence of white-coat or masked hypertension.12,13 We recommend using automated office blood pressure (AOBP) using a standardized technique with a validated device over manual auscultatory or a single oscillometric technique. AOBP has the capability to record multiple BP readings after a rest period with a single activation and provides an average of 3–5 readings (depending on how the machine is set up). It is not necessary to discard the first reading and can be performed attended or unattended.13 Ambulatory blood pressure monitoring (ABPM) over a 24-h period ideally should ideally be used to further mitigate errors and verify the diagnosis of resistant hypertension. As ABPM may not always be available or feasible, self-performed home blood pressure monitoring is another tool that can be used to compensate for the limitations of office measurements.14
Medication non-adherence is an important and underappreciated cause of apparent resistant hypertension. When medication adherence in hypertensive patients was analyzed using German prescription claims data over the course of 2 years, up to 50% of patients met criteria for non-adherence (defined as a ratio of medication doses dispensed to the dispensing period of <0.8).15 Failure to recognize medication non-adherence early in the disease course may result in unnecessary testing, complications of polypharmacy, delay inappropriate treatment, and worsen patient outcomes. Multiple studies have demonstrated that a significant fraction of patients referred for resistant hypertension are either partially or completely non-adherent. Hameed et al found that 25 of 50 (50%) of patients with apparent resistant hypertension were in fact not adherent.16 Similarly, when urinary drug metabolites were measured by Tomaszewski and colleagues, 25% of patients were at least partially non-adherent.17 Conversely, when patients with apparent resistant hypertension are placed under controlled medical therapy with direct observation, a significant fraction are able to achieve appropriate blood pressure control.18
An ideal medication regimen minimizes the number of therapies by using long-acting agents and combination therapies, uses low cost or generic medications, and tries to use agents with lower reported adverse effects. Comorbid conditions that may affect adherence such as alterations in cognitive function or mental illness should also be addressed. It is important for clinicians to always remain mindful of cultural and socioeconomic barriers that increase medication non-adherence. Physician assessment of medication non-adherence is quite poor; in at least one study less than half of patients with identifiable gaps in medication refills were identified as non-adherent by the treating physician.19 This suggests that there is ample opportunity to address medication non-adherence via the integration of electronic medical and pharmacy records, as well as data from ubiquitous-connected “smart” devices. Finally, the medication regimen should be carefully reviewed to identify any potential interfering agents that might cause or exacerbate hypertension (Table 1).
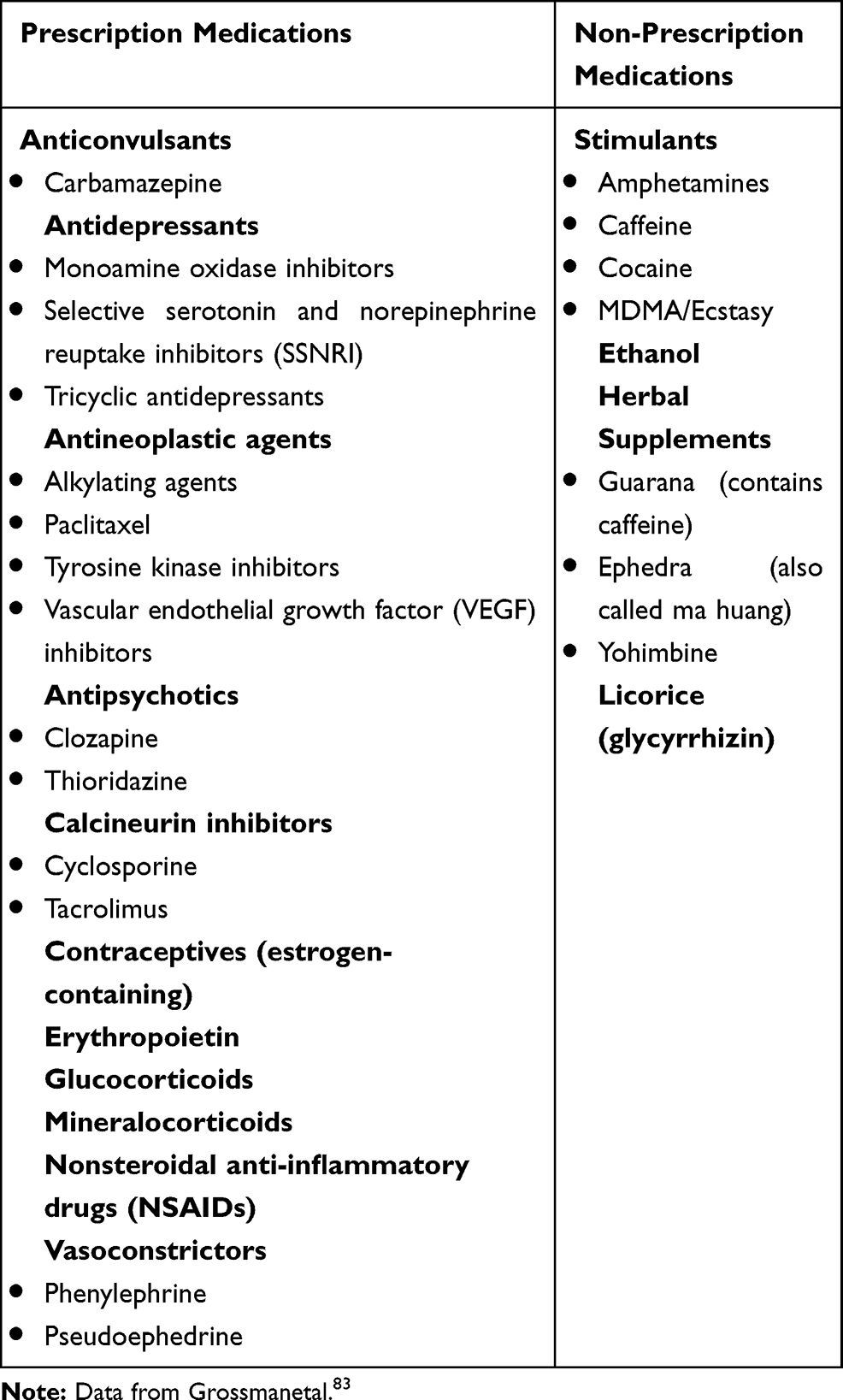 |
Table 1 Interfering Medications That Can Cause Hypertension |
Once the patient is determined to have true resistant hypertension, the next step is identification of underlying causes for uncontrolled hypertension. These may be broadly categorized as the detection of various hormonal and vascular disruptors that result in uncontrolled hypertension. The more common among these conditions include chronic kidney disease, primary hyperaldosteronism, and renovascular disease, as well as other less common conditions such as pheochromocytoma.
