Back to Journals » Psychology Research and Behavior Management » Volume 12
Resilience and recovery style: a retrospective study on associations among personal resources, symptoms, neurocognition, quality of life and psychosocial functioning in psychotic patients
Authors Zizolfi D, Poloni N ![]() , Caselli I, Ielmini M, Lucca G
, Caselli I, Ielmini M, Lucca G ![]() , Diurni M, Cavallini G
, Diurni M, Cavallini G ![]() , Callegari C
, Callegari C ![]()
Received 15 February 2019
Accepted for publication 17 April 2019
Published 29 May 2019 Volume 2019:12 Pages 385—395
DOI https://doi.org/10.2147/PRBM.S205424
Checked for plagiarism Yes
Review by Single anonymous peer review
Peer reviewer comments 2
Editor who approved publication: Dr Igor Elman
Daniele Zizolfi, Nicola Poloni, Ivano Caselli, Marta Ielmini, Giulia Lucca, Marcello Diurni, Greta Cavallini, Camilla Callegari
Department of Medicine and Surgery, Psychiatry, University of Insubria, Varese, VA 21100, Italy
Background: Personal resources have been identified as important factors in predicting patient healing or symptoms control in schizophrenia. This observational retrospective study aims to explore the influence of resilience and recovery style on the modalities of clinical presentation of the disease, as well as individual functioning and quality of life.
Methods: Participants were patients affected by schizophrenia spectrum disorders assessed at different mental health facilities. The rating scales considered are the following: Resilience Scale 10-items (RS); Recovery Style Questionnaire (RSQ); Montreal Cognitive Assessment (MoCA); Schizophrenia Quality of Life Scale (SQLS); Life Skills Profile (LSP); Positive and Negative Syndrome Scale (PANSS).
Results: Forty-four patients fulfilled the inclusion criteria. The mean age was 46 years; the average length of the history of the disease at recruitment was 23 years with an average age at first episode of psychosis (FEP) of 23 years. General psychopathology, neurocognition, and integration recovery style can predict psychosocial functioning and explain ∼54% of the LSP variance; RS total score and PANSS general psychopathology score can predict and explain ∼29% of the LSP variance. A negative association between PANSS general psychopathology and LSP total score supports the need to reduce first the symptomatology, and then successfully apply other types of interventions. A strong positive association between neurocognition and life functioning was detected, showing that deficits in neurocognition have proved to be important predictors of the functional outcome. Integration was also proven to be significantly associated with a good functional outcome. Psychotic symptoms turn out to be a negative predictive factor, whereas resilience can be hypothesized as a protective factor.
Conclusions: Resilience and recovery style “integration” can be considered as two complementary predictive resources for a good outcome; this result supports the need to set up personalized treatments, based on the characteristics of the patients.
Keywords: mental health recovery, psychological resilience, schizophrenia, cognition, life quality, community functioning
Introduction
In recent years, the stress-vulnerability model has been increasingly used to understand the development and the course of schizophrenia in the context of psychotic disorder treatment. According to this theory, progression of mental illness symptoms would proceed by an interaction between both biological and environmental factors, such as stressful life events, work difficulties, family, social and relational complications.1–3 In light of this concept, an integrative approach which includes pharmacological, psychological and socio-educational treatments is becoming increasingly shared as reference model in the treatment of mental disorders, such as schizophrenia, instead of only pharmacological approaches.4 Several studies published in professional literature have shown that an integrative approach in the treatment of schizophrenia leads to an improvement in the course and outcome of the illness.5,6 Schizophrenia is a mental illness with a huge health and social impact, determining a significant cognitive impairment, and a worsening in psychosocial functioning of people who suffer from it. The improvement of symptomatology due to psychopharmacological therapy, especially second-generation antipsychotics, partially guarantees a better quality of life, and a greater psychosocial functioning in people affected by psychosis;7–10 psychological, psychosocial, and rehabilitative treatments are further elements of an integrated program aimed to achieve functional recovery and social reintegration.11,12 Thus, to identify protective factors against relapses and to study elements promoting symptom remission is one of the goals in the study of schizophrenia treatment. The constructs of resilience and recovery style, in this context, assume significant relevance.13–17 Resilience is the psychological competence to deal with and go beyond traumatic or stressful events, resulting in being positively changed and strengthened. In other words, resilience is the ability to repair oneself after damage, to cope, to resist something, but also to build and succeed in a positive reorganizing life, despite difficult situations.18–22 Resilient individuals have the proficiency to rebuild the relations within their environment, enhancing themselves.23 Literature has highlighted that there are internal protective factors of resilience such as emotional stability, autonomy, adaptability and life planning, and organization skills,33,34 whereas the existence of a valid family and friendship support, as well as professional satisfaction, represent protective factors of extra-individual resilience.24–35 Furthermore, resilience is a dynamic, multidimensional construct which helps the individual to cope with stress, referring not only to psychological skills but also to the ability to include family, social, and external support systems.35–37
Recovery style indicates instead the strategy by which the subject heals from the illness and represents the set of individual responses produced by adaptation mechanisms that can allow the patient, first, to deal with the symptoms in order to make them more tolerable, and then, to overcome the acute phase of the disease.15,38,39
Recovery styles can be identified along a continuum between two opposite poles: “integration” versus “sealing over”.40 Integration is a process by which psychotic experience makes the subject become aware of a continuity between own thoughts and feelings. Sealing over is a mechanism through which psychotic and non-psychotic mental events remain separated and so excluded from awareness by detachment and removal.39,41,42 Psychotic patients who adopt integration fight against their dysfunctional psychotic characteristics and manage, gradually, to merge these features in a more integrative form. Psychotic thoughts are perceived as stimulating by this kind of patient, and they are considered part of the same individual; moreover, psychosis represents a source of enlightenment for the subject, who may try to transform even more positively the initial health status and behavior. Therefore, this sort of individual presents greater awareness about the care received, offering the possibility to establish a better therapeutic relationship. Integration can allow greater investment in relationships and a better knowledge and tolerance of psychotic symptoms.43
Alternatively, psychosis can be sensed by patients who undertake the sealing over mechanism as a stranger and an intrusive object that should be kept separate. Sealer patients also identify more with negative stereotypes of mental illness (stigma) and are significantly affected by subjective alienation and a conviction of not being a member of society, which leads these individuals to experience greater discrimination and isolation and, consequently, a worse psychosocial functioning, a poorer life quality and greater incidence of depressed mood.15 The psychopathological characteristics potentially related to recovery style are: the mode of onset, the age at the time of the first treatment, the length of the illness, the rate of admission in hospital and the symptomatology of the last acute psychotic episode. There is no significant correlation between demographic features and recovery style, except for a higher tendency towards the integration of patients older than 45 years.40 Recently, recovery styles and resilience have been identified as important factors in predicting patient healing or symptom control, as well as psychosocial functioning and therapeutic adherence, and have begun to be considered as basic elements of recovery strategies.11,13,14,16,44–48 According to the scientific literature, quality of life and psychosocial functioning in schizophrenic patients are mainly influenced by the clinical manifestations of the disorder, such as positive, cognitive and negative symptoms. Recently, some studies have shown a correlation between quality of life and functioning with resilience/recovery style. However, this association is not universally shared, and there is little research related to the relationship between resilience/recovery style and clinical manifestation such as onset and intensity of positive, negative and cognitive symptoms.13,16 The present study arises from the hypothesis that the personal resources mentioned above may be able to influence, directly or indirectly, the modalities of clinical presentation of the disease, as well as individual functioning and quality of life.