Chronic kidney disease (CKD) has a significant association with apparent resistant hypertension. In one large cross-sectional study, prevalence of apparent resistant hypertension ranged from 15.8% to 33.4% when estimated GFR changed from ≥60 mL/min to <45 mL/min.20 Similarly, analysis of data from the Chronic Renal Insufficiency Cohort (CRIC) study showed a prevalence of apparent resistant hypertension of 40.4%.21 While these studies are limited in their ability to distinguish apparent from true resistant hypertension, they nonetheless indicate the potential scope of the problem. Likely etiologies for the increased rate of RH in CKD patients include progressive sodium retention, up-regulation of the renin-angiotensin-aldosterone axis, sympathetic nervous system dysfunction, and increased vascular stiffness and dysfunction. However, the presence of CKD should not preclude investigation for other causes of RH.
Primary aldosteronism (PA) is the most common cause of secondary hypertension in patients with RH. Untreated PA is associated with adverse cardiovascular effects, insulin resistance, and chronic kidney disease.22 Cardiovascular effects are particularly notable: when compared with matched controls with essential hypertension, where PA patients were shown to have an increased risk of myocardial infarction (OR 6.5) and stroke (OR 4.2).23 Screening should be done using measurement of the plasma renin and aldosterone levels, with abnormal findings followed by confirmatory testing. Management of these patients centers on identifying appropriate surgical candidates (who have lateralizable disease) and treatment with mineralocorticoid-receptor antagonists in the remainder.
Obstructive sleep apnea (OSA) is also associated with uncontrolled and resistant hypertension.24 Estimates of prevalence vary widely. One case-control study comparing patients with resistant hypertension to those with controlled BP found that 71% of resistant hypertension patients had OSA compared with only 38% of controls.25 Patients undergoing evaluation should be screened for the possibility of OSA and referred as appropriate for further evaluation via polysomnography. Treatment with CPAP has been shown to reduce BP modestly by approximately 4/2 mm Hg but is more effective and has shown greater reductions in patients with resistant hypertension.26
Renal-artery stenosis (RAS) is another condition associated with resistant hypertension. It is typically due to atherosclerotic renovascular disease and less commonly due to fibromuscular dysplasia (FMD). Atherosclerotic renovascular disease is associated with older age and the presence of generalized atherosclerosis, whereas FMD is more typically seen in young and middle-aged adults and is more common in female patients. The prevalence of RAS has been shown to be as high as 24.2% in patients with resistant hypertension.27 In this study, the majority of cases were associated with peripheral vascular disease and only 3.5% of patients in whom RAS was identified were found to have FMD. Multiple recent studies have demonstrated that renal artery angioplasty and stenting do not broadly reduce the incidence of cardiovascular or renal disease.28,30 However, there are selected patients who may benefit, such as those with a solitary kidney, recurrent pulmonary edema, recurrent acute kidney injury following introduction of ACE-I or ARB, or otherwise unexplained progressive renal insufficiency.31 Remaining patients should be treated with optimal medical therapy that includes the use of ACE-I or ARBs, a statin, and aspirin.
Evaluation for otherwise unexplained resistant hypertension should also exclude the presence of neuroendocrine tumors such as pheochromocytoma, particularly when suggestive symptoms are present. Note that the absolute prevalence of these disorders is quite rare. A single-center retrospective found that of 104 adrenal lesions identified in patients referred for evaluation of secondary hypertension, only 3 (2.9%) were pheochromocytomas.32 Plasma-free metanephrine levels are the best initial screening test for pheochromocytoma.
Lifestyle Modification
Present guidelines for the management of hypertension recommend lifestyle modifications including limiting dietary sodium intake and increasing potassium intake (such as in the DASH diet), increasing physical activity, and moderating alcohol intake.33 Conversely, the same lifestyle-related risk factors are highly prevalent in patients with resistant hypertension, including obesity, low levels of physical activity, high dietary sodium intake, and excessive alcohol intake.34 There are varying degrees of evidence to support different lifestyle interventions specifically in resistant hypertension. Additionally, the correlation between factors such as dietary intake, exercise, and obesity makes treatment more challenging since there are likely common underlying determinants. The ongoing TRIUMPH trial is investigating the efficacy of integrated lifestyle modification including dietary changes, exercise, and weight reduction in patients with resistant hypertension.35
Dietary modification in hypertension has conventionally been conceived in terms of limiting sodium intake, but both dietary sodium restriction and increased potassium intake are important interventions for hypertensive patients. Typical dietary consumption of sodium in the United States is 150 mmol/day (3.5 g), far in excess of the 100 mmol/day (2.3 g) recommended in the DASH diet.36 Dietary sodium restriction in patients with resistant hypertension has been shown to have a dramatic impact on blood pressure control. Pimenta and colleagues found a 22.7 and 9.1 mm Hg reduction in systolic and diastolic blood pressure, respectively, when sodium intake was reduced from 250 mmol/day to 50 mmol/day.37 Numerous mechanisms have been proposed to explain the blood pressure-lowering effects of increased potassium intake, including promotion of natriuresis and alterations in endothelial function.38,39 The DASH diet itself recommends the consumption of plant-based foods which are often high in potassium. Multiple meta-analyses have found that increased potassium intake from both food intake and dietary supplementation reduced blood pressure in hypertensive patients with mean reductions in BP of 3.3/3 mm Hg. While the effect was most prominent in studies with high average sodium consumption (greater than 4g/day), blood pressure was still reduced across a range of average dietary sodium intakes.40,41
Lastly amongst the above dietary factors, alcohol intake has been correlated with severity of hypertension. A large study of Chinese patients found a 2.2-fold increase in hypertension in heavy drinkers (>30 drinks/week) as compared to non-drinkers.42 Conversely, a meta-analysis of alcohol intake reduction found a mean BP reduction of 3.3/2.0 mm Hg, with a consistent dose–response relationship.43 It is recommended that alcohol consumption be limited to ≤2 drinks per day in males and ≤1 drink per day in females.
Obesity is strongly associated with development of resistant hypertension, as seen in data from successive NHANES surveys where BMI ≥ 30 was independently associated with apparent treatment-resistant hypertension.44 Numerous factors having been implicated in the pathogenesis of obesity-related hypertension, including increased levels of oxidative stress leading to endothelial dysfunction and upregulation of sympathetic activity and renin-angiotensin-aldosterone systems.45,47 Obesity has been associated with increases in measured plasma and urine aldosterone levels.48 Bariatric surgery has been shown to be a successful, long-term treatment of obesity.49 Courcoulas et al found that 3 years post-surgery, 38.2% of Roux-en-Y gastric bypass and 17.4% of laparoscopic banding recipients had remission of hypertension.50 In another study by Schiavon, et al, the prevalence of resistant hypertension in recipients of bariatric surgery (Roux-en-Y Gastric Bypass) was reduced to 0% in the intervention arm compared to the control group which received only medical therapy.51 A notable strength of this study was the use of 24-h blood pressure monitoring for the primary endpoint.
Physical activity has long been thought to be beneficial in the treatment of hypertension and it is recommended that patients engage in at least 30 min of exercise most days of the week. It has been shown that in addition to aerobic exercise, isometric and resistance exercises are all beneficial in BP reduction. A large prospective cohort study by Narayan et al demonstrated that increases in cardiovascular fitness decreased mortality in patients with resistant hypertension. The difference between the most and least fit quartiles (as measured by peak exercise capacity in METs) was found to be 62%.52 Two recent meta-analyses also demonstrated that exercise therapy improved blood pressure control in patients with hypertension. Both meta-analyses included studies using aerobic and/or resistance training.53,54 Data is sparser for patients with resistant hypertension, but aerobic exercise has been demonstrated to lower BP in patients with RH.55 A summary of the different lifestyle modifications and the effects on BP reduction is shown in Table 2.
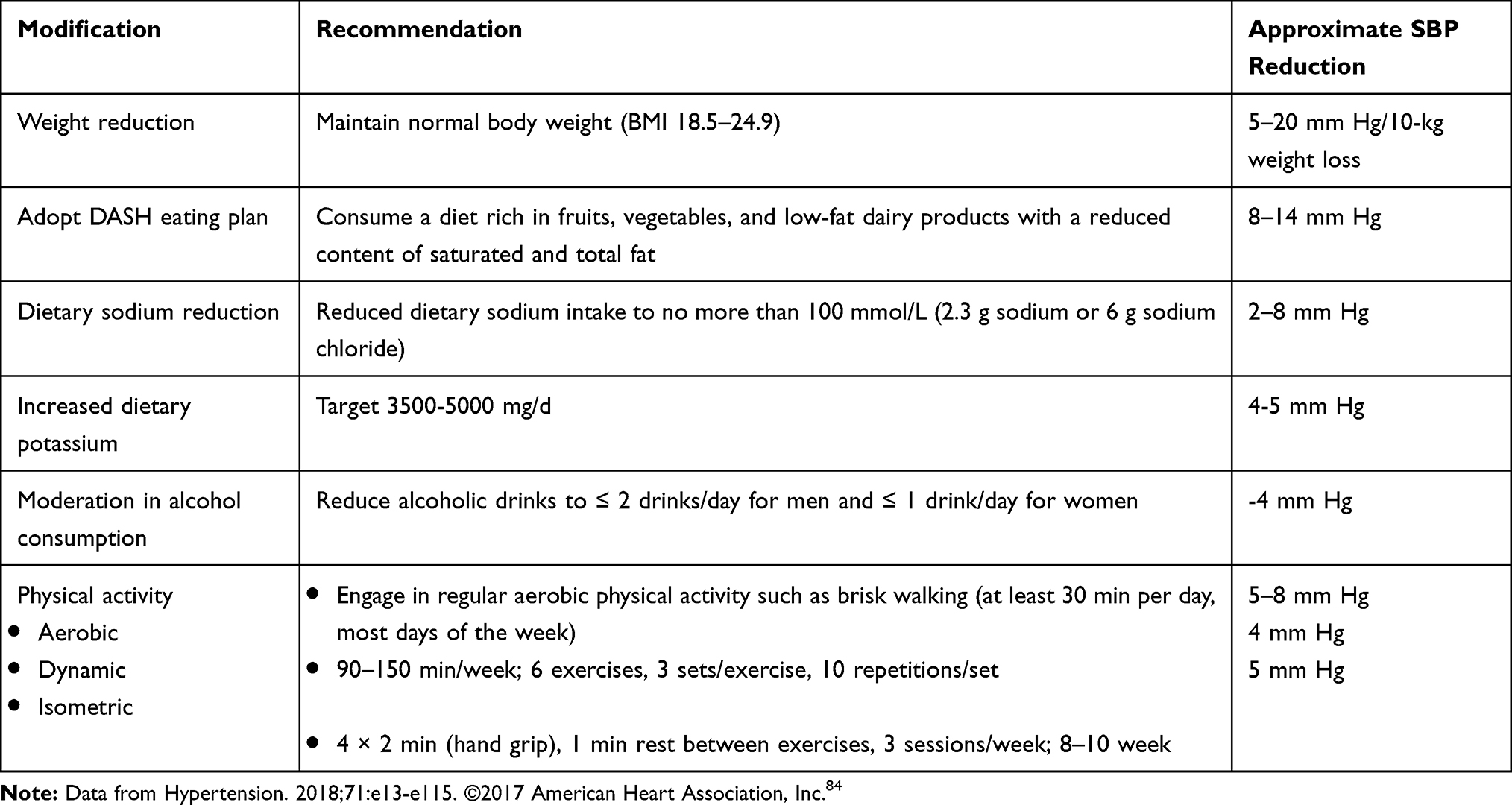 |
Table 2 Expected systolic blood pressure (SBP) reduction in hypertensive patients with lifestyle interventions |
Medical Therapies
Medical therapy for hypertension, resistant or otherwise, must balance the efficacy of treatment along with ease of adherence. As such regimens must be simplified to the degree possible while maintaining potency. Medication regimens should be simplified with once daily dosing if possible and the use of combination therapies. A diuretic should always be part of a multidrug regimen.
Appropriate therapy for these patients should include 3 agents, usually consisting of a calcium-channel blocker, a RAS system inhibitor, and a diuretic at maximally tolerated doses. Important considerations for the latter include diuretic selection and timing of administration. Of the thiazide or thiazide-like diuretics, indapamide and chlorthalidone have been shown to have more potent BP lower effects and should be preferred over hydrochlorothiazide.56 Loop diuretics are preferred agents for treatment of hypertension in advanced CKD however there is emerging data showing that thiazides are also effective at lower GFR and can be combined with loop diuretics.57 Loop diuretics with a shorter duration of action (such as furosemide) should be dosed multiple times daily or substituted for a longer-acting agent such as torsemide.58
An important component of medical therapy for resistant hypertension is the use of mineralocorticoid-receptor antagonists (MRA), and these agents should be considered when adding a 4th anti-hypertensive agent. Notably, these display efficacies even in patients who do not meet criteria for hyperaldosteronism. An analysis of data from the ASCOT study found that when used as a 4th line agent for RH, spironolactone resulted in a mean BP decline of 21.9/9.5 mm Hg.59 A recent study demonstrated that optimal medical therapy remains under-utilized with respect to both diuretics and MRA, with only 1.9% receiving the former and 5.6% the latter.4
The PATHWAY-2 study examined the use of MRA in resistant hypertension. This large, multicenter randomized control trial evaluated the use of spironolactone in patients already on a standard 3-drug regimen of a calcium-channel blocker, ACE-inhibitor/ARB, and a diuretic. Patients were randomized in rotating order to 12 weeks of spironolactone, bisoprolol, doxazosin and placebo. Spironolactone was found to be superior to all comparators, resulting in a 9mm Hg reduction in systolic blood pressure compared to placebo, and 5–6 mmHg greater reduction in SBP than bisoprolol or doxazosin. While this effect was most pronounced in patients with suppressed renin levels, it was maintained across all renin levels.60 A sub-study of PATHWAY-2 showed similar results when using amiloride, which inhibits the ENaC channel and thus the downstream effects of aldosterone on the kidney. A notable limitation of amiloride in this application is the inability to prevent adverse effects of excess aldosterone in other organs, such as cardiac fibrosis and hypertrophy.