The first aim of this research is to identify the potential capacity of resilience, recovery style, psychotic symptoms and neurocognition to influence psychosocial functioning and life quality of people with psychosis.
A secondary aim is to understand if personal resources, psychopathology, and neurocognition were independently associated with psychosocial functioning and quality of life, or through interactions between them.
Materials and methods
Sample
This observational naturalistic retrospective study observed patients assessed at different mental health facilities of the Psychiatric Unit of Varese, Northern Italy (Deliberate no. VIII/4221, February 28, 2007). Data collected were referred to the period between July 2017 and February 2018.
Data from patients who fulfilled the following inclusion criteria were collected: patients must be affected by a schizophrenia spectrum disorder (schizophrenia, schizoaffective disorder and other psychotic disorder) according to the Diagnostic and Statistical Manual of Mental Disorder - 5; must be aged between 18 and 65 years; must be a patient of the mental health facilities of the Psychiatric Unit; must sign a general written informed consent to the processing of their personal data; must have a CGI-S score <3; must have a history of illness >5 years; must have adhered to antipsychotic treatment over the previous year; and must have regular psychiatric evaluations.
Exclusion criteria were: incompetence to subscribe a generic informed consent for processing personal data; relevant organic and physical disadvantages or mental deficiency; psychopathological acute phase at first evaluation; current gestation or breastfeeding; current substance abuse.
All participants signed a general informed consent for processing personal data as a component of the normal diagnostic assessment procedure and quality check processes; the evaluation tools and rating scales were carried out by clinicians as part of the clinical routine.
Patient records were sealed in order to prevent the detectability of the participants, based on the Italian legislation (D.L. 196/2003, art. 110–24 July 2008, art. 13). The Provincial Health Ethical Review Board (Ethics Committee of Insubria – Varese, Italy) was previously consulted, and it confirmed that the study did not need authorization from the Board. The study was conducted in conformity with the ethical principles of the Declaration of Helsinki (with amendments) and Good Clinical Practice.
Evaluation tools
The rating scales considered are the following:
- Resilience Scale (RS), 10-items, Italian version.49 The Resilience Scale is the first scale for self-assessment of resilience published by Wagnild and Young in 1993.50 The initial scale consisted of 50 items, subsequently reduced to 25; subsequently, a 14-item version was elaborated, and also validated in Italian;51 finally, a short version of 10 items was created, that was widely used internationally. The measurement mode used, regardless of the version used, is a 7-point Likert scale (from 1= “strongly disagree” to 7= “strongly in agreement”). This instrument is built on five different dimensions, for each of which there are 5 or 2 items, respectively, in the 25-item and 10-item versions: perseverance or determination; balance or serenity; uniqueness; significance; self-confidence. The same Wagnild, however, revealed subsequently only two factors, namely personal competence and self-acceptance.52 RS total score is intended as a comprehensive indicator of resilience: bigger score means greater resilience. In this research we use the 10-item version, a clearer tool for the less well educated people or individuals with cognitive deficiency, like some subjects suffering from schizophrenia spectrum disorders. Cutoff scores for this scale are: less than 48 points reflects low resilience; between 49 and 59 indicates average resilience; higher than 59 indicates high resilience.
- Recovery Style Questionnaire (RSQ), Italian version.53 This questionnaire, compiled by the patient, is aimed at the rapid evaluation of the method of recovery from psychosis. This tool was originally developed by Drayton, Birchwood and Trower,44 and later translated and validated in Italian. The questionnaire is composed of 39 items, planned to mirror types expressed by those developed by Mc Glashan et al:42 these items, in groups of three, refer to the concepts of continuity, belonging, responsibility, curiosity, education, search for help, guilt, cause, optimism, impact, fear, appreciation, and satisfaction. For each item the patient can choose between two different types of answers, one representative of the recovery style “integration” type, the other reflecting the recovery style “sealing over” type. Thirteen scales were therefore computed: for each scale the patient is classified as “sealer“ or “integrator”, based on the answers given: if two of three answers for each item correspond to a particular recovery style (“integration” or “sealing over”), this style is attributed to the patient. In this study we calculated both scores: RSQ “sealing over” total score and RSQ “integrator” total score.
For this scale, cutoff values or normative scores have never been calculated.
- Montreal Cognitive Assessment (MoCA).54 This is a scale for fast evaluation of mild mental disability and evaluation of neurocognitive abilities. It evaluates eight cognitive aspects: attention and concentration, executive functions, memory, language, visual-constructive abilities, abstraction, calculation, and orientation. The highest score obtainable is 30; an amount equal to or greater than 23.28 is considered normal.55
- Schizophrenia Quality of Life Scale (SQLS).56 The SQoL is a tool aimed at assessing life quality, specific for subjects with schizophrenic disorders. It is a short self-assessment scale consisting of 30 items divided into three areas. 1) Psychosocial: 15 items that investigate affecting problems, such as a sensation of loneliness, depression or hopelessness, as well as problems in different collective contexts and concern for future. 2) Motivation and energy: 7 items that investigate motivation, will, and activity. 3) Symptoms and side effects: 8 items that assess aspects such as insomnia, blurred vision, vertigo, muscle contractions or xerostomia that could derive from antipsychotic therapies. The measurement mode used is a 5-point Likert scale, from 0=“never” to 4= “always”; greater scores correspond to a worse quality of life; for patients with a diagnosis of schizophrenia, normative scores are 44.97 points with a standard deviation of 21.23.
- Life Skills Profile (LSP), Italian version.57 This is an assessment scale of global functioning and disability of schizophrenic patients, administered by clinicians. The scale was developed in English by Parker and Rosen,58 and subsequently adapted in Italian in 1997. The term “life skill” expresses the concepts of basic skills and behaviors that allow an individual to adequately perform the activities of daily life and to be part of society. The scale has 39 questions with four multiple choices scoring from 1 (negative end) to 4 (positive end). The total score can oscillate from 39 to 156 points, whereas concerning the five subscales, each of which refers to specific social proficiencies in everyday life: “self-care” (10 items), “non-turbulence” (12 items), “social contact” (six items), “communicative” (six items), and “responsibility” (five items), higher scorings correspond to a greater competence. For patients with a diagnosis of schizophrenia, normative scores are 118.8 points with a standard deviation of 17.7 points.