A potential limitation in the use of MRA therapy is the development of hyperkalemia, particularly in patients with underlying CKD. The AMBER study examined the use of patiromer (a potassium binding resin) to enable use of spironolactone in patients with CKD and resistant hypertension. At the conclusion of the study, 86% of the patients in the patiromer-intervention arm were still on spironolactone, as compared to 66% of patients in the control arm. A concomitant reduction in the incidence of hyperkalemia was observed in the patiromer group.61
SGLT-2 inhibitors have not been studied in patients with resistant hypertension and have a modest reduction in BP of approximately 4/2 mm Hg but may be particularly important in resistant hypertension considering their impressive reductions in cardiovascular outcomes, heart failure, and the progression of CKD.62 A number of other novel agents are currently being evaluated in the treatment of resistant hypertension and may play a role in future BP lowering regimens. Endothelin A receptor antagonists act to cause vasodilation; members of this class are already in use in the treatment of pulmonary arterial hypertension. Vasopeptidase inhibitors decrease the generation of Angiotensin II and block the degradation of natriuretic peptides. Lastly, aminopeptidase A inhibitors act at the level of central control of the renin-angiotensin system. Further study is needed before any of these agents can be recommended for routine clinical practice.
Device-Based Therapies
Device-based therapies for hypertension have been intensively studied over the past decade and until recently results have not been consistently reproducible for widespread clinical implementation. Recognizing the above limitations in medication adherence and lifestyle modification, an ideal device-based therapy for hypertension, resistant or otherwise, would allow for durable reduction in BP following a single intervention while obviating the need for ongoing pharmacologic therapy. There are multiple approaches currently under development targeting various aspects of physiologic blood pressure regulation.
The first of these is renal denervation (RDN). The renal nerves have both afferent and efferent sympathetic innervation; the efferent fibers to the kidney arise from the sympathetic ganglia and are stimulated via the juxtaglomerular apparatus and are key regulators of the renin-angiotensin-aldosterone system as well as direct renal vascular resistance. Sensory afferent fibers regulate sympathetic outflow to the kidney and control systemic cardiovascular hemodynamics and sympathetic efferent activity. Numerous animal studies have demonstrated dramatic reduction in BP following renal denervation. Early surgical sympathectomy proved to have unacceptable side effects and was abandoned as a viable therapeutic option with the advent of modern anti-hypertensive drugs. Other techniques such as nerve ablation using ethanol have been used in pilot studies.63 However, newer technologies intended for broader human applications have focussed on the use catheter-based ablation of the renal nerves.
An early surge of interest in catheter-based RDN was typified by the proof-of-concept Symplicity HTN-1 study, an open-label trial using catheter-based radiofrequency ablation of the sympathetic plexus via the renal arteries. This study showed an excellent response rate with average reductions in systolic and diastolic BP of 32 mm Hg and 14.4 mm Hg, respectively.64 The follow-on randomized control trial SYMPLICITY HTN-2 showed similarly dramatic reductions in systolic and diastolic BP of 33 mm Hg and 14 mm Hg.65
This early progress came to a standstill with the negative results of the SYMPLICITY HTN-3 Trial.66 This RCT used the same catheter as the previous studies in the series but introduced a sham procedure for the control group. The results were statistically significant in favor of greater BP reduction in the intervention arm but did not meet pre-specified endpoints for efficacy. In addition, the placebo arm had a substantial reduction in BP. This unexpected outcome resulted in an outpouring of analysis in an attempt to explain the discrepancy given the extremely promising results of earlier studies. This included the confounding effect of anti-hypertensive medication changes, as well as technical limitations in the catheter technology and the experience of the proceduralists, which may have limited the ability to achieve satisfactory nerve ablation.
However, the field is now undergoing resurgence with multiple recent publications. The parallel SPYRAL HTN-OFF MED and SPYRAL HTN-ON MED trials used an updated radiofrequency ablation technology intended to provide more comprehensive sympathetic plexus ablation and included ablation of sympathetic nerves in the main renal artery as well as branch arteries. From the outset, they were designed with the limitations of SYMPLICITY HTN-3 in mind.67 Both trials were conducted in randomized fashion with sham procedures for the controls. The OFF MED trial again demonstrated reduction in both 24-h ABPM and office BP in patients not on medical therapy for hypertension, thus confirming the efficacy of RDN in reducing systemic blood pressure.68,69 The ON MED trial examined the efficacy of RDN in patients already on pharmacologic anti-hypertensive therapy.70 Stringent measures were taken to identify medication adherence, including the use of HPLC-MS screening following enrollment. In addition, medication changes were prohibited unless patients met pre-specified “escape” criteria. A statistically significant reduction in office and 24-h ambulatory blood pressure was seen in the intervention arm.
Similar results were seen in the RADIANCE-HTN SOLO trial which utilized ultrasound ablation.71 Like the SPYRAL HTN studies, the DENERHTN trial also standardized anti-hypertensive therapy in the control and intervention groups before and after randomization. The intervention group was found to have a 5.9mm Hg larger reduction in daytime ambulatory systolic blood pressure.72 Finally, the RADIOSOUND-HTN study evaluated both radiofrequency and ultrasound techniques head-to-head against sham controls, and demonstrated improvement in hypertension across all intervention groups and superior mean BP reduction for the ultrasound-based approach. Collectively, these studies have done much to rehabilitate RDN and permit further research.
There remain many unanswered questions about the viability of RDN. Notably, in all of the above trials the magnitude of mean BP reduction was smaller than in previous animal and human studies, with results on the order of < 10mm Hg. Speculated reasons for this include less than total renal nerve ablation, albeit with the caveat that all of the above trials used 3rd generation ablative technology. Further variability may have resulted from an inability to control for varying levels of medication adherence.