- Positive and Negative Syndrome Scale (PANSS).59 This is a 7-point instrument, standardized by Kay et al, and was conceived as an operational method for evaluating positive, negative and general psychological symptoms deriving from a semi-structured clinical assessment and other sources of information, such as clinical records. The scale is mainly used for psychotic spectrum disorders, although it is not diagnosis-specific and it can also be used for affective spectrum disorders. The following areas are investigated: positive symptoms; negative symptoms; and general psychopathology like physical manifestations (tensions, formalisms and posture, excitement, unaffectivity), interpersonal behaviors (poor relationships, lack of collaboration, lack of attention, hostility), verbal cognitive processes (mental disorganization, stereotyped thinking, lack of spontaneity and conversational flow), content of thought (grandiosity, concerns inherent to the physical aspect, feelings of guilt, disappointments), answer to structured interview (disorientation, anxiety, depression, difficulty in abstract thinking) and degree of aggression. For each of the 30 items the degree of intensity is expressed on a scale from 0 (none) to 7 (maximum). The total score and the scores of the single items are then calculated to define the patient’s clinical profile. PANSS is widely used in clinical practice as it has proved useful in resolving particularly difficult diagnostic cases and preparing detailed psychological relationships. It has also proved to be very sensitive to clinical changes related to both pharmacological and non-pharmacological therapies. In this study we used three different scores: positive symptom scoring; negative symptom scoring; and general psychopathology scoring. Normative scores are: 18.20 points with a standard deviation of 6.08 for positive symptoms; 21.02 points with a standard deviation of 6.17 for negative symptoms; 37.74 points with a standard deviation of 9.49 for general psychopathology.
Statistical analysis
We took into consideration continuous variables reporting averages and SD; we presented categorical variables as relative frequencies. We used the Kruskal–Wallis test to assess any statistically significant differences among subjects affected by schizophrenia and those with schizoaffective disorder or other psychotic disorder. General psychopathology (PANSS General Psychopathology Scale), positive psychotic symptoms (PANSS Positive Scale) and negative psychotic symptoms (PANSS Negative Scale), neurocognitive functions (MoCA total score), recovery style (RSQ Integrator and Sealing Over Scale) and resilience (RS total score) were considered as independent variables. Psychosocial functioning (LSP total score) and quality of life (SQoL total score) were considered dependent variables. Based on the data obtained from the Pearson correlation, we used multiple linear regression models to investigate the association among independent variables and psychosocial functioning or life quality. We used a simultaneous linear regression in both cases, inserting only the independent variables statistically correlated with the dependent variables to decrease the ordinary variance among variables and to ban less important variables. In the first analysis, LSP total score was fixed as the dependent variable; in the second analysis, the dependent variable was SQoL total score. Finally, two different generalized linear model were used to identify any statistically significant interactions among the independent variables and to detect any moderators. As in the previous case, in the first analysis, LSP total score was fixed as the dependent variable; in the second analysis, the dependent variable was SQoL total score. Only the independent variables statistically correlated with the dependent variables were considered as covariate variables. Results were analysed through the IBM® SPSS® Statistics, version 20.0.
Results
Demographic and clinical data
As shown in Table 1, among the 64 subjects evaluated, 44 patients fulfilled the inclusion criteria: 30 patients were male (68%), while the remaining 14 subjects were female (32%). The mean age was 46.48 years (SD 11.53); the mean length of the history of the disease at recruitment was 23.50 years (SD 11.29) with an average age at first episode of psychosis (FEP) of 23.70 years (SD 7.24). In 77% of the patients (n=34) a diagnosis of schizophrenia was observed, 11.5% (n=5) of the sample have a diagnosis of schizoaffective disorder, and in 11.5% (n=5) of the sample a diagnosis of other psychotic disorder was detected.
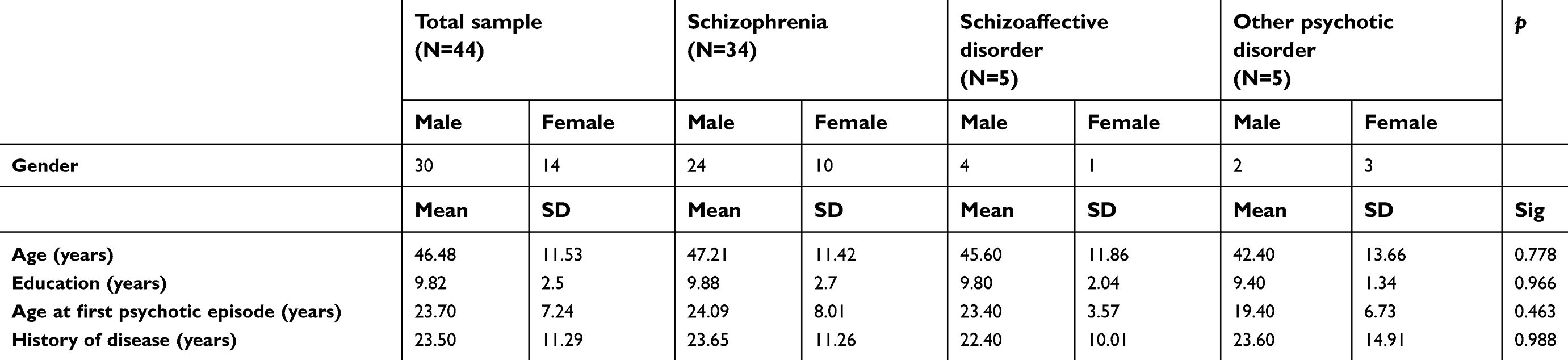 | Table 1 Characteristics of the sample |
Descriptive analyses of clinical variables are shown in Table 2. At first evaluation, the mean MoCA total score in the total sample was 21.34 (SD 4.47), the average RS total score was 52.30 (SD 9.68), while the average RSQ integration score and RSQ sealing over score were, respectively, 24.11 (SD 4.70) and 14.89 (SD 4.70); the average PANSS positive scale and negative scale were, respectively, 18.11 (SD 6.80) and 23.09 (SD 8.81), while the average PANSS general psychopathology scale was 45.50 (SD 14.84); the average LSP total score was 117.73 (SD 20.33), and the mean SQoL total rate was 51.93 (SD 13.22).
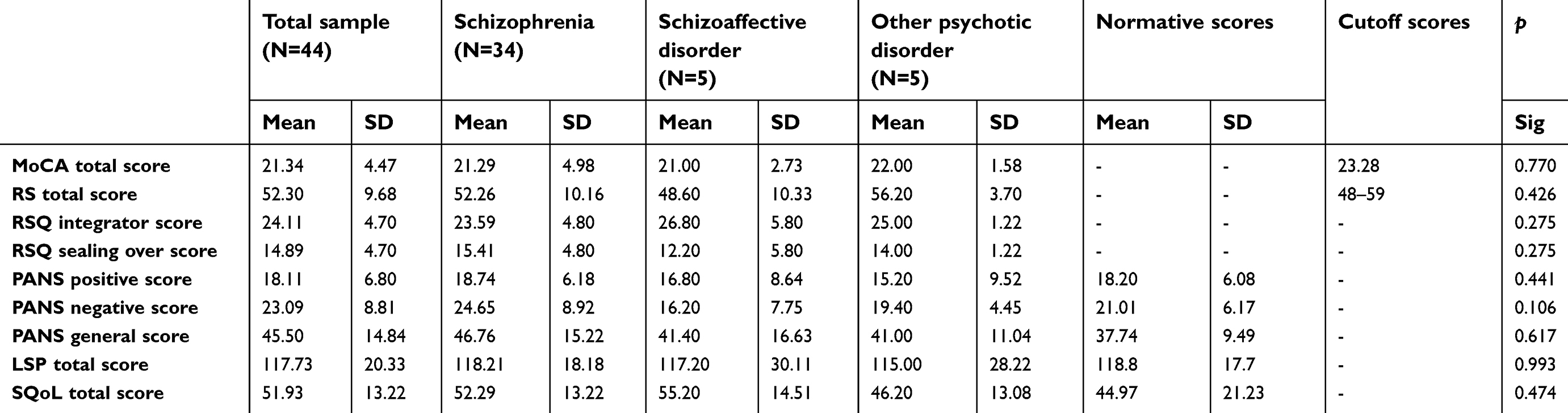 | Table 2 Data on resilience, recovery style, neurocognition, psychotic symptomatology, quality of life and social functioning |
As reported in Tables 1 and 2, no statistically significant differences among the three different psychotic disorders in any scales and demographic characteristics were observed. Furthermore, despite the small sample size, the clinical data can be considered representative, as evidenced by the comparison with the normative scores, especially regarding positive and negative symptoms, resilience and psychosocial functioning.
Multilinear regression
Pearson correlations are shown in Table 3. As regards the correlations with psychosocial functioning, a statistically significant negative correlation (p<0.001) among LSP global score and PANSS positive symptoms scoring and general psychopathology score emerged; however, a weak negative correlation (p<0.01) between LSP total score and RSQ sealing over score was described. RSQ integrator score and MoCA global scoring were found to be positively correlated with LSP total score, with a significance of p<0.01 and p<0.001, respectively.
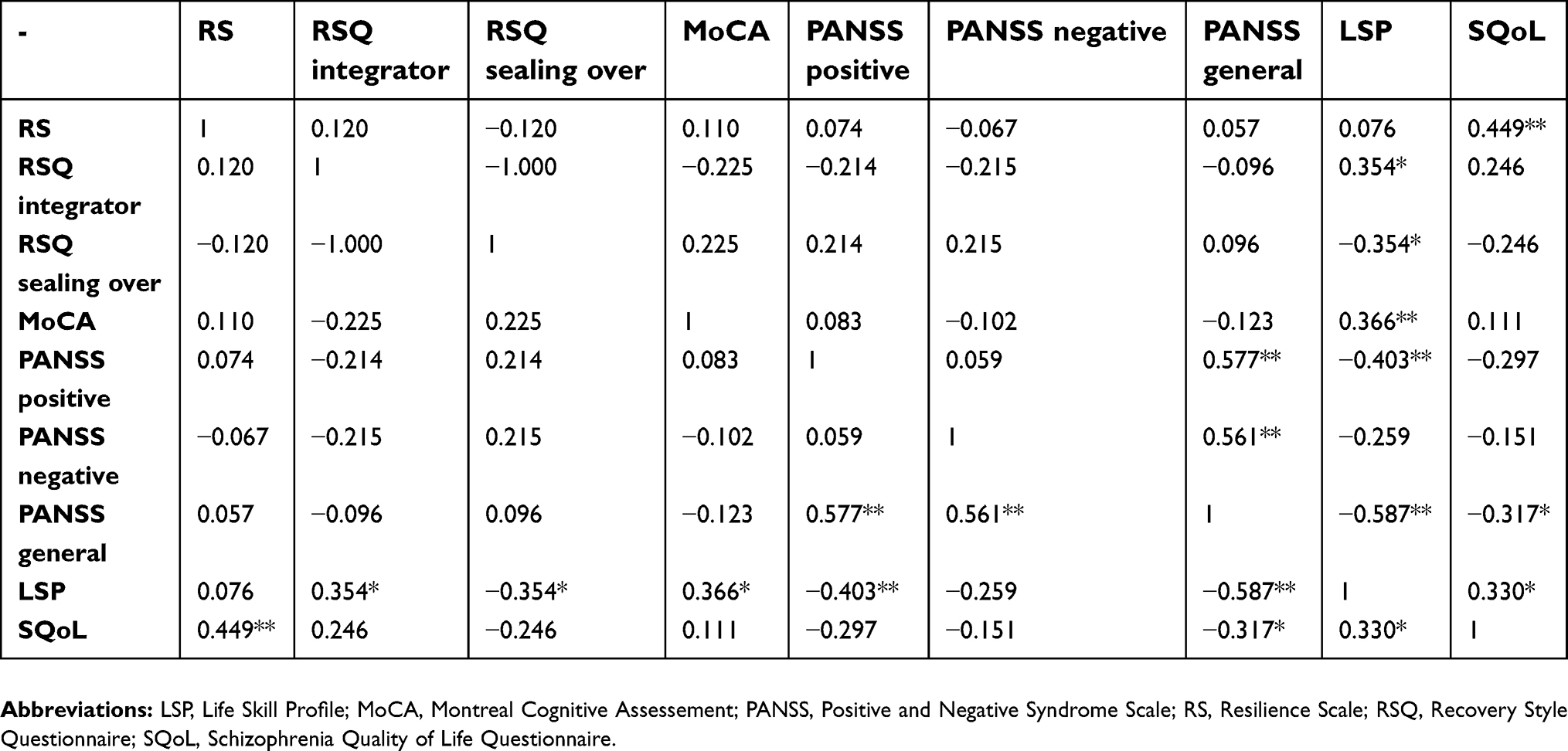 | Table 3 Pearson correlations among RS total score, RSQ “integrator” and RSQ “sealing over” score, MoCA total score, PANSS positive, negative and general psychopathology score; LSP total score and SQoL total score |
Quality of life was significantly and positively correlated with resilience (p<0.001), while a negative correlation with general psychopathology (p<0.01) emerged.