There is currently no reliable method to detect if adequate nerve ablation was achieved in the clinical setting and this effects responsiveness to the procedure and is an area of active research. Multiple methods for verification of successful RDN are under active investigation include direct neural stimulation, reflex elicitation, and passive monitoring.73 Additionally, there has been speculation that various renal nerves may have either inhibitory or stimulatory effects on renal sympathetic activation; only ablation of the latter would lead to improvement in hypertension and might further explain variability in BP response to RDN. Direct nerve stimulation during RDN offers a method of discrimination between inhibitory and stimulatory fibers and has shown initial promise in animal models as well as small human pilot studies.74,75
The longevity of the blood pressure reduction remains unknown although the Global SYMPLICITY registry has demonstrated persistent decreases in office and ambulatory BP in patients followed for up to 3 years post-RDN.76 Animal models have shown regrowth of both afferent and efferent sympathetic fibers however this has not been demonstrated in humans after undergoing RDN procedures.77
Patient characteristics are also crucial to understanding response rates, and studies have found a range of response, from “extreme-responders” to non-responders. This may be explained by the degree to which sympathetic activation is a major driver of hypertension in the individual patient. Persu and colleagues identified an association between lower eGFR and non-response, while women were more likely to be extreme responders.78 Additionally, non-response may arise from inaccurate measurement or confounders such as an unidentified secondary cause of hypertension.
These challenges speak to the ongoing need for further study in order to improve patient selection for these promising technologies, particularly with respect to patients with resistant hypertension in whom these techniques would be most beneficial.
The ROX device is a catheter-deployed arteriovenous shunt system intended to induce a drop in systemic vascular resistance and thereby lower systemic BP. The ROX CONTROL HTN examined the use of a central iliac arteriovenous anastomosis in patients with hypertension. The intervention arm demonstrated 26.9 and 13.5 mm Hg reductions in mean systolic BP measured by ABPM and office BP, respectively.79 However, 29% of patients developed venous stenosis, with further intervention required to ameliorate this. The company has since shut down and no trials are currently being conducted so there are no long-term data available regarding the durability of response.
Lastly, there remains interest in the prospect of electrical stimulation of the carotid baroreceptors. Experimental data from over 50 years ago have demonstrated the possibility of lowering blood pressure by stimulating the carotid baroreceptors via implantable electrodes. The Rheos and Barostim implantable baroreceptor stimulators have completed pilot studies with positive results.80,81 Finally, the MobiusHD device takes a different approach, aiming to amplify carotid stretch signals. An initial pilot study showed positive results, leading to an open-label study that was recently closed due to low recruitment.82
The use of device-based therapy for resistant hypertension is under active development but only catheter-based RDN and ultrasound ablation seem to have the potential to become incorporated into clinical care due to low patient acceptability and unacceptable side effects of the other devices. These device-based therapies do offer the tantalizing prospect of a paradigm shift in the treatment of particularly resistant hypertension but optimal patient selection is still unclear.
Summary
Resistant hypertension is increasingly recognized as an important area of study and intervention, particularly given the adverse long-term consequences if not appropriately treated. It is important to distinguish apparent resistant hypertension from true resistant hypertension due to incorrect BP measurement or from medication non-adherence. Successful treatment encompasses integrating lifestyle modification, improving medication adherence, and optimizing the use of diuretics and mineralocorticoid-receptor antagonists. Device-based therapies are an emerging category that hold potential promise for the future treatment of resistant hypertension, but their role in the treatment of resistant hypertension is still being defined and they are not currently recommended in routine clinical care.
Disclosure
The authors report no conflicts of interest in this work.
References
1. Daugherty SL, Powers JD, Magid DJ, et al. Incidence and prognosis of resistant hypertension in hypertensive patients. Circulation. 2012;125(13):1635–1642. doi:10.1161/CIRCULATIONAHA.111.068064
2. Carey RM, Calhoun DA, Bakris GL, et al. Resistant hypertension: detection, evaluation, and management: a scientific statement from the American heart association. Hypertension. 2018;72(5):e53–e90. doi:10.1161/HYP.0000000000000084
3. Achelrod D, Wenzel U, Frey S. Systematic review and meta-analysis of the prevalence of resistant hypertension in treated hypertensive populations. Am J Hypertens. 2015;28(3):355–361. doi:10.1093/ajh/hpu151
4. An J, Sim JJ, Calhoun DA, et al. Apparent treatment-resistant hypertension: characteristics and prevalence in a real-world environment of an integrated health system. J Hypertens. 9000:Publish Ahead of Print.
5. Muntner P, Davis BR, Cushman WC, et al. Treatment-resistant hypertension and the incidence of cardiovascular disease and end-stage renal disease: results from the antihypertensive and lipid-lowering treatment to prevent heart attack trial (ALLHAT). Hypertension. 2014;64(5):1012–1021. doi:10.1161/HYPERTENSIONAHA.114.03850
6. Noubiap JJ, Nansseu JR, Nyaga UF, Sime PS, Francis I, Bigna JJ. Global prevalence of resistant hypertension: a meta-analysis of data from 3.2 million patients. Heart. 2019;105(2):98–105. doi:10.1136/heartjnl-2018-313599
7. Beus E, Bots ML, ADv Z, Wetzels JFM, Blankestijn PJ. Prevalence of apparent therapy-resistant hypertension and its effect on outcome in patients with chronic kidney disease. Hypertension. 2015;66(5):998–1005.
8. Grassi G, Mark A, Esler M. The sympathetic nervous system alterations in human hypertension. Circ Res. 2015;116(6):976–990. doi:10.1161/CIRCRESAHA.116.303604.
9. Vasavada N, Agarwal R. Role of excess volume in the pathophysiology of hypertension in chronic kidney disease. Kidney Int. 2003;64(5):1772–1779. doi:10.1046/j.1523-1755.2003.00273.x
10. Gaddam KK, Nishizaka MK, Pratt-Ubunama M, et al. Characterization of resistant hypertension: association between resistant hypertension, aldosterone, and persistent intravascular volume expansion. INTEMED. 2008;168(11):1159–1164.
11. Jenifer M, Brown MD, Mohammed Siddiqui MD, et al. The unrecognized prevalence of primary aldosteronism. Ann Intern Med. 2020.