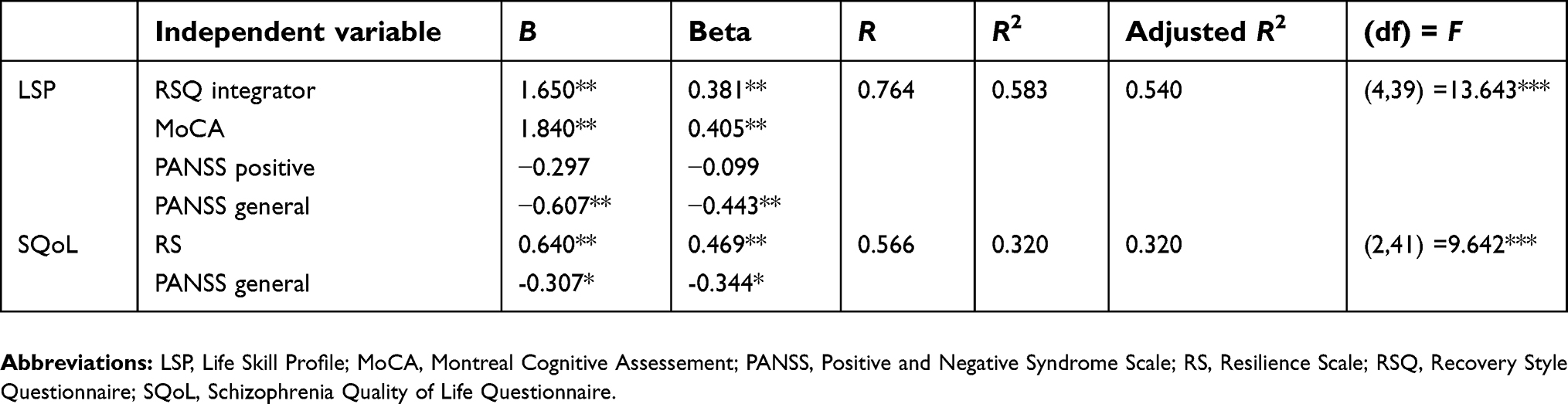
Results from multiple linear regression analysis are provided in Table 4.
 | Table 4 Multiple linear regression among LSP and SQoL total score, RS total score, RSQ integrator score, MoCA total score, PANSS positive score, and PANSS general psychopathology score |
LSP global scoring was fixed as the dependent variable; the predictors summed were RSQ integrator score, MoCA total score, PANSS positive symptoms score and PANSS general psychopathology score. RS total score and PANSS negative symptoms score were removed from these analyses since there was no significant correlation with psychosocial functioning; RSQ sealing over score was not entered because its correlation values were reciprocal to those of RSQ integration scores. The model obtained explained 54.0% of the psychosocial functioning variance in the sample being examined (adjusted R2=0.540; F (4.39) =13.643, p<0.001). In particular, PANSS general psychopathology score was the most associated variable with LSP total score (B= −0.607, beta =−0.443; p<0.001), followed by MoCA total score (B=1.840, beta=0.405; p<0.001) and RSQ integrator score (B=1.650, beta=0.381; p>0.001); PANSS positive symptoms score was not statistically associated with LSP total score (B=−0.297, beta=−0.443). PANSS general psychopathology score was negatively associated with LSP total score, while the RSQ integration score and MoCA total score were positively associated with LSP total score.
SQoL total score was fixed as the dependent variable; RS total score and PANSS general psychopathology were added as independent variables, following the principles previously adopted. This model explained only 28.7% of the quality of life variance in the total sample (adjusted R2=0.287; F (2.41) =9.642; p<0.01): only RS total score was positively associated with SQoL total score (B=0.640, beta=0.469; p<0.01), while general psychopathology score was negatively associated with quality of life (B=−0.307, beta=−0.344; p<0.01).
Generalized linear model
Results of the generalized linear models are reported in Table 5. First, LSP total score was fixed as the dependent variable, while RSQ integration score, MoCA total score, PANSS positive symptoms score, and PANSS general psychopathology score were set as covariate variables. In this analysis, all the independent variables, except PANSS positive symptoms score, present a statistically significant direct effect on LSP total score; however, no statistically significant interactions among the covariate variables were observed. The same results were obtained by inserting SQoL total score as the dependent variable, and RS standardized total score and PANSS standardized general psychopathology score as covariate variables. In both cases, no independent variables act as a moderator to each other as regards the effect on dependent variables.
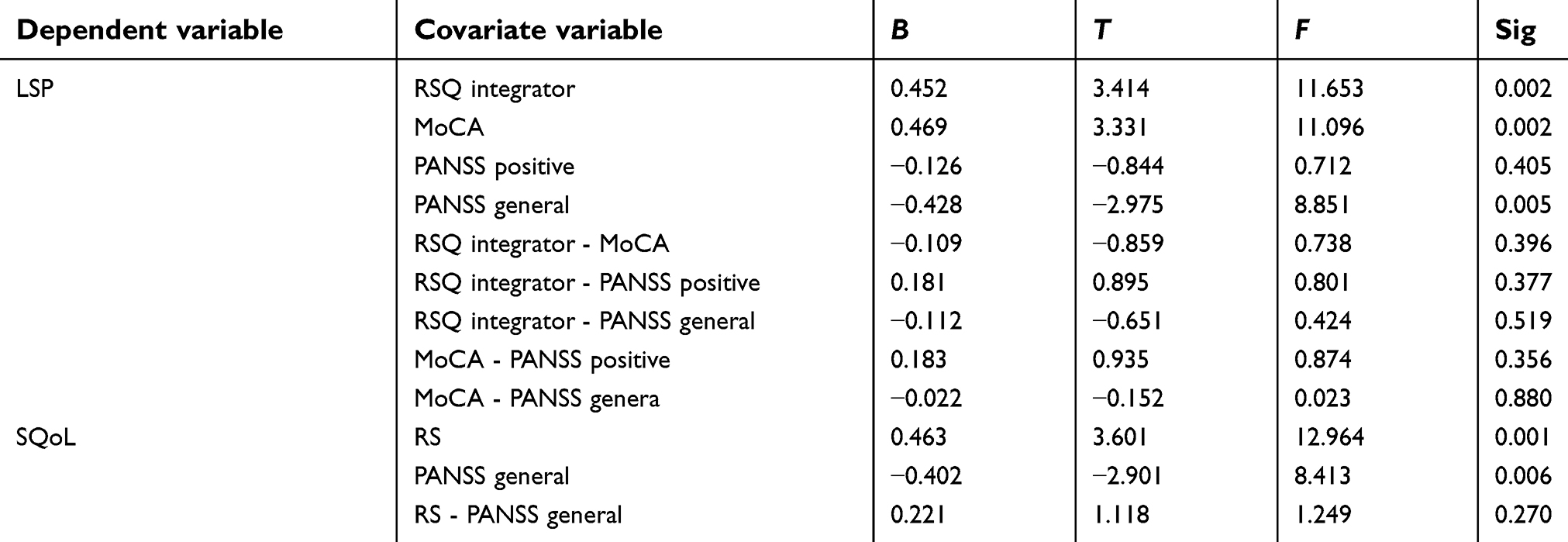 | Table 5 Generalized linear model among LSP and SQoL total score, RS total score, RSQ integrator score, MoCA total score, PANSS positive score and PANSS general psychopathology score |
Discussion
According to the current literature,14,16,17 a statistically significant correlation among personal resources, symptomatology, and real-life functioning was observed. Data show that general psychopathology, neurocognition, and integration recovery style can predict psychosocial functioning in people affected by psychosis, and explain ~54% of the LSP variance.
As expected, the association between PANSS general psychopathology score and LSP total score was negative;60 this is the heavier association with life functioning. This datum is complementary to that of other studies, which have shown the importance of reducing the psychotic symptomatology before successfully applying other types of interventions.61,62 In contrast, a strong positive association between neurocognition and psychosocial functioning was detected: deficits in psychomotor activity, attention, working memory, and executive functions have proved to be among the strongest predictors of the functional outcome.14,16,17,63 Precisely for this reason, cognitive remediation strategies are today considered as valuable tools in the treatment of chronic psychoses, especially if they are associated with psychosocial interventions.63,64 Among the personal resources, the integration recovery style was found to be significantly associated with a good functional outcome: thanks to greater acceptance of their psychotic experience and awareness of the need for support and care, the integrator patients are more likely to maintain their social role and to invest in interpersonal relationships.14,43 In spite of other research,14,22 in our study, no significant correlations between resilience and psychosocial functioning emerged, probably due to the use of a measurement tool built exclusively on the basis of individual abilities and predispositions, and not on family and external support too; indeed, some studies have highlighted the greater importance of intrapersonal resilience factors, such as family and social support, compared to intrapersonal factors in predicting psychosocial functioning.22
Intrapersonal resilience factors were instead associated with the life quality of psychotic subjects, together with the general symptomatology: data show that RS total score and PANSS general psychopathology score can predict and explain ~29% of the LSP variance. Also in this case, psychotic symptomatology turns out to be a negative predictive factor, whereas resilience can be considered as a protective factor. In fact, a good opinion of one’s own capabilities, a methodic style and a positive perception of the future permit psychotic patients to go beyond symptomatology distress.25,26,30 The better the self-perception, perspectives for the future, and the ability to design and organize the routine are, the better the perception of their own quality of life will be. Therefore, resilience and recovery style are two complementary personal resources, both important to guarantee a good outcome to psychotic patients, alongside the stabilization of psychotic symptoms with psychopharmacological therapy and the improvement of neurocognitive functions.
Despite the interesting results obtained, the study has some limits: first of all, the small sample size does not allow generalizable results, but only to provide elements for future research. Moreover, although a minority of patients had a diagnosis of psychotic disorder and schizoaffective disorder, a sub-analysis was not made, and this represents another limit of the results. Since we excluded patients with current use of substances, another limitation of the study could be represented by the bias derived from the possible influence on neurocognition and health-related quality of life of past use of psychoactive substances, as shown by recent literature.65–68
A future perspective could be the evaluation of a larger sample, inclusion of additional variables (such as stigma and social support) and follow-up research in order to identify causal links.
Conclusions
The present study has confirmed the existence of a strong association among personal resources and life quality and psychosocial functioning in individuals with psychosis. Resilience and recovery style are independent and complementary predictive factors: the first is able to positively influence the real-life functioning, and the second can improve the personal perception of the quality of life; together they allow better results in the treatment of psychosis, fighting the discomfort arising from the symptoms and cognitive impairment.
These results emphasize the need for tailor-made interventions for people with psychosis: the reduction of symptoms attributable to psychopharmacological therapy and cognitive remediation strategies are not enough to gain a functional outcome. Within psychosocial and rehabilitative interventions, mastering resilience and promoting integration recovery style could improve real-life functioning and ensuring a higher quality of life.11,46,61
Disclosure
No conflicts of interests in this work are reported by the authors.
References
1. Dean K, Murray RM. Environmental risk factors for psychosis. Dialogues Clin Neurosci. 2005;7(1):69–80.
2. Pruessner M, Cullen AE, Aas M, Walker EF. The neural diathesis-stress model of schizophrenia revisited: an update on recent findings considering illness stage and neurobiological and methodological complexities. Neurosci Biobehav Rev. 2017;73:191–218. doi:10.1016/j.neubiorev.2016.12.013
3. Caselli I, Poloni N, Ielmini M, Diurni M, Callegari C. Epidemiology and evolution of the diagnostic classification of factitious disorders in DSM-5. Psychol Res Behav Manag. 2017;10:387–394. doi:10.2147/PRBM.S153377
4. Callegari C, Berto E, Caselli I, Bressani R, Vender S. Multidisciplinary integrated approach to mental illness: semi-residential setting and quality of life. Minerva Psichiatr. 2016;57(1):34–41.
5. Velthorst E, Reichenberg A, Ivanov I, et al. An integrative approach to test the relationship between social impairment and the development of psychosis. Schizophr Bull. 2017;43(1):S53. Epub 2017 March 20. doi:10.1093/schbul/sbx021.137
6. Wigman JT, de Vos S, Wichers M, van Os J, Bartels-Velthuis AA. A transdiagnostic network approach to psychosis. Schizophr Bull. 2017;43(1):122–132. doi:10.1093/schbul/sbw095 Epub 2016 Jul 6.
7. Diurni M, Baranzini F, Costantini C, Poloni N, Vender S, Callegari C. Metabolic side effects of second generation antipsychotics in drug-naive patients: a preliminary study. Riv Psichiatr. 2009;44(3):176–178. Italian.
8. Bolla E, Bortolaso P, Ferrari M, et al. Are CYP1AA2*1F and *1C associated with clozapine tolerability? A preliminary investigation. Psychiatry Res. 2011;189(3):438. Epub 2011 Apr 8. doi:10.1016/j.psychres.2011.03.011
9. Albert U, Carmassi C, Cosci F, et al. Role and clinical implications of atypical antipsychotics in anxiety disorders, obsessive-compulsive disorder, trauma-related, and somatic symptom disorders: a systematized review. International Clin Psychopharmacol. 2016;31(5):249–258. doi:10.1097/YIC.0000000000000127
10. Ostuzzi G, Mazzi MA, Terlizzi S, et al. Factors associated with first- versus second-generation long-acting antipsychotics prescribed under ordinary clinical practice in Italy. PLoS One. 2018;13(8):e0201371. doi10.1371/journal.pone.0201371 eCollection 2018.
11. Semisa D, Casacchia M, Di Munzio W, et al. Gruppo SIEP-DIRECT’S. Promoting recovery of schizophrenic patients: discrepancy between routine practice and evidence. The SIEP-DIRECT’S Project. Epidemiol Psichiatr Soc. 2008;17(4) Italian:331–349. doi:10.1017/S1121189X00000130
12. Oorschot M, Lataster T, Thewissen V, et al. Symptomatic remission in psychosis and real-life functioning. Br J Psychiatry. 2012;201(3):215–220. Epub 2012 Jun 28. doi:10.1192/bjp.bp.111.104414
13. Kim KR, Song YY, Park JY, et al. The relationship between psychosocial functioning and resilience and negative symptoms in individuals at ultra-high risk for psychosis. Aust N Z J Psychiatry. 2013;47(8):762–771. doi:10.1177/0004867413488218
14. Galderisi S, Rossi A, Rocca P, et al. Italian network for research on psychoses. The influence of illness-related variables, personal resources and context-related factors on real-life functioning of people with schizophrenia. World Psychiatry. 2014;13(3):275–287. doi:10.1002/wps.20167
15. Espinosa R, Valiente C, Rigabert A, Song H. Recovery style and stigma in psychosis: the healing power of integrating. Cogn Neuropsychiatry. 2016;21(2):146–155. doi:10.1080/13546805.2016.1147427 Epub 2016 Feb 29.