12. Rakotz MK, Townsend RR, Yang J, et al. Medical students and measuring blood pressure: results from the American medical association blood pressure check challenge. J Clin Hypertension. 2017;19(6):614–619. doi:10.1111/jch.13018
13. Muntner P, Shimbo D, Carey R, et al. Measurement of blood pressure in humans: a scientific statement from the American heart association. Hypertension. 2019;73(5):e35–e66. doi:10.1161/HYP.0000000000000087
14. Oikawa T, Obara T, Ohkubo T, et al. Characteristics of resistant hypertension determined by self-measured blood pressure at home and office blood pressure measurements: the J-HOME study. J Hypertens. 2006;24(9):1737–1743. doi:10.1097/01.hjh.0000242397.53214.27
15. Schulz M, Krueger K, Schuessel K, et al. Medication adherence and persistence according to different antihypertensive drug classes: a retrospective cohort study of 255,500 patients. Int J Cardiol. 2016;220:668–676. doi:10.1016/j.ijcard.2016.06.263
16. Hameed MA, Tebbit L, Jacques N, Thomas M, Dasgupta I. Non-adherence to antihypertensive medication is very common among resistant hypertensives: results of a directly observed therapy clinic. J Hum Hypertens. 2016;30(2):83–89. doi:10.1038/jhh.2015.38
17. Tomaszewski M, White C, Patel P, et al. High rates of non-adherence to antihypertensive treatment revealed by high-performance liquid chromatography-tandem mass spectrometry (HP LC-MS/MS) urine analysis. Heart. 2014;100(11):855–861. doi:10.1136/heartjnl-2013-305063
18. Bunker J, Chang CL, Chapman N, et al. True resistant hypertension following observed drug ingestion: a systematic evaluation. J Clin Hypertens (Greenwich). 2017;19(3):250–255. doi:10.1111/jch.12896
19. Meddings J, Kerr EA, Heisler M, Hofer TP. Physician assessments of medication adherence and decisions to intensify medications for patients with uncontrolled blood pressure: still no better than a coin toss. BMC Health Serv Res. 2012;12(1):270. doi:10.1186/1472-6963-12-270
20. Tanner RM, Calhoun DA, Bell EK, et al. Prevalence of apparent treatment-resistant hypertension among individuals with CKD. Clin J Am Soc Nephrol. 2013;8(9):1583–1590. doi:10.2215/CJN.00550113
21. Thomas G, Xie D, Chen HY, et al. Prevalence and prognostic significance of apparent treatment resistant hypertension in chronic kidney disease: report from the chronic renal insufficiency cohort study. Hypertension. 2016;67(2):387–396. doi:10.1161/HYPERTENSIONAHA.115.06487
22. Funder JW, Carey RM, Mantero F, et al. The management of primary aldosteronism: case detection, diagnosis, and treatment: an endocrine society clinical practice guideline. J Clin Endocrinol Metab. 2016;101(5):1889–1916. doi:10.1210/jc.2015-4061
23. Milliez P, Girerd X, Plouin P, Blacher J, Safar ME, Mourad J. Evidence for an increased rate of cardiovascular events in patients with primary aldosteronism. J Am Coll Cardiol. 2005;45(8):1243–1248. doi:10.1016/j.jacc.2005.01.015
24. Pratt-Ubunama M, Nishizaka MK, Boedefeld RL, Cofield SS, Harding SM, Calhoun DA. Plasma aldosterone is related to severity of obstructive sleep apnea in subjects with resistant hypertension. Chest. 2007;131(2):453–459. doi:10.1378/chest.06-1442
25. Gonçalves SC, Martinez D, Gus M, et al. Obstructive sleep apnea and resistant hypertension: a case-control study. Chest. 2007;132(6):1858. doi:10.1378/chest.07-1170
26. Iftikhar I, Valentine C, Bittencourt L, et al. Effects of continuous positive airway pressure on blood pressure in patients with resistant hypertension and obstructive sleep apnea: a meta-analysis. J Hypertens. 2014;32(12):2341–2350. doi:10.1097/HJH.0000000000000372
27. Benjamin MM, Fazel P, Filardo G, Choi JW, Stoler RC. Prevalence of and risk factors of renal artery stenosis in patients with resistant hypertension. Am J Cardiol. 2014;113(4):687–690. doi:10.1016/j.amjcard.2013.10.046
28. Cooper CJ, Murphy TP, Cutlip DE, et al. Stenting and medical therapy for atherosclerotic renal-artery stenosis. N Engl J Med. 2014;370(1):13–22. doi:10.1056/NEJMoa1310753
29. Bax L, Woittiez AJ, Kouwenberg HJ, et al. Stent placement in patients with atherosclerotic renal artery stenosis and impaired renal function: a randomized trial. Ann Intern Med. 2009;150(12):840–841. doi:10.7326/0003-4819-150-12-200906160-00119
30. Investigators A, Wheatley K, Ives N, et al. Revascularization versus medical therapy for renal-artery stenosis. N Engl J Med. 2009;361(20):1953–1962.
31. Chatziioannou A, Mourikis D, Agroyannis B, et al. Renal artery stenting for renal insufficiency in solitary kidney in 26 patients. Eur J Vasc Endovasc Surg. 2002;23(1):49–54. doi:10.1053/ejvs.2001.1535
32. Aoe M, Okada A, Usui T, Manaka K, Nangaku M, Makita N. Comparison between the clinical characteristics of patients with adrenal incidentalomas and those with hypertension-associated adrenal tumors in a single center in Japan. Endocr J. 2020. doi:10.1507/endocrj.EJ19-0262
33. Carey RM, Whelton PK. Prevention, detection, evaluation, and management of high blood pressure in adults: synopsis of the 2017 American college of cardiology/american heart association hypertension guideline. Ann Intern Med. 2018;168(5):351–358. doi:10.7326/M17-3203
34. Shimbo D, Levitan E, Booth J, et al. The contributions of unhealthy lifestyle factors to apparent resistant hypertension: findings from the reasons for geographic and racial differences in stroke (REGARDS) study. J Hypertens. 2013;31(2):370–376. doi:10.1097/HJH.0b013e32835b6be7
35. Blumenthal JA, Sherwood A, Smith PJ, et al. Lifestyle modification for resistant hypertension: the TRIUMPH randomized clinical trial. Am Heart J. 2015;170(5):986–994.e5. doi:10.1016/j.ahj.2015.08.006
36. Sacks FM, Svetkey LP, Vollmer WM, et al. Effects on blood pressure of reduced dietary sodium and the dietary approaches to stop hypertension (DASH) diet. DASH-sodium collaborative research group. N Engl J Med. 2001;344(1):3. doi:10.1056/NEJM200101043440101
37. Eduardo P, Gaddam KK, Suzanne O, et al. Effects of dietary sodium reduction on blood pressure in subjects with resistant hypertension. Hypertension. 2009;54(3):475–481. doi:10.1161/HYPERTENSIONAHA.109.131235
38. He F, Marciniak M, Carney C, et al. Effects of potassium chloride and potassium bicarbonate on endothelial function, cardiovascular risk factors, and bone turnover in mild hypertensives. Hypertension. 2010;55(3):681–688. doi:10.1161/HYPERTENSIONAHA.109.147488
39. Smith SR, Klotman PE, Svetkey LP. Potassium chloride lowers blood pressure and causes natriuresis in older patients with hypertension. J Am Soc Nephrol. 1992;2(8):1302.
40. Whelton PK, He J, Cutler JA, et al. Effects of oral potassium on blood pressure: meta-analysis of randomized controlled clinical trials. JAMA. 1997;277(20):1624–1632. doi:10.1001/jama.1997.03540440058033
41. Aburto NJ, Hanson S, Gutierrez H, Hooper L, Elliott P, Cappuccio FP. Effect of increased potassium intake on cardiovascular risk factors and disease: systematic review and meta-analyses. BMJ. 2013;346(7903):14.
42. Wildman R, Gu D, Muntner P, et al. Alcohol intake and hypertension subtypes in Chinese men. J Hypertens. 2005;23(4):737–743. doi:10.1097/01.hjh.0000163141.82212.5f
43. Xin X, He J, Frontini MG, Ogden LG, Motsamai OI, Whelton PK. Effects of alcohol reduction on blood pressure: a meta-analysis of randomized controlled trials. Hypertension. 2001;38(5):1112–1117. doi:10.1161/hy1101.093424
44. Egan BM, Zhao Y, Axon RN, Brzezinski WA, Ferdinand KC. Uncontrolled and apparent treatment resistant hypertension in the united states, 1988 to 2008. Circulation. 2011;124(9):1046–1058. doi:10.1161/CIRCULATIONAHA.111.030189
45. Lohmeier T, Iliescu R. The sympathetic nervous system in obesity hypertension. Curr Hypertens Rep. 2013;15(4):409–416. doi:10.1007/s11906-013-0356-1
46. Huby A, Antonova G, Groenendyk J, et al. Adipocyte-derived hormone leptin is a direct regulator of aldosterone secretion, which promotes endothelial dysfunction and cardiac fibrosis. Circulation. 2015;132(22):2134–2145. doi:10.1161/CIRCULATIONAHA.115.018226
47. Furukawa S, Fujita T, Shimabukuro M, et al. Increased oxidative stress in obesity and its impact on metabolic syndrome. J Clin Invest. 2004;114(12):1752–1761. doi:10.1172/JCI21625
48. Kawarazaki W, Fujita T. The role of aldosterone in obesity-related hypertension. Am J Hypertens. 2016;29(4):415–423. doi:10.1093/ajh/hpw003
49. Chang S, Stoll CRT, Song J, Varela JE, Eagon CJ, Colditz GA. The effectiveness and risks of bariatric surgery: an updated systematic review and meta-analysis, 2003-2012. JAMA Surg. 2014;149(3):275–287. doi:10.1001/jamasurg.2013.3654
50. Courcoulas AP, Christian NJ, Belle SH, et al. Weight change and health outcomes at 3 years after bariatric surgery among individuals with severe obesity. JAMA. 2013;310(22):2416–2425. doi:10.1001/jama.2013.280928
51. Schiavon CA, Ikeoka D, Santucci EV, et al. Effects of bariatric surgery versus medical therapy on the 24-hour ambulatory blood pressure and the prevalence of resistant hypertension. Hypertension. 2019;73(3):571–577. doi:10.1161/HYPERTENSIONAHA.118.12290
52. Narayan P, Doumas M, Kumar A, et al. Impact of cardiorespiratory fitness on mortality in black male veterans with resistant systemic hypertension. Am J Cardiol. 2017;120(9):1568–1571. doi:10.1016/j.amjcard.2017.07.055
53. Naci H, Salcher-Konrad M, Dias S, et al. How does exercise treatment compare with antihypertensive medications? A network meta-analysis of 391 randomised controlled trials assessing exercise and medication effects on systolic blood pressure. Br J Sports Med. 2019;53(14):859–869. doi:10.1136/bjsports-2018-099921
54. Noone C, Leahy J, Morrissey EC, et al. Comparative efficacy of exercise and anti-hypertensive pharmacological interventions in reducing blood pressure in people with hypertension: a network meta-analysis. Eur J Prev Cardiol. 2020;27(3):247–255. doi:10.1177/2047487319879786
55. Dimeo F, Pagonas N, Seibert F, Arndt R, Zidek W, Westhoff TH. Aerobic exercise reduces blood pressure in resistant hypertension. Hypertension. 2012;60(3):653–658. doi:10.1161/HYPERTENSIONAHA.112.197780
56. Roush GC, Ernst ME, Kostis JB, Tandon S, Sica DA. Head-to-head comparisons of hydrochlorothiazide with indapamide and chlorthalidone: antihypertensive and metabolic effects. Hypertension. 2015;65(5):1041–1046. doi:10.1161/HYPERTENSIONAHA.114.05021
57. Agarwal R, Sinha AD, Pappas MK, Ammous F. Chlorthalidone for poorly controlled hypertension in chronic kidney disease: an interventional pilot study. Am J Nephrol. 2014;39(2):171–182. doi:10.1159/000358603
58. Malha L, Mann S. Loop diuretics in the treatment of hypertension. Curr Hypertens Rep. 2016;18(4):1–10. doi:10.1007/s11906-016-0636-7
59. Chapman N, Dobson J, Wilson S, et al. Effect of spironolactone on blood pressure in subjects with resistant hypertension. Hypertension. 2007;49(4):839–845. doi:10.1161/01.HYP.0000259805.18468.8c
60. Williams B, MacDonald TM, Morant S, et al. Spironolactone versus placebo, bisoprolol, and doxazosin to determine the optimal treatment for drug-resistant hypertension (PATHWAY-2): a randomised, double-blind, crossover trial. The Lancet. 2015;386(10008):2059–2068. doi:10.1016/S0140-6736(15)00257-3
61. Agarwal R, Rossignol P, Romero A, et al. Patiromer versus placebo to enable spironolactone use in patients with resistant hypertension and chronic kidney disease (AMBER): a Phase 2, randomised, double-blind, placebo-controlled trial. Lancet. 2019;394(10208):1540–1550. doi:10.1016/S0140-6736(19)32135-X
62. Maliha G, AB, Townsend RR. SGLT2 inhibitors: their potential reduction in blood pressure. J Am Soc Hypertension. 2015;9(1):48–53. doi:10.1016/j.jash.2014.11.001
63. Nanni GS, Hawkins IF, Orak JK. Control of hypertension by ethanol renal ablation. Radiology. 1983;148(1):51–54. doi:10.1148/radiology.148.1.6856864
64. Krum H, Schlaich MP, Sobotka PA, et al. Percutaneous renal denervation in patients with treatment-resistant hypertension: final 3-year report of the symplicity HTN-1 study. Lancet. 2014;383(9917):622–629. doi:10.1016/S0140-6736(13)62192-3
65. Esler MD, Böhm M, Sievert H, et al. Catheter-based renal denervation for treatment of patients with treatment-resistant hypertension: 36 month results from the SYMPLICITY HTN-2 randomized clinical trial. Eur Heart J. 2014;35(26):1752–1759. doi:10.1093/eurheartj/ehu209
66. Bhatt DL, Kandzari DE, O’Neill WW, et al. A controlled trial of renal denervation for resistant hypertension. N Engl J Med. 2014;370(15):1393–1401. doi:10.1056/NEJMoa1402670