16. Rossi A, Galderisi S, Rocca P, et al. Italian network for research on psychoses. The relationships of personal resources with symptom severity and psychosocial functioning in persons with schizophrenia: results from the Italian network for research on psychoses study. Eur Arch Psychiatry Clin Neurosci. 2017;267(4):285–294. doi:10.1007/s00406-016-0710-9
17. Rossi A, Amore M, Galderisi S, et al. Italian network for research on psychoses. The complex relationship between self-reported ‘personal recovery’ and clinical recovery in schizophrenia. Schizophr Res. 2018;192:108–112.Epub 2017 May 9. doi10.1016/j.schres.2017.04.040
18. Luthar S. Resilience and Vulnerability: Adaptation in the Context of Childhood Adversities. New York: Cambridge University Press; 2003.
19. Rutter M. Implications of resilience concepts for scientific understanding. Ann N Y Acad Sci. 2006;1094:1–12. doi:10.1196/annals.1376.002
20. Callegari C, Bertù L, Caselli I, et al. Resilience in older adults: influence of the admission in nursing home and psychopatology. Neuropsychiatry. 2016a;6(4):117–123. doi:10.4172/Neuropsychiatry.1000129
21. Kim-Cohen J. Resilience and developmental psychopathology. Child Adolesc Psychiatr Clin N Am. 2007;16(2):271–283. doi:10.1016/j.chc.2006.11.003
22. Poloni N, Zizolfi D, Ielmini M, et al. A naturalistic study on the relationship among resilient factors, psychiatric symptoms, and psychosocial functioning in a sample of residential patients with psychosis. Psychol Res Behav Manag. 2018;11:123–131.eCollection 2018. doi10.2147/PRBM.S159571
23. Laudadio A, Fiz Perez F, Mazzocchetti L. Valutare La Resilienza. Teorie, Modelli E Strumenti. Roma: Carrocci; 2011. Italian.
24. Marulanda S, Addington J. Resilience in individuals at clinical high risk for psychosis. Early Interv Psychiatry. 2016;10(3):212–219. doi:10.1111/eip.12174
25. Morin L, Franck N. Rehabilitation interventions to promote recovery from schizophrenia: a systematic review. Front Psychiatry. 2017;12(8):100. doi:10.3389/fpsyt.2017.00100
26. Jordan G, Malla A, Iyer SN. Posttraumatic growth following a first episode of psychosis: a mixed methods research protocol using a convergent design. BMC Psychiatry. 2016;25(16):262. doi:10.1186/s12888-016-0977-4
27. Mizuno Y, Wartelsteiner F, Frajo-Apor B. Resilience research in schizophrenia: a review of recent developments. Curr Opin Psychiatry. 2016;29(3):218–223. doi:10.1097/YCO.0000000000000248
28. Christiani CJ, Jepsen JRM, Thorup A, et al. Social cognition, language, and social behavior in 7-year-old children at familial high-risk of developing schizophrenia or bipolar disorder: the danish high risk and resilience study via 7-a population-based cohort study. Schizophr Bull. 2019. doi:10.1093/schbul/sbz001
29. Henderson AR, Cock A. The responses of young people to their experiences of first-episode psychosis: harnessing resilience. Community Ment Health J. 2015;51(3):322–328. doi:10.1007/s10597-014-9769-9
30. Torgalsbøen AK, Fu S, Czajkowski N. Resilience trajectories to full recovery in first-episode schizophrenia. Eur Psychiatry. 2018;52:54–60. doi:10.1016/j.eurpsy.2018.04.007
31. Salmon P, Dowrick C, Ring A, Humphris G. Voiced but unheard agendas: qualitative analysis of the psychosocial cues that patients with unexplained symptoms present to general practitioners. Br J Gen Pract. 2004;54(3):171–176.
32. Dowrick C, Kokanovic R, Hegarty K, Griffiths F, Gunn J. Resilience and depression: perspectives from primary care. Health (London). 2008;12(4):439–452. doi:10.1177/1363459308094419
33. O’Keeffe D, Hannigan A, Doyle R, et al. The iHOPE-20 study: relationships between and prospective predictors of remission, clinical recovery, personal recovery and resilience 20 years on from a first episode psychosis. Aust N Z J Psychiatry. 2019;6:4867419827648.
34. Milioni M, Alessandri G, Eisenberg N, et al. Reciprocal relations between emotional self-efficacy beliefs and ego-resiliency across time. J Pers. 2015;83(5):552–563. doi:10.1111/jopy.12131
35. Gooding PA, Littlewood D, Owen R, Johnson J, Tarrier N. Psychological resilience in people experiencing schizophrenia and suicidal thoughts and behaviours. J Ment Health. 2017;28:1–7. doi:10.1080/09638237.2017.1294742
36. Rebagliati GA, Sciumè L, Iannello P, et al. Frailty and resilience in an older population. The role of resilience during rehabilitation after orthopedic surgery in geriatric patients with multiple comorbidities. Funct Neurol. 2016;31(3):171–177.
37. Bozikas VP, Parlapani E, Holeva V, et al. Resilience in patients with recent diagnosis of a schizophrenia spectrum disorder. J Nerv Ment Dis. 2016;204(8):578–584. doi:10.1097/NMD.0000000000000541
38. Poloni N, Diurni M, Buzzi A, et al. Recovery style, symptoms and psychosocial functioning in psychotic patients: a preliminary study. Riv Psichiatr. 2013;48(5) Italian:386–392. doi:10.1708/1356.15065
39. Callegari C, Caselli I, Bertù L, et al. Evaluation of the burden management in a psychiatric day center: distress and recovery style. Riv Psichiatr. 2016d;51(4):149–155. Italian.
40. Staring AB, van der Gaag M, Mulder CL. Recovery style predicts remission at one-year follow-up in outpatients with schizophrenia spectrum disorders. J Nerv Ment Dis. 2011;199(5):295–300. doi:10.1097/NMD.0b013e3182174e97
41. Cavelti M, Homan P, Vauth R. The impact of thought disorder on therapeutic alliance and personal recovery in schizophrenia and schizoaffective disorder: an exploratory study. Psychiatry Res. 2016;239:92–98. doi:10.1016/j.psychres.2016.02.070
42. Lemos-Giráldez S, García-Alvarez L, Paino M, et al. Measuring stages of recovery from psychosis. Compr Psychiatry. 2015;56:51–58. doi:10.1016/j.comppsych.2014.09.021
43. Bell MD, Zito W. Integrated versus sealed-over recovery in Schizophrenia BORRTI and executive functions. J Nerv Ment Dis. 2005;193(1):3–8.
44. Rampling J, Furtado V, Winsper C, et al. Non-pharmacological interventions for reducing aggression and violence in serious mental illness: A systematic review and narrative synthesis. Eur Psychiatry. 2016;34:17–28. doi:10.1016/j.eurpsy.2016.01.2422
45. Pilling S, Bebbington P, Kuipers E, et al. Psychological treatments in schizophrenia: II. Meta-analyses of randomized controlled trials of social skills training and cognitive remediation. Psychol Med. 2002;32(5):783–791. doi:10.1017/S0033291702005640
46. Harrow M, Jobe TH. Factors involved in outcome and recovery in schizophrenia patients not on antipsychotic medication: a 15-year multifollow-up study. J Nerv Ment Dis. 2007;195(5):406–414.
47. Rudnick A, Martins J. Coping and schizophrenia: a re-analysis. Arch Psychiatr Nurs. 2009;23(1):11–15. doi:10.1016/j.apnu.2008.02.009
48. Poloni N, Armani S, Ielmini M, et al. Characteristics of the caregiver in mental health: stress and strain. Minerva Psichiatr. 2017;58(3):118–124.
49. Girtler N, Casari EF, Brugnolo A, et al. Italian validation of the Wagnild and Young Resilience Scale: a perspective to rheumatic diseases. Clin Exp Rheumatol. 2010;28(5):669–678.
50. Wagnild GM, Young HM. Development and psychometric evaluation of the resilience scale. J Nurs Meas. 1993;1:165–178.
51. Callegari C, Bertù L, Lucano M, Ielmini M, Braggio E, Vender S. Reliability and validity of the Italian version of the 14-item resilience scale. Psychol Res Behav Manag. 2016c;3(9):277–284. doi:10.2147/PRBM.S115657
52. Wagnild GM, Collins JA. Assessing Resilience. J Psychosoc Nurs Ment Health Serv. 2009;47(12):28–33. doi:10.3928/02793695-20091103-01
53. Poloni N, Callegari C, Buzzi A, et al. The Italian version of ISOS and RSQ, two suitable scales for investigating recovery style from psychosis. Epidemiol Psichiatr Soc. 2010;19(4):352–359. Italian.
54. Nasreddine ZS, Phillips NA, Bédirian V, et al. The montreal cognitive assessment, MOCA: a brief screening tool for mild cognitive impairment. J Am Geriatr Soc. 2009;53(4):695–699. doi:10.1111/j.1532-5415.2005.53221.x
55. Conti S, Bonazzi S, Laiacona M, Masina M, Coralli MV. Montreal Cognitive Assessment (MoCA)-Italian version: regression based norms and equivalent scores. Neurol Sci. 2015;36(2):209–214. doi:10.1007/s10072-014-1921-3 Epub 2014 Aug 20.
56. Wilkinson G, Hesdon B, Wild D, et al. Self-report quality of life measure for people with schizophrenia: the SQLS. Br J Psychiatry. 2000;177:42–46.
57. Rosen A, Hadzi-Pavlov D, Parker G. The Life Skills Profile: a measure assessing function and disability in schizophrenia. Schizophr Bull. 1989;15(2):325–337. doi:10.1093/schbul/15.2.325
58. Zizolfi S. The Italian version of Life Skills Profile (LSP), an instrument for evaluating performance and disabilities of schizophrenic patients. Epidemiol Psichiatr Soc. 1997;6(3):196–204. Italian. doi:10.1017/S1121189X00005054
59. Kay SR, Fiszbein A, Opler LA. The Positive and Negative Syndrome Scale (PANSS) for Schizophrenia. Schizophr Bull. 1987;13(2):261–276. doi:10.1093/schbul/13.2.261
60. Llorca PM, Blanc O, Samalin L, Bosia M, Cavallaro R. Factors involved in the level of functioning of patients with schizophrenia according to latent variable modeling. Eur Psychiatry. 2012;27(6):396–400. doi:10.1016/j.eurpsy.2011.01.010
61. Hogarty GE. Personal Therapy for Schizophrenia and Related Disorders: A Guide to Individualized Treatment. New York: Guilford; 2002.
62. Tandon R, Nasrallah HA, Keshavan MS. Schizophrenia, “just the facts” 5: treatment and prevention. Past, present, and future. Schizophr Res. 2010;122(1–3): 1–23. doi:10.1016/j.schres.2010.05.025
63. Mc Gurk SR, Twamley EW, Sitzer DI, McHugo GJ, Mueser KT. A meta-analysis on cognitive remediation in schizophrenia. Am J Psychiatry. 2007;164(12):1791–1802. doi:10.1176/appi.ajp.2007.07060906
64. Wykes T, Huddy V, Cellard C, McGurk SR, Czobor P. A meta-analysis of cognitive remediation for schizophrenia: methodology and effect sizes. Am J Psychiatry. 2011;168(5):472–485. doi:10.1176/appi.ajp.2010.10060855
65. Benaiges I, Serra-Grabulosa JM, Adan A. Neuropsychological functioning and age-related changes in schizophrenia and/or cocaine dependence. Prog Neuropsychopharmacol Biol Psychiatry. 2013;40:298–305. doi:10.1016/j.pnpbp.2012.10.016
66. Benaiges I, Prat G, Adan A. Health-related quality of life in patients with dual diagnosis: clinical correlates. Health Qual Life Outcomes. 2012;5(10):106. doi:10.1186/1477-7525-10-106
67. Adan A, Arredondo AY, Capella MD, Prat G, Forero DA, Navarro JF. Neurobiological underpinnings and modulating factors in schizophrenia spectrum disorders with a comorbid substance use disorder: A systematic review. Neurosci Biobehav Rev. 2017;75:361–377. doi:10.1016/j.neubiorev.2017.01.038
68. Benaiges I, Serra-Grabulosa JM, Prat G, Adan A. Executive functioning in individuals with schizophrenia and/or cocaine dependence. Hum Psychopharmacol. 2013;28(1):29–39. doi:10.1002/hup.2279
 © 2019 The Author(s). This work is published and licensed by Dove Medical Press Limited. The
full terms of this license are available at https://www.dovepress.com/terms
and incorporate the Creative Commons Attribution
- Non Commercial (unported, 3.0) License.
By accessing the work you hereby accept the Terms. Non-commercial uses of the work are permitted
without any further permission from Dove Medical Press Limited, provided the work is properly
attributed. For permission for commercial use of this work, please see paragraphs 4.2 and 5 of our Terms.
© 2019 The Author(s). This work is published and licensed by Dove Medical Press Limited. The
full terms of this license are available at https://www.dovepress.com/terms
and incorporate the Creative Commons Attribution
- Non Commercial (unported, 3.0) License.
By accessing the work you hereby accept the Terms. Non-commercial uses of the work are permitted
without any further permission from Dove Medical Press Limited, provided the work is properly
attributed. For permission for commercial use of this work, please see paragraphs 4.2 and 5 of our Terms.