67. Kandzari DE, Kario K, Mahfoud F, et al. The SPYRAL HTN global clinical trial program: rationale and design for studies of renal denervation in the absence (SPYRAL HTN OFF-MED) and presence (SPYRAL HTN ON-MED) of antihypertensive medications. Am Heart J. 2015;171(1):82–91. doi:10.1016/j.ahj.2015.08.021
68. Townsend RR, Mahfoud F, Kandzari DE, et al. Catheter-based renal denervation in patients with uncontrolled hypertension in the absence of antihypertensive medications (SPYRAL HTN-OFF MED): a randomised, sham-controlled, proof-of-concept trial. The Lancet. 2017;390(10108):2160–2170. doi:10.1016/S0140-6736(17)32281-X
69. Böhm M, Kario K, Kandzari DE, et al. Efficacy of catheter-based renal denervation in the absence of antihypertensive medications (SPYRAL HTN-OFF MED pivotal): a multicentre, randomised, sham-controlled trial. The Lancet. 2020;395(10234):1444–1451. doi:10.1016/S0140-6736(20)30554-7
70. Kandzari DE, Böhm M, Mahfoud F, et al. Effect of renal denervation on blood pressure in the presence of antihypertensive drugs: 6-month efficacy and safety results from the SPYRAL HTN-ON MED proof-of-concept randomised trial. The Lancet. 2018;391(10137):2346–2355. doi:10.1016/S0140-6736(18)30951-6
71. Azizi M, Schmieder RE, Mahfoud F, et al. RADIANCE-HTN SOLO: a multicenter, randomized, sham-controlled study of renal denervation in patients with uncontrolled hypertension in the absence of antihypertensive medications. J Hypertens. 2018;36 Suppl 1 - ESH 2018 Abstract Book(Supplement 1):e238. doi:10.1097/01.hjh.0000539670.57475.6c
72. Azizi M, Sapoval M, Gosse P, et al. Optimum and stepped care standardised antihypertensive treatment with or without renal denervation for resistant hypertension (DENERHTN): a multicentre, open-label, randomised controlled trial. Lancet. 2015;385(9981):1957–1965. doi:10.1016/S0140-6736(14)61942-5
73. Kiuchi MG, Esler MD, Fink GD, et al. Renal denervation update from the International sympathetic Nervous System summit: JACC state-of-the-art review. J Am Coll Cardiol. 2019;73(23):3006–3017. doi:10.1016/j.jacc.2019.04.015
74. Tsioufis KP, Feyz L, Dimitriadis K, et al. Safety and performance of diagnostic electrical mapping of renal nerves in hypertensive patients. Euro Intervention. 2018;14(12):e1334. doi:10.4244/EIJ-D-18-00536
75. Lu J, Wang Z, Zhou T, et al. Selective proximal renal denervation guided by autonomic responses evoked via high-frequency stimulation in a preclinical canine model. Circ Cardiovasc Interv. 2015;8:6.
76. Mahfoud F, Böhm M, Schmieder R, et al. Effects of renal denervation on kidney function and long-term outcomes: 3-year follow-up from the global SYMPLICITY registry. Eur Heart J. 2019;40(42):3474–3482. doi:10.1093/eurheartj/ehz118
77. Booth L, Nishi E, Yao S, et al. Reinnervation of renal afferent and efferent nerves at 5.5 and 11 months after catheter-based radiofrequency renal denervation in sheep. Hypertension. 2015;65(2):393–400. doi:10.1161/HYPERTENSIONAHA.114.04176
78. Persu A, Azizi M, Jin Y, et al. Hyperresponders vs. nonresponder patients after renal denervation: do they differ? J Hypertens. 2014;32(12):2422–2427. doi:10.1097/HJH.0000000000000347
79. Lobo MD, Sobotka PA, Stanton A, et al. Central arteriovenous anastomosis for the treatment of patients with uncontrolled hypertension (the ROX CONTROL HTN study): a randomised controlled trial. The Lancet. 2015;385(9978):1634–1641. doi:10.1016/S0140-6736(14)62053-5
80. Bakris GL, Nadim MK, Haller H, et al. Baroreflex activation therapy provides durable benefit in patients with resistant hypertension: results of long-term follow-up in the Rheos Pivotal Trial. J Am Soc Hypertension. 2012;6(2):152–158. doi:10.1016/j.jash.2012.01.003
81. Lohmeier T, Hall J. Device-based neuromodulation for resistant hypertension therapy: too early for prime time? Circ Res. 2019;124(7):1071–1093. doi:10.1161/CIRCRESAHA.118.313221
82. Spiering W, Van Der Heyden J, Kroon AA, et al. [Op.8d.01] controlling and lowering blood pressure with the MobiusHD device: first-in-man interim results (calm-fim study). J Hypertens. 2016;34 Suppl 2 - ESH 2016 Abstract Book:e105. doi:10.1097/01.hjh.0000491608.58838.2e
83. Grossman A, Messerli FH, Grossman E. Drug induced hypertension – an unappreciated cause of secondary hypertension. Eur J Pharmacol. 2015;763:15–22. doi:10.1016/j.ejphar.2015.06.027
84. Whelton PK, Carey RM, Aronow WS, et al. 2017 ACC/AHA/AAPA/ABC/ACPM/AGS/APhA/ASH/ASPC/NMA/PCNA guideline for the prevention, detection, evaluation, and management of high blood pressure in adults: a report of the American college of cardiology/american heart association task force on clinical practice guidelines. Hypertension. 2018;71(6):e13–e115.
 © 2020 The Author(s). This work is published and licensed by Dove Medical Press Limited. The
full terms of this license are available at https://www.dovepress.com/terms
and incorporate the Creative Commons Attribution
- Non Commercial (unported, 3.0) License.
By accessing the work you hereby accept the Terms. Non-commercial uses of the work are permitted
without any further permission from Dove Medical Press Limited, provided the work is properly
attributed. For permission for commercial use of this work, please see paragraphs 4.2 and 5 of our Terms.
© 2020 The Author(s). This work is published and licensed by Dove Medical Press Limited. The
full terms of this license are available at https://www.dovepress.com/terms
and incorporate the Creative Commons Attribution
- Non Commercial (unported, 3.0) License.
By accessing the work you hereby accept the Terms. Non-commercial uses of the work are permitted
without any further permission from Dove Medical Press Limited, provided the work is properly
attributed. For permission for commercial use of this work, please see paragraphs 4.2 and 5 of our Terms.